
Development and Validation of the COVID-19 Knowledges and Behavior Questionnaire in a French Population (CoVQuest-CC)

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire Development
2.2. Validation of the Questionnaire
Statistical Analysis for Psychometric Validation
3. Results
3.1. Participants Characteristics
3.2. Face Validity, Content Validity and PreTest Phase
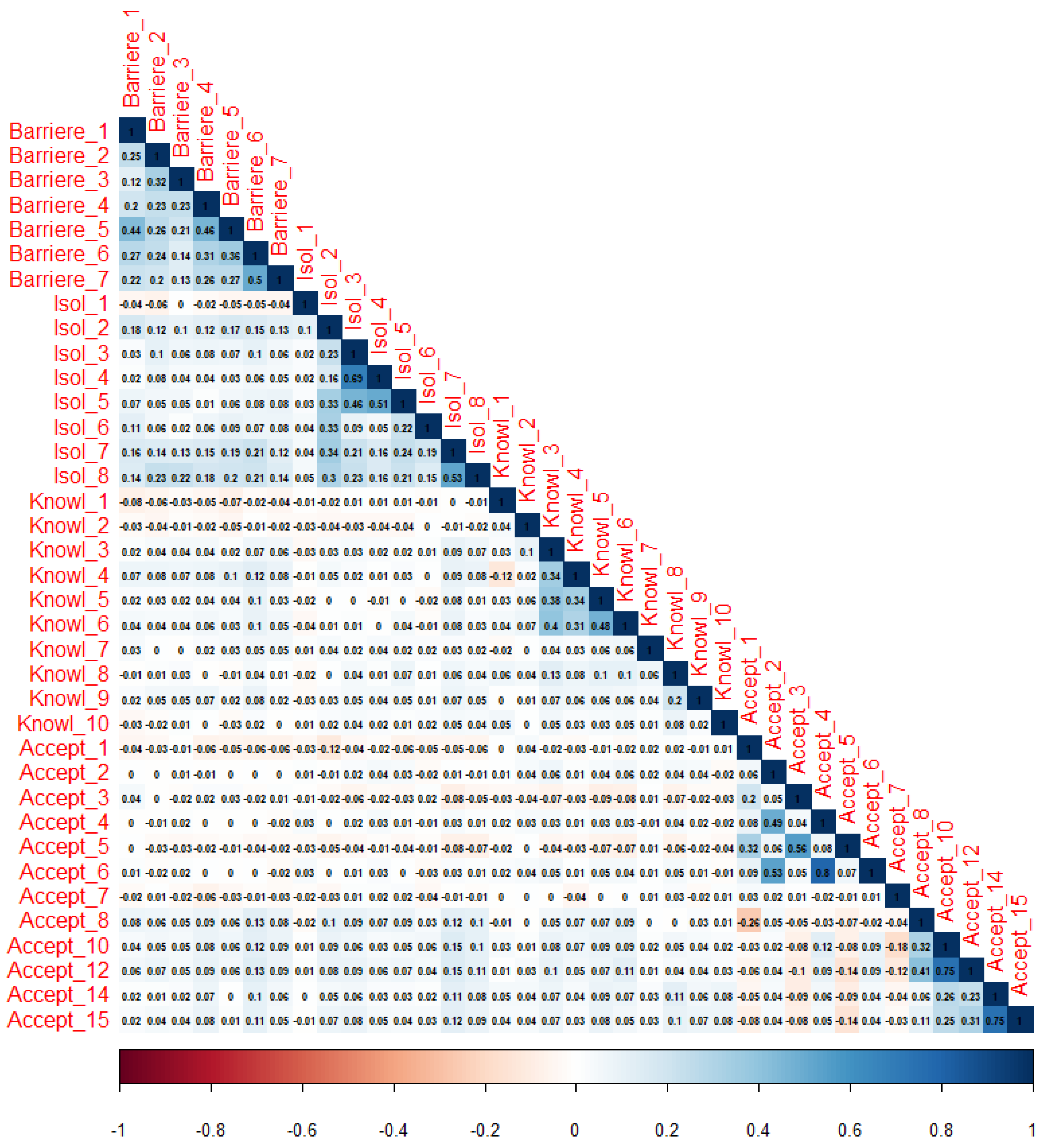
3.3. Redundancy Assessment
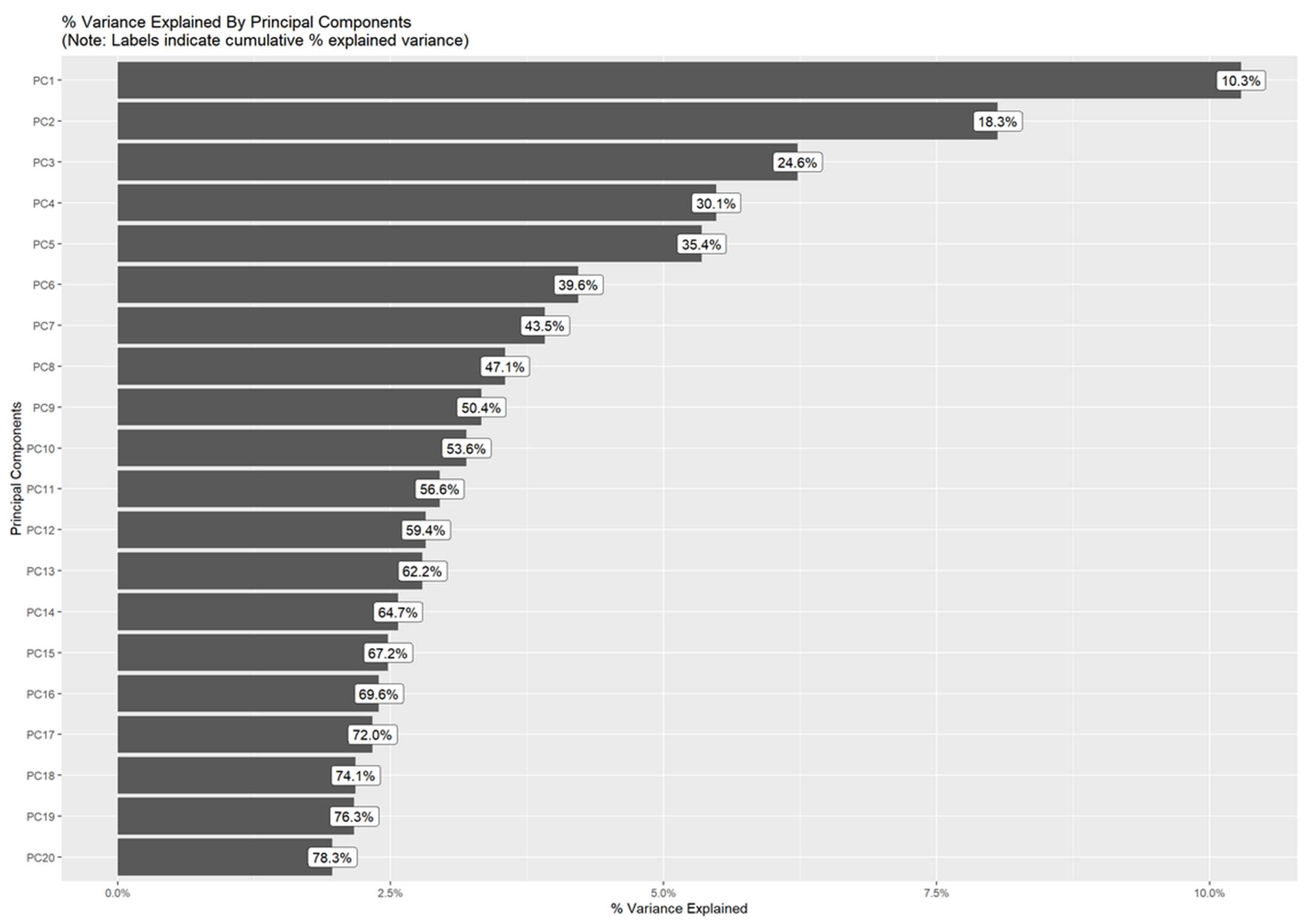
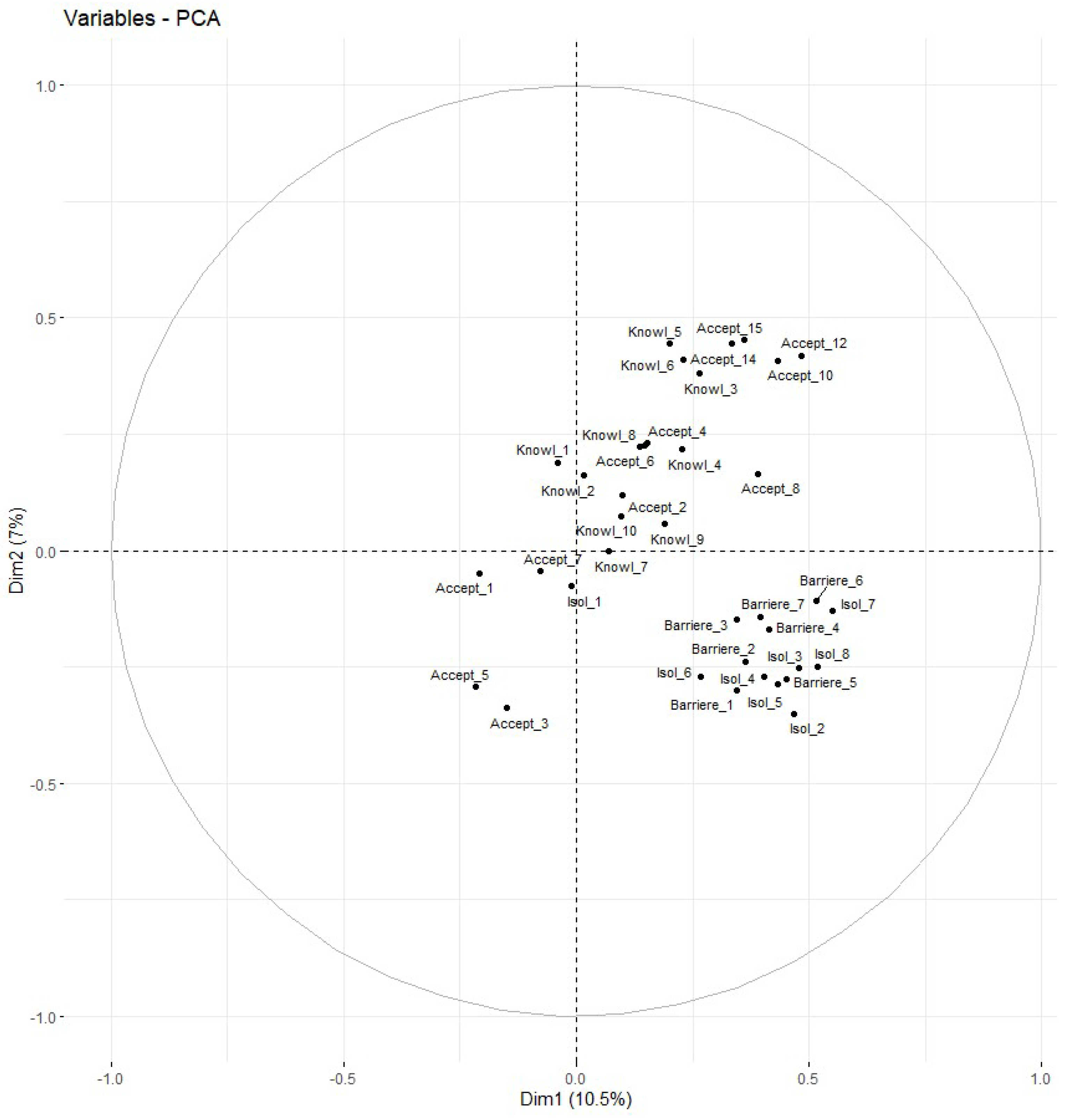
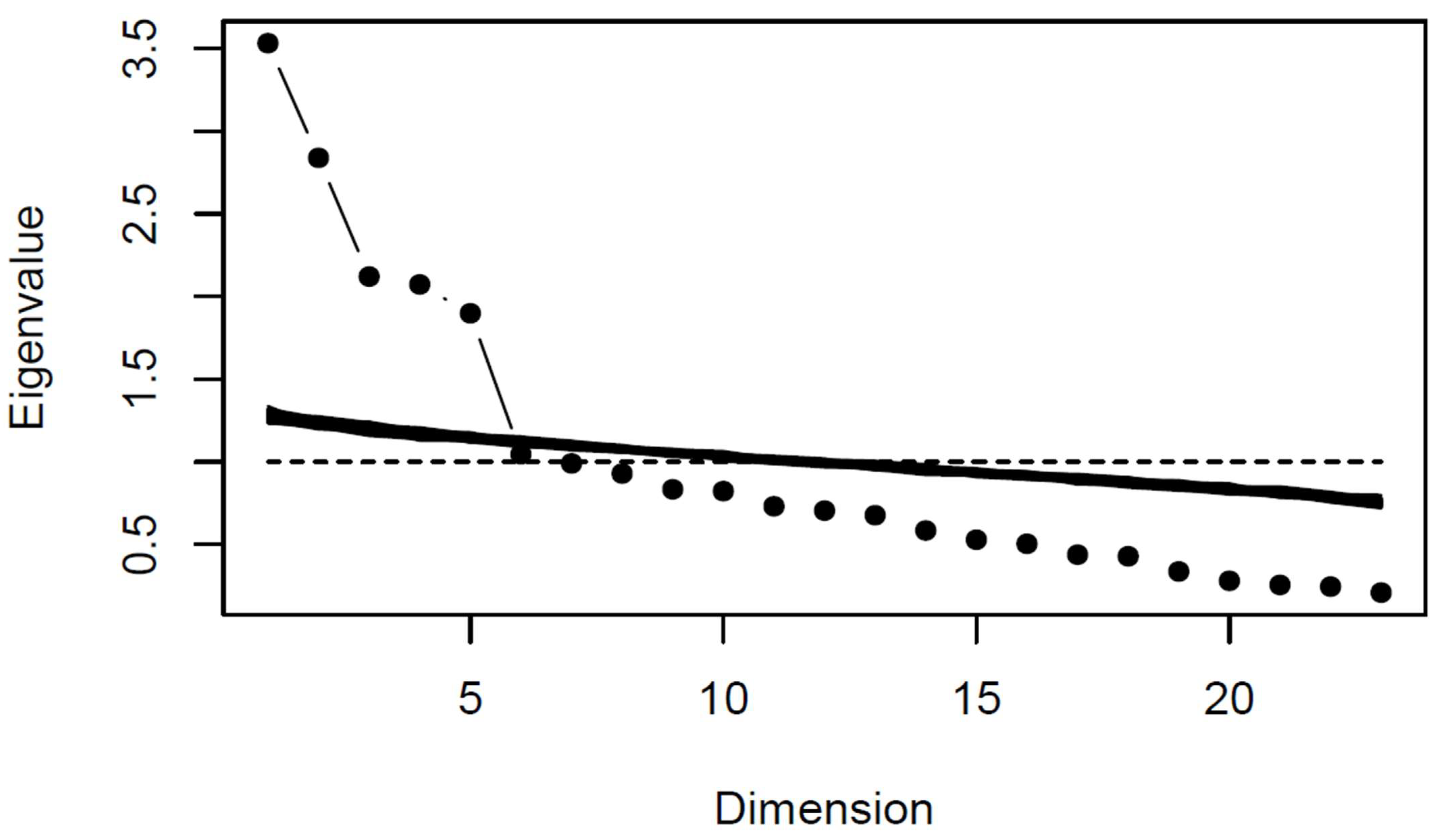
3.4. Exploratory Factorial Analysis
3.5. Confirmatory Factorial Analysis
3.6. Global Score Calculations and Search for Flooring and Ceiling Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| I. Evaluation De Vos Connaisssances Sur Les Modes De Transmission Du Virus Free translation for English-speaking readers: Assessment of your knowledge of the modes of transmission of the virus Parmi ces exemples de la vie courante, merci d’évaluer le risque de transmission du virus pour chacune d’entre elles (“Nul” = sans risque de transmission a “Très important” = risque très fort de transmission): Free translation for English-speaking readers: Among these examples from everyday life, please evaluate the risk of transmission of the virus for each of them (“Nil” = no risk of transmission a “Very important” = very high risk of transmission): Knowl_1: Discuter a 3 personnes, toutes masquées, pendant 5 min, dans une pièce sans fenêtre] Free translation for English-speaking readers: Talking to 3 people, all masked, for 5 min, in a room without windows -Nul (0.5) -Très faible (1) -Faible (1) -Modéré (0.5) -Important (0) -Très important (0) |
| Knowl_2: Discuter a 4 personnes pendant 30 min, à l’extérieur, aucune n’étant masquée et toutes sont à 1 m les unes des autres. Free translation for English-speaking readers: Talking to 4 people for 30 min, outside, none of them being masked and all of them being 1 m away from each other -Nul (0) -Très faible (0) -Faible (0.5) -Modéré (1) -Important (1) -Très important (0.5) |
| Knowl_3: Chanter sans masque a 25 personnes pendant 30 min en chorale dans une grande salle. Free translation for English-speaking readers: Singing without a mask to 25 people for 30 min in a choir in a large room -Nul (0) -Très faible (0) -Faible (0) -Modéré (0.5) -Important (1) -Très important (1) |
| Knowl_4: Faire une réunion a 10 personnes, toutes masquées, pendant 2 h, dans une petite pièce (<15 m2) sans fenêtre. Free translation for English-speaking readers: Having a meeting with 10 people, all masked, for 2 h, in a small room (<15 m2) without windows -Nul (0) -Très faible (0) -Faible (0) -Modéré (0.5) -Important (1) -Très important (1) |
| Knowl_5: Prendre un repas avec 8 amis, pour une durée de 3 heures à l’intérieur, avec une fenêtre entre-ouverte. Free translation for English-speaking readers: Having a meal with 8 friends, for 3 h indoors, with a window ajar -Nul (0) -Très faible (0) -Faible (0) -Modéré (0.5) -Important (1) -Très important (1) |
| Knowl_6: Prendre un apéritif avec 4 amis au cours d’une soirée, à l’extérieur sur une terrasse de café bondée. Free translation for English-speaking readers: Having an aperitif with 4 friends during an evening, outside on a crowded café terrace -Nul (0) -Très faible (0) -Faible (0) -Modéré (0.5) -Important (1) -Très important (1) |
| Knowl_7: Selon vous, le coronavirus peut se transmettre: [Par l’air] Free translation for English-speaking readers: In your opinion, coronavirus can be transmitted: [Through the air] -Non (0) -Oui (1) -Ne sais pas (0) |
| Knowl_8: Selon vous, le coronavirus peut se transmettre: [Par les postillons] Free translation for English-speaking readers: In your opinion, coronavirus can be transmitted: [Through sputum] -Non (0) -Oui (1) -Ne sais pas (0) |
