
Association between Abnormal Gait Patterns and an Elevated Degree of Pain after Daily Walking: A Preliminary Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Assessment of Pain
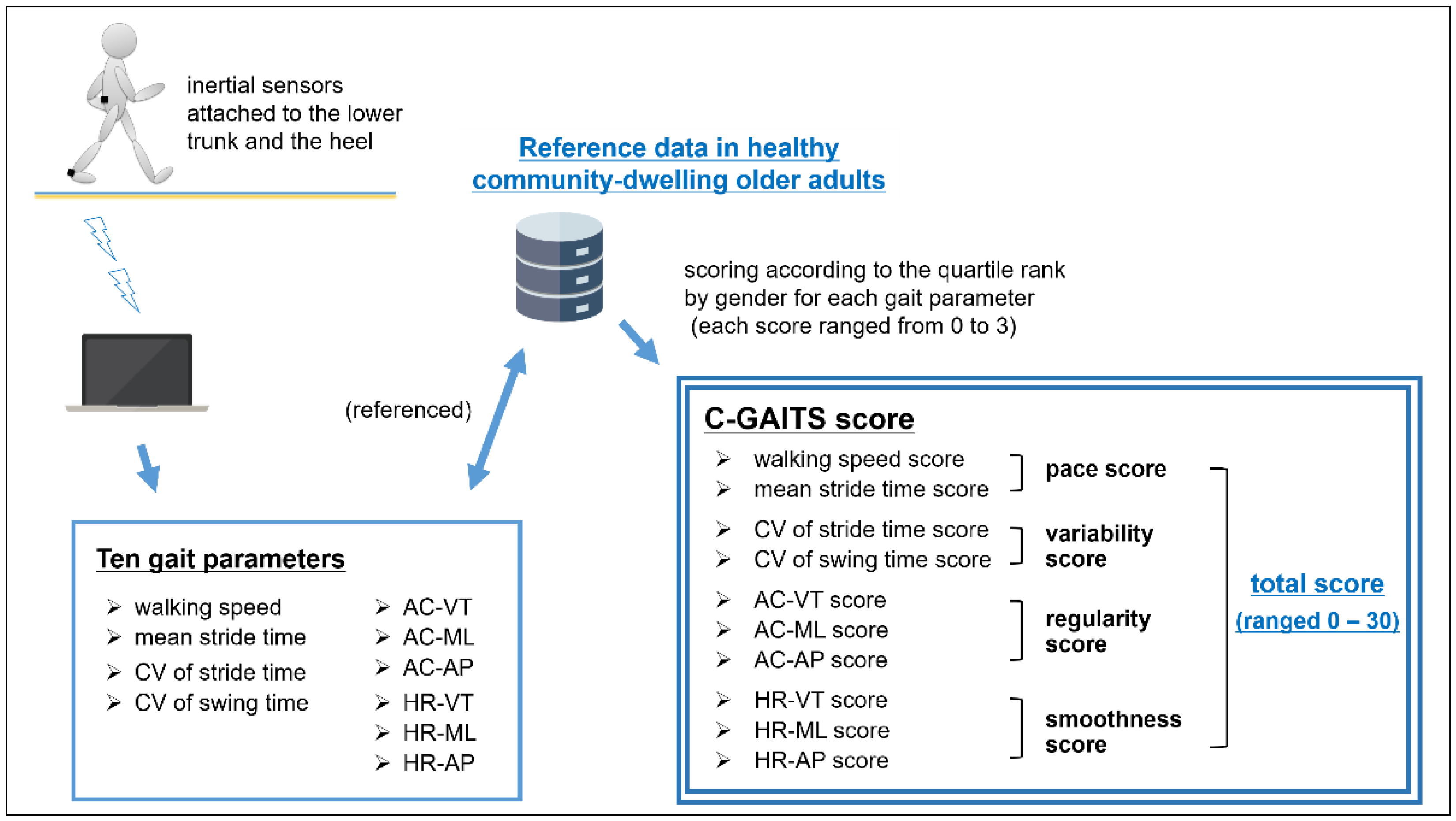
2.3. Assessment of Gait Pattern
2.4. Statistical Analyses
3. Results
3.1. Characteristics of the Study Subjects
3.2. Experiencing an Elevated Degree of Pain after Walking and C-GAITS Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Helme, R.D.; Gibson, S.J. The epidemiology of pain in elderly people. Clin. Geriatr. Med. 2001, 17, 417–431. [Google Scholar] [CrossRef]
- Iijima, H.; Suzuki, Y.; Aoyama, T.; Takahashi, M. Relationship between Varus Thrust during Gait and Low Back Pain in Individuals with Knee Osteoarthritis. Arthritis Care Res. 2020, 72, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- van der Esch, M.; Steultjens, M.P.M.; Harlaar, J.; van den Noort, J.C.; Knol, D.L.; Dekker, J. Lateral trunk motion and knee pain in osteoarthritis of the knee: A cross-sectional study. BMC Musculoskelet. Disord. 2011, 12, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Lu, Q. A current review of foot disorder and plantar pressure alternation in the elderly. Phys. Act. Health 2020, 4, 95–106. [Google Scholar] [CrossRef]
- Ko, S.-U.; Simonsick, E.M.; Deshpande, N.; Studenski, S.; Ferrucci, L. Ankle Proprioception-Associated Gait Patterns in Older Adults: Results from the Baltimore Longitudinal Study of Aging. Med. Sci. Sports Exerc. 2016, 48, 2190–2194. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, E.F.; Shi, L.; Bean, J.F.; Hausdorff, J.M.; Dong, Z.; Manor, B.; McLean, R.R.; Leveille, S.G. Chronic Pain Characteristics and Gait in Older Adults: The MOBILIZE Boston Study II. Arch. Phys. Med. Rehabil. 2020, 101, 418–425. [Google Scholar] [CrossRef]
- Sawa, R.; Doi, T.; Misu, S.; Saito, T.; Sugimoto, T.; Murata, S.; Asai, T.; Yamada, M.; Ono, R. The severity and number of musculoskeletal pain associated with gait in community-dwelling elderly individuals. Gait Posture 2017, 54, 242–247. [Google Scholar] [CrossRef]
- Farkas, G.J.; Schlink, B.R.; Fogg, L.F.; Foucher, K.C.; Wimmer, M.A.; Shakoor, N. Gait asymmetries in unilateral symptomatic hip osteoarthritis and their association with radiographic severity and pain. Hip Int. 2019, 29, 209–214. [Google Scholar] [CrossRef]
