
Did COVID-19-Related Alcohol Sales Restrictions Reduce Alcohol Consumption? Findings from a National Online Survey in South Africa

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Type of Study
2.2. Population and Sample
2.3. Instrument and Procedure
2.4. Statistics
2.5. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Johns Hopkins University. COVID-19 Data Repository by the Center for Systems Science and Engineering (CSSE). Available online: https://github.com/CSSEGISandData/COVID-19 (accessed on 19 November 2021).
- Zuma, N.D. Declaration of a national state of disaster. In 43096, Affairs; Department of cooperative governance and traditional affairs. Eds.: Pretoria, South Africa, 2020; Volume 313. [Google Scholar]
- Zuma, N.D. Disaster management act, 2002: Amendment of regulations issued in terms of section 27(2). In 43148, Affairs; Department of cooperative governance and traditional affairs Eds.: Pretoria, South Africa, 2020; Volume 11B, p. 6. [Google Scholar]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Man, J.; Smith, M.R.; Schneider, M.; Tabana, H. An exploration of the impact of COVID-19 on mental health in South Africa. Psychol. Health Med. 2021, 27, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Zuma, N.D. Disaster managment act 2002: Amendment of regulations issued in terms of sections 27(2). In 44838, Governance; Department of cooperative governance and traditional affairs. Eds.: Pretoria, South Africa, 2020; Volume 610. [Google Scholar]
- Ndlovu, H. Four Things You Need to Know About the Illegal Alcohol Trade. In South African Food Review, SyndiGate Media Inc.: 2020. Available online: https://www.b2bcentral.co.za/four-things-you-need-to-know-about-the-illegal-alcohol-trade/ (accessed on 21 October 2021).
- WHO. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Harker, N.; Londani, M.; Morojele, N.; Petersen Williams, P.; Parry, C.D. Characteristics and Predictors of Heavy Episodic Drinking (HED) among Young People Aged 16–25: The International Alcohol Control Study (IAC), Tshwane, South Africa. Int. J. Environ. Res. 2020, 17, 3537. [Google Scholar] [CrossRef]
- National Department of Health (NDoH); Statistics South Africa (Stats SA); South African Medical Research Council (SAMRC); ICF. South Africa Demographic and Health Survey 2016; 2019. Available online: https://dhsprogram.com/pubs/pdf/FR337/FR337.pdf (accessed on 21 October 2021).
- Degenhardt, L.; Charlson, F.; Ferrari, A.; Santomauro, D.; Erskine, H.; Mantilla-Herrara, A.; Whiteford, H.; Leung, J.; Naghavi, M.; Griswold, M. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry 2018, 5, 987–1012. [Google Scholar] [CrossRef] [Green Version]
- Chu, K.M.; Marco, J.L.; Owolabi, E.O.; Duvenage, R.; Londani, M.; Lombard, C.; Parry, C.D. Trauma trends during COVID-19 alcohol prohibition at a South African regional hospital. Drug Alcohol Rev. 2022, 41, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Moultrie, T.; Dorrington, R.; Laubscher, R.; Groenewald, P.; Parry, C.; Matzopoulos, R.; Bradshaw, D. Unnatural deaths, alcohol bans and curfews: Evidence from a quasi-natural experiment during COVID-19. S. Afr. Med. J. 2021, 111, 834–837. [Google Scholar] [CrossRef] [PubMed]
- Matzopoulos, R.G.; Truen, S.; Bowman, B.; Corrigall, J. The cost of harmful alcohol use in South Africa. S. Afr. Med. J. 2014, 104, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Stats, S.A. Economic Growth. Available online: http://www.statssa.gov.za/?p=14660 (accessed on 21 October 2021).
- Shield, K.D.; Parry, C.; Rehm, J. Chronic diseases and conditions related to alcohol use. Alcohol Res. Health 2014, 35, 155. [Google Scholar]
- Probst, C.; Parry, C.D.; Wittchen, H.-U.; Rehm, J. The socioeconomic profile of alcohol-attributable mortality in South Africa: A modelling study. BMC Med. 2018, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dean, A.S.; Sullivan, K.M.; Soe, M.M. OpenEpi: Open Source Epidemiologic Statistics for Public Health, Version. Available online: https://www.openepi.com/SampleSize/SSPropor.htm (accessed on 10 September 2020).