| Knowl_9: Selon vous, le coronavirus peut se transmettre: [Par les mains] Free translation for English-speaking readers: In your opinion, coronavirus can be transmitted: [By hands] -Non (0) -Oui (1) -Ne sais pas (0) |
| Knowl_10: Selon vous, le coronavirus peut se transmettre: [Par le sang] Free translation for English-speaking readers: In your opinion, coronavirus can be transmitted: [Through blood] -Non (0) -Oui (1) -Ne sais pas (0) |
| II. EVALUATION DE VOTRE COMPORTEMENT VIS A VIS DES GESTES BARRIERES Free translation for English-speaking readers: Assessment of your current behavior with respect to barrier gestures Barriere_1: A quelle fréquence portez-vous le masque dans la vie de tous les jours à votre domicile quand vous recevez des gens qui ne vivent pas sous votre toit (enfants, petits-enfants, amis, voisins…) ? Free translation for English-speaking readers: How often do you wear the mask in everyday life in your home when entertaining people who do not live in your home (children, grandchildren, friends, neighbors…)? -Jamais (0) -De temps en temps (1) -La moitié du temps (2) -Souvent (3) -Tout le temps (4) |
| Barriere_2: A l’extérieur, faites-vous une hygiène des mains avec une solution hydro-alcoolique SYSTEMATIQUEMENT (après avoir touché de l’argent, surfaces lors de courses, sièges des transports en commun, …)? Free translation for English-speaking readers: When your are outside, do you SYSTEMATICALLY perform hand hygiene with a hydro-alcoholic solution (after touching money, surfaces when shopping, public transportation seats, …)? -Jamais (0) -De temps en temps (1) -La moitié du temps (2) -Souvent (3) -Tout le temps (4) |
| Barriere_3: EN DEHORS de l’utilisation de solution hydro-alcoolique, à quelle fréquence vous lavez-vous les mains depuis le début de la pandémie ? Free translation for English-speaking readers: OTHER THAN using hydro-alcoholic solution, how often have you washed your hands since the beginning of the pandemic? -Jamais (0) -De temps en temps (1) -La moitié du temps (2) -Souvent (3) -Tout le temps (4) |
| Barriere_4: A quelle fréquence pensez-vous respecter la distanciation physique (>1 m), dans votre vie a l’exterieur (courses, vie sociale…) ? Free translation for English-speaking readers: How often do you think you respect the physical distance (>1 m), in your life outside (shopping, social life...)? -Jamais (0) -De temps en temps (1) -La moitié du temps (2) -Souvent (3) -Tout le temps (4) |
| Barriere_5: A quelle fréquence considérez-vous respecter la distanciation physique (au moins 1 m) dans votre vie a l’intérieur lorsque vous recevez des personnes qui n’habitent pas sous le même toit (repas de famille, repas avec des amis, visite des enfants, petits-enfants…) ? Free translation for English-speaking readers: How often do you consider respecting the physical distance (at least 1 m) in your indoor life when you receive people who do not live under the same roof (family meals, meals with friends, visits from children, grandchildren…)? -Jamais (0) -De temps en temps (1) -La moitié du temps (2) -Souvent (3) -Tout le temps (4) |
| Barriere_6: Etes-vous d’accord avec les affirmations suivantes: [“Je limite le nombre de personnes avec lesquelles j’interagis dans ma vie PERSONNELLE”] Free translation for English-speaking readers: Do you agree with the following statements: [“I limit the number of people I interact with in my PERSONAL life”] -Pas du tout d’accord (0) -Pas d’accord (1) -Ni plus, ni moins d’accord (2) -D’accord (3) -Tout a fait d’accord (4) |
| Barriere_7: Etes-vous d’accord avec les affirmations suivantes: [“Je limite le nombre de personnes avec lesquelles j’interagis dans ma vie PROFESSIONNELLE”] Free translation for English-speaking readers: Do you agree with the following statements: [“I limit the number of people I interact with in my PROFESSIONAL life”] -Pas du tout d’accord (0) -Pas d’accord (1) -Ni plus, ni moins d’accord (2) -D’accord (3) -Tout à fait d’accord (4) |
