
Emotional Situation of Children and Adolescents during the COVID-19 Pandemic in Germany: Results from the COVID-19 Snapshot Monitoring Study (COSMO)

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Variables and Measures
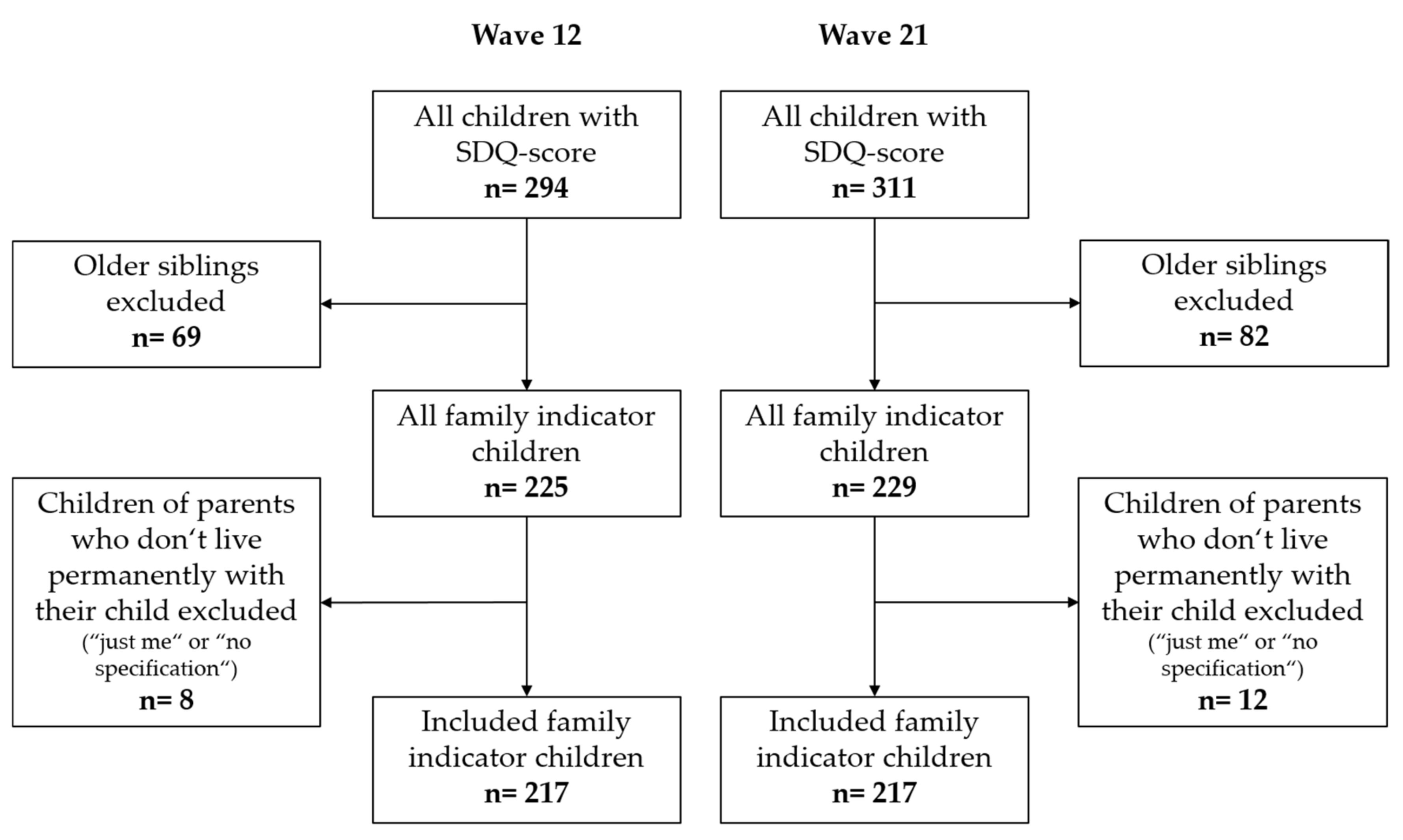
2.2.1. Primary Outcome Variable and Exclusion Criteria
2.2.2. Covariates
2.3. Statistical Analysis
3. Results
3.1. Descriptive Analysis/Sample Overview
3.2. Emotional Symptoms by the Strengths and Difficulties Questionnaire
3.3. Univariate Analysis
3.4. Multivariate Logistic Regression
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Statistical Analysis


{kind=link}
{kind=link}
| Characteristics | OR (Wave 12 vs. Wave 21) Reference Wave 12 | 95% CI |
|---|---|---|
| Total | 1.04 | [0.70–1.56] |
| Children 3–5 years | 0.64 | [0.30–1.38] |
| Children 6–9 years | 1.12 | [0.58–2.16] |
| Children 10–13 years | 0.83 | [0.43–1.58] |
| Children 14–17 years | 1.49 | [0.66–3.36] |
References
- Bundesregierung. Besprechung der Bundeskanzlerin mit den Regierungschefinnen und Regierungschefs der Länder vom 22.03.2020. 2021. Available online: https://www.bundesregierung.de/breg-de/themen/coronavirus/besprechung-der-bundeskanzlerin-mit-den-regierungschefinnen-und-regierungschefs-der-laender-vom-22-03-2020-1733248 (accessed on 29 December 2021).