- Corporation, M. Microsoft Excel; Microsoft Corporation: Irving, TX, USA, 2018. [Google Scholar]
- Corp. I. IBM SPSS Statistics for Windows, 27.0; IBM Corp: Armonk, NY, USA, 2020. [Google Scholar]
- StataCorp. Stata Statistical Software, 17; StataCorp LLC.: College Station, TX, USA, 2021. [Google Scholar]
- Trangenstein, P.J.; Morojele, N.K.; Lombard, C.; Jernigan, D.H.; Parry, C.D. Heavy drinking and contextual risk factors among adults in South Africa: Findings from the International Alcohol Control study. Subst. Abus. Treat. Prev. Policy 2018, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Parry, C.D.; Morojele, N.K.; Myers, B.J.; Kekwaletswe, C.T.; Manda, S.O.; Sorsdahl, K.; Ramjee, G.; Hahn, J.A.; Rehm, J.; Shuper, P.A. Efficacy of an alcohol-focused intervention for improving adherence to antiretroviral therapy (ART) and HIV treatment outcomes–a randomised controlled trial protocol. BMC Infect. Dis. 2014, 14, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, B.; Carney, T.; Rooney, J.; Malatesta, S.; White, L.F.; Parry, C.D.; Bouton, T.C.; Ragan, E.J.; Horsburgh, C.R.; Warren, R.M. Alcohol and Tobacco Use in a Tuberculosis Treatment Cohort during South Africa’s COVID-19 Sales Bans: A Case Series. Int. J. Environ. Res. 2021, 18, 5449. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.R.; Ackerman, J.M.; Wolfson, J.A.; Gearhardt, A.N. COVID-19 stress and eating and drinking behaviors in the United States during the early stages of the pandemic. Appetite 2021, 162, 105163. [Google Scholar] [CrossRef] [PubMed]
- Greyling, T.; Rossouw, S.; Adhikari, T. The good, the bad and the ugly of lockdowns during COVID-19. PLoS ONE 2021, 16, e0245546. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Budlender, J.; Zizzamia, R.; Bassier, I. The Labor Market and Poverty Impacts of COVID-19 in South Africa; Cape Town: SALDRU, UCT. (SALDRU Working Paper No. 264); 2020. Available online: http://www.opensaldru.uct.ac.za/bitstream/handle/11090/980/2020_264_Saldruwp.pdf?sequence=1 (accessed on 21 October 2021).
