
Profiles of Health-Related Patient Activation and Their Determinants: The Results of a Cluster Analysis of Older Adults—Conclusions for Patient Counselling



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analyses
3. Results
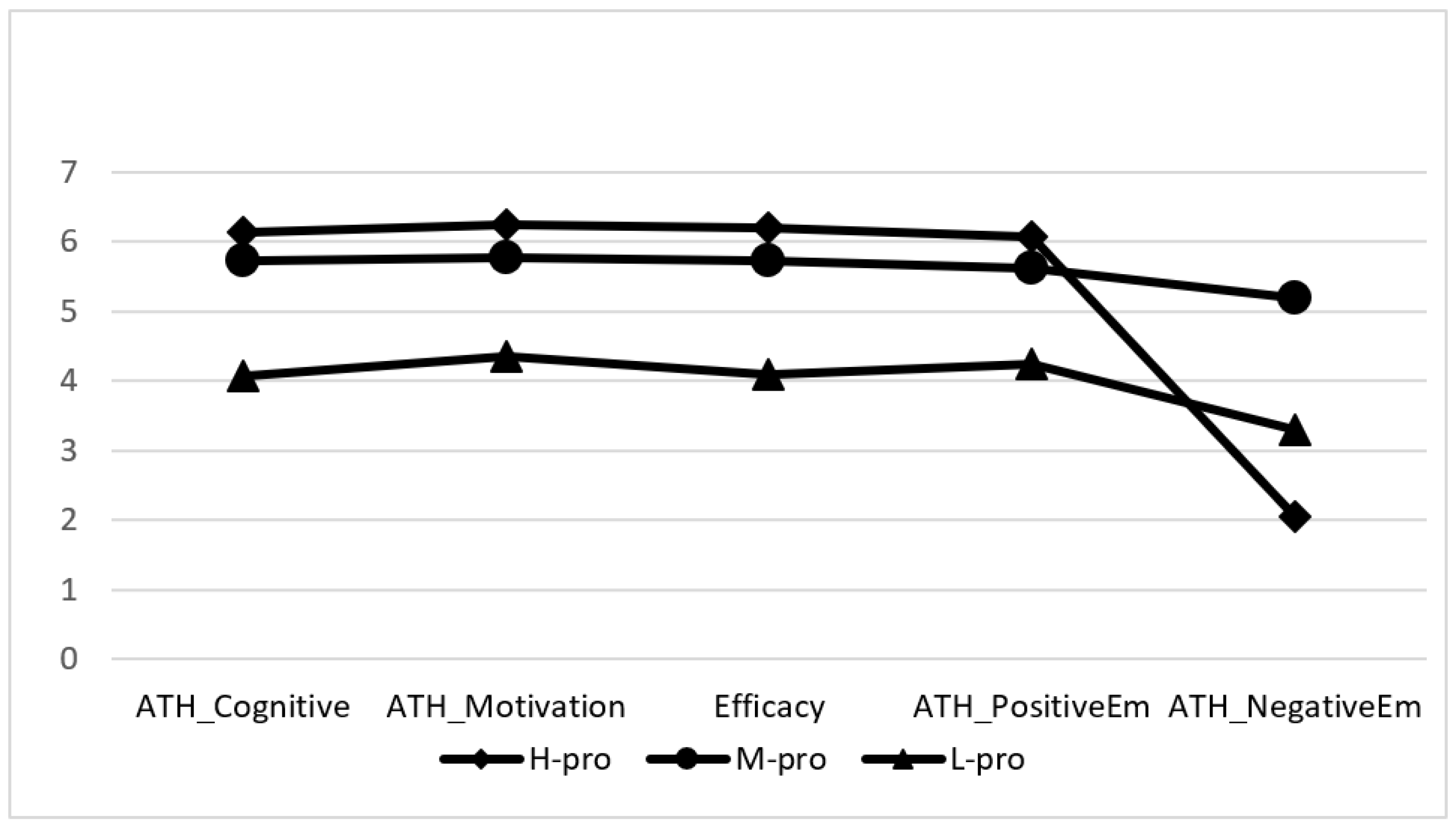
3.1. Characteristics of Health Proactivity Profiles
3.2. Differences between Health Proactivity Profiles according to Sociodemographic Factors
3.3. Differences between Health Proactivity Profiles according to Health Status, Reasons for the Current Visit, and Satisfaction with the Visit
3.4. Differences between Health Proactivity Profiles according to Pre-Visit Expectations and Visit Experiences
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Good Health Adds Life to Years. Global Brief for World Health Day 2012. Available online: http://apps.who.int/ (accessed on 2 February 2017).