- Schober, T.; Rack-Hoch, A.; Kern, A.; von Hübner, J.B.U. Coronakrise: Kinder haben das Recht auf Bildung. Dtsch. Aerzteblatt 2020, 117, A-990/B-837. [Google Scholar]
- Kaman, A.; Otto, C.; Adedeji, A.; Devine, J.; Erhart, M.; Napp, A.; Becker, M.; Blanck-Stellmacher, U.; Fertmann, R.; Saier, U.; et al. Belastungserleben und psychische Auffälligkeiten von Kindern und Jugendlichen in Hamburg während der COVID-19-Pandemie. Nervenheilkunde 2021, 40, 319–326. [Google Scholar] [CrossRef]
- Stocker, D.; Schläpfer, D.; Németh, P.; Jäggi, J.; Liechti, L.; Künzi, K. Der Einfluss der COVID-19-Pandemie auf die Psychische Gesundheit der Schweizer Bevölkrung und die Psychiatrisch-Psychotherapeut; Bundesamt für Gesundheit (BAG): Bern, Switzerland, 2020. [Google Scholar]
- Ravens-Sieberer, U.; Kaman, A.; Otto, C.; Adedeji, A.; Devine, J.; Erhart, M.; Napp, A.; Becker, M.; Blanck-Stellmacher, U.; Löffler, C.; et al. Mental Health and Quality of Life in Children and Adolescents During the COVID-19 Pandemic-Results of the Copsy Study. Dtsch. Arztebl. Int. 2020, 117, 828–829. [Google Scholar] [CrossRef]
- DAK-Gesundheit. Homeschooling in Corona-Zeiten. Erfahrungen von Eltern und Schülern. Ergebnisse einer Eltern-Kind-Befragung mit Forsa. Available online: https://www.dak.de/dak/download/forsa-studie-2266768.pdf (accessed on 29 December 2021).
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19: A Meta-analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Fegert, J.M.; Vitiello, B.; Plener, P.L.; Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc. Psychiatry Ment. Health 2020, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Fegert, J.M.; Berthold, O.; Clemens, V.; Kölch, M. COVID-19-Pandemie: Kinderschutz ist systemrelevant. Dtsch. Aerzteblatt 2020, 117, 703–706. [Google Scholar]
- Bundesministerium für Bildung und Forschung-BMBF. Kinder und Jugendliche nach der Corona-Pandemie Stärken. 2021. Available online: https://www.bmbf.de/bmbf/shareddocs/kurzmeldungen/de/kinder-und-jugendliche-nach-der-corona-pandemie-staerken.html (accessed on 29 December 2021).
- Ravens-Sieberer, U.; Kaman, A.; Otto, C.; Adedeji, A.; Napp, A.; Becker, M.; Blanck-Stellmacher, U.; Löffler, C.; Schlack, R.; Hölling, H.; et al. Seelische Gesundheit und psychische Belastungen von Kindern und Jugendlichen in der ersten Welle der COVID-19-Pandemie–Ergebnisse der COPSY-Studie. Bundesgesundheitsblatt Gesundh. Gesundh. 2021, 64, 1512–1521. [Google Scholar] [CrossRef]
- Cornelia, B.; Lothar, W.; Michael, B.; Michael, R.; Volker, S.; Saad, O.; Lars, K.; Philipp, S.; Lisa, F.; Sarah, E.; et al. Germany COVID-19 Snapshot MOnitoring (COSMO Germany): Monitoring knowledge, risk perceptions, preventive behaviours, and public trust in the current coronavirus outbreak in Germany. PsychArchives 2020. [Google Scholar] [CrossRef]
- COSMO. Methode|COSMO. 2021. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/method/ (accessed on 29 December 2021).