- Gibbs, N.; Angus, C.; Dixon, S.; Parry, C.; Meier, P. Effects of minimum unit pricing for alcohol in South Africa across different drinker groups and wealth quintiles: A modelling study. BMJ Open 2021, 11, e052879. [Google Scholar] [CrossRef] [PubMed]
- Maluleke, R. Inequality Trends in South Africa. A Multidimensional Diagnostic of Inequality. Statistics South Africa 2019. Available online: https://www.statssa.gov.za/publications/Report-03-10-19/Report-03-10-192017.pdf (accessed on 10 October 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domains | Variables | Measures |
|---|---|---|
| Socio-demographics | Date of birth | Numerical input (year of birth) |
| Sex | Male | |
| Female | ||
| Ethnicity | Black African | |
| Coloured | ||
| White | ||
| Asian/other | ||
| Province of residence | Eastern Cape | |
| Free State | ||
| Gauteng | ||
| Kwazulu-Natal | ||
| Mpumalanga | ||
| Limpopo | ||
| Northern Cape | ||
| North West | ||
| Western Cape | ||
| Change in monthly household income during COVID-19 | Decreased income | |
| No change | ||
| Increased income | ||
| Aged 70+, serious medical condition, or immunocompromised | Yes | |
| No | ||
| COVID-19 pandemic restrictions at the time of completing the survey | 1 Total restriction | |
| 2 Very restricted | ||
| 3 Moderate restriction | ||
| 4 Limited restriction | ||
| 5 Social distancing only | ||
| 6 No restriction | ||
| consumption, prevalence of HED, illegal alcohol purchasing and effect of alcohol on reducing drinking and social distancing of males and females that consume alcohol | Frequency of alcohol consumption | ≥1 times per day |
| 1–6 times a week | ||
| 1–4 times per month | ||
| Less than once a month | ||
| 1–3 times per year | ||
| Classified as heavy episodic drinkers * | Yes | |
| No | ||
| Heavy episodic drinking frequency | Daily | |
| Weekly | ||
| Monthly | ||
| Less than monthly | ||
| Illegal alcohol purchasing | Yes | |
| No | ||
| First time buying alcohol illegally | Yes | |
| No | ||
| Restrictions made it harder to cut down on drinking | Yes | |
| No | ||
| Alcohol makes social/physical distancing more difficult | Yes | |