- Hibbard, J.H.; Greene, J. What the evidence shows about patient activation: Better health outcomes and care experiences; fewer data on costs. Health Aff. 2013, 32, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Mosen, D.M.; Schmittdiel, J.; Hibbard, J.; Sobel, D.; Remmers, C.; Bellows, J. Is patient activation associated with outcomes of care for adults with chronic conditions? J. Ambul. Care Manag. 2007, 30, 21–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hibbard, J.H.; Mahoney, E. Toward a theory of patient and consumer activation. Patient Educ. Couns. 2010, 78, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Greene, J.; Hibbard, J.H.; Sacks, R.; Overton, V.; Parrotta, C.D. When patient activation levels change, health outcomes and costs change, too. Health Aff. 2015, 34, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Rask, K.J.; Ziemer, D.C.; Kohler, S.A.; Hawley, J.N.; Arinde, F.J.; Barnes, C.S. Patient activation is associated with healthy behaviors and ease in managing diabetes in an indigent population. Diabetes Educ. 2009, 35, 622–630. [Google Scholar] [CrossRef]
- Harvey, L.; Fowles, J.B.; Xi, M.; Terry, P. When activation changes, what else changes? The relationship between change in patient activation measure (PAM) and employees’ health status and health behaviors. Patient Educ. Couns. 2012, 88, 338–343. [Google Scholar] [CrossRef]
- Hendriks, M.; Rademakers, J. Relationships between patient activation, disease-specific knowledge and health outcomes among people with diabetes; a survey study. BMC Health Serv. Res. 2014, 14, 393. [Google Scholar] [CrossRef] [Green Version]
- Shively, M.J.; Gardetto, N.J.; Kodiath, M.F.; Kelly, A.; Smith, T.L.; Stepnowsky, C.; Maynard, C.; Larson, C.B. Effect of patient activation on self-management in patients with heart failure. J. Cardiovasc. Nurs. 2013, 28, 20–34. [Google Scholar] [CrossRef]
- Smith, S.G.; Pandit, A.; Rush, S.R.; Wolf, M.S.; Simon, C.J. The role of patient activation in preferences for shared decision making: Results from a national survey of U.S. adults. J. Health Commun. 2016, 21, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Remmers, C.; Hibbard, J.; Mosen, D.M.; Wagenfield, M.; Hoye, R.E.; Jones, C. Is patient activation associated with future health outcomes and healthcare utilization among patients with diabetes? J. Ambul. Care Manag. 2009, 32, 320–327. [Google Scholar] [CrossRef]
- Graffigna, G.; Barello, S.; Bonanomi, A. The role of patient health engagement model (PHE-model) in affecting patient activation and medication adherence: A structural equation model. PLoS ONE 2017, 12, e0179865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinney, R.L.; Lemon, S.C.; Person, S.D.; Pagoto, S.L.; Saczynski, J.S. The association between patient activation and medication adherence, hospitalization, and emergency room utilization in patients with chronic illnesses: A systematic review. Patient Educ. Couns. 2015, 98, 545–552. [Google Scholar] [CrossRef] [PubMed]
- James, J. Health Affairs. Health Policy Brief. Patient Engagement. 2013. Available online: https://www.healthaffairs.org/do/10.1377/hpb20130214.898775/full/healthpolicybrief_86.pdf (accessed on 29 December 2021).
