
Pain Neuroscience Education and Motor Control Exercises versus Core Stability Exercises on Pain, Disability, and Balance in Women with Chronic Low Back Pain


 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Interventions
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CST | core stability training |
| CLBP | chronic low back pain |
| PNE/MCE | pain neuroscience education/motor control exercise |
| LBP | low back pain |
| GE | group-based exercise |
| VAS | Visual Analog Scale |
| RMDQ | Roland–Morris Disability Questionnaire |
| TUG | Timed Up and Go |
References
- Nijs, J.; Clark, J.; Malfliet, A.; Ickmans, K.; Voogt, L.; Don, S.; den Bandt, H.; Goubert, D.; Kregel, J.; Coppieters, I. In the spine or in the brain? Recent advances in pain neuroscience applied in the intervention for low back pain. Clin. Exp. Rheumatol. 2017, 35, S108–S115. [Google Scholar]
- Oh, Y.-J.; Park, S.-H.; Lee, M.-M. Comparison of effects of abdominal draw-in lumbar stabilization exercises with and without respiratory resistance on women with low back pain: A randomized controlled trial. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e921295. [Google Scholar] [CrossRef]
- Da Silva, R.A.; Vieira, E.R.; Fernandes, K.B.; Andraus, R.A.; Oliveira, M.R.; Sturion, L.A.; Calderon, M.G. People with chronic low back pain have poorer balance than controls in challenging tasks. Disabil. Rehabil. 2018, 40, 1294–1300. [Google Scholar] [CrossRef] [PubMed]
- Berenshteyn, Y.; Gibson, K.; Hackett, G.C.; Trem, A.B.; Wilhelm, M. Is standing balance altered in individuals with chronic low back pain? A systematic review. Disabil. Rehabil. 2019, 41, 1514–1523. [Google Scholar] [CrossRef] [PubMed]
- Koch, C.; Hänsel, F. Chronic non-specific low back pain and motor control during gait. Front. Psychol. 2018, 9, 2236. [Google Scholar] [CrossRef] [PubMed]
- Mu, J.; Furlan, A.D.; Lam, W.Y.; Hsu, M.Y.; Ning, Z.; Lao, L. Acupuncture for chronic nonspecific low back pain. Cochrane Database Syst. Rev. 2020, 2020, CD013814. [Google Scholar]
- Sonmezer, E.; Özköslü, M.A.; Yosmaoğlu, H.B. The effects of clinical pilates exercises on functional disability, pain, quality of life and lumbopelvic stabilization in pregnant women with low back pain: A randomized controlled study. J. Back Musculoskelet. Rehabil. 2021, 34, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Ghavipanje, V.; Rahimi, N.M.; Akhlaghi, F. Six Weeks Effects of Dynamic Neuromuscular Stabilization (DNS) Training in Obese Postpartum Women with Low Back Pain: A Randomized Controlled Trial. Biol. Res. Nurs. 2022, 24, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; Ferreira, P.H.; Fritz, J.M.; Koes, B.W.; Peul, W. Prevention and treatment of low back pain: Evidence, challenges, and promising directions. Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef]