- COSMO. Über das Projekt|COSMO. 2021. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/about/ (accessed on 29 December 2021).
- Das Bildungssystem in Zeiten der Krise: Empirische Befunde, Konsequenzen und Potentiale für das Lehren und Lernen; Reintjes, C.; Porsch, R.; Im Brahm, G. (Eds.) Waxmann: Münster, NY, USA, 2021. [Google Scholar]
- Robert Koch-Institut. Deutsches Jugendinstitut. Monatsbericht der Corona-KiTa-Studie; Robert Koch-Institut: Berlin, Germany, 2020. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Hölling, H.; Schlack, R.; Petermann, F.; Ravens-Sieberer, U.; Mauz, E. Psychische Auffälligkeiten und psychosoziale Beeinträchtigungen bei Kindern und Jugendlichen im Alter von 3 bis 17 Jahren in Deutschland-Prävalenz und zeitliche Trends zu 2 Erhebungszeitpunkten (2003–2006 und 2009–2012): Ergebnisse der KiGGS-Studie-Erste Folgebefragung (KiGGS Welle 1). Bundesgesundheitsblatt Gesundh. Gesundh. 2014, 57, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. Psychometric properties of the strengths and difficulties questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Koglin, U.; Barquero, B.; Mayer, H.; Scheithauer, H.; Petermann, F. Deutsche Version des Strengths and Difficulties Questionnaire (SDQ-Deu). Diagnostica 2007, 53, 175–183. [Google Scholar] [CrossRef]
- Youthinmind. 2020. Available online: https://www.sdqinfo.org/py/sdqinfo/b3.py?language=German (accessed on 12 February 2022).
- Klasen, H.; Woerner, W.; Rothenberger, A.; Goodman, R. Die deutsche Fassung des Strengths and Difficulties Questionnaire (SDQ-Deu)—Ubersicht und Bewertung erster Validierungs- und Normierungsbefunde. Prax Kinderpsychol Kinderpsychiatr. 2003, 52, 491–502. [Google Scholar]
- Janitza, S.; Klipker, K.; Hölling, H. Age-specific norms and validation of the German SDQ parent version based on a nationally representative sample (KiGGS). Eur. Child Adolesc. Psychiatry 2020, 29, 123–136. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.; Woerner, W.; Hasselhorn, M.; Banaschewski, T.; Rothenberger, A. Validation of the parent and teacher SDQ in a clinical sample. Eur. Child Adolesc. Psychiatry 2004, 13 (Suppl. 2), II11-6. [Google Scholar] [CrossRef]
- Goodman, R.; Ford, T.; Simmons, H.; Gatward, R.; Meltzer, H. Using the Strengths and Difficulties Questionnaire (SDQ) to screen for child psychiatric disorders in a community sample. Br. J. Psychiatry 2000, 177, 534–539. [Google Scholar] [CrossRef]
- Mathai, J.; Anderson, P.; Bourne, A. The Strengths and Difficulties Questionnaire (SDQ) as a screening measure prior to admission to a Child and Adolescent Mental Health Service (CAMHS). Aust. e-J. Adv. Ment. Health 2002, 1, 235–246. [Google Scholar] [CrossRef]
- Nijenhuis, E.R.S. The Scoring and Interpretation of the SDQ-20 and SDQ-5. Act. Nerv. Super. 2010, 52, 24–28. [Google Scholar] [CrossRef] [Green Version]
- He, J.-P.; Burstein, M.; Schmitz, A.; Merikangas, K.R. The Strengths and Difficulties Questionnaire (SDQ): The factor structure and scale validation in U.S. adolescents. J. Abnorm. Child Psychol. 2013, 41, 583–595. [Google Scholar] [CrossRef]