| No | ||
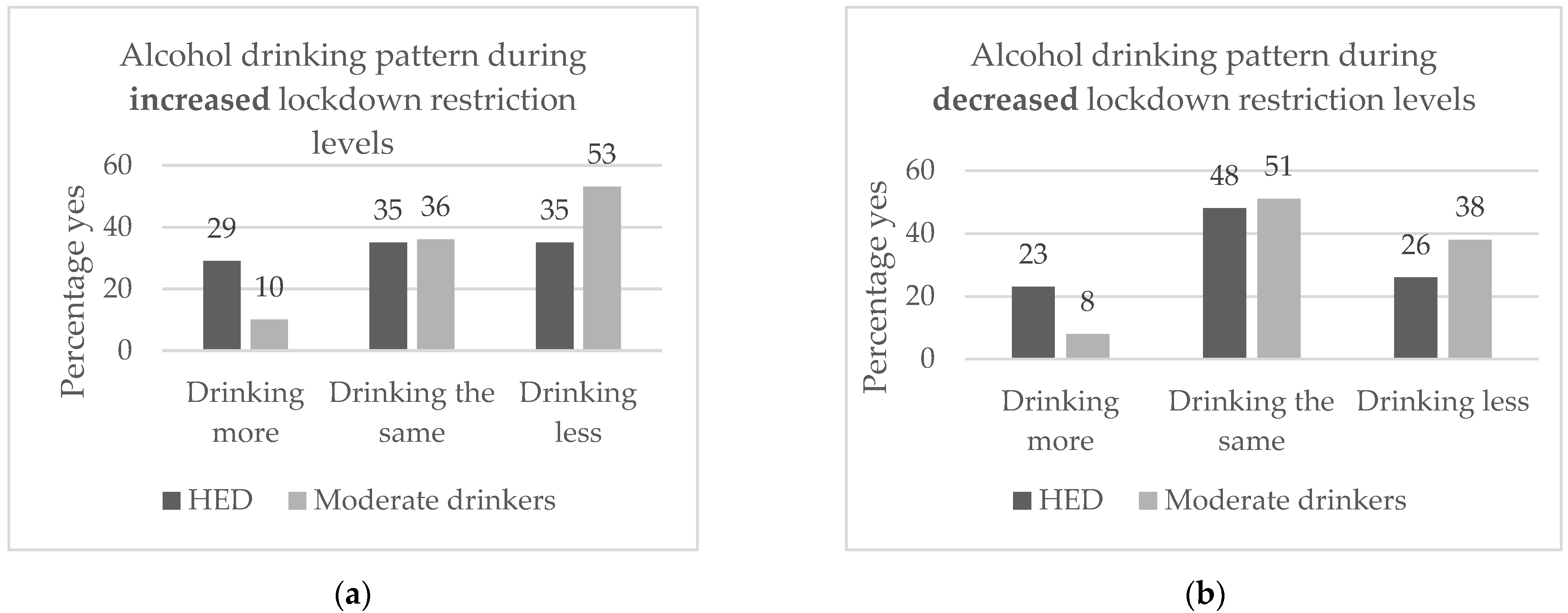
| Pattern of alcohol consumption during increased and decreased levels of lockdown | During the COVID-19 pandemic restrictions, did your drinking change from your usual level as the restrictions? | Drinking more |
| Drinking the same | ||
| Drinking less | ||
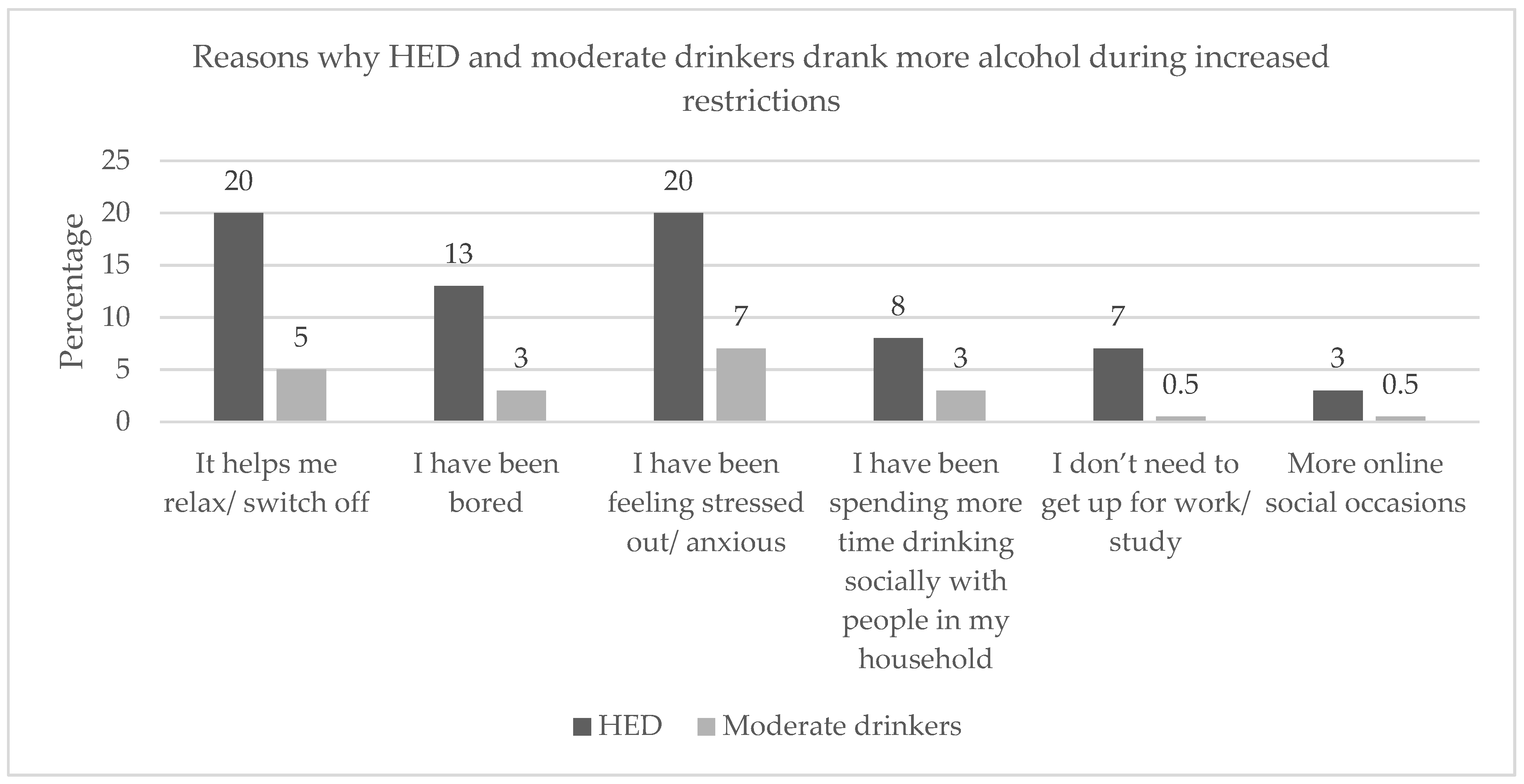
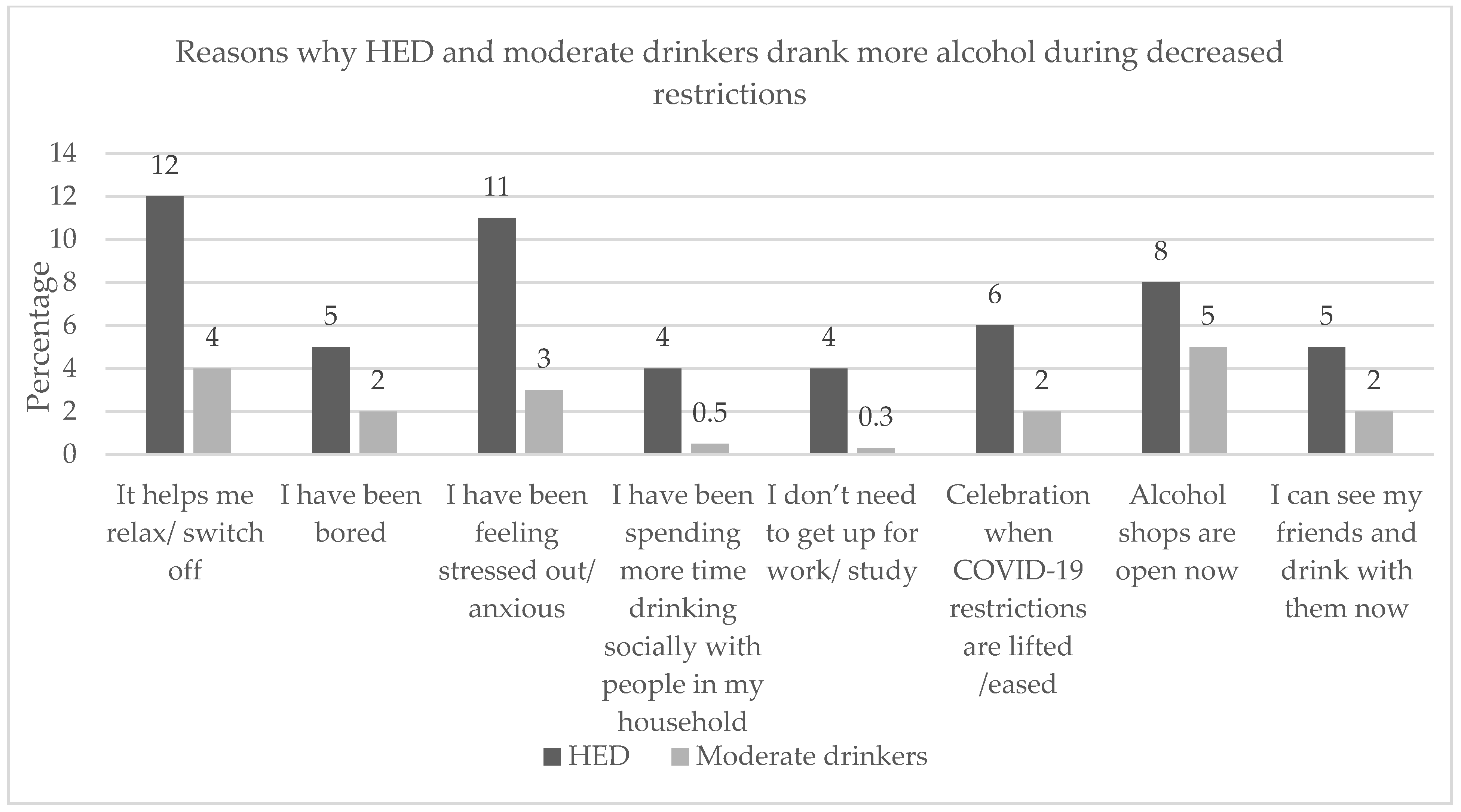
| Behaviour change | What are the reasons for drinking more during increased and decreased restrictions? You can tick more than one |
|
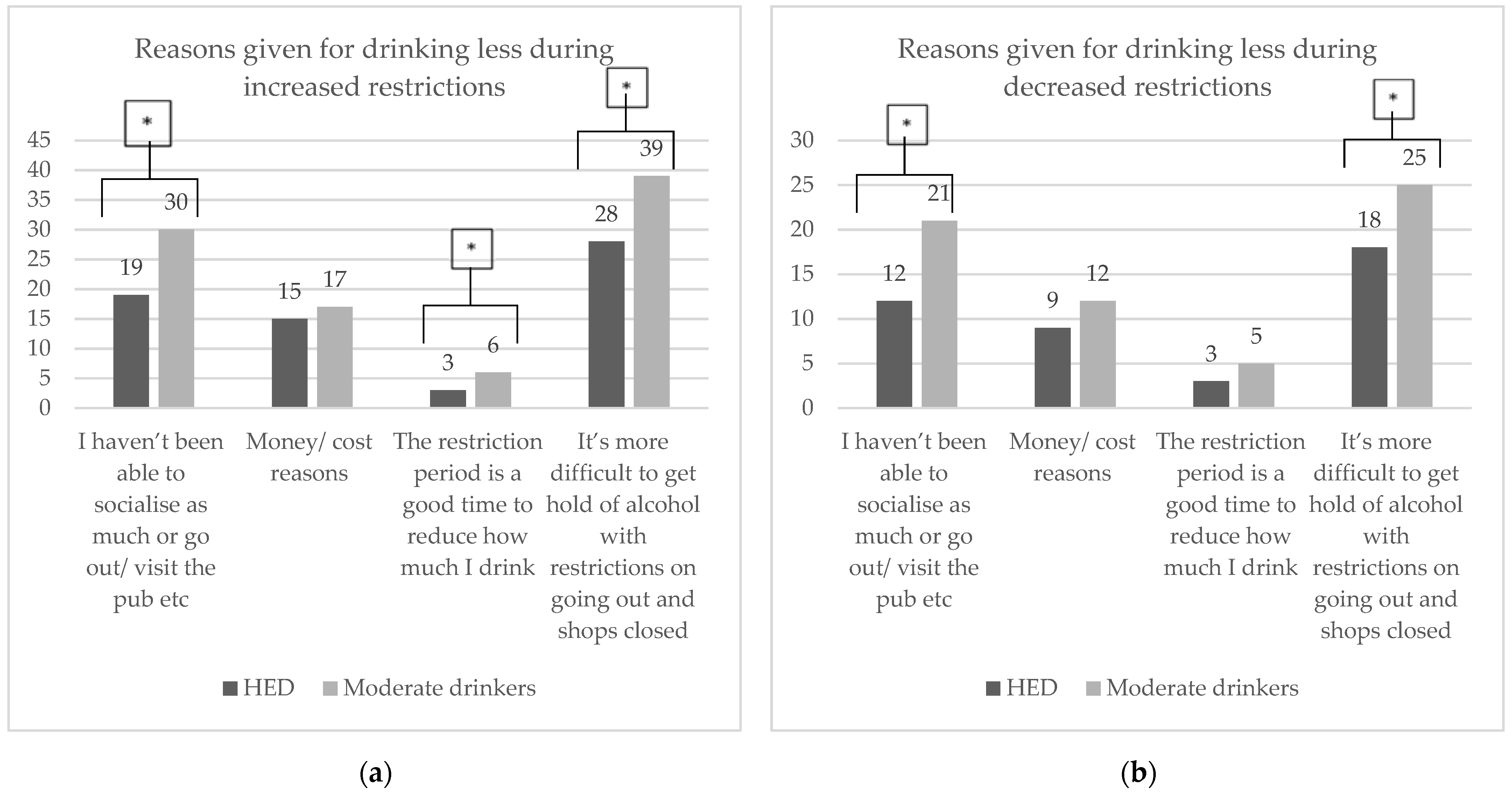
| What are the reasons for drinking less during increased and decreased restrictions? You can tick more than one |
|
| Variables | Total Dataset | Males | Females |
|---|---|---|---|
| n(%) 95% CI * | n(%) 95% CI * | n(%) 95% CI * | |
| Age | |||
| 18–34 | 105(13.5)11.2–16 | 33(14.2)10.1–19.1 | 72(13.2)10.5–16.2 |
| 35–44 | 141(18.1)15.5–20.9 | 28(16.3)12–21.5 | 103(18.9)15.8–22.3 |
| 45–54 | 165(21.2)18.4–24.2 | 41(17.6)13.1–22.9 | 124(22.7)19.3–26.4 |
| 55–64 | 228(29.3)26.2–32.5 | 64(27.5)22–33.5 | 164(30)26.3–34 |
| ≥65 | 140(18)15.4–20.8 | 57(24.5)19.3–30.3 | 83(15.2)12.4–18.4 |
| Ethnicity | |||
| Black African | 73(9.2)7.4–11.4 | 25(10.5)7.1–14.9 | 48(8.7)6.7–11.2 |
| Coloured | 35(4.4)3.2–6 | 10(4.2)2.2–7.3 | 25(4.5)3–6.5 |
| White | 658(83.2)80.5–85.7 | 196(82.4)77.1–86.8 | 462(83.5)80.3–86.5 |
| Asian/other | 25(3.2)2.1–4.6 | 7(2.9)1.3–5.7 | 18(3.3)2–5 |
| Province | |||
| Eastern Cape | 63(7.9)6.2–10 | 21(8.7)5.6–12.7 | 42(7.6)5.6–10 |
| Free State | 30(3.8)2.6–5.3 | 9(3.7)1.9–6.7 | 21(3.8)2.4–5.6 |
| Gauteng | 319(40.1)36.8–43.6 | 99(40.9)34.9–47.2 | 220(39.8)35.8–43.9 |
| Kwazulu-Natal | 120(15.1)12.7–17.7 | 31(12.8)9–17.5 | 89(16.1)13.2–19.3 |
| Mpumalanga | 31(3.9)2.7–5.4 | 10(4.1)2.1–7.2 | 21(3.8)2.4–5.6 |
| Limpopo | 27(3.4)2.3–4.8 | 9(3.7)1.9–6.7 | 18(3.3)2–5 |
| Northern Cape | 11(1.4)0.7–2.4 | 2(0.8)0.2–2.6 | 9(1.6)0.8–2.9 |
| North West | 22(2.8)1.8–4.1 | 8(3.3)1.6–6.1 | 14(2.5)1.5–4.1 |
| Western Cape | 172(21.6)18.9–24.6 | 53(21.9)17–27.4 | 119(21.5)18.2–25.1 |