- Greene, J.; Hibbard, J.H. Why does patient activation matter? An examination of the relationships between patient activation and health-related outcomes. J. Gen. Intern. Med. 2011, 27, 520–526. [Google Scholar] [CrossRef] [Green Version]
- Graffigna, G.; Barello, S.; Bonanomi, A.; Lozza, E. Measuring patient engagement: Development and psychometric properties of the patient health engagement (PHE) scale. Front. Psychol. 2015, 6, 274. [Google Scholar] [CrossRef] [PubMed]
- Menichetti, J.; Cipresso, P.; Bussolin, D.; Graffigna, G. Engaging older people in healthy and active lifestyles: A systematic review. Ageing Soc. 2016, 36, 2036–2060. [Google Scholar] [CrossRef]
- Dattilo, J.; Martire, L.; Gottschall, J.; Weybright, E. A pilot study of an intervention designed to promote walking, balance, and self-efficacy in older adults with fear of falling. Educ. Gerontol. 2014, 40, 26–39. [Google Scholar] [CrossRef]
- Wlodarczyk, D.; Chylinska, J.; Lazarewicz, M.; Rzadkiewicz, M.; Jaworski, M.; Adamus, M.; Haugan, G.; Lillefjell, M.; Espnes, G.A.; Taveira-Gomes, T.; et al. Enhancing doctors’ competencies in communication with and activation of older patients: The promoting active aging (PRACTA) computer-based intervention study. J. Med. Internet Res. 2017, 19, e45. [Google Scholar] [CrossRef] [Green Version]
- Lazarewicz, M.A.; Wlodarczyk, D.; Chylinska, J.; Jaworski, M.; Rzadkiewicz, M.; Adamus, M.; Haugan, G.; Lillefjell, M.; Espnes, G.A. Testing a new tool assessing attitude towards treatment and health in primary health care setting: Senior patients and doctors perspectives. Scand. J. Public Health 2019, 47, 61–69. [Google Scholar] [CrossRef]
- Chylinska, J.; Lazarewicz, M.A.; Rzadkiewicz, M.; Adamus, M.; Jaworski, M.; Haugan, G.; Lillefjel, M.; Espnes, G.A.; Włodarczyk, D. The role of gender in the active attitude toward treatment and health among patients in primary health care-self-assessed health status and sociodemographic factors as moderators. BMC Geriatr. 2017, 17, 284. [Google Scholar] [CrossRef] [Green Version]
- Levy, S.R. Toward reducing ageism: PEACE (Positive Education about Aging and Contact Experiences) model. Gerontologist 2018, 58, 226–232. [Google Scholar] [CrossRef]
- Wyman, M.F.; Shiovitz-Ezra, S.; Bengel, J. Ageism in the health care system: Providers, patients, and systems. In Contemporary Perspectives on Ageism. International Perspectives on Aging; Ayalon, L., Tesch-Römer, C., Eds.; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef] [Green Version]
- Mukhtar, O.; Weinman, J.; Jackson, S.H.D. Intentional non-adherence to medications by older adults. Drugs Aging 2014, 31, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Kvarnström, K.; Airaksinen, M.; Liira, H. Barriers and facilitators to medication adherence: A qualitative study with general practitioners. BMJ Open 2018, 8, e015332. [Google Scholar] [CrossRef] [PubMed]
- Bos-Touwen, I.; Schuurmans, M.; Monninkhof, E.M.; Korpershoek, Y.; Spruit-Bentvelzen, L.; Ertugrul-van der Graaf, I.; de Wit, N.; Trappenburg, J. Patient and disease characteristics associated with activation for self-management in patients with diabetes, chronic obstructive pulmonary disease, chronic heart failure and chronic renal disease: A cross-sectional survey study. PLoS ONE 2015, 10, e0126400. [Google Scholar] [CrossRef]
- Hibbard, J.H.; Cunningham, P.J. How engaged are consumers in their health and health care, and why does it matter? Res. Brief 2008, 8, 1–9. [Google Scholar]
- Skolasky, R.L.; Green, A.F.; Scharfstein, D.; Boult, C.; Reider, L.; Wegener, S.T. Psychometric properties of the patient activation measure among multimorbid older adults. Health Serv. Res. 2011, 46, 457–478. [Google Scholar] [CrossRef]