- Nishi, Y.; Shigetoh, H.; Fujii, R.; Osumi, M.; Morioka, S. Changes in Trunk Variability and Stability of Gait in Patients with Chronic Low Back Pain: Impact of Laboratory versus Daily-Living Environments. J. Pain Res. 2021, 14, 1675–1686. [Google Scholar] [CrossRef]
- Misu, S.; Asai, T.; Doi, T.; Sawa, R.; Ueda, Y.; Murata, S.; Saito, T.; Sugimoto, T.; Isa, T.; Tsuboi, Y.; et al. Development and validation of Comprehensive Gait Assessment using InerTial Sensor score (C-GAITS score) derived from acceleration and angular velocity data at heel and lower trunk among community-dwelling older adults. J. Neuroeng. Rehabil. 2019, 16, 62. [Google Scholar] [CrossRef] [Green Version]
- Murata, S.; Doi, T.; Sawa, R.; Nakamura, R.; Isa, T.; Ebina, A.; Kondo, Y.; Tsuboi, Y.; Torizawa, K.; Fukuta, A.; et al. Association Between Objectively Measured Physical Activity and the Number of Chronic Musculoskeletal Pain Sites in Community-Dwelling Older Adults. Pain Med. 2019, 20, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, L.H.P.; Leveille, S.G.; Shi, L.; Kiely, D.K.; Shmerling, R.H.; Jones, R.N.; Guralnik, J.M.; Bean, J.F. Pain characteristics associated with the onset of disability in older adults: The maintenance of balance, independent living, intellect, and zest in the Elderly Boston Study. J. Am. Geriatr. Soc. 2014, 62, 1007–1016. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Kalbe, E.; Calabrese, P.; Schwalen, S.; Kessler, J. The Rapid Dementia Screening Test (RDST): A new economical tool for detecting possible patients with dementia. Dement. Geriatr. Cogn. Disord. 2003, 16, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Pahor, M.; Guralnik, J.M.; Ambrosius, W.T.; Blair, S.; Bonds, D.E.; Church, T.S.; Espeland, M.A.; Fielding, R.A.; Gill, T.M.; Groessl, E.J.; et al. Effect of structured physical activity on prevention of major mobility disability in older adults: The LIFE study randomized clinical trial. JAMA 2014, 311, 2387–2396. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait variability: Methods, modeling and meaning. J. Neuroeng. Rehabil. 2005, 2, 19. [Google Scholar] [CrossRef] [Green Version]
- Moe-Nilssen, R.; Helbostad, J.L. Estimation of gait cycle characteristics by trunk accelerometry. J. Biomech. 2004, 37, 121–126. [Google Scholar] [CrossRef]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait Posture 2003, 18, 35–46. [Google Scholar] [CrossRef]