| III. EVALUATION DE VOTRE COMPORTEMENT POSSIBLE SI VOUS ETIEZ DEPISTE POSITIF Free translation for English-speaking readers: Assessment of your possible behavior if you tested positive for the virus Isol_1: Si vous deviez vous isoler pendant 7 à 10 jours en cas de résultat positif, quel serait votre niveau d’inquiétude: Free translation for English-speaking readers: If you were to isolate yourself for 7–10 days in case of a positive result, what would be your level of concern: -Angoisse(e) (4) -Très inquiet(e) (3) -Inquiet(e) (2) -Peu inquiet(e) (1) -Pas inquiet(e) (0) |
| Isol_2: Si vous deviez vous isoler pendant 7 à 10 jours en cas de résultat positif, vous serait-il possible de mettre en œuvre les mesures suivantes: [Rester pendant 7 jours, le plus longtemps possible (jour et nuit), seul(e) dans une pièce (sans avoir de contacts physiques avec votre entourage)] Free translation for English-speaking readers: If you were to isolate yourself for 7–10 days in case of a positive result, would you be able to implement the following measures: [Stay for 7 days, for as long as possible (day and night), alone in a room (with no physical contact with those around you)] -Impossible (4) -Très difficile (3) -Difficile (2) -Facile (1) -Très facile (0) |
| Isol_3: Si vous deviez vous isoler pendant 7 à 10 jours en cas de résultat positif, vous serait-il possible de mettre en œuvre les mesures suivantes: [Faire intervenir quelqu’un pour faire les courses] Free translation for English-speaking readers: If you were to isolate yourself for 7–10 days if you tested positive, would you be able to implement the following measures: [Get someone to do the shopping] -Impossible (4) -Très difficile (3) -Difficile (2) -Facile (1) -Très facile (0) |
| Isol_4: Si vous deviez vous isoler pendant 7 à 10 jours en cas de résultat positif, vous serait-il possible de mettre en œuvre les mesures suivantes: [Faire intervenir quelqu’un pour faire le repas] Free translation for English-speaking readers: If you were to isolate yourself for 7–10 days if you tested positive, would you be able to implement the following measures: [Get someone to make the meal] -Impossible (4) -Très difficile (3) -Difficile (2) -Facile (1) -Très facile (0) |
| Isol_5: Si vous deviez vous isoler pendant 7 à 10 jours en cas de résultat positif, vous serait-il possible de mettre en œuvre les mesures suivantes: [Faire intervenir quelqu’un pour prendre en charge les enfants] Free translation for English-speaking readers: If you were to isolate yourself for 7–10 days in the event of a positive result, would you be able to implement the following measures: [Get someone to take care of the children] -Impossible (4) -Très difficile (3) -Difficile (2) -Facile (1) -Très facile (0) |
| Isol_6: Si vous deviez vous isoler pendant 7 à 10 jours en cas de résultat positif, vous serait-il possible de mettre en œuvre les mesures suivantes: [Utilisez des toilettes qui vous seraient réservées] Free translation for English-speaking readers: If you were to isolate yourself for 7–10 days in the event of a positive result, would you be able to implement the following measures: [Use a restroom that would be reserved for you] -Impossible (4) -Très difficile (3) -Difficile (2) -Facile (1) -Très facile (0) |
| Isol_7: Si vous deviez vous isoler pendant 7 à 10 jours en cas de résultat positif, vous serait-il possible de mettre en œuvre les mesures suivantes: [Utilisez un masque à domicile en présence de votre entourage] Free translation for English-speaking readers: If you were to isolate yourself for 7–10 days in the event of a positive result, would you be able to implement the following measures: [Use a mask at home in the presence of others] -Impossible (4) -Très difficile (3) -Difficile (2) -Facile (1) -Très facile (0) |
