
Bacterial Coinfections Increase Mortality of Severely Ill COVID-19 Patients in Saudi Arabia

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Ethical Approval
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Patients’ Characteristics
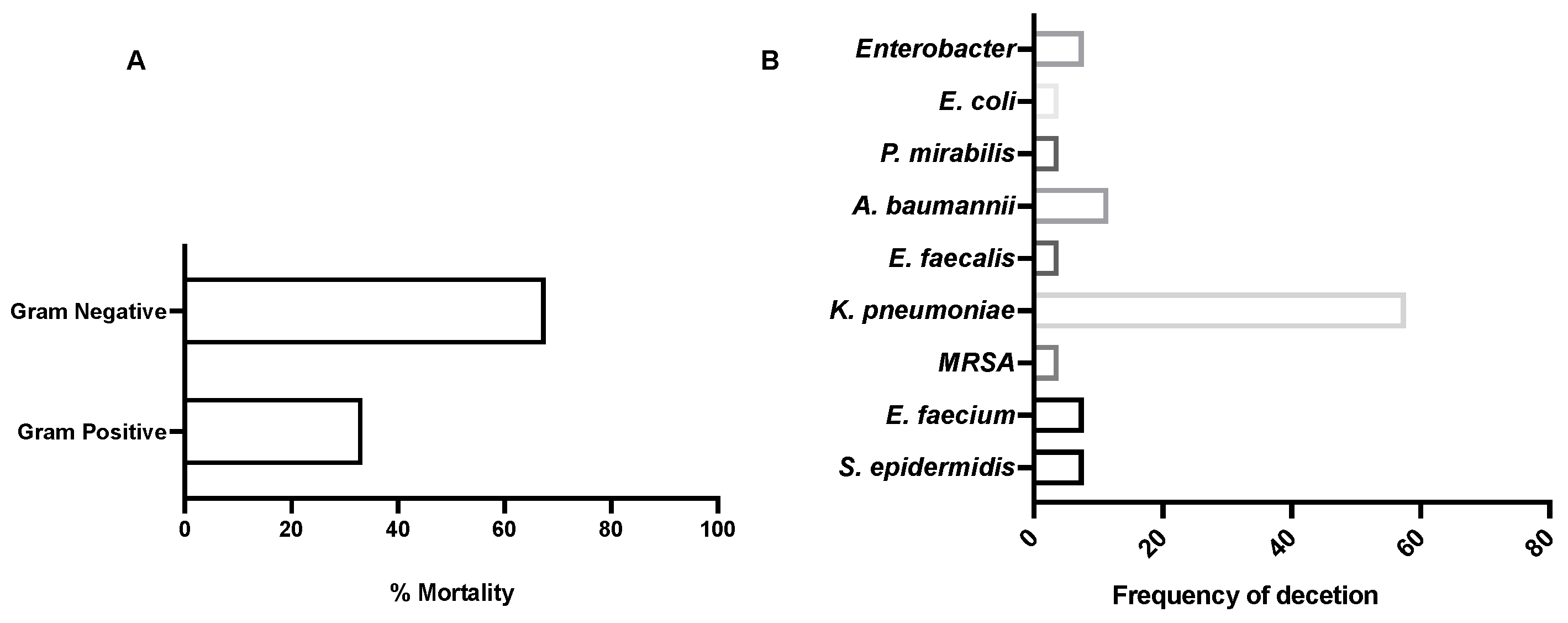
3.2. Bacterial Isolation and Antimicrobial Resistance Patterns
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Weekly Epidemiological Update. 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---31-august-2021 (accessed on 3 January 2022).