| Change in monthly net household income since the COVID-19 pandemic restrictions | |||
| Decreased income | 489(65.4)61.9–68.7 | 149(63.9)57.6–69.9 | 340(66)61.8–70 |
| No change | 220(29.4)26.2–32.8 | 66(28.3)22.8–34.4 | 154(29.9)26.1–34 |
| Increased income | 39(5.2)3.8–7 | 18(7.7)4.8–11.7 | 21(4.1)2.6–6.1 |
| Aged 70+, serious medical condition, or immunocompromised | |||
| Yes | 97(12.6)10.4–15.1 | 27(11.6)8–16.2 | 70(13.1)10.4–16.1 |
| No | 672(87.4)84.9–89.6 | 206(88.4)83.8–92 | 466(86.9)83.9–89.6 |
| COVID-19 pandemic restrictions at the time of completing the survey | |||
| 1 Total restriction | 7(0.9)0.4–1.7 | 1(0.4)0–1.9 | 6(1.1)0.5–2.2 |
| 2 Very restricted | 95(11.9)9.8–14.3 | 24(9.9)6.6–14.2 | 71(12.8)10.2–15.8 |
| 3 Moderate restriction | 406(51)47.5–54.5 | 113(46.7)40.5–53 | 293(52.9)48.7–57 |
| 4 Limited restriction | 248(31.2)28–34.4 | 89(36.8)30.9–43 | 159(28.7)25.1–32.6 |
| 5 Social distancing only | 19(2.4)1.5–3.6 | 11(4.5)2.4–7.7 | 8(1.4)0.7–2.7 |
| 6 No restriction | 21(2.6)1.7–3.9 | 4(1.7)0.6–3.9 | 17(3.1)1.9–4.8 |
| Variables | Total Dataset | Males | Females |
|---|---|---|---|
| n(%) 95% CI ** | n(%) 95% CI ** | n(%) 95% CI ** | |
| Frequency of alcohol consumption | |||
| ≥1 times per day | 195(26.8)23.7–30.1 | 81(35.7)29.7–42.1 | 114(22.8)19.2–26.6 |
| 1–6 times a week | 388(53.3)49.7–56.9 | 110(48.5)42–54.9 | 278(55.5)51.1–59.8 |
| 1–4 times per month | 98(13.5)11.1–16.1 | 24(10.6)7.1–15.1 | 74(14.8)11.9–18.1 |
| Less than once a month | 37(5.1)3.7–6.9 | 10(4.4)2.3–7.7 | 27(5.4)3.7–7.6 |
| 1–3 times per year | 10(1.4)0.7–2.4 | 2(0.9)0.2–2.8 | 8(1.6)0.8–3 |
| Classified as Heavy episodic drinkers * | |||
| Yes | 346(48.5)44.9–52.2 | 137(61.4)54.9–67.6 | 209(42.7)38.3–47.1 |
| No | 367(51.5)47.8–55.1 | 86(38.6)32.4–45.1 | 281(57.3)52.9–61.7 |
| Heavy episodic drinking frequency | |||
| Daily | 82(17.9)14.6–21.6 | 45(27.8)21.3–35 | 37(12.5)9.1–16.6 |
| Weekly | 182(39.7)35.3–44.3 | 68(42)34.6–49.7 | 114(38.5)33.1–44.1 |
| Monthly | 82(17.9)14.6–21.6 | 24(14.8)10–20.9 | 58(19.6)15.4–24.4 |
