
‘Who Else If Not We’. Medical Students’ Perception and Experiences with Volunteering during the COVID-19 Crisis in Poznan, Poland


Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Participant Recruitment and Data Collection
2.3. Data Analysis
3. Results
3.1. Participants
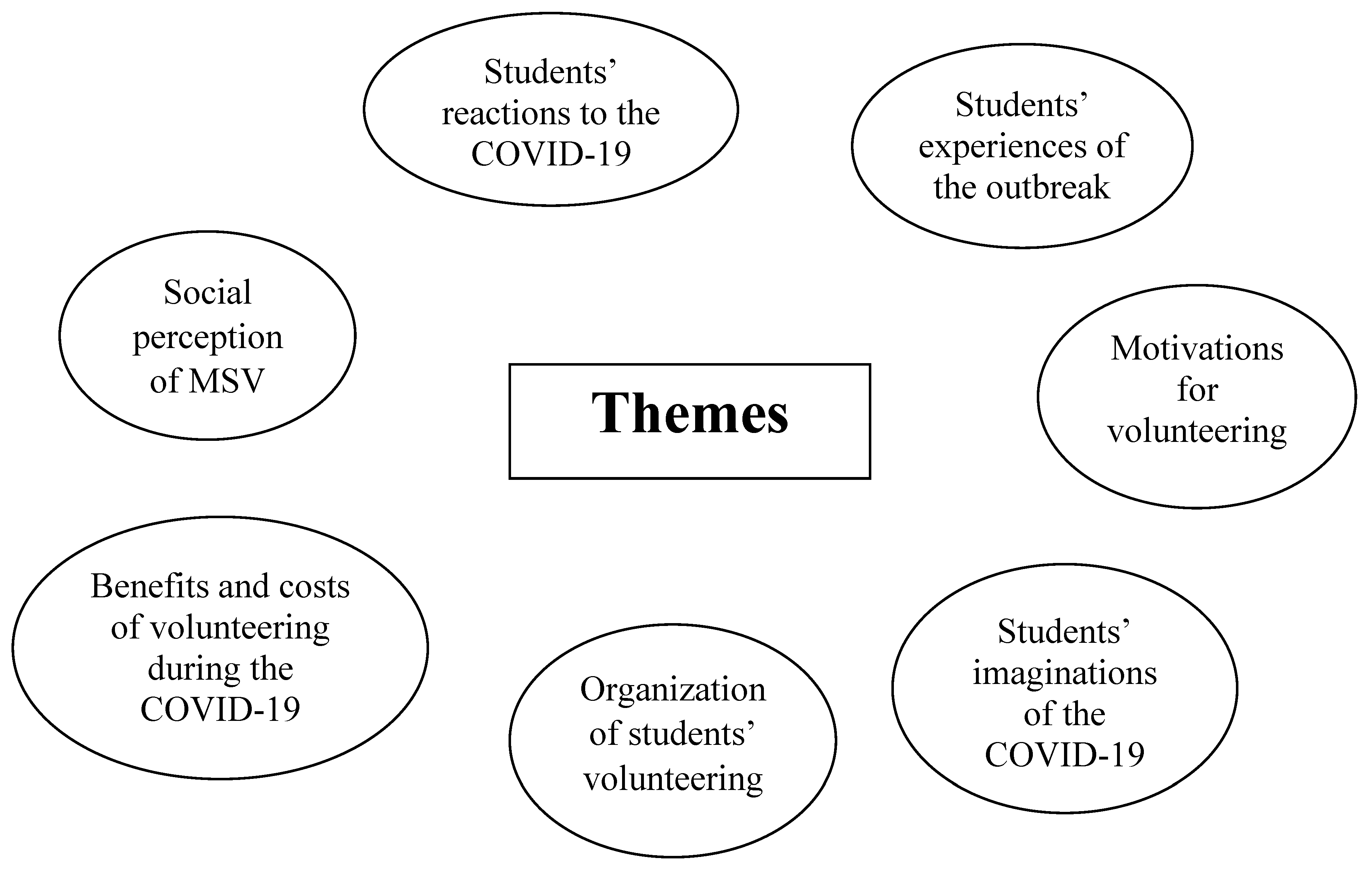
3.2. Findings
3.2.1. Theme 1: Medical Students’ Reactions to the COVID-19 Pandemic
At the beginning it was fear. I thought it would be like a plague and that people would be dying on the streets, especially that the media were constantly showing images from Italy with the soldiers on the streets. There was also rumours that they would close the entire city, so I thought I would be cut off from the world. It was fear and insecurity.(MSV3)
There was a lot of adrenaline. I had this feeling that a war was coming.(MSV10)
When they [the government—JD] told us that it was going to last for two weeks only, I already knew that it would be much longer, as no epidemic lasts for two weeks.(MSV2)
While I was thinking that in relation to the number of infections restrictions were too harsh, I also knew that it wouldn’t be as promising as the minister Szumowski [the Minster of Health—JD] was saying.(MSV8)
At the beginning I didn’t believe it was a real pandemic (…) Later when the number grew and the virus appeared in Italy and Poland, I was mad that so many people didn’t follow the restrictions.(MSV15)
[i]n October I was very sceptical about it. I thought it would be like in the case of Ebola: they were scaring us that it would also come to Europe but nothing like that happened. When it came to Poland (…) I was scared that Poland would turn into a second Italy.(MSV17)
I was mad and furious. My anxiety over the future mixed with anger that my plans couldn’t be realized. I was sad and mad that my study trip to Summer School abroad was cancelled.(MSV6)
I was very upset that all the classes were suspended. I thought it was unnecessary and exaggerated. I was mad that they took away my time from clinical classes.(MSV19)
Respondents were also afraid over the health of their loved ones, including parents and grandparents.