- Qaseem, A.; Wilt, T.J.; McLean, R.M.; Forciea, M.A.; for the Clinical Guidelines Committee of the American College of Physicians *. Noninvasive treatments for acute, subacute, and chronic low back pain: A clinical practice guideline from the American College of Physicians. Ann. Intern. Med. 2017, 166, 514–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuge, B. Evidence of stabilizing exercises for low back-and pelvic girdle pain–A critical review. Braz. J. Phys. Ther. 2019, 23, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Kliziene, I.; Sipaviciene, S.; Klizas, S.; Imbrasiene, D. Effects of core stability exercises on multifidus muscles in healthy women and women with chronic low-back pain. J. Back Musculoskelet. Rehabil. 2015, 28, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.O.; Maher, C.G.; Latimer, J.; Hodges, P.W.; Herbert, R.D.; Refshauge, K.M.; McAuley, J.H.; Jennings, M.D. Motor control exercise for chronic low back pain: A randomized placebo-controlled trial. Phys. Ther. 2009, 89, 1275–1286. [Google Scholar] [CrossRef] [PubMed]
- Hides, J.; Stanton, W.; McMahon, S.; Sims, K.; Richardson, C. Effect of stabilization training on multifidus muscle cross-sectional area among young elite cricketers with low back pain. J. Orthop. Sports Phys. Ther. 2008, 38, 101–108. [Google Scholar] [CrossRef]
- França, F.R.; Burke, T.N.; Hanada, E.S.; Marques, A.P. Segmental stabilization and muscular strengthening in chronic low back pain: A comparative study. Clinics 2010, 65, 1013–1017. [Google Scholar] [CrossRef] [Green Version]
- D’hooge, R.; Hodges, P.; Tsao, H.; Hall, L.; MacDonald, D.; Danneels, L. Altered trunk muscle coordination during rapid trunk flexion in people in remission of recurrent low back pain. J. Electromyogr. Kinesiol. 2013, 23, 173–181. [Google Scholar] [CrossRef]
- Roussel, N.; De Kooning, M.; Schutt, A.; Mottram, S.; Truijen, S.; Nijs, J.; Daenen, L. Motor control and low back pain in dancers. Int. J. Sports Med. 2013, 34, 138–143. [Google Scholar] [CrossRef] [Green Version]
- Radebold, A.; Cholewicki, J.; Polzhofer, G.K.; Greene, H.S. Impaired postural control of the lumbar spine is associated with delayed muscle response times in patients with chronic idiopathic low back pain. Spine 2001, 26, 724–730. [Google Scholar] [CrossRef]
- Louw, A.; Zimney, K.; Puentedura, E.J.; Diener, I. The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiother. Theory Pract. 2016, 32, 332–355. [Google Scholar] [CrossRef]
- Pardo, G.B.; Girbés, E.L.; Roussel, N.A.; Izquierdo, T.G.; Penick, V.J.; Martín, D.P. Pain neurophysiology education and therapeutic exercise for patients with chronic low back pain: A single-blind randomized controlled trial. Arch. Phys. Med. Rehabil. 2018, 99, 338–347. [Google Scholar] [CrossRef]