- Eurosurveillance Editorial Team. Updated rapid risk assessment from ECDC on the risk related to the spread of new SARS-CoV-2 variants of concern in the EU/EEA-first update. Eurosurveillance 2021, 26, 2101211. [Google Scholar] [CrossRef]
- Guan, W.-j.; Ni, Z.-y.; Hu, Y.; Liang, W.-h.; Ou, C.-q.; He, J.-x.; Liu, L.; Shan, H.; Lei, C.-l.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.; Lima, C.; Magalhães, V.; Baltazar, L.; Peres, N.; Caligiorne, R.; Moura, A.; Fereguetti, T.; Martins, J.; Rabelo, L.; et al. Fungal and bacterial coinfections increase mortality of severely ill COVID-19 patients. J. Hosp. Infect. 2021, 113, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.R.; Sheng, Z.M.; Ely, S.F.; Guinee, D.G., Jr.; Beasley, M.B.; Suh, J.; Deshpande, C.; Mollura, D.J.; Morens, D.M.; Bray, M.; et al. Pulmonary pathologic findings of fatal 2009 pandemic influenza A/H1N1 viral infections. Arch. Pathol. Lab. Med. 2010, 134, 235–243. [Google Scholar] [CrossRef]
- Bisno, A.L.; Griffin, J.P.; VAN Epps, K.A.; Niell, H.B.; Rytel, M.W. Pneumonia and Hong Kong influenza: A prospective study of the 1968–1969 epidemic. Am. J. Med. Sci. 1971, 261, 251–263. [Google Scholar] [CrossRef]
- Hers, J.; Masurel, N.; Mulder, J. Bacteriology and histopathology of the respiratory tract and lungs in fatal Asian influenza. Lancet 1958, 272, 1141–1143. [Google Scholar] [CrossRef]
- Brundage, J.F.; Shanks, G.D. Deaths from Bacterial Pneumonia during 1918–19 Influenza Pandemic. Emerg. Infect. Dis. 2008, 14, 1193–1199. [Google Scholar] [CrossRef]
- Cillóniz, C.; Ewig, S.; Menéndez, R.; Ferrer, M.; Polverino, E.; Reyes, S.; Gabarrús, A.; Marcos, M.A.; Cordoba, J.; Mensa, J.; et al. Bacterial co-infection with H1N1 infection in patients admitted with community acquired pneumonia. J. Infect. 2012, 65, 223–230. [Google Scholar] [CrossRef]
- McCullers, J.A. The co-pathogenesis of influenza viruses with bacteria in the lung. Nat. Rev. Genet. 2014, 12, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Hanada, S.; Pirzadeh, M.; Carver, K.Y.; Deng, J.C. Respiratory Viral Infection-Induced Microbiome Alterations and Secondary Bacterial Pneumonia. Front. Immunol. 2018, 9, 2640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersdorf, R.G. Pulmonary Infections Complicating Asian Influenza. Arch. Intern. Med. 1959, 103, 262–272. [Google Scholar] [CrossRef]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L.S.P. Bacterial and fungal coinfection among hospitalized patients with COVID-19: A retrospective cohort study in a UK secondary-care setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A.H. Bacterial and Fungal Coinfection in Individuals with Coronavirus: A Rapid Review To Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Liu, W.; Jiang, M.; Huang, P.; Xiang, Z.; Deng, D.; Chen, P.; Xie, L. Clinical characteristics of COVID-19 patients with clinically diagnosed bacterial co-infection: A multi-center study. PLoS ONE 2021, 16, e0249668. [Google Scholar] [CrossRef]
- Elabbadi, A.; Turpin, M.; Gerotziafas, G.T.; Teulier, M.; Voiriot, G.; Fartoukh, M. Bacterial coinfection in critically ill COVID-19 patients with severe pneumonia. Infection 2021, 49, 559–562. [Google Scholar] [CrossRef] [PubMed]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Flandre, P.L.; Dubert, M.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H.; et al. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann. Intensiv. Care 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Baskaran, V.; Lawrence, H.; Lansbury, L.E.; Webb, K.; Safavi, S.; Zainuddin, N.I.; Huq, T.; Eggleston, C.; Ellis, J.; Thakker, C.; et al. Co-infection in critically ill patients with COVID-19: An observational cohort study from England. J. Med. Microbiol. 2021, 70, 001350. [Google Scholar] [CrossRef]