| Less than monthly | 112(24.5)20.7–28.5 | 25(15.4)10.5–21.6 | 87(29.4)24.4–34.8 |
| Illegal alcohol purchasing | |||
| Yes | 438(55.3)51.8–58.7 | 146(60.8)54.6–66.8 | 292(52.9)48.7–57 |
| No | 354(44.7)41–48.2 | 94(39.2)33.2–45.4 | 260(47.1)43–51.3 |
| First time buying alcohol illegally | |||
| Yes | 361(84)80.3–87 | 108(76.1)68.6–82.5) | 253(87.8)83.7–91.2 |
| No | 69(16)12.8–19.7 | 34(23.9)17.5–31.4 | 35(12.2)8.8–16.3 |
| Restrictions made it harder to cut down on drinking | |||
| Yes | 130(29.6)25.5–34 | 31(22.6)16.2–30.2 | 99(32.8)27.7–38.2 |
| No | 309(70.4)66–74.5 | 106(77.4)69.8–83.8 | 203(67.2)61.8–72.3 |
| Alcohol makes social/physical distancing more difficult | |||
| Yes | 109(13.8)11.6–16.4 | 30(12.6)8.8–17.2 | 79(14.4)11.6–17.5 |
| No | 679(86.2)83.6–88.4 | 209(87.4)82.8–91.2 | 470(85.6)82.5–88.4 |
| Variables | Heavy Episodic Drinkers | Moderate Drinkers | p-Value |
|---|---|---|---|
| n(%) 95% CI ** | n(%) 95% CI ** | (Chi-Square Test) | |
| Sex | |||
| Male | 137(39.6)34.5–44.8 | 86(24.4)19.3–28 | <0.001 |
| Female | 209(60.4)55.2–65.5 | 281(76.6)72–80.7 | |
| Age | |||
| 18–34 | 57(17)13.2–21.3 | 43(11.7)8.8–15.3 | <0.001 |
| 35–44 | 80(23.8)19.5–28.6 | 45(12.3)9.2–16 | |
| 45–54 | 83(24.7)20.3–29.5 | 66(18)14.4–22.2 | |
| 55–64 | 79(23.5)19.2–28.3 | 132(36.1)31.3–41.1 | |
| >65 | 37(11)8–14.7 | 80(21.9)17.9–26.3 | |
| Ethnicity | |||
| Black African | 37(10.7) 7.8–14.3 | 26(7)4.7–9.9 | 0.343 |
| Coloured | 15(4.3) 2.6–6.9 | 14(3.8)2.2–6.1 | |
| White | 282(81.5) 77.2–85.3 | 319(85.8)81.9–89.0 | |
| Asian/Other | 12(3.5) 1.9–5.8 | 13(3.5)2.0–5.7 | |
| Province | |||
| Eastern Cape | 26(7.4) 5.0–10.6 | 28(7.5) 5.1–10.5 | 0.956 |
| Free State | 11(3.2) 1.7–5.4 | 17(4.5) 2.8–7.0 | |
| Gauteng | 146(41.8)36.7–47.1 | 149(39.8)35–44.9 | |
| Kwazulu-Natal | 52(14.9)11.5–18.9 | 59(15.8)12.4–19.7 | |
| Mpumalanga | 16(4.6)2.8–7.2 | 12(3.2)1.8–5.4 | |
| Limpopo | 11(3.2)1.7–5.4 | 12(3.2)1.8–5.4 | |
| Northern Cape | 4(1.1)0.4–2.7 | 6(1.6)0.7–3.3 | |
| North West | 8(2.3)1.1–4.3 | 11(2.9)1.6–5 | |
| Western Cape | 75(21.5)17.4–26 | 80(21.4)17.5–25.8 | |