I was afraid over the health of my parents and grandparents.(MSV12)
I was worried that my grandparents may be infected.(MSV20)
3.2.2. Theme 2: Medical Students’ Experiences of the Outbreak
When the pandemic gained momentum I was scared over the health of my loved ones, my family.(MSV11)
I was more afraid of being a carrier than of being infected. Because of my age and good physical shape I didn’t feel endangered. I was afraid that I might infect others.(MSV20)
After two or three months I started wondering how it would affect my education. I worried that we didn’t have access to clinical classes and patients, and that online lectures and seminars were not enough, as we were unable to talk to the patients and examine them.(MSV1)
I was afraid that I wouldn’t be able to finish my studies. As we have lost almost a year and a half now, I was wondering how we could catch up and how we would handle ourselves in the future job. I was afraid that we would have to learn everything in practice, at work. It was hard.(MSV15)
I didn’t experience any special worries. (…) I thought it was an opportunity for me, a chance to gain extra knowledge.(MSV5)
To be honest, I wasn’t scared, nor had any negative feeling about it because I knew that I wasn’t in the group of increased risk. So I tried not to panic. It didn’t affect me.(MSV19)
I was scared over my future and health, how I would handle the isolation. Such negative feelings affected me a lot. My relationship broke up, and weeks of isolation resulted in panic attacks.(MSV6)
It was social isolation, a prohibition to leave home and an inability to realize my passions that were the hardest experience; and fear over my loved ones. These were the most dominant feelings.(MSV1)
3.2.3. Theme 3: Motivations for Volunteering
I had a feeling of duty. Although I don’t study medicine or pharmacy, I thought that as a public health student I could help. I was thinking ‘Who else if not we’, at the medical university.(MSV4)
It may sound naïve, but it was a kind of imperative: you must give something from yourself, especially as you have finished medical university. I wanted to do something, and not be the observer and commentator. I had the sense of vocation.(MSV7)
Because I have chosen my studies to help people and I often wondered what would I do if a war started or something I thought that maybe this was the right time to step up. It was a sense of a mission, the feeling of solidarity with the medics and the desire to help the sick.(MSV17)
For me it was a natural decision, to continue my medical volunteering I have started a year before the pandemic.(MSV5)
It wasn’t a difficult decision. I have been engaged in voluntary service from early high school. In high-school I was a member of the Red Cross. I’ve always liked such activity.(MSV6)
Because I come from a small town, I was tired of sitting at home doing nothing apart from walking around or jogging. I wanted to help and engage in something.(MSV15)
It had a therapeutic value, because due to the lockdown it was impossible to leave home, meet people or travel. It was difficult; so if I didn’t volunteer it would be an even harder experience, especially that I had moments when I felt helpless and very uncertain.(MSV17)
My colleague posted a message that we can pass our summer internships as volunteers. I thought it was a good opportunity to observe how management in a state agency functions. I also wanted to escape a bit from my bad mood.(MSV21)
I wanted to be closer to what was going on. I wouldn’t gain all that knowledge while sitting at home next to the computer.(MSV4)
I thought it was an opportunity: being my age and working during the pandemic. I thought that it may not be the last pandemic and that this experience could benefit me in the future.(MSV5)
Because I study at this faculty [rescue medicine—JD], I felt, I’ll say it a bit lofty, a moral duty to help. I was also afraid that the healthcare system wouldn’t handle it. I believed that even a freshman like me could help. It was also a kind of adventure. Finally, I was hoping that as our education switched online I could learn something.(MSV8)
At the beginning it was the desire to help, but later I was also motivated by the possibility to pass my summer internship.(MSV20)
There was a kind of social pressure, especially in the media, that we should volunteer.(MSV16)
There was a kind of pressure, even from some professors. For example, one professor posted a message on Facebook saying: ‘Either you’d be with us or not’.(MSV17)
3.2.4. Theme 4: Medical Students’ Perceptions of the COVID-19 Volunteering
I had this image, like they showed it on the TV, that we would be placed in the military tents at the front of the hospitals, which would serve as a kind of ‘dying rooms’. I was expecting that I might get infected. I knew I was putting myself at risk.(MSV3)
I was thinking that (…) we would be sent to covid wards where we would be caring for the sick and monitor their life functions. It made me scared. I thought it might be dangerous.(MSV17)
I worried that I might infect somebody. I felt a great responsibility that some persons might be hospitalized because of me. Such worries accompanied me during my entire volunteering. Only when we all got vaccinated I felt secure enough I could visit my family at home.(MSV15)
Soon after I made the decision I started to worry, and I’ve felt it for months, that I might infect others. My anxiety was intensified by the constant information that young people are mainly carriers.(MSV16)
Back then I was studying for only six months, so I was worried that my knowledge was vague and that they could assign me things I was not familiar with.(MSV2)