- Fu, Y.; Yang, Q.; Xu, M.; Kong, H.; Chen, H.; Fu, Y.; Yao, Y.; Zhou, H.; Zhou, J. Secondary Bacterial Infections in Critical Ill Patients With Coronavirus Disease 2019. Open Forum Infect. Dis. 2020, 7, ofaa220. [Google Scholar] [CrossRef]
- Mahmoudi, H. Bacterial co-infections and antibiotic resistance in patients with COVID-19. GMS. Hyg. Infect. Control 2020, 15, Doc35. [Google Scholar] [CrossRef]
- Feng, Y.; Ling, Y.; Bai, T.; Xie, Y.; Huang, J.; Li, J.; Xiong, W.; Yang, D.; Chen, R.; Lu, F.; et al. COVID-19 with Different Severities: A Multicenter Study of Clinical Features. Am. J. Respir. Crit. Care Med. 2020, 201, 1380–1388. [Google Scholar] [CrossRef] [PubMed]
- Chertow, D.S.; Memoli, M.J. Bacterial Coinfection in Influenza. JAMA 2013, 309, 275–282. [Google Scholar] [CrossRef]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influ. Other Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finelli, L.; Fiore, A.; Dhara, R.; Brammer, L.; Shay, D.K.; Kamimoto, L.; Fry, A.; Hageman, J.; Gorwitz, R.; Bresee, J.; et al. Influenza-Associated Pediatric Mortality in the United States: Increase of Staphylococcus aureus Coinfection. Pediatrics 2008, 122, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Cui, W.; Zhao, H.; Lu, X.; Wen, Y.; Zhou, Y.; Deng, B.; Wang, Y.; Wang, W.; Kang, J.; Liu, P. Factors associated with death in hospitalized pneumonia patients with 2009 H1N1 influenza in Shenyang, China. BMC Infect. Dis. 2010, 10, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahariadis, G.; Gooley, T.A.; Ryall, P.; Hutchinson, C.; Latchford, M.I.; Fearon, M.A.; Jamieson, F.B.; Richardson, S.; Kuschak, T.; Mederski, B. Risk of Ruling out Severe Acute Respiratory Syndrome by Ruling in another Diagnosis: Variable Incidence of Atypical Bacteria Coinfection Based on Diagnostic Assays. Can. Respir. J. 2006, 13, 17–22. [Google Scholar] [CrossRef]
- Lee, N.; Hui, D.; Wu, A.; Chan, P.; Cameron, P.; Joynt, G.M.; Ahuja, A.; Yung, M.Y.; Leung, C.; To, K.; et al. A Major Outbreak of Severe Acute Respiratory Syndrome in Hong Kong. N. Engl. J. Med. 2003, 348, 1986–1994. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Merad, M.; Martin, J.C. Pathological inflammation in patients with COVID-19: A key role for monocytes and macrophages. Nat. Rev. Immunol. 2020, 20, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Liu, Z.; Chen, Y.; Xiao, Y.; Huang, X.; Fan, X.-G. Bacterial and fungal infections in COVID-19 patients: A matter of concern. Infect. Control Hosp. Epidemiol. 2020, 41, 1124–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2020, 27, 83–88. [Google Scholar] [CrossRef]
- Melvin, P.; Weinstein, M.D. M100 Performance Standard for Antimicrobial Susceptibility Testing, 30th ed.; Clinical and Laboratory Standards Institute: Malvern, PA, USA, 2020. [Google Scholar]
- CDC. Types of Healthcare-Associated Infections. 2014. Available online: https://www.cdc.gov/hai/infectiontypes.html (accessed on 3 January 2021).
- Frater, J.L.; Zini, G.; D’Onofrio, G.; Rogers, H.J. COVID-19 and the clinical hematology laboratory. Int. J. Lab. Hematol. 2020, 42, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Wang, J.; Yang, Y.; Cai, P.; Cao, J.; Cai, X.; Zhang, Y. Etiology and antimicrobial resistance of secondary bacterial infections in patients hospitalized with COVID-19 in Wuhan, China: A retrospective analysis. Antimicrob. Resist. Infect. Control 2020, 9, 1–7. [Google Scholar] [CrossRef] [PubMed]