- Bellanca, J.L.; Lowry, K.A.; Vanswearingen, J.M.; Brach, J.S.; Redfern, M.S. Harmonic ratios: A quantification of step to step symmetry. J. Biomech. 2013, 46, 828–831. [Google Scholar] [CrossRef] [Green Version]
- Boyer, K.A.; Hafer, J.F. Gait mechanics contribute to exercise induced pain flares in knee osteoarthritis. BMC Musculoskelet. Disord. 2019, 20, 107. [Google Scholar] [CrossRef] [Green Version]
- Marriott, K.A.; Birmingham, T.B.; Leitch, K.M.; Pinto, R.; Giffin, J.R. Strong independent associations between gait biomechanics and pain in patients with knee osteoarthritis. J. Biomech. 2019, 94, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Kuwahara, W.; Kurumadani, H.; Tanaka, N.; Nakanishi, K.; Nakamura, H.; Ishii, Y.; Ueda, A.; Deie, M.; Adachi, N.; Sunagawa, T. Correlation between spinal and pelvic movements during gait and aggravation of low back pain by gait loading in lumbar spinal stenosis patients. J. Orthop. Sci. 2019, 24, 207–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novaczyk, Z.B.; Georgiadis, A.G.; Boyer, E.R. Association of back pain and pelvic tilt during gait in individuals with cerebral palsy. Gait Posture 2019, 74, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Tateuchi, H.; Akiyama, H.; Goto, K.; So, K.; Kuroda, Y.; Ichihashi, N. Gait- and Posture-Related Factors Associated with Changes in Hip Pain and Physical Function in Patients with Secondary Hip Osteoarthritis: A Prospective Cohort Study. Arch. Phys. Med. Rehabil. 2019, 100, 2053–2062. [Google Scholar] [CrossRef]
- Wink, A.E.; Gross, K.D.; Brown, C.A.; Lewis, C.E.; Torner, J.; Nevitt, M.C.; Tolstykh, I.; Sharma, L.; Felson, D.T. Association of Varus Knee Thrust during Walking with Worsening Western Ontario and McMaster Universities Osteoarthritis Index Knee Pain: A Prospective Cohort Study. Arthritis Care Res. 2019, 71, 1353–1359. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Did Not Experience an Elevated Degree of Pain after Daily Walking (n = 199, 89.2%) | Experienced An Elevated Degree of Pain after Daily Walking (n = 24, 10.8%) | p-Value | |
|---|---|---|---|---|
| Age | (y) | 74.6 ± 5.4 | 75.8 ± 6.6 | 0.35 |
| Female | (n (%)) | 115 (57.8) | 18 (75.0) | 0.13 |
| Body mass index | (kg/m2) | 23.1 ± 2.8 | 23.8 ± 2.9 | 0.27 |
| Medical history | (n (%)) | |||
| Hypertension 1 | 79 (39.9) | 13 (54.2) | 0.19 | |
| Diabetes 1 | 21 (10.6) | 5 (20.8) | 0.17 | |
| Arteriosclerosis 2 | 1 (0.5) | 0 (0.0) | 1.00 | |
| Stroke 1 | 5 (2.5) | 2 (8.3) | 0.17 | |