I had some worries, especially during my first meeting with the patients. I felt uncertain and tentative as I was not sure whether I was qualified to do all those things. I was anxious that I may not be gentle enough or even harm those people who were already suffering.(MSV14)
3.2.5. Theme 5: Organization of Medical Students’ Volunteering
We underwent basic training sessions on occupational hygiene, safety procedures and infectious diseases. (…) I was also trained in the patients’ personal data protection. Additionally, there were always persons who were watching and helping us.(MSV2)
We underwent sanitary-epidemiological training: how to disinfect our hands and the workplace, wear masks and uniforms. We also knew exactly what to do during our volunteering; and someone was always helping us. I felt very safe and secure.(MSV17)
To be honest I felt like being thrown into deep water, without proper preparation. In fact, on the evening before I started someone called me and asked whether I could come the next day. However, I didn’t receive any type of training regarding safety or communication. I simply joined a nurse and was learning from her.(MSV14)
We barely had any training and it was my colleagues who showed me everything.(MSV1).
It was well organized. I felt safe and secure. We were provided with the PPE, although at the beginning there were some problems, as there were only reusable masks. Later they gave us also FFP2s and FFP3s.(MSV5)
At the beginning we didn’t have much protective equipment, there were very few masks or disinfectant liquid, but as it [the pandemic—JD] developed we were given the visors and dispensable aprons, and after a month it was much safer.(MSV2)
Although everyone was very supportive in technical issues, we didn’t have any psychological or emotional support. I missed the possibility of debriefing, and having a chance to share my experiences, anxieties and worries.(MSV6)
We didn’t have any type of institutional support, and some persons needed such psychological help, especially those who volunteered at the beginning, as it was a hard, and stressful work. After eight, ten hours on a duty we experienced a psychological and emotional burden.(MSV16)
I see how it has changed. Now, when students include volunteering as part of their practice their motivations are much different than it used to be when it all began. It has lost its spirit. Back then we were all excited that we were taking part in it, but later many students lacked that commitment. They simply wanted to pass their summer internships. They became more mercenary.(MSV3)
Because we do a normal job, I think that students could be offered a regular contract.(MSV5)
I think it was a good decision, especially at the beginning when the numbers were skyrocketing. There was a staff shortage and the system needed us.(MSV17)
I think it was a good decision, because we are preparing ourselves for a profession which is a kind of sacrifice and it was a chance to prove oneself.(MSV14)
3.2.6. Theme 6: Benefits and Costs of Volunteering during COVID-19
Now I see clearly that these studies have a purpose. Volunteering made me realize how great it is to work for such a great cause. It also helped me to develop self-confidence.(MSV3)
The most satisfying was that I had the feeling that I didn’t waste that time. I was useful and I was doing something important. I wasn’t passive.(MSV7)
I could test myself as I didn’t know how would I react in such a critical situation, whether I would go to the front line. Now I know I will, so I have proved this to myself.(MSV10)
I felt great satisfaction each time I managed to do something I have learnt during the classes. It was very satisfying when the personnel called for help as they already knew that I could do something and they were treating me as a member of their team.(MSV2)
It gave me a lot of practical knowledge and skills. I also developed many soft skills. I learnt how to communicate with people. I was able to work in a team, under pressure and to cope with difficult situations.(MSV4)
I have learnt more than I would during regular classes. On the intensive care unit, I was allowed to assist in some procedures that otherwise I could observe only after specialization. I also performed some procedures done typically by physicians, I would never do these as a nurse.(MSV13)
It helped me to develop compassion for the sick and dying patients and improved my communication skills. Now when we are on the ward during the classes I find it much easier to deal with toilet issues, wash the patient or change their diaper.(MSV14)
As a future physician I could observe and work with other healthcare professionals, i.e., nurses, and know their peculiarities. (…) It strengthened a solidarity between healthcare professionals.(MSV4)
I could observe how the system works during the pandemic, how do hospitals work during this new situation. I could watch how the ward operates and how nurses, paramedics, physicians and technicians work.(MSV8)
The hardest thing was conversations. Sometimes it was difficult to forget about them. I kept them in my head and I often thought that I should have said something else or differently. (…) I remember one conversation with a mother of a teenage girl who struggled with self-destructive behaviours: scarification, the ‘S thoughts’, overdosing paracetamol [silence]. This was the worst call. I was shaken emotionally and I reminiscenced about it for a long time and had flashbacks [silence]. After such calls I needed a day or two off to go through it.(MSV6)
The most difficult were conversations with the patients. Sometimes I felt helpless, as no one knew back then what to do, how to respond to questions… We were so confused.(MSV10)