- Woerner, W.; Becker, A.; Friedrich, C.; Klasen, H.; Goodman, R.; Rothenberger, A. Normierung und Evaluation der deutschen Elternversion des Strengths and Difficulties Questionnaire (SDQ): Ergebnisse einer repräsentativen Felderhebung. Z. Kinder Jugendpsychiatr. Psychother. 2002, 30, 105–112. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: Children’s mental health services in England are “nowhere near sufficient,” says commissioner. BMJ 2021, 372, n258. [Google Scholar] [CrossRef] [PubMed]
- Cost, K.T.; Crosbie, J.; Anagnostou, E.; Birken, C.S.; Charach, A.; Monga, S.; Kelley, E.; Nicolson, R.; Maguire, J.L.; Burton, C.L.; et al. Mostly worse, occasionally better: Impact of COVID-19 pandemic on the mental health of Canadian children and adolescents. Eur. Child Adolesc. Psychiatry 2021. [Google Scholar] [CrossRef] [PubMed]
- Patrick, S.W.; Henkhaus, L.E.; Zickafoose, J.S.; Lovell, K.; Halvorson, A.; Loch, S.; Letterie, M.; Davis, M.M. Well-being of Parents and Children During the COVID-19 Pandemic: A National Survey. Pediatrics 2020, 146, e2020016824. [Google Scholar] [CrossRef]
- Saurabh, K.; Ranjan, S. Compliance and Psychological Impact of Quarantine in Children and Adolescents due to Covid-19 Pandemic. Indian J. Pediatr. 2020, 87, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Xue, Q.; Zhou, Y.; Zhu, K.; Liu, Q.; Zhang, J.; Song, R. Mental Health Status Among Children in Home Confinement During the Coronavirus Disease 2019 Outbreak in Hubei Province, China. JAMA Pediatr. 2020, 174, 898–900. [Google Scholar] [CrossRef] [Green Version]
- Orgilés, M.; Morales, A.; Delvecchio, E.; Mazzeschi, C.; Espada, J.P. Immediate Psychological Effects of the COVID-19 Quarantine in Youth From Italy and Spain. Front. Psychol. 2020, 11, 579038. [Google Scholar] [CrossRef]
- Barkmann, C.; Schulte-Markwort, M. Prevalence of emotional and behavioural disorders in German children and adolescents: A meta-analysis. J. Epidemiol. Community Health 2012, 66, 194–203. [Google Scholar] [CrossRef] [Green Version]
- Klasen, F.; Meyrose, A.-K.; Otto, C.; Reiss, F.; Ravens-Sieberer, U. Psychische Auffälligkeiten von Kindern und Jugendlichen in Deutschland. Mon. Kinderheilkd 2017, 165, 402–407. [Google Scholar] [CrossRef]
- de Quervain, D.; Aerni, A.; Bentz, D.; Amini, E.; Freytag, V.; Coynel, D.; Gerhards, C.; Papassotiropoulos, A.; Schicktanz, N.; Schlitt, T.; et al. The Swiss Corona Stress Study. OSF Preprints 2020. [Google Scholar] [CrossRef]
- Wissmath, B.; Mast, F.W.; Kraus, F.; Weibel, D. Understanding the psychological impact of the COVID-19 pandemic and containment measures: An empirical model of stress. PLoS ONE 2021. [Google Scholar] [CrossRef]

| Sociodemographic Characteristics | Wave 12 (19th/20th May 2020) | Wave 21 (15th/16th September 2020) | ||||||
|---|---|---|---|---|---|---|---|---|
| Total n = 972 | Parents of children 3–17 Years n = 225 | Total n = 1013 | Parents of children 3–17 Years n = 229 | |||||
| N | % | n | % | N | % | n | % | |
| Total | 972 | 100 | 225 | 100 | 1013 | 100 | 229 | 100 |