- Newland, P.; Lorenz, R.; Oliver, B.J. Patient activation in adults with chronic conditions: A systematic review. J. Health Psychol. 2021, 26, 103–114. [Google Scholar] [CrossRef]
- Blakemore, A.; Hann, M.; Howells, K.; Panagioti, M.; Sidaway, M.; Reeves, D.; Bower, P. Patient activation in older people with long-term conditions and multimorbidity: Correlates and change in a cohort study in the United Kingdom. BMC Health Serv. Res. 2016, 16, 58. [Google Scholar] [CrossRef]
- Zimbudzi, E.; Lo, C.; Ranasinha, S.; Fulcher, G.R.; Jan, S.; Kerr, P.G.; Polkinghorne, K.R.; Russell, G.; Walker, R.G.; Zoungas, S. Factors associated with patient activation in an Australian population with comorbid diabetes and chronic kidney disease: A cross-sectional study. BMJ Open 2017, 7, e017695. [Google Scholar] [CrossRef]
- Gerber, L.M.; Barrón, Y.; Mongoven, J.; McDonald, M.; Henriquez, E.; Andreopoulos, E.; Feldman, P.H. Activation among chronically ill older adults with complex medical needs: Challenges to supporting effective self-management. J. Ambul. Care Manag. 2011, 34, 292–303. [Google Scholar] [CrossRef]
- Schinkel, S.; Schouten, B.C.; Street, R.L.; van den Putte, B.; van Weert, J.C.M. Enhancing health communication outcomes among ethnic minority patients: The effects of the match between participation preferences and perceptions and doctor–patient concordance. J. Health Commun. 2016, 21, 1251–1259. [Google Scholar] [CrossRef] [Green Version]
- Stewart, M.; Meredith, L.; Brown, J.B.; Galajda, J. The influence of older patient-physician communication on health and health-related outcomes. Clin. Geriatr. Med. 2000, 16, 25–36. [Google Scholar] [CrossRef]
- Street, R.L., Jr. How clinician-patient communication contributes to health improvement: Modeling pathways from talk to outcome. Patient Educ. Couns. 2013, 92, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Sanders, R.; Araujo, T.B.; Vliegenthart, R.; van Eenbergen, M.C.; van Weert, J.C.M.; Linn, A.J. Patients’ convergence of mass and interpersonal communication on an online forum: Hybrid methods analysis. J. Med. Internet Res. 2020, 22, e18303. [Google Scholar] [CrossRef] [PubMed]
- Jaworski, M.; Rzadkiewicz, M.; Adamus, M.; Chylińska, J.; Lazarewicz, M.; Haugan, G.; Lillefjell, M.; Espnes, G.A.; Wlodarczyk, D. Primary care patients’ expectations regarding medical appointment and their experiences during a visit: Does age matter? Patient Prefer. Adherence 2017, 11, 1121–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rzadkiewicz, M.; Chylińska, J.; Jaworski, M.; Lazarewicz, M.; Adamus, M.; Haugan, G.; Lillefjell, M.; Espnes, G.A.; Wlodarczyk, D. Activation of older patients through intervention for primary healthcare doctors: Does the method matters? Eur. J. Public Health 2017, 27, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Madhulatha, T.S. An overview on clustering methods. IOSR J. Eng. 2012, 2, 719–725. [Google Scholar] [CrossRef]
- Couture, É.M.; Chouinard, M.C.; Fortin, M.; Hudon, C. The relationship between health literacy and patient activation among frequent users of healthcare services: A cross-sectional study. BMC Fam. Pract. 2018, 19, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hibbard, J.H.; Mahoney, E.R.; Stock, R.; Tusler, M. Do increases in patient activation result in improved self-management behaviors? Health Serv. Res. 2007, 42, 1443–1463. [Google Scholar] [CrossRef] [PubMed]
- Adler, R.; Vasiliadis, A.; Bickell, N. The relationship between continuity and patient satisfaction: A systematic review. Fam. Pract. 2010, 27, 171–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Patients Forum. Adherence and Concordance. Position Paper, March 2015. Available online: https://www.eu-patient.eu/globalassets/policy/adherence-compliance-concordance/adherence-paper-final-rev_external.pdf (accessed on 20 November 2021).