- Rabiei, P.; Sheikhi, B.; Letafatkar, A. Comparing Pain Neuroscience Education Followed by Motor Control Exercises with Group-Based Exercises for Chronic Low Back Pain: A Randomized Controlled Trial. Pain Pract. 2021, 21, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Malfliet, A.; Kregel, J.; Coppieters, I.; De Pauw, R.; Meeus, M.; Roussel, N.; Cagnie, B.; Danneels, L.; Nijs, J. Effect of pain neuroscience education combined with cognition-targeted motor control training on chronic spinal pain: A randomized clinical trial. JAMA Neurol. 2018, 75, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L. Joining forces–combining cognition-targeted motor control training with group or individual pain physiology education: A successful treatment for chronic low back pain. J. Man. Manip. Ther. 2003, 11, 88–94. [Google Scholar] [CrossRef]
- Nijs, J.; Meeus, M.; Cagnie, B.; Roussel, N.A.; Dolphens, M.; Van Oosterwijck, J.; Danneels, L. A modern neuroscience approach to chronic spinal pain: Combining pain neuroscience education with cognition-targeted motor control training. Phys. Ther. 2014, 94, 730–738. [Google Scholar] [CrossRef] [Green Version]
- O’Keeffe, M.; Hayes, A.; McCreesh, K.; Purtill, H.; O’Sullivan, K. Are group-based and individual physiotherapy exercise programmes equally effective for musculoskeletal conditions? A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 126–132. [Google Scholar] [CrossRef]
- Hayden, J.A.; Van Tulder, M.W.; Tomlinson, G. Systematic review: Strategies for using exercise therapy to improve outcomes in chronic low back pain. Ann. Intern. Med. 2005, 142, 776–785. [Google Scholar] [CrossRef]
- Ferreira, P.H.; Ferreira, M.L.; Maher, C.G.; Herbert, R.D.; Refshauge, K. Specific stabilisation exercise for spinal and pelvic pain: A systematic review. Aust. J. Physiother. 2006, 52, 79–88. [Google Scholar] [CrossRef] [Green Version]
- Macedo, L.G.; Smeets, R.J.; Maher, C.G.; Latimer, J.; McAuley, J.H. Graded activity and graded exposure for persistent nonspecific low back pain: A systematic review. Phys. Ther. 2010, 90, 860–879. [Google Scholar] [CrossRef]
- Saragiotto, B.T.; Maher, C.G.; Yamato, T.P.; Costa, L.O.; Costa, L.C.M.; Ostelo, R.W.; Macedo, L.G. Motor control exercise for chronic non-specific low-back pain. Cochrane Database Syst. Rev. 2016, 1, CD012004. [Google Scholar] [CrossRef]
- Shiri, R.; Coggon, D.; Falah-Hassani, K. Exercise for the prevention of low back and pelvic girdle pain in pregnancy: A meta-analysis of randomized controlled trials. Eur. J. Pain 2018, 22, 19–27. [Google Scholar] [CrossRef]
- Wang, X.-Q.; Zheng, J.-J.; Yu, Z.-W.; Bi, X.; Lou, S.-J.; Liu, J.; Cai, B.; Hua, Y.-H.; Wu, M.; Wei, M.-L. A meta-analysis of core stability exercise versus general exercise for chronic low back pain. PLoS ONE 2012, 7, e52082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scrimshaw, S.V.; Maher, C. Responsiveness of visual analogue and McGill pain scale measures. J. Manip. Physiol. Ther. 2001, 24, 501–504. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.J.; Parnianpour, M.; Mehdian, H.; Montazeri, A.; Mobini, B. The Oswestry disability index, the Roland-Morris disability questionnaire, and the Quebec back pain disability scale: Translation and validation studies of the Iranian versions. Spine 2006, 31, E454–E459. [Google Scholar] [CrossRef] [PubMed]