Sometimes I felt irritated because there were so many patients and due to staff shortages they were not cared for enough. It was very frustrating because I often couldn’t devote them more time and answer all their questions. I often left the zone embittered, irritated and felt sorry for the patients.(MSV5)
Especially during the first month patients were very against us. They associated us with restrictions in entering hospital and called us many bad words. We faced many negative emotions, especially when they gathered together, were tired and didn’t understand why we let some persons in and others not. Frequently we met with insults.(MSV16)
Although during the first year we had some humanities, pedagogy or psychology, the studies didn’t prepare me for that: meeting people face-to-face, when they were often mad or aggressive while waiting for such a long time at the front of the hospital. Sometimes it was a bit dangerous.(MSV15)
Some of us could have been used better. Being a PhD student myself, I graduated from biotechnology and I am familiar with all those laboratory things like isolation, and PCR. I would be more useful in the COVID Lab.(MSV7)
I still have this feeling that we were not being used properly. There were hundreds of volunteers, but they didn’t recognize properly our potential and didn’t used us properly. People were very eager to work but our potential was wasted.(MSV16)
After performing the same tasks for two months I was a bit tired and bored. It was so monotonous and non-developing.(MSV1)
The hardest thing was to reconcile volunteering and studies.(MSV19)
It negatively affected my social relations.(MSV16)
3.2.7. Theme 7: Social Perception of MSV
My family was very supportive and proud. However, my extended family was like: ‘Why do you need it’, ‘Give it a break’. They were telling me I risk a lot and that I put relatives at risk. They discouraged me. But it was only at the beginning. Later they were proud and supportive.(MSV2)
My entire family was against it. My parents were afraid and they tried to discourage me. Now they are proud and I have become a ‘family star’.(MSV8)
On the University’s web page I saw videos describing our work. It stressed that not only professionals work in the laboratory but also the volunteers. I saw their gratitude. I felt appreciated and it made me very happy.(MSV17)
A dean came to us several times to see how we work and to show his appreciation. We even received an email from the hospital’s director who acknowledged our work.(MSV16)
Healthcare professionals were very supportive and they often expressed their gratitude and told us how they appreciate our presence and help.They often called us ‘heroes’.(MSV1)
Medical personnel appreciated us a lot. They were very thankful and stressed that thanks to us those, who worked at the front line were much safer. Nurses and receptionists were calling us ‘our angels’.(MSV16)
My friends from the university who didn’t know that I had volunteered were saying it was for the idiots; that one might get infected, that there was no equipment, one wouldn’t get paid and that it was not worth it as they wouldn’t let us do anything important.(MSV8)
My colleagues tried to discourage me and said I shouldn’t do it; and on Facebook ‘the swamp’ spilled. I saw the discussion on the web saying that they were trying to use us as a cheap workforce. They were mad at the University that it asked us to volunteer. It really irritated me. I couldn’t understand their need to comment on my decision and being so negative and aggressive about it.(MSV3)
Once, when I returned to my apartment after a twelve or eighteen hours of service I found a note stuck in the door saying that my neighbours were asking me to leave my apartment immediately because I was a possible ‘source of the plague’. I felt bitterness and disbelief.(MSV8)
In the summer time, when I was wondering whether I should come to a party, some friends told me ‘No, no, you don’t have to come. We know you are at work, you know’. It was such small things. Also some teachers, at another university where I also study, who knew about it, were afraid of letting me into the classes.(MSV10)
4. Discussion
5. Strengths and Limitations
6. Conclusions
- To ensure that medical students can effectively volunteer in future disasters, policymakers and university authorities should not overlook the potential force of medical students as a support to the health system;
- There is an urgent need for promoting the idea of volunteering among all medical students;
- Students’ participation should always be voluntary, and free of any type of external, formal, or informal pressure;
- Students volunteering should be treated as a way of supporting the student learning process and incorporated into university curricula;
- Medical universities should integrate global health and disaster medicine to the medical curricula;
- There is a need for special preparation courses that would improve students’ communication skills and handling of difficult situations;
- Dedicated university courses on emergency decision making, coping, and leadership during a crisis should be integrated into the medical curricula;
- To minimize the risk of litigation, students should always receive proper induction and be trained about their responsibilities, procedures, and protocols;
- All tasks performed by MSVs should be safe, adjusted to their capabilities and level of training, and performed under supervision and institutional medico-legal protection;
- When engaging MSVs, special attention should be paid to the risks of infecting the patients and students as well as to the PPE shortages;
- Because MSVs may perform some tasks remotely, telemedicine should be further developed;
- Because volunteering during the pandemic was physically and emotionally challenging, MSVs must be provided with mental health support in physically or emotionally challenging roles.