- MacVane, S.H. Antimicrobial Resistance in the Intensive Care Unit: A Focus on Gram-Negative Bacterial Infections. J. Intensive Care Med. 2017, 32, 25–37. [Google Scholar] [CrossRef]
- Arteaga-Livias, K.; Pinzas-Acosta, K.; Perez-Abad, L.; Panduro-Correa, V.; Rabaan, A.A.; Pecho-Silva, S.; Dámaso-Mata, B. A multidrug-resistant Klebsiella pneumoniae outbreak in a Peruvian hospital: Another threat from the COVID-19 pandemic. Infect. Control Hosp. Epidemiol. 2021, 1–2. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | All Patients (n = 34) | SARS-CoV-2 (n = 16) (47%) | SARS-CoV-2/Bacterial Coinfection (n = 18) (53%) | p-Value |
|---|---|---|---|---|
| Age (years), median | 64 | 66 | 63 | 0.6892 |
| Gender, n (%) | ||||
| Male | 27 (79.5) | 13 (81.25) | 14 (77.7) | 0.8315 |
| Female | 7 (20.5) | 3 (18.75) | 4 (22.3) | |
| Mortality, (%) | 35.2 | 18.7 | 50 | 0.0589 |
| Length of stay in ICU, days, (mean) | 25.7 | 16.2 | 35.2 | 0.0001 * |
| Sample site | Bacterial investigations undertaken (n) | |||
| Blood | 14 | 1 | 11 | |
| Sputum | 8 | 3 | 5 | |
| Lung lavage | 1 | 0 | 1 | |
| Endotracheal Tube | 7 | 2 | 5 | |
| Urine | 10 | 7 | 3 | |
| Throat Swab | 4 | 3 | 1 | |
| Bronchial Secretion | 1 | 1 | 0 | |
| Parameter | Patients with No Bacterial Infection (n = 16) (47%) | Patients with Bacterial Infection (n = 18) (53%) | p-Values |
|---|---|---|---|
| ALT (U/L) | 72.3 ± 69.9 | 94.04 ± 126.3 | 0.5867 |
| AST (U/L) | 104.7 ±174.1 | 132 ± 274 | 0.7563 |
| Urea (mg/dL) | 70.96 ± 73.2 | 132.3 ± 108.6 | 0.0422 * |
| Random blood sugar (RBS) (mg/dL) | 249.8 ±174.2 | 153.5 ± 74.7 | 0.0428 * |
| Creatinine (mg/dL) | 1.882 ± 2.6 | 1.858 ± 1.38 | 0.9734 |
| Potassium Mmol/L | 4.581 ±1.23 | 4.282 ± 0.69 | 0.3971 |
| Activated Partial Thromboplastin Time (APTT) (Seconds) | 50.79 ±46.22 | 65.34 ± 39.36 | 0.3852 |
| Prothrombin Time (Seconds) | 19.44 ± 14.75 | 18.78 ± 9.86 | 0.8905 |
| WBCs (103/μL) | 13.26 ± 11.9 | 15.64 ± 18.76 | 0.6675 |
| RBCs (106/μL) | 4.308 ± 1.1 | 2.920 ± 0.68 | <0.0001 * |
| Hemoglobin (g/dL) | 12.63 ± 5.58 | 8.100 ± 1.88 | 0.0028 * |
| Hematocrit (%) | 39.01 ± 14.59 | 26.04 ± 6.39 | 0.0017 * |
| MCV (fl) | 79.85 ± 15.18 | 89.08 ± 7.19 | 0.0276 * |
| MCH (pg) | 26.78 ± 2.8 | 27.74 ± 1.9 | 0.2466 |
| MCHC (g/dL) | 44.55 ± 5.3 | 31.26 ± 2.1 | 0.2799 |
| Platelets (103/μL) | 209.0 ± 125.1 | 106.2 ± 86 | 0.0082 * |
| RDW (fL) | 45.14 ± 12.6 | 54.08 ± 13.3 | 0.0543 |
| Neutrophils (%) | 72.32 ± 26.6 | 82.72 ± 15.3 | 0.1664 |
| Absolute Neutrophils (103/UL) | 8.946 ± 7.6 | 14.08 ± 18.6 | 0.3118 |
| Lymphocytes (%) | 14.62 ± 17 | 8.144 ± 8 | 0.1590 |
| Absolute Lymphocyte Count (103/μL) | 2.348 ± 4.2 | 0.7372 ± 0.59 | 0.1243 |
| Monocytes (%) | 5.162 ± 3.7 | 4.017 ± 2.6 | 0.3054 |
| Absolute monocytes (103/μL) | 0.6500 ± 0.68 | 0.4933 ± 0.40 | 0.4141 |
| Eosinophils (%) | 1.609 ± 2.7 | 4.817 ± 13.7 | 0.3661 |
| Basophils (%) | 0.5775 ± 0.93 | 0.3118 ± 0.3 | 0.2742 |
| Neutrophil Lymphocyte Ratio (NLR) | 9.4 ± 68.1 | 16.6 ± 59.67 | 0.7431 |
| Bacterial Species (n = 9) | Bacteria | Sample Site (n = Frequency) |
|---|---|---|
| Gram-positive (n = 4, 44.4%) | Staphylococcus epidermidis | Blood (2) |
| Enterococcus faecium | Blood (3) | |
| MRSA | Blood (1) | |
| Enterococcus faecalis | Blood (1) | |
| Gram-negative (n = 5, 55.6%) | Acinetobacter baumannii | Blood (2), throat swab (1) |
| Klebsiella pneumoniae | Blood (3), sputum (4), endotracheal tube (3), urine (2) | |
| Proteus mirabilis | Lung lavage (1) | |
| E. coli | Urine (1) | |
| Enterobacter | Sputum (1), endotracheal tube (1) |
| Patients ID (n = 8 (44.4%)) | Sample Site | Bacteria |
|---|---|---|
| 1 | Blood | Acinetobacter baumannii |