| Change in monthly net household income since the COVID-19 pandemic restrictions | |||
| Decreased income | 240(70.2)65.2–74.8 | 222(59.8)54.8–64.7 | 0.004 |
| No change | 82(24)19.7–28.7 | 131(35.3)30.6–40.3 | |
| Increased income | 20(5.8)3.7–8.7 | 18(4.9)3–7.4 | |
| Aged 70+, serious medical condition, or immunocompromised | |||
| Yes | 31(9.1)6.4–12.5 | 60(16.7)13.1–20.8 | 0.003 |
| No | 309(90.9)87.5–93.6 | 300(83.3)79.2–86.9 | |
| COVID-19 pandemic restrictions | |||
| 1 Total restriction | 3(0.8)0.2–2.2 | 4(1)0.3–2.4 | 0.150 |
| 2 Very restricted | 43(11.8)8.8–15.4 | 47(12)9.1–15.5 | |
| 3 Moderate restriction | 182(49.9)44.8–55 | 199(50.9)45.9–55.8 | |
| 4 Limited restriction | 112(30.7)26.1–35.6 | 131(33.5)29–38.3 | |
| 5 Social distancing only | 13(3.6)2–5.8 | 5(1.3)0.5–2.8 | |
| 6 No restriction | 12(3.3)1.8–5.5 | 5(1.3)0.5–2.8 | |
| Frequency of alcohol consumption | |||
| ≥1 times per day | 121(33.2)28.5–38.1 | 78(20.1)16.3–24.3 | <0.001# |
| 1–6 times a week | 209(57.3)52.1–62.3 | 188(48.5)43.5–53.4 | |
| 1–4 times per month | 25(6.8)11.7–16.7 | 81(20.9)17.1–25.1 | |
| Less than once a month | 10(2.7)4.1–7.4 | 32(8.2)5.8–11.3 | |
| 1–3 times per year | 0 | 9(2.3)1.2–4.2 | |
| Illegal alcohol purchasing | |||
| Yes | 278(76.2)71.6–80.3 | 171(44.2)39.3–49.2 | <0.001 |
| No | 87(23.8)19.7–28.4 | 216(55.8)50.8–60.7 | |
| First time buying alcohol illegally | |||
| Yes | 220(80.9)75.9–85.2 | 153(90)84.8–93.8 | 0.010 |
| No | 52(19.1)14.8–24.1 | 17(10)6.2–15.2 | |
| Restrictions made it harder to cut down on drinking | |||
| Yes | 92(38)32.1–44.2 | 35(20)14.6–26.4 | <0.001 |
| No | 150(62)55.8–67.9 | 140(80)73.6–85.4 | |
| Alcohol makes social/physical distancing more difficult | |||
| Yes | 38(10.9)7.9–14.5 | 64(17)13.4–21 | 0.018 |
| No | 311(89.1)85.5–92.1 | 313(83)79–86.6 |
| Variables | AOR * | 95%CI ** | p-Value |
|---|---|---|---|
| Sex | |||
| Male | (ref) | ||
| Female | 0.30 | 0.13–0.70 | 0.006 |
| Age | |||
| 18–34 | (ref) | ||
| 35–44 | 1.58 | 0.50–4.99 | 0.439 |
| 45–54 | 1.17 | 0.39–3.54 | 0.775 |
| 55–64 | 0.46 | 0.16–1.31 | 0.144 |