| Isol_8: Si vous deviez vous isoler pendant 7 a 10 jours en cas de résultat positif, vous serait-il possible de mettre en œuvre les mesures suivantes: [Nettoyer les surfaces plusieurs fois par jour les surfaces touchées (poignées de porte, rampes d’escalier, interrupteurs, …)] Free translation for English-speaking readers: If you were to isolate yourself for 7 to 10 days in case of a positive result, would you be able to implement the following measures: [Clean the surfaces several times a day the affected surfaces (door handles, stair railings, light switches, …)] -Impossible (4) -Très difficile (3) -Difficile (2) -Facile (1) -Très facile (0) |
| IV. LES PRELEVEMENTS Free translation for English-speaking readers: Tests for screening Accept_1: Concernant le prélèvement nasopharyngé (SI VOUS EN AVEZ DEJA BENEFICIE), sur une échelle de 0 a 10, diriez-vous qu’il était: [Douloureux (0 = pas douloureux du tout à 10 = pire douleur imaginable)] Free translation for English-speaking readers: Regarding the nasopharyngeal swab (IF YOU HAVE EVER HAD IT), on a scale of 0 to 10, would you say it was: [Painful (0 = not painful at all to10 = worst pain imaginable)] |
| Accept_2: Concernant le prélèvement nasopharyngé (SI VOUS EN AVEZ DEJA BENEFICIE), sur une échelle de 0 a 10, diriez-vous qu’il était: [Pratique (facile, rapide — 0 = pas pratique du tout à 10 = extrêmement pratique)] Free translation for English-speaking readers: Regarding nasopharyngeal swabbing (IF YOU HAVE EVER HAD IT), on a scale of 0 to 10, would you say it was: [Convenient (easy, quick - 0 = not convenient at all to 10 = extremely convenient)] |
| Accept_3: Concernant le prélèvement salivaire, sur une échelle de 0 a 10, diriez-vous qu’il était: [Douloureux (0 = pas douloureux du tout à 10 = pire douleur imaginable)] Free translation for English-speaking readers: Regarding the saliva collection, on a scale of 0 to 10, would you say it was: [Painful (0 = not painful at all to 10 = worst pain imaginable)] |
| Accept_4: Concernant le prélèvement salivaire, sur une échelle de 0 a 10, diriez-vous qu’il était: [Pratique (facile, rapide - 0 = pas pratique du tout à 10 = extrêmement pratique)] Free translation for English-speaking readers: Regarding saliva collection, on a scale of 0 to 10, would you say it was: [Convenient (easy, quick - 0 = not convenient at all to 10 = extremely convenient)] |
| Accept_5: Concernant le prélèvement l’auto-prélèvement salive et nez antérieur, sur une échelle de 0 a 10, diriez-vous qu’il était: [Douloureux (0 = pas douloureux du tout à 10 = pire douleur imaginable)] Free translation for English-speaking readers: Regarding the saliva and anterior nose swab, on a scale of 0 to 10, would you say it was: [Painful (0 = not painful at all to 10 = worst pain imaginable)] |
| Accept_6: Concernant le prélèvement l’auto-prélèvement salive et nez antérieur, sur une échelle de 0 a 10, diriez-vous qu’il était: [Pratique (facile, rapide — 0 = pas pratique du tout à 10 = extrêmement pratique)] Free translation for English-speaking readers: Concerning the self-sampling of saliva and anterior nose, on a scale of 0 to 10, would you say that it was: [Convenient (easy, quick — 0 = not convenient at all to 10 = extremely convenient)] |
| Accept_7: Si vous deviez faire un nouveau test, quel test préfériez-vous faire? -Pas de préférence (0) -Test sur crachat salivaire (1) -Test sur auto-prélèvement salivaire et nez antérieur (2) -Test classique (dans le nez) (3) Free translation for English-speaking readers: If you were to take a new test, which test would you prefer to take? -No preference (0) -Saliva sputum test (1) -Saliva swab and anterior nose test (2) -Classic test (in the nose) (3) |