| Hip OA 1 | 5 (2.5) | 5 (20.8) | 0.002 | |
| Knee OA 1 | 26 (13.1) | 8 (33.3) | 0.016 | |
| Spinal canal stenosis 1 | 18 (9.1) | 3 (12.5) | 0.48 | |
| Other spinal disease 2 | 18 (9.1) | 5 (20.8) | 0.085 | |
| Any musculoskeletal pain 1 | (n (%)) | 104 (52.5) | 21 (87.5) | <0.001 |
| Lower extremity pain 1 | (n (%)) | 59 (29.8) | 16 (66.7) | <0.001 |
| Low back pain 1 | (n (%)) | 40 (20.2) | 13 (54.2) | <0.001 |
| Variable | Did Not Experience an Elevated Degree of Pain after Daily Walking (n = 199, 89.2%) | Experienced An Elevated Degree of Pain after Daily Walking (n = 24, 10.8%) | p-Value |
|---|---|---|---|
| Total score | 14.4 ± 6.3 | 10.3 ± 6.1 | 0.003 |
| Subscores | |||
| Pace score | 2.8 ± 2.0 | 1.5 ± 1.5 | 0.004 |
| Variability score | 3.2 ± 1.9 | 2.6 ± 2.3 | 0.17 |
| Regularity score | 3.6 ± 2.8 | 2.9 ± 2.9 | 0.21 |
| Smoothness score | 4.8 ± 2.6 | 3.3 ± 2.5 | 0.007 |
| Independent Variable | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | |
| C-GAITS score | ||||||
| Total score | 0.90 | 0.83–0.97 | 0.008 | |||
| Pace score | 0.74 | 0.57–0.97 | 0.032 | |||
| Smoothness score | 0.83 | 0.69–0.99 | 0.045 | |||
| Age | 1.02 | 0.98–1.11 | 0.68 | 1.01 | 0.93–1.10 | 0.76 |
| Sex (female) | 2.12 | 0.79–5.68 | 0.12 | 1.70 | 0.62–4.64 | 0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Misu, S.; Asai, T.; Murata, S.; Nakamura, R.; Isa, T.; Tsuboi, Y.; Oshima, K.; Koyama, S.; Sawa, R.; Fukumoto, Y.; et al. Association between Abnormal Gait Patterns and an Elevated Degree of Pain after Daily Walking: A Preliminary Study. Int. J. Environ. Res. Public Health 2022, 19, 2842. https://doi.org/10.3390/ijerph19052842
Misu S, Asai T, Murata S, Nakamura R, Isa T, Tsuboi Y, Oshima K, Koyama S, Sawa R, Fukumoto Y, et al. Association between Abnormal Gait Patterns and an Elevated Degree of Pain after Daily Walking: A Preliminary Study. International Journal of Environmental Research and Public Health. 2022; 19(5):2842. https://doi.org/10.3390/ijerph19052842
Chicago/Turabian StyleMisu, Shogo, Tsuyoshi Asai, Shunsuke Murata, Ryo Nakamura, Tsunenori Isa, Yamato Tsuboi, Kensuke Oshima, Shota Koyama, Ryuichi Sawa, Yoshihiro Fukumoto, and et al. 2022. "Association between Abnormal Gait Patterns and an Elevated Degree of Pain after Daily Walking: A Preliminary Study" International Journal of Environmental Research and Public Health 19, no. 5: 2842. https://doi.org/10.3390/ijerph19052842