- Aung, E.; Donald, M.; Coll, J.R.; Williams, G.M.; Doi, S.A. Association between patient activation and patient-assessed quality of care in type 2 diabetes: Results of a longitudinal study. Health Expect. 2016, 19, 356–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, R.J. Improving health outcomes with better patient understanding and education. Risk Manag. Healthc. Policy. 2010, 3, 61–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greene, J.; Hibbard, J.H.; Sacks, R.; Overton, V. When seeing the same physician, highly activated patients have better care experiences than less activated patients. Health Aff. 2013, 32, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, B.; Ferrer, R.; O’Brien, P.; Watt, G.; Gottlieb, L.; Pinto, A.; Willems, S.; Currie, J.; Harriott, D.; Leitch, J.; et al. Improving equity through primary care: Proceedings of the 2019 Toronto International Conference on Quality in Primary Care. Ann. Fam. Med. 2020, 18, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Black, B.S.; Johnston, D.; Leoutsakos, J.; Reuland, M.; Kelly, J.; Amjad, H.; Davis, K.; Willink, A.; Sloan, D.; Lyketsos, C.; et al. Unmet needs in community-living persons with dementia are common, often non-medical and related to patient and caregiver characteristics. Int. Psychogeriatr. 2019, 31, 1643–1654. [Google Scholar] [CrossRef]
- Mazurek, J.; Szcześniak, D.; Urbańska, K.; Dröes, R.M.; Rymaszewska, J. Met and unmet care needs of older people with dementia living at home: Personal and informal carers’ perspectives. Dementia 2019, 18, 1963–1975. [Google Scholar] [CrossRef]
- Kalánková, D.; Stolt, M.; Scott, P.A.; Papastavrou, E.; Suhonen, R. Unmet care needs of older people: A scoping review. Nurs. Ethics 2021, 28, 149–178. [Google Scholar] [CrossRef]


{kind=link}
| Factor | Level | H-pro | M-pro | L-pro | Test (p) |
|---|---|---|---|---|---|
| Age (M; SD) | 73.65 (5.88) | 72.92 (6.41) | 74.16 (6.51) | F = 9.44 (<0.001) H > M; H = L; M < L * | |
| Gender, n (%) | women | 860 (59) | 495(60) | 656 (60) | chi2 = 0.31 (0.85) |
| man | 603 (41) | 337 (40) | 440 (40) | ||
| Marital status | single | 86 (6) | 50 (6) | 31 (3) | chi2 = 91.16 (<0.001) |
| married | 664 (45) | 459 (2755) | 613 (56) | ||
| divorced | 136 (9) | 42 (5) | 24 (2) | ||
| widowed | 577 (40) | 281 (34) | 428 (39) | ||
| Cohabitation | alone | 597 (41) | 211 (25.8) | 222 (20.6) | chi2 = 140 (<0.001) |
| family | 857 (58.8) | 613 (74) | 866 (79) | ||
| institution | 3 (0.2) | 2 (0.2) | 4 (440.4) | ||
| Place of living | rural area | 90 (6) | 54 (6) | 180 (16) | chi2 = 283.63 (<0.001) |
| below 20,000 | 53 (4) | 67 (8) | 61 (6) | ||
| between 21–100,000 | 170 (12) | 131 (16) | 102 (9) | ||
| between 101–500,000 | 14 (1) | 9 (1) | 51 (5) | ||
| above 500,000 | 457 (31) | 182 (22) | 120 (11) | ||
| capital | 679 (46) | 389 (47) | 582 (53) | ||