- Agten, A.; Verbrugghe, J.; Stevens, S.; Eijnde, B.O.; Timmermans, A.; Vandenabeele, F. High Intensity Training Increases Muscle Area Occupied by Type II Muscle Fibers of the Multifidus Muscle in Persons with Non-Specific Chronic Low Back Pain: A Pilot Trial. Appl. Sci. 2021, 11, 3306. [Google Scholar] [CrossRef]
- Kerzman, H.; Chetrit, A.; Brin, L.; Toren, O. Characteristics of falls in hospitalized patients. J. Adv. Nurs. 2004, 47, 223–229. [Google Scholar] [CrossRef]
- Gheitasi, M.; Khaledi, A.; Daneshjoo, A. The effect of combined core stability and sensory-motor exercises on Pain, Performance and movement fear in retired male athletes with non-specific chronic low back pain. Anesthesiol. Pain 2020, 11, 38–48. [Google Scholar]
- Dolphens, M.; Nijs, J.; Cagnie, B.; Meeus, M.; Roussel, N.; Kregel, J.; Malfliet, A.; Vanderstraeten, G.; Danneels, L. Efficacy of a modern neuroscience approach versus usual care evidence-based physiotherapy on pain, disability and brain characteristics in chronic spinal pain patients: Protocol of a randomized clinical trial. BMC Musculoskelet. Disord. 2014, 15, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Sahrmann, S.A. Does postural assessment contribute to patient care? J. Orthop. Sports Phys. Ther. 2002, 32, 376–379. [Google Scholar] [CrossRef] [Green Version]
- Comerford, M.J.; Mottram, S.L. Functional stability re-training: Principles and strategies for managing mechanical dysfunction. Man. Ther. 2001, 6, 3–14. [Google Scholar] [CrossRef]
- Richardson, C.; Jull, G. Muscle control–pain control. What exercises would you prescribe? Man. Ther. 1995, 1, 2–10. [Google Scholar] [CrossRef]
- Keselman, H.J.; Huberty, C.J.; Lix, L.M.; Olejnik, S.; Cribbie, R.A.; Donahue, B.; Kowalchuk, R.K.; Lowman, L.L.; Petoskey, M.D.; Keselman, J.C. Statistical practices of educational researchers: An analysis of their ANOVA, MANOVA, and ANCOVA analyses. Rev. Educ. Res. 1998, 68, 350–386. [Google Scholar] [CrossRef]
- Saragiotto, B.T.; Maher, C.G.; Yamato, T.P.; Costa, L.O.; Costa, L.C.M.; Ostelo, R.W.; Macedo, L.G. Motor control exercise for nonspecific low back pain: A cochrane review. Spine 2016, 41, 1284–1295. [Google Scholar] [CrossRef] [PubMed]
- Hodges, P.; van den Hoorn, W.; Dawson, A.; Cholewicki, J. Changes in the mechanical properties of the trunk in low back pain may be associated with recurrence. J. Biomech. 2009, 42, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Omkar, S.; Vishwas, S. Yoga techniques as a means of core stability training. J. Bodyw. Mov. Ther. 2009, 13, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Cabanas-Valdés, R.; Bagur-Calafat, C.; Girabent-Farrés, M.; Caballero-Gómez, F.M.; Hernández-Valiño, M.; Urrutia Cuchi, G. The effect of additional core stability exercises on improving dynamic sitting balance and trunk control for subacute stroke patients: A randomized controlled trial. Clin. Rehabil. 2016, 30, 1024–1033. [Google Scholar] [CrossRef] [PubMed]