| Gender of answering parent | ||||||||
| Male | 477 | 49.1 | 109 | 48.4 | 506 | 50.0 | 109 | 47.6 |
| Female | 495 | 50.9 | 116 | 51.6 | 507 | 50.0 | 120 | 52.4 |
| Age of answering parent | ||||||||
| 18–29 | 188 | 19.3 | 27 | 12.0 | 191 | 18.9 | 18 | 7.9 |
| 30–44 | 310 | 31.9 | 118 | 52.4 | 304 | 30.0 | 138 | 60.3 |
| 45–64 | 354 | 36.4 | 77 | 34.2 | 366 | 36.1 | 71 | 31.0 |
| ≥65 | 120 | 12.3 | 3 | 1.3 | 152 | 15.0 | 2 | 0.9 |
| Number of inhabitants of answering parent’s place of residence | ||||||||
| ≤5000 | 148 | 15.2 | 33 | 14.7 | 168 | 16.6 | 42 | 18.3 |
| 5001–20,000 | 211 | 21.7 | 53 | 23.6 | 203 | 20.0 | 49 | 21.4 |
| 20,001–100,000 | 241 | 24.8 | 53 | 23.6 | 267 | 26.4 | 62 | 27.1 |
| 100,001–500,000 | 183 | 18.8 | 39 | 17.3 | 190 | 18.8 | 38 | 16.6 |
| >500,000 | 189 | 19.4 | 47 | 20.9 | 185 | 18.3 | 38 | 16.6 |
| Local region of answering parent’s place of residence | ||||||||
| East | 199 | 20.5 | 51 | 22.7 | 207 | 20.4 | 48 | 21.0 |
| West | 773 | 79.5 | 174 | 77.3 | 806 | 79.6 | 181 | 79.0 |
| Education of answering parent | ||||||||
| ≤9 years | 105 | 10.8 | 13 | 5.8 | 121 | 11.9 | 21 | 9.2 |
| ≥10 years (no A-Level) | 334 | 34.4 | 88 | 39.1 | 357 | 35.2 | 81 | 35.4 |
| ≥10 years (A-Level) | 533 | 54.8 | 124 | 55.1 | 535 | 52.8 | 127 | 55.5 |
| Self-employed status of answering parent | ||||||||
| Yes | 100 | 10.3 | 27 | 12.0 | 77 | 7.6 | 19 | 8.3 |
| No | 872 | 89.7 | 198 | 88.0 | 936 | 92.4 | 210 | 91.7 |
| Health professional occupation of answering parent | ||||||||
| Yes | 96 | 9.9 | 34 | 15.1 | 66 | 6.5 | 20 | 8.7 |
| No | 876 | 90.1 | 191 | 84.9 | 947 | 93.5 | 209 | 91.3 |
| Relationship/marriage of answering parent | ||||||||
| Yes | 621 | 63.9 | 193 | 85.8 | 639 | 63.1 | 191 | 83.4 |
| No | 351 | 36.1 | 32 | 14.2 | 374 | 36.9 | 38 | 16.6 |
| Household language other than German | ||||||||
| Yes | 244 | 25.1 | 64 | 28.4 | 257 | 25.4 | 66 | 28.8 |
| No | 728 | 74.9 | 161 | 71.6 | 756 | 74.6 | 163 | 71.2 |
| Household size of answering parent | ||||||||
| Just me | 284 | 29.2 | 7 | 3.1 | 294 | 29.0 | 12 | 5.2 |
| 2 persons | 351 | 36.1 | 20 | 8.9 | 369 | 36.4 | 22 | 9.6 |
| 3–4 persons | 276 | 28.4 | 162 | 72.0 | 297 | 29.3 | 156 | 68.1 |
| >4 persons | 59 | 6.1 | 35 | 15.6 | 51 | 5.0 | 39 | 17.0 |
| No specification | 2 | 0.2 | 1 | 0.4 | 2 | 0.2 | 0 | 0.0 |
| Age of all children of parents | ||||||||
| Total | x | x | 294 | x | x | X | 311 | x |
| 3–5 | x | x | 64 | x | x | X | 55 | x |
| 6–9 | x | x | 77 | x | x | X | 87 | x |
| 10–13 | x | x | 72 | x | x | X | 107 | x |
| 14–17 | x | x | 81 | x | x | X | 62 | x |
| Single-parent status | ||||||||
| Yes | x | x | 35 | 15.6 | x | X | 40 | 17.5 |
| No | x | x | 190 | 84.4 | x | X | 189 | 82.5 |
| Chronic disease of answering parent | ||||||||
| Yes | 347 | 35.7 | 65 | 28.9 | 347 | 34.3 | 68 | 29.7 |
| No | 600 | 61.7 | 156 | 69.3 | 643 | 63.5 | 156 | 68.1 |
| Don’t know | 25 | 2.6 | 4 | 1.8 | 23 | 2.3 | 5 | 2.2 |
| All children with SDQ subscale Emotional Symptoms Ratings | 294 | 311 | ||||||
| Not at risk | x | x | 202 | x | x | X | 218 | x |