| Accept_8: Si l’on devait vous refaire un test classique (dans le nez) dans les jours à venir, que feriez-vous? -Je refuserais certainement (0) -Je refuserais probablement (1) -J’accepterais probablement (2) -J’accepterais certainement (3) Free translation for English-speaking readers: If you were to be tested again with a test in the front part of your nose in the next few days, what would you do? -I would definitely refuse (0) -I would probably refuse (1) -I would probably accept (2) -I would definitely accept (3) |
| Accept_9: Si refus, pourquoi? -Autre -Difficultés pratiques pour effectuer l’examen (délais de rendez-vous, temps d’attente, etc.) -Examen trop désagréable, douloureux Free translation for English-speaking readers: If no, why? -Other -Practical difficulties to perform the examination (appointment delays, waiting time, etc.) -Examination too unpleasant, painful |
| Accept_10: Si l’on devait vous refaire un test salivaire dans les jours a venir, que feriez-vous? -Je refuserais certainement (0) -Je refuserais probablement (1) -J’accepterais probablement (2) -J’accepterais certainement (3) Free translation for English-speaking readers: If you were to be retested with a saliva test in the next few days, what would you do? -I would definitely refuse (0) -I would probably refuse (1) -I would probably accept (2) -I would definitely accept (3) |
| Accept_11: Si refus, pourquoi? -Autre -Difficultés pratiques pour effectuer l’examen (délais de rendez-vous, temps d’attente, etc.) -Examen trop désagréable, douloureux Free translation for English-speaking readers: If no, why? -Other -Practical difficulties to perform the examination (appointment delays, waiting time, etc.) -Examination too unpleasant, painful |
| Accept_12: Si l’on devait vous refaire un test salivaire et nez anterieur dans les jours a venir, que feriez-vous? -Je refuserais certainement (0) -Je refuserais probablement (1) -J’accepterais probablement (2) -J’accepterais certainement (3) Free translation for English-speaking readers: If you were to have a saliva test and a test in the front part of your nose again in the next few days, what would you do? -I would definitely refuse (0) -I would probably refuse (1) -I would probably accept (2) -I would definitely accept (3) |
| Accept_13: Si refus, pourquoi? -Autre -Difficultés pratiques pour effectuer l’examen (délais de rendez-vous, temps d’attente, etc.) -Examen trop désagréable, douloureux Free translation for English-speaking readers: If no, why? -Other -Practical difficulties to perform the examination (appointment delays, waiting time, etc.) -Examination too unpleasant, painful |
| Accept_14: Vous sentiriez-vous capable de faire le prélèvement de crachat salivaire seul dans un pot chez vous puis le déposer au laboratoire? -Certainement non (0) -Probablement non (1) -Probablement oui (2) -Certainement oui (3) Free translation for English-speaking readers: Would you feel able to take a salivary sputum sample alone in a jar at home and then take it to the laboratory? -Certainly not (0) -Probably no (1) -Probably yes (2) -Definitely yes (3) |
| Accept_15: Vous sentiriez-vous capable de faire l’auto prélèvement de crachat salivaire et nez antérieur seul dans un pot chez vous puis le déposer au laboratoire? -Certainement non (0) -Probablement non (1) -Probablement oui (2) -Certainement oui (3) Free translation for English-speaking readers: Would you feel able to do the self-sampling of salivary sputum and anterior nose alone in a jar at home and then take it to the laboratory? -Certainly not (0) -Probably no (1) -Probably yes (2) -Certainly yes (3) |