| Education | primary | 139 (10) | 90 (11) | 199 (18) | chi2 = 128.31 (<0.001) |
| vocational | 577 (39) | 252 (30) | 366 331) | ||
| Secondary (no diploma) | 219 (15) | 102 (12) | 215 (20) | ||
| Secondary (diploma) | 329 (22) | 235 (28) | 235 (22) | ||
| higher | 199 (14) | 153 (19) | 81 (7) | ||
| Professional status | retired | 1342 (92) | 703 (85) | 947 (86.8) | chi2 = 44.10 (<0.001) |
| working | 104 (7.6) | 106 (13) | 128 (12) | ||
| unemployed | 6 (0.4) | 18 (2) | 9 (0.2) | ||
| Economic status (M;SD) | 3.11 (0.79) | 3.00 (0.86) | 2.78 (0.70) | BF = 57.05 (<0.001) H > M; H > L; M > L * |
| Factor | Level | H-pro | M-pro | L-pro | Test (p) |
|---|---|---|---|---|---|
| Number of diseases (M; SD) | - | 1.88 (0.88) | 1.62 (0.86) | 1.97 (1.87) | F = 23.58 (<0.001) H > M; H = L; M < L * |
| Number of diseases, n (%) | none | 75 (5) | 62 (7) | 93 (8) | chi2 = 89.09 (<0.001) |
| 1 disease | 406 (28) | 313 (38) | 337 (31) | ||
| 2–3 diseases | 634 (43) | 362 (44) | 392 (36) | ||
| 4 or more | 358 (24) | 95 (11) | 274 (25) | ||
| Health service within last 6 months, n (%) | no | 1322 (90) | 743 (89) | 825 (75) | chi2 = 127.85 (<0.001) |
| yes | 141 (10) | 89 (11) | 271 (25) | ||
| SRH (M; SD) | - | 2.89 (0.66) | 3.02 (0.82) | 3.16 (0.68) | 43.38 (<0.001) H < M;H < L; M < L * |
| HIA global | - | 1.74 (0.74) | 1.57 (0.69) | 1.96 (0.81) | 66.17 (<0.001) H > M; H < L; M < L * |
| Aim of the visit, n (%) | treatment | 1389 (95) | 752 (90) | 999 (92) | chi2 = 24.46 (<0.001) |
| formal | 73 (5) | 77 (10) | 90 (8) | ||
| First visit | no | 1424 (44) | 761 (24) | 1012 (32) | chi2 = 54.19 (<0.001) |
| yes | 39 (20) | 71 (37) | 84 (43) | ||
| Attendance length; years (M; SD) | - | 7.28 (4.76) | 6.59 (4.44) | 6.95 (4.33) | 5.71 (<0.001) H > M; H > L; M = L * |
| Attendance last year (M; SD) | - | 1.93 (0.67) | 1.68 (0.82) | 1.58 (0.80) | 74.36 (<0.001) H > M; H > L; M > L * |
| Waiting time from the registration (M; SD) | - | 1.93 (0.99) | 2.41 (1.33) | 1.99 (0.96) | 58.08 (<0.001) H < M; H = L; M > L * |
| Difficulty in registration (M; SD) | - | 2.30 (0.83) | 2.43 (0.95) | 2.72 (0.78) | 76.99 (<0.001) H < M; H < L; M < L * |
| Length of a visit; minutes (M; SD) | - | 21.10 (7.63) | 20.16 (6.83) | 20.00 (7.51) | 7.94 (<0.001) H > M; H > L; M = L * |
| SVS global (M; SD) | - | 6.18 (0.79) | 5.70 (0.73) | 4.72 (0.85) | 1051.40 (<0.001) H > M; H > L; M > L * |
| H-pro | M-pro | L-pro | F | Post Hoc Test * | |
|---|---|---|---|---|---|
| Pre-Visit Expectations | |||||
| Disease Explanation | 6.58 (0.82) | 6.40 (0.74) | 6.47 (0.81) | 14.7 (<0.001) | H > M; H > L; M = L |
| Treatment Explanation | 6.52 (0.81) | 6.23 (0.83) | 6.40 (0.74) | 34.38 (<0.001) | H > M; H > L; M < L |
| Emotional Support | 6.39 (0.97) | 5.91 (1.15) | 6.34 (0.90) | 64.43 (<0.001) | H > M; H = L; M < L |
| Health Promotion | 6.30 (1.02) | 5.50 (1.09) | 6.11 (1.01) | 39.34 (<0.001) | H > M; H > L; M < L |