- Jeffreys, I. Developing a progressive core stability program. Strength Cond. J. 2002, 24, 65–66. [Google Scholar] [CrossRef]
- Demoulin, C.; Crielaard, J.-M.; Vanderthommen, M. Spinal muscle evaluation in healthy individuals and low-back-pain patients: A literature review. Jt. Bone Spine 2007, 74, 9–13. [Google Scholar] [CrossRef]
- Ong, A.; Anderson, J.; Roche, J. A pilot study of the prevalence of lumbar disc degeneration in elite athletes with lower back pain at the Sydney 2000 Olympic Games. Br. J. Sports Med. 2003, 37, 263–266. [Google Scholar] [CrossRef] [Green Version]
- Sandrey, M.A.; Mitzel, J.G. Improvement in dynamic balance and core endurance after a 6-week core-stability-training program in high school track and field athletes. J. Sport Rehabil. 2013, 22, 264–271. [Google Scholar] [CrossRef]
- Hooper, T. The Effect of Low Back Pain Status and a Volitional Preemptive Abdominal Contraction on Dynamic Balance Test Performance in People Iwth Low Back Pain. Doctoral Dissertation, Texas Tech University, Lubbock, TX, USA, 2015. [Google Scholar]
- Djordjevic, O.; Konstantinovic, L.; Miljkovic, N.; Bijelic, G. Relationship between electromyographic signal amplitude and thickness change of the trunk muscles in patients with and without low back pain. Clin. J. Pain 2015, 31, 893–902. [Google Scholar] [CrossRef]
- Hooper, T.L.; James, C.R.; Brismée, J.-M.; Rogers, T.J.; Gilbert, K.K.; Browne, K.L.; Sizer, P.S. Dynamic balance as measured by the Y-Balance Test is reduced in individuals with low back pain: A cross-sectional comparative study. Phys. Ther. Sport 2016, 22, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Kim, C.W.; Kim, Y.I.; Kim, K.B.; Lee, S.S.; Shin, K.O. Alterations of muscular strength and left and right limb balance in weightlifters after an 8-week balance training program. J. Phys. Ther. Sci. 2013, 25, 895–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emami, F.; Yoosefinejad, A.K.; Razeghi, M. Correlations between core muscle geometry, pain intensity, functional disability and postural balance in patients with nonspecific mechanical low back pain. Med. Eng. Phys. 2018, 60, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Anderson, K.; Curnew, R.S. Muscle force and activation under stable and unstable conditions. J. Strength Cond. Res. 2002, 16, 416–422. [Google Scholar]
- Hwangbo, G.; Lee, C.-W.; Kim, S.-G.; Kim, H.-S. The effects of trunk stability exercise and a combined exercise program on pain, flexibility, and static balance in chronic low back pain patients. J. Phys. Ther. Sci. 2015, 27, 1153–1155. [Google Scholar] [CrossRef] [Green Version]