| -Questions acronyms are indicated in bold type. The only purpose of these acronyms is to refer more easily to the questions in this article, and they therefore were not present in distributed questionnaires. -All categorical questions integrated in the internal consistency validation procedure were converted into numerical variables for the purpose of this procedure. For these variables, numerical conversion values are indicated in brackets next to each modality. These values were not indincated in the distributed questionnaires. -People responding “Autre” at Accept_9, Accept_11 and Accept_13 were given the possibility to precise their reason in a free-form text |




References
- Cauchemez, S.; Kiem, C.T.; Paireau, J.; Rolland, P.; Fontanet, A. Lockdown impact on COVID-19 epidemics in regions across metropolitan France. Lancet 2020, 396, 1068–1069. [Google Scholar] [CrossRef]
- Broucke, S.V.D. Why health promotion matters to the COVID-19 pandemic, and vice versa. Health Promot. Int. 2020, 35, 181–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Easton, P.; Entwistle, V.A.; Williams, B. Health in the ’hidden population’ of people with low literacy. A systematic review of the literature. BMC Public Health 2010, 10, 459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferron, C. La litteratie en Santé: Synthèse Bibliographique; Fédération Nationale d’Education et de promotion de la Santé: Paris, France, 2017; ISBN 1471245810. [Google Scholar]
- Okan, O.; Sørensen, K.; Messer, M. COVID-19: A guide to good practice on keeping people well informed. Conversation 2020, 19, 2020. [Google Scholar]
- Spring, H. Health literacy and COVID-19. Health Inf. Libr. J. 2020, 37, 171–172. [Google Scholar] [CrossRef]
- West, R.; Michie, S.; Rubin, G.J.; Amlôt, R. Applying principles of behaviour change to reduce SARS-Co, V-2 transmission. Nat. Hum. Behav. 2020, 4, 451–459. [Google Scholar] [CrossRef]
- Matterne, U.; Egger, N.; Tempes, J.; Tischer, C.; Lander, J.; Dierks, M.-L.; Bitzer, E.-M.; Apfelbacher, C. Health literacy in the general population in the context of epidemic or pandemic coronavirus outbreak situations: Rapid scoping review. Patient Educ. Couns. 2021, 104, 223–234. [Google Scholar] [CrossRef]
- Hiltrop, K.; Hiebel, N.; Geiser, F.; Kriegsmann-Rabe, M.; Gambashidze, N.; Morawa, E.; Erim, Y.; Weidner, K.; Albus, C.; Ernstmann, N. Measuring COVID-19 Related Health Literacy in Healthcare Professionals—Psychometric Evaluation of the HL-COV-HP Instrument. Int. J. Environ. Res. Public Health 2021, 18, 11959. [Google Scholar] [CrossRef]
- Salameh, B.; Basha, S.; Basha, W.; Abdallah, J. Knowledge, Perceptions, and Prevention Practices among Palestinian University Students during the COVID-19 Pandemic: A Questionnaire-Based Survey. Inq. J. Health Care Organ. Provis. Financ. 2021, 58. [Google Scholar] [CrossRef] [PubMed]
- McCaffery, K.J.; Dodd, R.H.; Cvejic, E.; Ayrek, J.; Isautier, J.M.; Copp, T.; Bonner, C.; Pickles, K.; Nickel, B.; Dakin, T.; et al. Health literacy and disparities in COVID-19–related knowledge, attitudes, beliefs and behaviours in Australia. Public Health Res. Pract. 2020, 30. [Google Scholar] [CrossRef] [PubMed]
- Coroiu, A.; Moran, C.; Campbell, T.; Geller, A.C. Barriers and facilitators of adherence to social distancing recommendations during COVID-19 among a large international sample of adults. PLoS ONE 2020, 15, e0239795. [Google Scholar] [CrossRef]
- McCormack, L.A.; Squiers, L.; Frasier, A.M.; Bevc, C.; Lynch, M.; Bann, C.M.; Macdonald, P.D. Gaps in Knowledge About COVID-19 Among US Residents Early in the Outbreak. Public Health Rep. 2021, 136, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, A.A.; Alshammary, F.; Amin, J.; Rathore, H.A.; Hassan, I.; Ilyas, M.; Alam, M.K. Knowledge and practice regarding prevention of COVID-19 among the Saudi Arabian population. Work 2020, 66, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Comparison of Strategies Based on RT-PCR or Antigenic Test for the Screening of SARS-CoV-2 Infection (COVID-19). (AutoCoV). 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT04859023?term=autocov&cntry=FR&draw=2&rank=1 (accessed on 27 July 2021).