| Quality of Life | 5.62 (1.74) | 5.06 (1.79) | 5.30 (1.78) | 28.15 (<0.001) | H > M; H > L; M < L |
| Rapport | 6.58 (0.61) | 6.23 (0.77) | 6.32 (0.73) | 78.27 (<0.001) | H > M; H > L; M < L |
| Communication Skills | 6.42 (0.63) | 5.94 (0.71) | 6.11 (0.79) | 137.84 (<0.001) | H > M; H > L; M < L |
| Post-Visit Experiences | |||||
| Disease Explanation | 6.14 (0.93) | 5.68 (0.81) | 4.51 (0.96) | 1018.87 (<0.001) | H > M; H > L; M = L |
| Treatment Explanation | 5.97 (1.08) | 5.60 (0.88) | 4.43 (1.1) | 708.36 (<0.001) | H > M; H > L; M > L |
| Emotional Support | 5.49 (1.04) | 5.54 (0.90) | 4.13 (1.02) | 692.88 (<0.001) | H = M; H > L; M > L |
| Health Promotion | 5.42 (1.06) | 5.43 (1.03) | 4.23 (1.05) | 482.44 (<0.001) | H = M; H > L; M > L |
| Quality of Life | 4.63 (1.63) | 4.84 (1.54) | 2.84 (1.38) | 550.87 (<0.001) | H < M; H > L; M > L |
| Rapport | 5.88 (0.81) | 5.74 (0.82) | 4.92 (1.25) | 325.65 (<0.001) | H > M; H > L; M > L |
| Communication Skills | 6.03 (0.76) | 5.45 (0.71) | 4.43 (0.82) | 1352.98 (<0.001) | H > M; H > L; M > L |
| Post-Pre: Discrepancy between Expectations and Experiences | |||||
| Disease Explanation | −0.44 (0.85) | −0.72 (1.01) | −1.95 (1.15) | 772.18 (<0.001) | H > M; H > L; M > L |
| Treatment Explanation | −0.54 (0.97) | −0.62 (1.09) | −1.96 (1.23) | 596.70 (<0.001) | H = M; H > L; M > L |
| Emotional Support | −0.89 (1.29) | −0.37 (1.42) | −2.20 (1.30) | 511.24 (<0.001) | H < M; H > L; M > L |
| Health Promotion | −0.87 (1.23) | −0.47 (1.35) | −1.88 (1.22) | 338.33 (<0.001) | H < M; H > L; M > L |
| Quality of Life | −0.99 (1.76) | −0.22 (2.09) | −2.46 (1.98) | 349.42 (<0.001) | H < M; H > L; M > L |
| Rapport | −0.69 (0.95) | −0.49 (1.01) | −1.40 (1.21) | 212.22 (<0.001) | H < M; H > L; M > L |
| Communication Skills | −0.39 (.68) | −0.48 (0.84) | −1.69 (0.94) | 891.86 (<0.001) | H > M; H > L; M > L |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Włodarczyk, D.; Chylińska, J. Profiles of Health-Related Patient Activation and Their Determinants: The Results of a Cluster Analysis of Older Adults—Conclusions for Patient Counselling. Int. J. Environ. Res. Public Health 2022, 19, 2487. https://doi.org/10.3390/ijerph19042487
Włodarczyk D, Chylińska J. Profiles of Health-Related Patient Activation and Their Determinants: The Results of a Cluster Analysis of Older Adults—Conclusions for Patient Counselling. International Journal of Environmental Research and Public Health. 2022; 19(4):2487. https://doi.org/10.3390/ijerph19042487
Chicago/Turabian StyleWłodarczyk, Dorota, and Joanna Chylińska. 2022. "Profiles of Health-Related Patient Activation and Their Determinants: The Results of a Cluster Analysis of Older Adults—Conclusions for Patient Counselling" International Journal of Environmental Research and Public Health 19, no. 4: 2487. https://doi.org/10.3390/ijerph19042487