- Gardner, T.; Refshauge, K.; McAuley, J.; Hübscher, M.; Goodall, S.; Smith, L. Combined education and patient-led goal setting intervention reduced chronic low back pain disability and intensity at 12 months: A randomised controlled trial. Br. J. Sports Med. 2019, 53, 1424–1431. [Google Scholar] [CrossRef]
- Waseem, M.; Karimi, H.; Gilani, S.A.; Hassan, D. Treatment of disability associated with chronic non-specific low back pain using core stabilization exercises in Pakistani population. J. Back Musculoskelet. Rehabil. 2019, 32, 149–154. [Google Scholar] [CrossRef]
- Macedo, L.G.; Latimer, J.; Maher, C.G.; Hodges, P.W.; McAuley, J.H.; Nicholas, M.K.; Tonkin, L.; Stanton, C.J.; Stanton, T.R.; Stafford, R. Effect of motor control exercises versus graded activity in patients with chronic nonspecific low back pain: A randomized controlled trial. Phys. Ther. 2012, 92, 363–377. [Google Scholar] [CrossRef] [Green Version]
- Thiamwong, L.; Stout, J.R.; Sole, M.L.; Ng, B.P.; Yan, X.; Talbert, S. Physio-Feedback and Exercise Program (PEER) improves balance, muscle strength, and fall risk in older adults. Res. Gerontol. Nurs. 2020, 13, 289–296. [Google Scholar] [CrossRef]
- Fletcher, C.; Bradnam, L.; Barr, C. The relationship between knowledge of pain neurophysiology and fear avoidance in people with chronic pain: A point in time, observational study. Physiother. Theory Pract. 2016, 32, 271–276. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercise | Sets and Repetitions per Week | |||||||
|---|---|---|---|---|---|---|---|---|
| 1–2 Weeks | 3–4 Weeks | 5–6 Weeks | 7–8 Weeks | |||||
| Set | R/S | Set | R/S | Set | R/S | Set | R/S | |
| Stomach abduction (static contraction of the abdominal muscles) (S) | 3 | 20 | 3 | 25 | 4 | 30 | 5 | 30 |
| Four-legged position with raising the opposite arm and leg (R) | 3 | 20 | 3 | 25 | 4 | 30 | 5 | 30 |
| Single leg adjusted side bridge for each side of the body (R) | 3 | 10 | 3 | 15 | 4 | 15 | 5 | 15 |
| Supine on a Swiss ball with static contraction of the abdominal muscles (S) | 3 | 10 | 3 | 15 | 4 | 15 | 5 | 15 |
| Raise the opposite arm and leg on the Swiss ball (R) | 3 | 10 | 3 | 15 | 4 | 15 | 5 | 15 |
| Standing on one leg with the knee flexed (S) | 3 | 10 | 3 | 15 | 4 | 15 | 5 | 15 |
| Standing on two legs with balance sandals in an anatomical position or with eyes closed (S) | 3 | 8 | 3 | 12 | 4 | 15 | 5 | 15 |
| Standing with feet on the wobble board (S) | 3 | 8 | 3 | 12 | 4 | 15 | 5 | 15 |
| Standing and walking with balance sandals on two legs | 3 | 8 | 3 | 12 | 4 | 15 | 5 | 15 |
| Stride using balance sandals | 3 | 8 | 3 | 12 | 4 | 15 | 5 | 15 |
| Standing and walking with balance sandals and with the knee flexed at feet | 3 | 8 | 3 | 12 | 4 | 15 | 5 | 15 |
| Phase | Weeks | Set | R/S | Exercises |
|---|---|---|---|---|
| A | 1–2 Weeks | 3 | 10 | Pelvic tilt, double leg stance, bridge, cat and cow exercise |
| 3–4 Weeks | 3 | 10 | Single leg stance, single leg bridge, cobra with hands off floor, quadruped trunk rotation | |