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Armocida, B.; Formenti, B.; Ussai, S.; Palestra, F.; Missoni, E. The Italian health system and the COVID-19 challenge. Lancet Public Health 2020, 5, e253. [Google Scholar] [CrossRef]
- Sabbah, M.Y. The Novel Coronavirus Disease (COVID-19) Outbreak: The Israeli Experience. J. Med. Sci. 2020, 89, e413. [Google Scholar] [CrossRef]
- Blumenthal, D.; Fowler, E.J.; Abrams, M.; Collins, S.R. COVID-19—Implications for the Health Care System. N. Engl. J. Med. 2020, 383, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Papoutsi, E.; Giannakoulis, V.G.; Ntella, V.; Pappa, S.; Katsaounou, P. Global burden of COVID-19 pandemic on healthcare workers. ERJ Open Res. 2020, 6, 00195. [Google Scholar] [CrossRef]
- Viguria, U.A.; Casamitjana, N. Early Interventions and Impact of COVID-19 in Spain. Int. J. Environ. Res. Public Health 2021, 18, 4026. [Google Scholar] [CrossRef] [PubMed]
- Soled, D.; Goel, S.; Barry, D.; Erfani, P.; Joseph, N.; Kochis, M.; Uppal, N.; Velasquez, D.; Vora, K.; Scott, K.W. Medical Student Mobilization during a Crisis: Lessons from a COVID-19 Medical Student Response Team. Acad. Med. 2020, 95, 1384–1387. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A. COVID-19: Medical students should not work outside their competency, says BMA. BMJ 2020, 368, m1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeWitt, D.E. Fighting COVID-19: Enabling Graduating Students to Start Internship Early at Their Own Medical School. Ann. Intern. Med. 2020, 173, 143–144. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.H.; Tan, S.; Raubenheimer, K. Rethinking the role of senior medical students in the COVID-19 response. Med. J. Aust. 2020, 212, 490. [Google Scholar] [CrossRef]
- Bauchner, H.; Sharfstein, J. A bold response to the COVID-19 pandemic: Medical students, National Service, and Public Health. JAMA 2020, 323, 1790–1791. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, S.; Sperling, P.; Poulsen, M.S.; Emmersen, J.; Andersen, S. Medical students for health-care staff shortages during the COVID-19 pandemic. Lancet 2020, 395, e79–e80. [Google Scholar] [CrossRef]
- Drexler, R.; Hambrecht, J.M.; Oldhafer, K.J. Involvement of Medical Students during the Coronavirus Disease 2019 Pandemic: A Cross-Sectional Survey Study. Cureus 2020, 12, e10147. [Google Scholar] [CrossRef]
- Bazan, D.; Nowicki, M.; Rzymski, P. Medical students as the volunteer workforce during the COVID-19 pandemic: Polish experience. Int. J. Disaster Risk Reduct. 2021, 55, 102109. [Google Scholar] [CrossRef] [PubMed]
- Chawłowska, E.; Staszewski, R.; Lipiak, A.; Giernaś, B.; Karasiewicz, M.; Bazan, D.; Nowosadko, M.; Cofta, M.; Wysocki, J. Student Volunteering as a Solution for Undergraduate Health Professions Education: Lessons from the COVID-19 Pandemic. Front. Public Health 2021, 8, 633888. [Google Scholar] [CrossRef] [PubMed]
- Domaradzki, J.; Walkowiak, D. Medical Students’ Voluntary Service during the COVID-19 Pandemic in Poland. Front. Public Health 2021, 9, 618608. [Google Scholar] [CrossRef] [PubMed]
- Domaradzki, J.; Walkowiak, D. Does Religion Influence the Motivations of Future Healthcare Professionals to Volunteer during the COVID-19 Pandemic in Poland? An Exploratory Study. J. Relig. Health 2021, 60, 1507–1520. [Google Scholar] [CrossRef]
- Tran, B.X.; Vo, L.H.; Phan, H.T.; Pham, H.Q.; Vu, G.T.; Le, H.T.; Latkin, C.A.; Ho, C.S.; Ho, R.C. Mobilizing medical students for COVID-19 responses: Experience of Vietnam. J. Glob. Health 2020, 10, 020319. [Google Scholar] [CrossRef]