| Family indicator children at risk by SDQ subscale Emotional Symptoms (at risk/not at risk) (rated by 217 parents per wave) ** | 217 | 217 | ||||||
| Not at risk | x | x | 147 *** | x | x | X | 145 *** | X |
| At risk | x | x | 70 *** | x | x | X | 72 *** | X |
| Characteristics | Wave 12—19th/20th May 2020 (Parents with Family Indicator Children at Risk for Emotional Symptoms n = 70 vs. Parents without Family Indicator Children at Risk n = 147) | Wave 21—15th/16th September 2020 (Parents with Family Indicator Children at Risk for Emotional Symptoms n = 72 vs. Parents without Family Indicator Children at Risk n = 145) | ||||||
|---|---|---|---|---|---|---|---|---|
| n | % | OR | 95% CI | n | % | OR | 95% CI | |
| Gender of answering parent | ||||||||
| Male (reference) | 36 | 51.4 | 29 | 40.3 | ||||
| Female | 34 | 48.6 | 0.79 | [0.45–1.40] | 43 | 59.7 | 1.35 | [0.76–2.39] |
| Age of answering parent | ||||||||
| 18–29 (reference) | 15 | 21.4 | 4 | 5.6 | ||||
| 30–44 | 40 | 57.1 | 0.43 | [0.18–1.01] | 41 | 56.9 | 1.45 | [0.45–4.71] |
| 45–64 | 15 | 21.4 | 0.21 | [0.08–0.53] | 27 | 37.5 | 2.31 | [0.68–7.86] |
| Number of inhabitants of answering parent’s place of residence | ||||||||
| ≤5000 (reference) | 8 | 11.4 | 14 | 19.4 | ||||
| 5001–20,000 | 15 | 21.4 | 1.29 | [0.47–3.51] | 13 | 18.1 | 0.66 | [0.27–1.65] |
| 20,001–100,000 | 19 | 27.1 | 1.78 | [0.67–4.75] | 20 | 27.8 | 0.97 | [0.41–2.26] |
| 100,001–500,000 | 12 | 17.1 | 1.38 | [0.48–3.97] | 12 | 16.7 | 0.86 | [0.33–2.22] |
| >500,000 | 16 | 22.9 | 1.60 | [0.59–4.37] | 13 | 18.1 | 1.01 | [0.39–2.59] |
| Local region of answering parent’s place of residence | ||||||||
| East (reference) | 16 | 22.9 | 13 | 18.1 | ||||
| West | 54 | 77.1 | 0.94 | [0.47–1.86] | 59 | 81.9 | 1.13 | [0.55–2.34] |
| Education of answering parent | ||||||||
| No A-Level (reference) | 27 | 38.6 | 32 | 44.4 | ||||
| A-Level | 43 | 61.4 | 1.41 | [0.79–2.52] | 40 | 55.6 | 1.04 | [0.59–1.84] |
| Self-employed status of answering parent | ||||||||
| No (reference) | 60 | 85.7 | 68 | 94.4 | ||||
| Yes | 10 | 14.3 | 1.27 | [0.55–2.95] | 4 | 5.6 | 0.65 | [0.20–2.10] |
| Health professional occupation of answering parent | ||||||||
| No (reference) | 56 | 80.0 | 65 | 90.3 | ||||
| Yes | 14 | 20.0 | 1.79 | [0.83–3.85] | 7 | 9.7 | 1.19 | [0.45–3.17] |
| Relationship/marriage of answering parent | ||||||||
| No (reference) | 12 | 17.1 | 11 | 15.3 | ||||
| Yes | 58 | 82.9 | 0.51 | [0.22–1.17] | 61 | 84.7 | 0.74 | [0.33–1.67] |
| Household language other than German | ||||||||
| No (reference) | 42 | 60.0 | 50 | 69.4 | ||||
| Yes | 28 | 40.0 | 2.22 | [1.20–4.09] | 22 | 30.6 | 1.12 | [0.60–2.07] |
| Household size of answering parent | ||||||||
| 2 persons (reference) | 9 | 12.9 | 12 | 16.7 | ||||
| 3–4 persons | 49 | 70.0 | 0.53 | [0.21–1.36] | 48 | 66.7 | 0.37 | [0.15–0.92] |
| >4 persons | 12 | 17.1 | 0.64 | [0.21–1.96] | 12 | 16.7 | 0.37 | [0.13–1.09] |
| Age of Family Indicator Children | ||||||||
| 3–5 (reference) | 25 | 35.7 | 16 | 22.2 | ||||
| 6–9 | 19 | 27.1 | 0.74 | [0.35–1.56] | 26 | 36.1 | 1.47 | [0.69–3.15] |