| ≥65 | 0.23 | 0.06–0.91 | 0.037 |
| Change in monthly net household income since the COVID-19 pandemic restrictions | |||
| Decreased income | (ref) | ||
| No change | 0.97 | 0.42–2.22 | 0.937 |
| Increased income | 1.46 | 0.34–6.19 | 0.607 |
| Aged 70+, serious medical condition, or immunocompromised | |||
| Yes | (ref) | ||
| No | 1.21 | 0.39–3.79 | 0.738 |
| Frequency of alcohol consumption | |||
| ≥1 times per day | (ref) | ||
| 1–6 times a week | 0.74 | 0.33–1.66 | 0.464 |
| 1–4 times per month | 0.13 | 0.03–0.45 | 0.001 |
| Less than once a month | 0.56 | 0.10–3.07 | 0.507 |
| Illegal alcohol purchasing | |||
| Yes | (ref) | ||
| No | 0.20 | 0.10–0.40 | <0.001 |
| First time buying alcohol illegally | |||
| Yes | (ref) | ||
| No | 1.72 | 0.63–4.66 | 0.287 |
| Restrictions made it harder to cut down on drinking | |||
| Yes | (ref) | ||
| No | 0.49 | 0.24–1.00 | 0.051 |
| Alcohol makes social/physical distancing more difficult | |||
| Yes | (ref) | ||
| No | 1.68 | 0.60–4.66 | 0.321 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theron, M.; Swart, R.; Londani, M.; Parry, C.; Petersen Williams, P.; Harker, N. Did COVID-19-Related Alcohol Sales Restrictions Reduce Alcohol Consumption? Findings from a National Online Survey in South Africa. Int. J. Environ. Res. Public Health 2022, 19, 2422. https://doi.org/10.3390/ijerph19042422
Theron M, Swart R, Londani M, Parry C, Petersen Williams P, Harker N. Did COVID-19-Related Alcohol Sales Restrictions Reduce Alcohol Consumption? Findings from a National Online Survey in South Africa. International Journal of Environmental Research and Public Health. 2022; 19(4):2422. https://doi.org/10.3390/ijerph19042422
Chicago/Turabian StyleTheron, Marieke, Rina Swart, Mukhethwa Londani, Charles Parry, Petal Petersen Williams, and Nadine Harker. 2022. "Did COVID-19-Related Alcohol Sales Restrictions Reduce Alcohol Consumption? Findings from a National Online Survey in South Africa" International Journal of Environmental Research and Public Health 19, no. 4: 2422. https://doi.org/10.3390/ijerph19042422