- Lazarus, G.; Findyartini, A.; Putera, A.M.; Gamalliel, N.; Nugraha, D.; Adli, I.; Phowira, J.; Azzahra, L.; Ariffandi, B.; Widyahening, I.S. Willingness to volunteer and readiness to practice of undergraduate medical students during the COVID-19 pandemic: A cross-sectional survey in Indonesia. BMC Med. Educ. 2021, 21, 138. [Google Scholar] [CrossRef]
- Thomson, E.; Lovegrove, S. ‘Let us Help’—Why senior medical students are the next step in battling the COVID-19 Pandemic. Int. J. Clin. Pract. 2020, 74, e13516. [Google Scholar] [CrossRef] [Green Version]
- Ms, D.C.S. Senior Medical Students in the COVID-19 Response: An Opportunity to Be Proactive. Acad. Emerg. Med. 2020, 27, 343–345. [Google Scholar] [CrossRef] [Green Version]
- Menon, A.; Klein, E.J.; Kollars, K.; Kleinhenz, A.L. Medical Students Are Not Essential Workers: Examining Institutional Responsibility during the COVID-19 Pandemic. Acad. Med. 2020, 95, 1149–1151. [Google Scholar] [CrossRef] [PubMed]
- Cervera-Gasch, Á.; González-Chordá, V.M.; Mena-Tudela, D. COVID-19: Are Spanish medicine and nursing students prepared? Nurse Educ. Today 2020, 92, 104473. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.G.; Pierson, L.; Doernberg, S. The Role of Medical Students during the COVID-19 Pandemic. Ann. Intern. Med. 2020, 173, 145–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalet, A.; Jotterand, F.; Muntz, M.; Thapa, B.; Campbell, B. Hearing the Call of Duty: What We Must Do to Allow Medical Students to Respond to the COVID-19 Pandemic. WMJ 2020, 119, 6–7. [Google Scholar] [PubMed]
- Gallagher, T.H.; Schleyer, A.M. “We Signed Up for This!”—Student and Trainee Responses to the COVID-19 Pandemic. N. Engl. J. Med. 2020, 382, e96. [Google Scholar] [CrossRef] [PubMed]
- Bank, I.; Wijnen-Meijer, M. Why should medical students (not) be recruited to care for patients with COVID-19? BMC Med. Educ. 2020, 20, 342. [Google Scholar] [CrossRef] [PubMed]
- O’Byrne, L.; Gavin, B.; McNicholas, F. Medical students and COVID-19: The need for pandemic preparedness. J. Med. Ethics 2020, 46, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.M.; Bhatia, S.; Brown, S.; Cambridge, W.; Kamarajah, S.K.; McLean, K.A.; Brindl, N.; Lapolla, P.; Pérez-Ajates, S.; Raubenheimer, K.; et al. Representatives of the STARSurg Collaborative, EuroSurg Collaborative, and TASMAN Collaborative. Medical student involvement in the COVID-19 response. Lancet 2020, 395, 1254. [Google Scholar] [CrossRef]
- Astorp, M.S.; Sørensen, G.V.B.; Rasmussen, S.; Emmersen, J.; Erbs, A.W.; Andersen, S. Support for mobilising medical students to join the COVID-19 pandemic emergency healthcare workforce: A cross-sectional questionnaire survey. BMJ Open 2020, 10, e039082. [Google Scholar] [CrossRef]
- Michno, D.A.; Tan, J.; Adelekan, A.; Konczalik, W.; Woollard, A.C.S. How can we help? Medical students’ views on their role in the COVID-19 pandemic. J. Public Health 2021, 43, 479–489. [Google Scholar] [CrossRef]
- Pickell, Z.; Gu, K.; Williams, A.M. Virtual volunteers: The importance of restructuring medical volunteering during the COVID-19 pandemic. Med. Humanit. 2020, 46, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Trautwein, S.; Liberatore, F.; Lindenmeier, J.; von Schnurbein, G. Satisfaction with Informal Volunteering during the COVID-19 Crisis: An Empirical Study Considering a Swiss Online Volunteering Platform. Nonprofit Volunt. Sect. Q. 2020, 49, 1142–1151. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2021: OECD Indicators; OECD Publishing: Paris, France, 2021; Available online: https://data.oecd.org/healthres/doctors.htm (accessed on 27 January 2022).
- Puls Medycyny. 2021. Available online: https://pulsmedycyny.pl/koronawirus-wiemy-ilu-zmarlo-lekarzy-ile-pielegniarek-ratownikow-farmaceutow-1136222 (accessed on 27 January 2022).