| B | 5–6 Weeks | 4 | 15 | Single leg stance eyes closed, flexion and extension of the back without weights, straight leg raise, walking on stable board |
| 7–8 Weeks | 5 | 15 | Forward bending, flexion and extension of the back with weights on unstable board, walking on unstable board, cross straight leg raise, eccentric squat |
| Characteristic | PNE/MCE (n = 18) | CST (n = 19) | p-Value |
|---|---|---|---|
| Age (years) | 55.16 ± 2.61 | 54.63 ± 2.38 | 0.52 |
| Body weight (kg) | 1.63 ± 0.06 | 63.36 ± 4.75 | 0.55 |
| Body height (m) | 63.72 ± 5.47 | 1.65 ± 0.04 | 0.83 |
| Body Mass Index (kg/m2) | 23.56 ± 1.61 | 23.08 ± 0.89 | 0.47 |
| Low back pain duration, months | 4.00 ± 076 | 3.89 ± 0.73 | 0.67 |
| Dependent Variables | Group | Baseline Mean ± SD | Post 8 Weeks Mean ± SD | Δ Pre–Post | Main Effect: Time | Main Effect: Group | Interaction: Time × Group | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p | ηp2 | F | p | ηp2 | F | p | ηp2 | |||||
| VAS (au) | PNE/MCE | 5.16 ± 0.70 | 2.16 ± 0.072 | ↓58% | 563.34 | <0.001 * | 0.971 | 6.16 | 0.024 * | 0.266 | 4.21 | 0.05 * | 0.198 |
| CST | 5.10 ± 0.80 | 2.94 ± 0.91 | ↓42% | ||||||||||
| RMDQ (au) | PNE/MCE | 14.38 ± 1.94 | 6.61 ± 0.92 | ↓54% | 567.06 | <0.001 * | 0.971 | 3.45 | 0.08 | 0.169 | 13.69 | 0.002 * | 0.446 |
| CST | 14.57 ± 2.77 | 9.05 ± 3.55 | ↓37% | ||||||||||
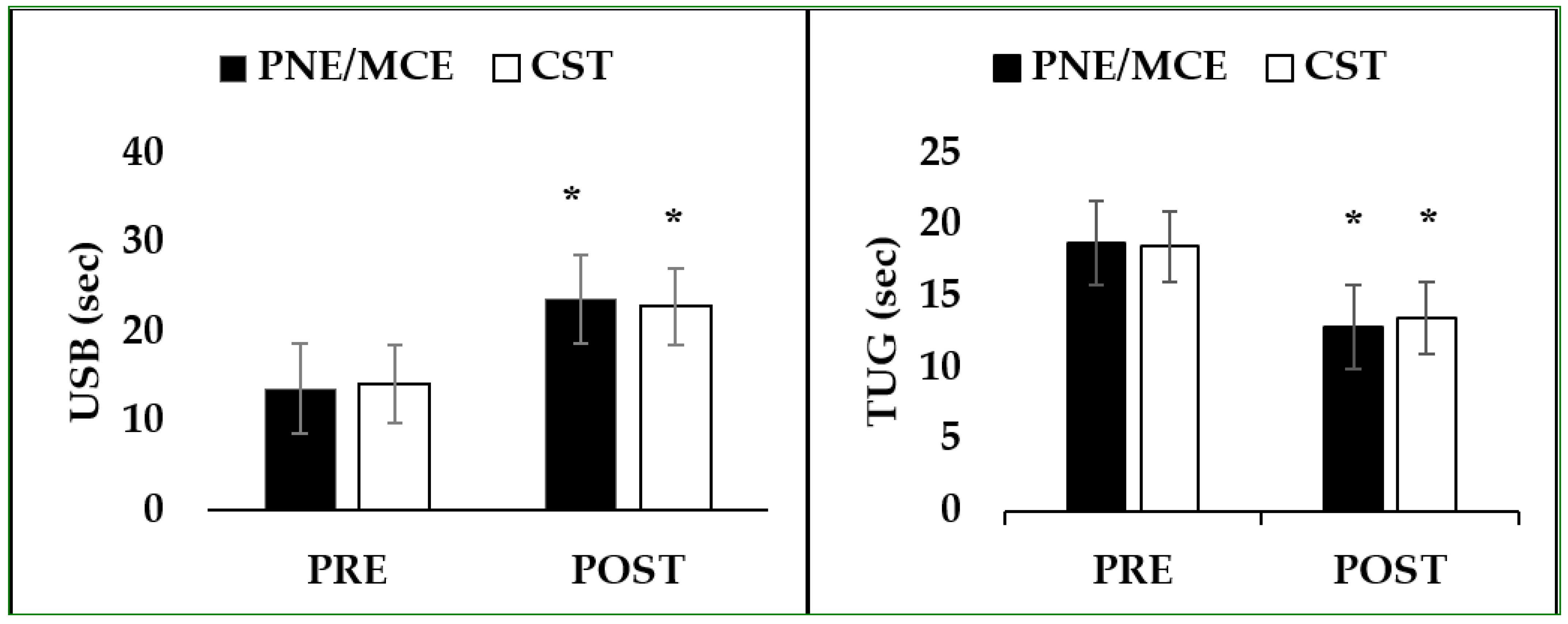
| USB (sec) | PNE/MCE | 13.62 ± 1.37 | 23.59 ± 2.05 | ↑73% | 712.9 | <0.001 * | 0.977 | 0.031 | 0.863 | 0.002 | 3.71 | 0.071 | 0.179 |
| CST | 14.13 ± 2.16 | 22.80 ± 1.69 | ↑61% | ||||||||||
| TUG (sec) | PNE/MCE | 18.70 ± 0.74 | 12.84 ± 1.26 | ↑31% | 654.38 | <0.001 * | 0.975 | 0.262 | 0.615 | 0.015 | 2.98 | 0.102 | 0.149 |
| CST | 18.46 ± 0.96 | 13.46 ± 1.12 | ↑27% | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorji, S.M.; Mohammadi Nia Samakosh, H.; Watt, P.; Henrique Marchetti, P.; Oliveira, R. Pain Neuroscience Education and Motor Control Exercises versus Core Stability Exercises on Pain, Disability, and Balance in Women with Chronic Low Back Pain. Int. J. Environ. Res. Public Health 2022, 19, 2694. https://doi.org/10.3390/ijerph19052694
Gorji SM, Mohammadi Nia Samakosh H, Watt P, Henrique Marchetti P, Oliveira R. Pain Neuroscience Education and Motor Control Exercises versus Core Stability Exercises on Pain, Disability, and Balance in Women with Chronic Low Back Pain. International Journal of Environmental Research and Public Health. 2022; 19(5):2694. https://doi.org/10.3390/ijerph19052694
Chicago/Turabian StyleGorji, Sahar Modares, Hadi Mohammadi Nia Samakosh, Peter Watt, Paulo Henrique Marchetti, and Rafael Oliveira. 2022. "Pain Neuroscience Education and Motor Control Exercises versus Core Stability Exercises on Pain, Disability, and Balance in Women with Chronic Low Back Pain" International Journal of Environmental Research and Public Health 19, no. 5: 2694. https://doi.org/10.3390/ijerph19052694