| 10–13 | 16 | 22.9 | 0.97 | [0.43–2.18] | 21 | 29.2 | 1.19 | [0.54–2.60] |
| 14–17 | 10 | 14.3 | 0.34 | [0.14–0.79] | 9 | 12.5 | 0.93 | [0.35–2.44] |
| Single-parent status | ||||||||
| No (reference) | 56 | 80.0 | 59 | 81.9 | ||||
| Yes | 14 | 20.0 | 1.50 | [0.71–3.16] | 13 | 18.1 | 1.01 | [0.48–2.10] |
| Chronic disease of answering parent | ||||||||
| No/don’t know (reference) | 48 | 68.6 | 51 | 70.8 | ||||
| Yes | 22 | 31.4 | 1.18 | [0.64–2.20] | 21 | 29.2 | 1.04 | [0.56–1.95] |
| Characteristics | Wave 12—19th/20th May 2020 (Parents with Family Indicator Children at Risk for Emotional Symptoms n = 70 vs. Parents with Family Indicator Children Not at Risk n = 147) | Wave 21—15th/16th September 2020 (Parents with Family Indicator Children at Risk for Emotional Symptoms n = 72 vs. Parents with Family Indicator Children Not at Risk n = 145) | ||||||
|---|---|---|---|---|---|---|---|---|
| % | OR | 95% CI | SE | % | OR | 95% CI | SE | |
| Gender of answering parent | ||||||||
| Male (reference) | 51.4 | 40.3 | ||||||
| Female | 48.6 | 0.76 | [0.41–1.38] | 0.31 | 59.7 | 1.43 | [0.79–2.60] | 0.30 |
| Age of answering parent | ||||||||
| 18–29 (reference) | 21.4 | 5.6 | ||||||
| 30–44 | 57.1 | 0.52 | [0.21–1.27] | 0.46 | 56.9 | 1.36 | [0.41–4.46] | 0.61 |
| 45–64 | 21.4 | 0.23 | [0.09–0.62] | 0.50 | 37.5 | 2.31 | [0.67–7.95] | 0.63 |
| Education of answering parent | ||||||||
| No A-Level (reference) | 38.6 | 44.4 | ||||||
| A-Level | 61.4 | 1.51 | [0.82–2.80] | 0.31 | 55.6 | 1.16 | [0.64–2.09] | 0.30 |
| Household language other than German | ||||||||
| No (reference) | 60.0 | 69.4 | ||||||
| Yes | 40.0 | 2.03 | [1.06–3.91] | 0.33 | 30.6 | 1.12 | [0.60–2.10] | 0.32 |
| Pseudo-R² | 0.1288 | 0.0398 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rathgeb, C.; Schillok, H.; Voss, S.; Coenen, M.; Schulte-Körne, G.; Merkel, C.; Eitze, S.; Jung-Sievers, C.; on behalf of the COSMO Study Team. Emotional Situation of Children and Adolescents during the COVID-19 Pandemic in Germany: Results from the COVID-19 Snapshot Monitoring Study (COSMO). Int. J. Environ. Res. Public Health 2022, 19, 2698. https://doi.org/10.3390/ijerph19052698
Rathgeb C, Schillok H, Voss S, Coenen M, Schulte-Körne G, Merkel C, Eitze S, Jung-Sievers C, on behalf of the COSMO Study Team. Emotional Situation of Children and Adolescents during the COVID-19 Pandemic in Germany: Results from the COVID-19 Snapshot Monitoring Study (COSMO). International Journal of Environmental Research and Public Health. 2022; 19(5):2698. https://doi.org/10.3390/ijerph19052698
Chicago/Turabian StyleRathgeb, Chiara, Hannah Schillok, Stephan Voss, Michaela Coenen, Gerd Schulte-Körne, Christina Merkel, Sarah Eitze, Caroline Jung-Sievers, and on behalf of the COSMO Study Team. 2022. "Emotional Situation of Children and Adolescents during the COVID-19 Pandemic in Germany: Results from the COVID-19 Snapshot Monitoring Study (COSMO)" International Journal of Environmental Research and Public Health 19, no. 5: 2698. https://doi.org/10.3390/ijerph19052698