- Koronawirus w Polsce (SARS-CoV-2). Available online: https://koronawirusunas.pl (accessed on 27 January 2022).
- Ministerstwo Zdrowia. Wolontariat. Available online: http://www.archiwum.mz.gov.pl/system-ochrony-zdrowia/kadra-medyczna-i-ksztalcenie/wolontariat/ (accessed on 27 January 2022).
- Creswell, J.W.; Porth, C. Qualitative Inquiry and Research Design: Choosing among Five Approaches, 4th ed.; SAGE: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Peat, G.; Rodriguez, A.; Smith, J. Interpretive phenomenological analysis applied to healthcare research. Évid. Based Nurs. 2019, 22, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Buschle, C.; Reiter, H.; Bethmann, A. The qualitative pretest interview for questionnaire development: Outline of programme and practice. Qual. Quant. 2021, 1–20. [Google Scholar] [CrossRef]
- Boddy, C.R. Sample size for qualitative research. Qual. Mark. Res. Int. J. 2016, 19, 426–432. [Google Scholar] [CrossRef]
- Colaizzi, P.F. Psychological research as the phenomenologist views its. In Existential-Phenomenological Alternatives for Psychology; Valle, R.S., King, M., Eds.; Oxford University Press: New York, NY, USA, 1978; pp. 48–71. [Google Scholar]
- Tempski, P.; Arantes-Costa, F.M.; Kobayasi, R.; Siqueira, M.A.M.; Torsani, M.B.; Amaro, B.Q.R.C.; Nascimento, M.E.F.M.; Siqueira, S.L.; Santos, I.S.; Martins, M.A. Medical students’ perceptions and motivations during the COVID-19 pandemic. PLoS ONE 2021, 16, e0248627. [Google Scholar] [CrossRef]
- Buckland, R. Medical student volunteering during COVID-19: Lessons for future interprofessional practice. J. Interprof. Care 2020, 34, 679–681. [Google Scholar] [CrossRef]
- Klasen, J.M.; Meienberg, A.; Bogie, B.J.M. Medical student engagement during COVID-19: Lessons learned and areas for improvement. Med. Educ. 2021, 55, 115–118. [Google Scholar] [CrossRef]
- Prisca, O.A.; Olawale, A.M.; Adeniyi, F.O.; Adelani, W.T.; Ijeoma, L.O.; Simeon, K.O.; Mfuh, A.Y.L.; Adisa, B.I.; Iyanuoluwa, O.O.; Ifeoluwapo, O.K.; et al. Knowledge, attitude and willingness of Nigerian nursing students to serve as volunteers in covid-19 pandemic. Int. J. Nurs. Midwifery 2021, 13, 1–10. [Google Scholar] [CrossRef]
- AlOmar, R.S.; AlShamlan, N.A.; AlAmer, N.A.; Aldulijan, F.; AlMuhaidib, S.; Almukhadhib, O.; Algarni, S.A.; Alshaibani, A.; Darwish, M.; Al Shammari, M. What are the barriers and facilitators of volunteering among healthcare students during the COVID-19 pandemic? A Saudi-based cross-sectional study. BMJ Open 2021, 11, e042910. [Google Scholar] [CrossRef]
- Wang, S.; Dai, M. Status and situation of postgraduate medical students in China under the influence of COVID-19. Postgrad. Med. J. 2020, 96, 728–730. [Google Scholar] [CrossRef] [PubMed]
- Gouda, P.; Kirk, A.; Sweeney, A.-M.; O’Donovan, D. Attitudes of Medical Students Toward Volunteering in Emergency Situations. Disaster Med. Public Health Prep. 2020, 14, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Haines, M.J.; Yu, A.C.M.; Ching, G.; Kestler, M. Integrating a COVID-19 volunteer response into a Year-3 md curriculum. Med. Educ. 2020, 54, 960–961. [Google Scholar] [CrossRef] [PubMed]
- Klasen, J.M.; Meienberg, A.; Nickel, C.; Bingisser, R. SWAB team instead of SWAT team: Medical students as a frontline force during the COVID-19 pandemic. Med. Educ. 2020, 54, 860. [Google Scholar] [CrossRef]
- Altillo, B.S.A.; Gray, M.; Avashia, S.B.; Norwood, A.; Nelson, E.A.; Johnston, C.; Bhavnani, D.; Patel, H.; Allen, C.H.; Adeni, S.; et al. Global health on the front lines: An innovative medical student elective combining education and service during the COVID-19 pandemic. BMC Med. Educ. 2021, 21, 186. [Google Scholar] [CrossRef]
- Kopp, A.R.; Rikin, S.; Cassese, T.; Berger, M.A.; Raff, A.C.; Gendlina, I. Medical student remote eConsult participation during the COVID-19 pandemic. BMC Med. Educ. 2021, 21, 120. [Google Scholar] [CrossRef]
- Cullum, R.J.; Shaughnessy, A.; Mayat, N.Y.; El Brown, M. Identity in lockdown: Supporting primary care professional identity development in the COVID-19 generation. Educ. Prim. Care 2020, 31, 200–204. [Google Scholar] [CrossRef]