- Zahiruddin, W.M.; Arifin, W.N.; Mohd-Nazri, S.; Sukeri, S.; Zawaha, I.; Abu Bakar, R.; Hamat, R.A.; Malina, O.; Jamaludin, T.Z.M.T.; Pathman, A.; et al. Development and validation of a new knowledge, attitude, belief and practice questionnaire on leptospirosis in Malaysia. BMC Public Health 2018, 18, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Mallah, N.; Rodríguez-Cano, R.; Figueiras, A.; Takkouche, B. Design, reliability and construct validity of a Knowledge, Attitude and Practice questionnaire on personal use of antibiotics in Spain. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Angarita-Díaz, M.d.P.; Forero-Escobar, D.; Mora-Reina, J.E.; Torres-Gaona, L.P.; Gómez-Trujillo, R.N. Development and validation of a questionnaire to determine knowledge, attitudes and practices in antibiotics prescription in dentistry. Rev. Fac. Odontol. 2019, 31, 112–121. [Google Scholar] [CrossRef]
- Geer, L.A.; Curbow, B.A.; Anna, D.H.; Lees, P.S.J.; Buckley, T.J. Development of a questionnaire to assess worker knowledge, attitudes and perceptions underlying dermal exposure. Scand. J. Work. Environ. Health 2006, 32, 209–218. [Google Scholar] [CrossRef] [Green Version]
- Rios-Castillo, I.; González-Madden, E.; Kodish, S.; González-Medina, G.; Lebrija, A.; Avila-Pozos, R. Construct Validity and Reliability of a Knowledge, Attitude, Perception, and Behaviors on Dietary Practices Questionnaire for School-Age Children in Panama. J. Nutr. Health Sci. 2020, 7, 104. [Google Scholar]
- Likert, R. Technique for the measurement of attitudes. Arch. Psychol. 1932, 140, 1–55. [Google Scholar]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cattell, R.B. The Scree Test For The Number of Factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef]
- Horn, J.L. A rationale and test for the number of factors in factor analysis. Psychom. 1965, 30, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Tabachnick, B.; Fidell, L. Using Multivariate Statistics, International Student Edition; Pearson: Boston, MA, USA, 2001; ISBN 0-321-05677-9. [Google Scholar]
- Gallucci, M.; Perugini, M. The marker index: A new method of selection of marker variables in factor analysis. TPM-Test. Psychom. Methodol. Appl. Psychol. 2007, 14, 3–25. [Google Scholar]
- Bollen, K.A.; Stine, R.A. Bootstrapping Goodness-of-Fit Measures in Structural Equation Models. Sociol. Methods Res. 1992, 21, 205–229. [Google Scholar] [CrossRef]
- Hu, L.-T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Helander, M.; Landauer, T.K.; Prabhu, P. Behavioral research methods in human-computer interaction. In Handbook of Human-Computer Interaction; Elsevier: Amsterdam, The Netherlands, 1997; ISBN 9780080532882. [Google Scholar]
- Greer, M.L.; Sample, S.; Jensen, H.K.; McBain, S.; Lipschitz, R.; Sexton, K.W. COVID-19 Is Connected with Lower Health Literacy in Rural Areas. Stud. Health Technol. Inform. 2021, 281, 804–808. [Google Scholar] [CrossRef]
- Silva, M.; Santos, P. The Impact of Health Literacy on Knowledge and Attitudes towards Preventive Strategies against COVID-19: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5421. [Google Scholar] [CrossRef]
- Zhu, Y.; Duan, M.-J.; Dijk, H.H.; Freriks, R.D.; Dekker, L.H.; Mierau, J.O. Association between socioeconomic status and self-reported, tested and diagnosed COVID-19 status during the first wave in the Northern Netherlands: A general population-based cohort from 49 474 adults. BMJ Open 2021, 11, e048020. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Karim, S.S.A.; Karim, Q.A. Omicron SARS-Co, V-2 variant: A new chapter in the COVID-19 pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef]
- Santé Publique France. COVID-19: Point Epidémiologique en Auvergne-Rhône-Alpes du 29 Octobre 2020. Available online: https://www.santepubliquefrance.fr/regions/auvergne-rhone-alpes/documents/bulletin-regional/2020/covid-19-point-epidemiologique-en-auvergne-rhone-alpes-du-29-octobre-2020 (accessed on 9 July 2021).
- Veresiu, E.; Robinson, T. Successful Health Campaigns during COVID-19 Need to Manage Our Altered Ideas about the Future. Available online: https://theconversation.com/successful-health-campaigns-during-covid-19-need-to-manage-our-altered-ideas-about-the-future-163246 (accessed on 23 July 2021).
| I. Assessment of Your Knowledge of the Modes of Transmission of the Virus Among these examples from everyday life, please evaluate the risk of transmission of the virus for each of them: |
| Knowl_1: Talking to 3 people, all masked, for 5 min, in a room without windows |
| Knowl_2: Talking to 4 people for 30 min, outside, none of them being masked and all of them being 1 m away from each other |
| Knowl_3: Singing without a mask to 25 people for 30 min in a choir in a large room |
| Knowl_4: Having a meeting with 10 people, all masked, for 2 h, in a small room (<15 m2) without windows |
| Knowl_5: Having a meal with 8 friends, for 3 h indoors, with a window ajar |
| Knowl_6: Having an aperitif with 4 friends during an evening, outside on a crowded café terrace |
| In your opinion, coronavirus can be transmitted: |
| Knowl_7: Through the air |
| Knowl_8: Through sputum |
| Knowl_9: By hands |
| Knowl_10: Through blood |
| II. Assessment of Your Current Behavior with Respect to Barrier Gestures |
| Barriere_1: How often do you wear the mask in everyday life in your home when entertaining people who do not live in your home (children, grandchildren, friends, neighbors…)? |
| Barriere_2: When your are outside, do you SYSTEMATICALLY perform hand hygiene with a hydro-alcoholic solution (after touching money, surfaces when shopping, public transportation seats,…)? |
| Barriere_3: OTHER THAN using hydro-alcoholic solution, how often have you washed your hands since the beginning of the pandemic? |
| Barriere_4: How often do you think you respect the physical distance (>1 m), in your life outside (shopping, social life…)? |