| Sputum | Klebsiella pneumoniae | |
| 2 | Blood | Staphylococcus epidermidis |
| Lung lavage | Proteus mirabilis | |
| 3 | Blood | Enterococcus faecalis |
| Endo Tracheal Tube | Acinetobacter baumannii | |
| 4 | Blood | Klebsiella pneumoniae |
| Sputum | Klebsiella pneumoniae | |
| 5 | Blood | Klebsiella pneumoniae |
| Sputum | Klebsiella pneumoniae | |
| 6 | Blood | Klebsiella pneumoniae |
| Endo Tracheal Tube | Klebsiella pneumoniae | |
| 7 | Urine | E. coli |
| Endo Tracheal Tube | Klebsiella pneumoniae | |
| 8 | Urine | Klebsiella pneumoniae |
| Endo Tracheal Tube | Klebsiella pneumoniae |
| Antibiotics Used for Screening Gram-Positive Bacteria | Antibiotics Used for Screening Gram-Negative Bacteria |
|---|---|
| Ampicillin | Amikacin |
| Azithromycin | amoxicillin and clavulanic acid |
| Ciprofloxacin | Ampicillin/Sulbactam |
| Clindamycin | Aztreonam |
| Daptomycin | Cefepime |
| Erythromycin | Cefotaxime |
| Fosfomycin | Cefoxitin |
| Fusidic Acid | Ceftazidime |
| Gentamicin | Ceftriaxone |
| Levofloxacin | Cefuroxime |
| Linezolid | Ciprofloxacin |
| Moxifloxacin | Colistin |
| Mupirocin | Ertapenem |
| Nitrofurantoin | Gentamicin |
| Oxacillin | Imipenem |
| Penicillin | Levofloxacin |
| Rifampin | Meropenem |
| Sulfamethoxazole and trimethoprim | Minocycline |
| Synercid | Moxifloxacin |
| Teicoplanin | Nitrofurantoin |
| Tetracyclin | Piperacillin/tazobactam |
| Tigecycline | Sulfamethoxazole and trimethoprim |
| Vancomycin | Tigecycline |
| Tobramycin |
| Antibiotics/Isolates (n) | A. baumannii (4) | Enterobacter spp. (2) | K. pneumoniae (12) | E. coli (1) | P. mirabilis (1) |
|---|---|---|---|---|---|
| Gentamicin | 100% | 50% | 75% | 100% | 100% |
| Amikacin | 75% | 50% | 75% | 0% | 0% |
| Tobramycin | 75% | 100% | 100% | 0% | 0% |
| amoxicillin and clavulanic acid | 100% | 100% | 100% | 100% | 0% |
| Ampicillin/Sulbactam | 25% | 100% | 100% | 100% | 0% |
| Cefepime | 100% | 100% | 100% | 100% | 0% |
| Cefotaxime | 100% | 100% | 100% | 100% | 0% |
| Cefoxitin | 100% | 100% | 100% | 100% | 0% |
| Ceftazidime | 100% | 100% | 100% | 100% | 0% |
| Ceftriaxone | 100% | 100% | 100% | 100% | 0% |
| Cefuroxime | 100% | 100% | 100% | 100% | 0% |
| Piperacillin/tazobactam | 100% | 100% | 92% | 0% | 0% |
| Ciprofloxacin | 100% | 50% | 100% | 100% | 0% |
| Levofloxacin | 100% | 50% | 100% | 100% | 100% |
| Ertapenem | 100% | 50% | 100% | 0% | 0% |
| Imipenem | 100% | 50% | 50% | 0% | 0% |
| Meropenem | 100% | 50% | 100% | 0% | 0% |
| Tigecycline | 50% | 0% | 0% | 0% | 0% |
| Colistin | 0% | 50% | 50% | 0% | 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, A.; Alamer, E.; Mir, M.; Alasmari, A.; Alshahrani, M.M.; Asiri, M.; Ahmad, I.; Alhazmi, A.; Algaissi, A. Bacterial Coinfections Increase Mortality of Severely Ill COVID-19 Patients in Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 2424. https://doi.org/10.3390/ijerph19042424
Alqahtani A, Alamer E, Mir M, Alasmari A, Alshahrani MM, Asiri M, Ahmad I, Alhazmi A, Algaissi A. Bacterial Coinfections Increase Mortality of Severely Ill COVID-19 Patients in Saudi Arabia. International Journal of Environmental Research and Public Health. 2022; 19(4):2424. https://doi.org/10.3390/ijerph19042424
Chicago/Turabian StyleAlqahtani, Abdulaziz, Edrous Alamer, Mushtaq Mir, Ali Alasmari, Mohammed Merae Alshahrani, Mohammed Asiri, Irfan Ahmad, Abdulaziz Alhazmi, and Abdullah Algaissi. 2022. "Bacterial Coinfections Increase Mortality of Severely Ill COVID-19 Patients in Saudi Arabia" International Journal of Environmental Research and Public Health 19, no. 4: 2424. https://doi.org/10.3390/ijerph19042424