- Findyartini, A.; Anggraeni, D.; Husin, J.M.; Greviana, N. Exploring medical students’ professional identity formation through written reflections during the COVID-19 pandemic. J. Public Health Res. 2020, 9 (Suppl. 1). [Google Scholar] [CrossRef]
- Shibu, A. Medical student engagement during the COVID-19 pandemic—A student perspective. Med. Educ. 2021, 55, 768. [Google Scholar] [CrossRef]
- Slivkoff, M.D.; Johnson, C.; Tackett, S. First-Year Medical Student Experiences Adjusting to the Immediate Aftermath of COVID-19. Med. Sci. Educ. 2021, 31, 557–564. [Google Scholar] [CrossRef]
- Roncone, R.; Giusti, L.; Mammarella, S.; Salza, A.; Bianchini, V.; Lombardi, A.; Prosperococco, M.; Ursini, E.; Scaletta, V.; Casacchia, M. “Hang in There!”: Mental Health in a Sample of the Italian Civil Protection Volunteers during the COVID-19 Health Emergency. Int. J. Environ. Res. Public Health 2021, 18, 8587. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No | Code | Gender | Faculty | Year of Study (While Volunteering) | Time Spent Volunteering | Tasks Performed | Earlier Volunteering |
|---|---|---|---|---|---|---|---|
| 1. | MSV1 | female | medicine | 5 | 2 months | triage in the hospital | yes |
| 2. | MSV2 | female | medicine | 1 | 3 months | triage, nurse assistance | yes |
| 3. | MSV3 | male | medicine | 2 | 5 months | tele-information in the hospital | yes |
| 4. | MSV4 | female | public health | 4 | 1.5 months | telephone advice in a sanitary-epidemiological station | yes |
| 5. | MSV5 | male | rescue medicine | 2 | 12 months | emergency room | yes |
| 6. | MSV6 | female | public health | 1 | 2 months | tele-information | yes |
| 7. | MSV7 | female | medicine | 2 (PhD student) | 1.5 months | drive-thru testing | yes |
| 8. | MSV8 | male | rescue medicine | 1 | 3 months | pre-triage in the hospital and bringing packages from families to patients | no |
| 9. | MSV9 | female | pharmacy | 4 | 2 months | drive-thru testing | yes |
| 10. | MSV10 | female | nursing | 2 | 3 months | call-centre in the hospital, triage in the hospital | yes |
| 11. | MSV11 | female | medicine | 4 | 4 months | organization of PPE supplies; translation of English texts about COVID-19 | yes |
| 12. | MSV12 | female | medical analytics | 3 | 2,5 months | telephone advice in a sanitary-epidemiological station | yes |
| 13. | MSV13 | male | nursing | 1&2 | 4 months | hospice, anestiosiology, intensive care ward | yes |
| 14. | MSV14 | female | nursing | 1 | 5 months | hospice, non-COVID-19 wards | no |
| 15. | MSV15 | female | nursing | 2 | 6 months | translation of English texts about COVID-19 | yes |
| 16. | MSV16 | female | medicine | 5 | 3 months | triage in the hospital | yes |
| 17. | MSV17 | female | medicine | 3 | 1 month | the University Coronavirus Laboratory at PUMS (administrative work) | no |
| 18. | MSV18 | female | nursing | 4 | 3 months | triage, nurse assistance | no |
| 19. | MSV19 | female | medicine | 1 | 2 months | triage in the hospital | no |
| 20. | MSV20 | female | nursing | 3 | 2.5 months | triage, nurse assistance | yes |
| 21. | MSV21 | male | medicine | 3 | 3 months | tele-information in the hospital | yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domaradzki, J. ‘Who Else If Not We’. Medical Students’ Perception and Experiences with Volunteering during the COVID-19 Crisis in Poznan, Poland. Int. J. Environ. Res. Public Health 2022, 19, 2314. https://doi.org/10.3390/ijerph19042314
Domaradzki J. ‘Who Else If Not We’. Medical Students’ Perception and Experiences with Volunteering during the COVID-19 Crisis in Poznan, Poland. International Journal of Environmental Research and Public Health. 2022; 19(4):2314. https://doi.org/10.3390/ijerph19042314
Chicago/Turabian StyleDomaradzki, Jan. 2022. "‘Who Else If Not We’. Medical Students’ Perception and Experiences with Volunteering during the COVID-19 Crisis in Poznan, Poland" International Journal of Environmental Research and Public Health 19, no. 4: 2314. https://doi.org/10.3390/ijerph19042314