| Barriere_5: How often do you consider respecting the physical distance (at least 1 m) in your indoor life when you receive people who do not live under the same roof (family meals, meals with friends, visits from children, grandchildren…)? |
| Do you agree with the following statements: |
| Barriere_6: I limit the number of people I interact with in my PERSONAL life |
| Barriere_7: I limit the number of people I interact with in my PROFESSIONAL life |
| III. Assessment of Your Possible Behavior If You Tested Positive for the Virus |
| Isol_1: If you were to isolate yourself for 7–10 days in case of a positive result, what would be your level of concern? |
| If you were to isolate yourself for 7–10 days in case of a positive result, would you be able to implement the following measures: |
| Isol_2: Stay for 7 days, for as long as possible (day and night), alone in a room (with no physical contact with those around you) |
| Isol_3: Get someone to do the shopping |
| Isol_4: Get someone to make the meal |
| Isol_5: Get someone to take care of the children |
| Isol_6: Use a restroom that would be reserved for you |
| Isol_7: Use a mask at home in the presence of others |
| Isol_8: Clean several times a day the affected surfaces (door handles, stair railings, light switches,…) |
| IV. Tests For Screening |
| Accept_1: Regarding the nasopharyngeal screening test (IF YOU HAVE EVER HAD IT), on a scale of 0 to 10, would you say it was? |
| Accept_2: Regarding nasopharyngeal swabbing (IF YOU HAVE EVER HAD IT), on a scale of 0 to 10, would you say it was? |
| Accept_3: Regarding the saliva collection, on a scale of 0 to 10, would you say it was? |
| Accept_4: Regarding saliva collection, on a scale of 0 to 10, would you say it was? |
| Accept_5: Regarding the saliva and anterior nose swab, on a scale of 0 to 10, would you say it was? |
| Accept_6: Concerning the self-sampling of saliva and anterior nose, on a scale of 0 to 10, would you say that it was? |
| Accept_7: If you were to take a new test, which test would you prefer to take? |
| Accept_8: If you were to be tested again with a test in the front part of your nose in the next few days, what would you do? |
| Accept_9: If no, why? |
| Accept_10: If you were to be retested with a saliva test in the next few days, what would you do? |
| Accept_11: If no, why? |
| Accept_12: If you were to have a saliva test and a test in the front part of your nose again in the next few days, what would you do? |
| Accept_13: If no, why? |
| Accept_14: Would you feel able to take a salivary sputum sample alone in a jar at home and then take it to the laboratory? |
| Accept_15: Would you feel able to do the self-sampling of salivary sputum and anterior nose alone in a jar at home and then take it to the laboratory? |
| Characteristics | January (n = 3338,%) | February (n = 4707, %) | Total (n = 8045, %) |
|---|---|---|---|
| Age (years) | |||
| 10–19 | 157 (4.7) | 272 (5.8) | 429 (5.3) |
| 20–29 | 359 (10.8) | 604 (12.8) | 963 (12.0) |
| 30–39 | 345 (10.4) | 524 (11.1) | 869 (10.8) |
| 40–49 | 442 (13.3) | 756 (16.1) | 1198 (14.9) |
| 50–59 | 496 (14.9) | 810 (17.2) | 1306 (16.3) |
| 60–69 | 698 (21.0) | 899 (19.1) | 1597 (19.9) |
| 70–79 | 614 (18.5) | 695 (14.8) | 1309 (16.3) |
| 80–89 | 188 (5.7) | 136 (2.9) | 324 (4.0) |
| More than 90 | 24 (0.7) | 7 (0.1) | 31 (0.4) |
| Gender | |||
| Female | 1704 (51.9) | 2634 (56.1) | 4338 (54.4) |
| Male | 1581 (48.1) | 2058 (43.9) | 3639 (45.6) |
| Profession | |||
| School student | 15 (0.5) | 152 (3.3) | 167 (2.1) |
| Student | 294 (8.9) | 370 (7.9) | 664 (8.3) |
| Unemployed | 256 (7.8) | 234 (5.0) | 490 (6.2) |
| Healthcare Worker | 174 (5.3) | 464 (9.9) | 638 (8.0) |
| Employee | 1025 (31.1) | 1584 (33.9) | 2609 (32.8) |
| Self-employed | 109 (3.3) | 142 (3.0) | 251 (3.2) |
| Retired | 1290 (39.2) | 1474 (31.5) | 2764 (34.7) |
| Other | 129 (3.9) | 254 (5.4) | 383 (4.8) |
| Subscales | Items | Factor Loading | Cronbach Alpha [95% CI] |
|---|---|---|---|
| SARS-CoV-2 transmission knowledge | Knowl_2 | 0.458 | 0.83 [0.81–0.84] |
| Knowl_3 | 0.815 | ||
| Knowl_4 | 0.732 | ||
| Knowl_5 | 0.856 | ||
| Knowl_6 | 0.812 | ||
| Knowl_8 | 0.212 | ||
| Barrier gestures respect | Barriere_1 | 0.564 | 0.71 [0.69–0.73] |
| Barriere_2 | 0.364 | ||
| Barriere_4 | 0.547 | ||
| Barriere_5 | 0.675 | ||
| Barriere_6 | 0.58 | ||
| Barriere_7 | 0.472 | ||
| Screening tests acceptability | Accept_8 | 0.448 | 0.65 [0.63–0.69] |
| Accept_10 | 0.822 | ||
| Accept_12 | 0.928 | ||
| Accept_15 | 0.336 | ||
| Home isolation possibility | Isol_2 | 0.825 | 0.72 [0.69–0.74] |
| Isol_3 | 0.818 | ||
| Isol_4 | 0.602 | ||
| Isol_5 | 0.29 | ||
| Tests practicability | Accept_2 | 0.504 | 0.83 [0.81–0.84] |
| Accept_4 | 0.848 | ||
| Accept_6 | 0.876 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verot, E.; Bonjean, P.; Chaux, R.; Gagnaire, J.; Gagneux-Brunon, A.; Pozzetto, B.; Berthelot, P.; Botelho-Nevers, E.; Chauvin, F. Development and Validation of the COVID-19 Knowledges and Behavior Questionnaire in a French Population (CoVQuest-CC). Int. J. Environ. Res. Public Health 2022, 19, 2569. https://doi.org/10.3390/ijerph19052569
Verot E, Bonjean P, Chaux R, Gagnaire J, Gagneux-Brunon A, Pozzetto B, Berthelot P, Botelho-Nevers E, Chauvin F. Development and Validation of the COVID-19 Knowledges and Behavior Questionnaire in a French Population (CoVQuest-CC). International Journal of Environmental Research and Public Health. 2022; 19(5):2569. https://doi.org/10.3390/ijerph19052569
Chicago/Turabian StyleVerot, Elise, Paul Bonjean, Robin Chaux, Julie Gagnaire, Amandine Gagneux-Brunon, Bruno Pozzetto, Philippe Berthelot, Elisabeth Botelho-Nevers, and Franck Chauvin. 2022. "Development and Validation of the COVID-19 Knowledges and Behavior Questionnaire in a French Population (CoVQuest-CC)" International Journal of Environmental Research and Public Health 19, no. 5: 2569. https://doi.org/10.3390/ijerph19052569