
Estonian Dental Students’ Oral Health-Related Knowledge, Attitudes and Behaviours (KAB): National Survey-Based Study

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
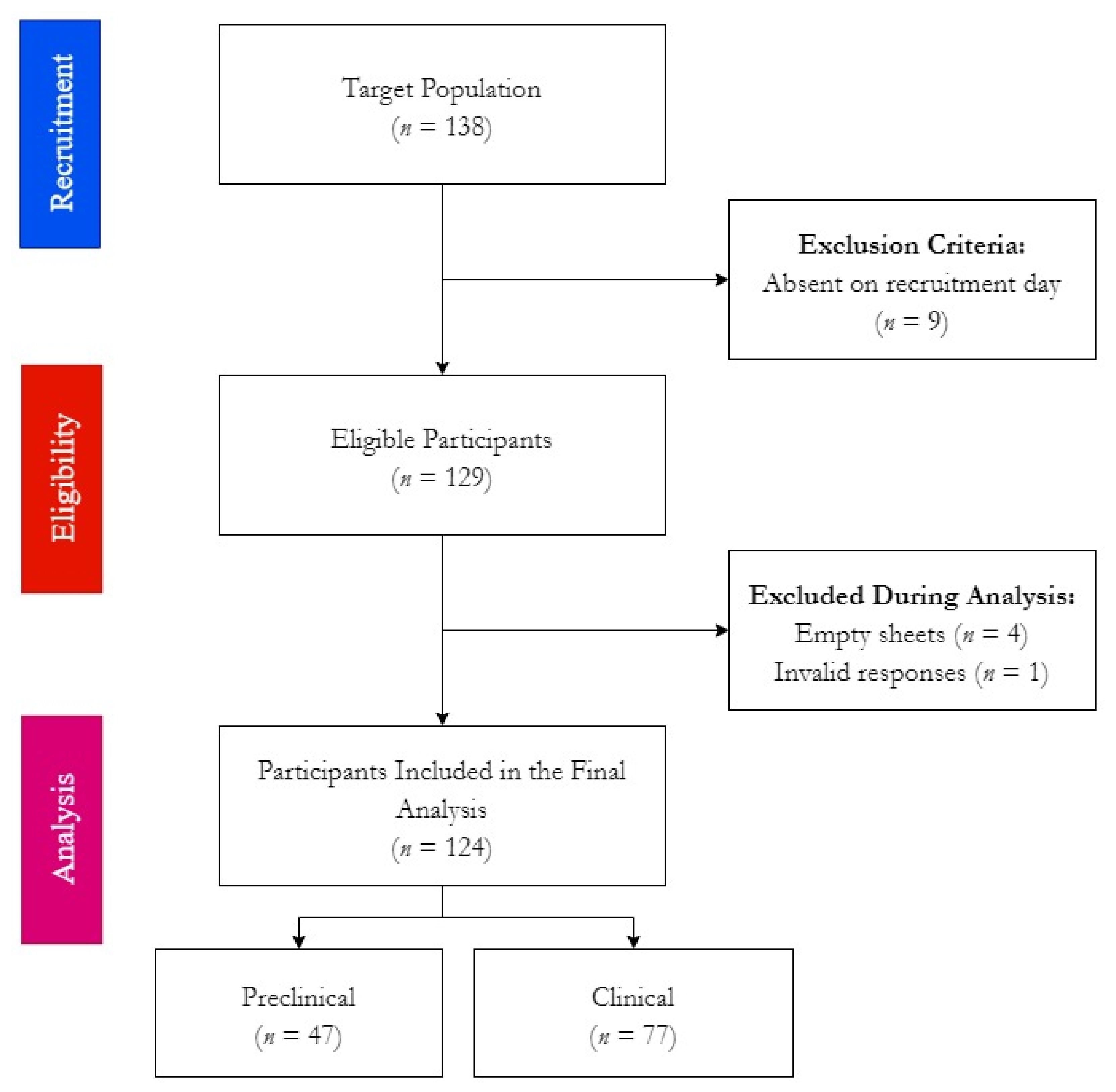
2.1. Design
2.2. Participants
2.3. Instrument
2.4. Ethics
2.5. Analyses
3. Results
3.1. Demographic Characteristics
3.2. Health Behaviours
3.3. HU-DBI Responses
3.3.1. Gender
3.3.2. Academic Level
3.3.3. Clinical Experience
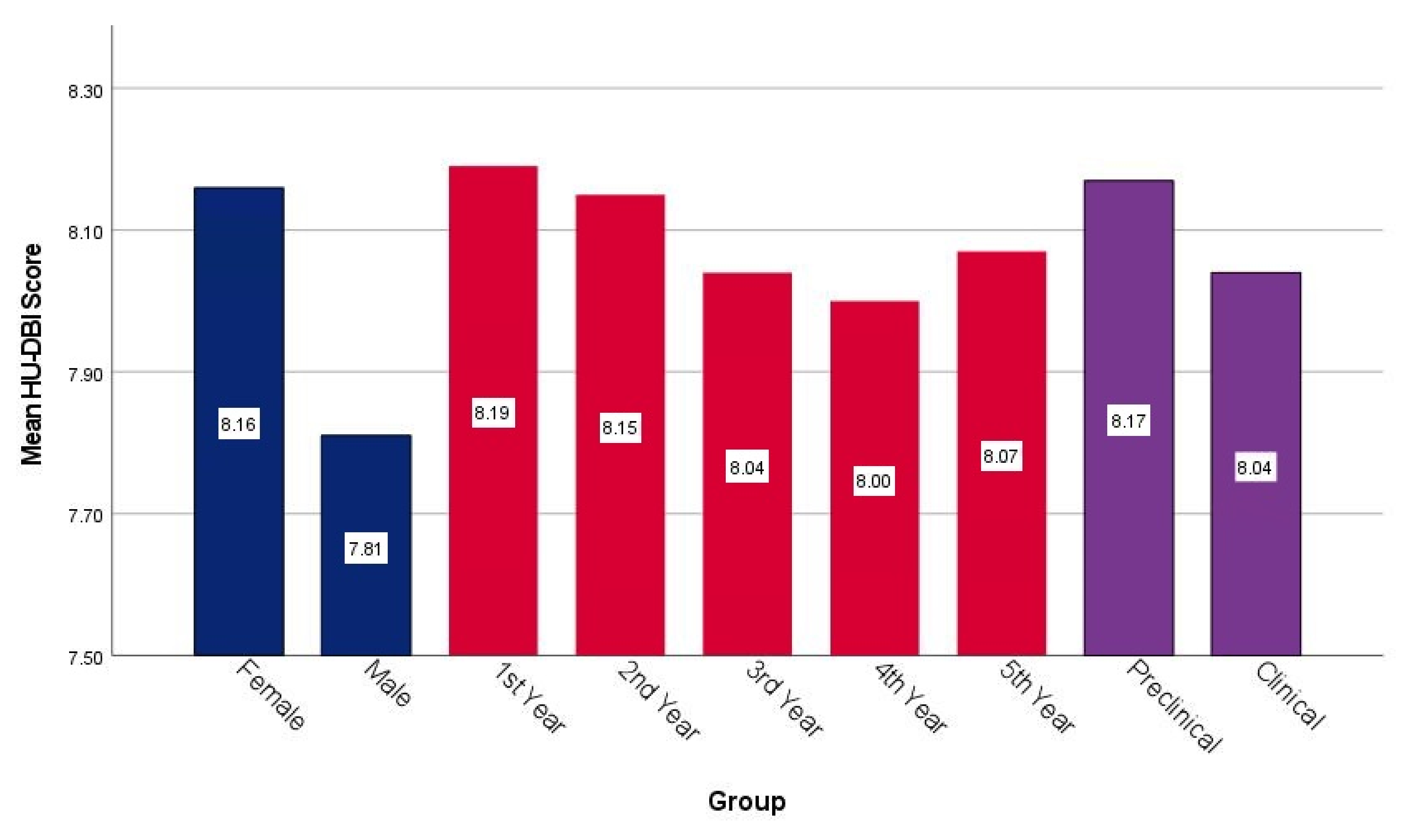
3.4. HU-DBI Scores
3.5. Year-Over-Year Analysis
3.6. Tobacco Smoking
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| # | Item | Agree | Disagree |
| 1 | I do not worry much about visiting the dentist. | □ | □ |
| 2 | My gum tends to bleed when I brush my teeth. | □ | □ |
| 3 | I worry about the color of my teeth. | □ | □ |
| 4 | I have noticed some white sticky deposits on my teeth. | □ | □ |
| 5 | I use a child sized toothbrush. | □ | □ |
| 6 | I think that I cannot help having false teeth when I am old. | □ | □ |
| 7 | I am bothered by the color of my gum. | □ | □ |
| 8 | I think my teeth are getting worse despite my daily brushing. | □ | □ |
| 9 | I brush each of my teeth carefully. | □ | □ |
| 10 | I have never been taught professionally how to brush. | □ | □ |
| 11 | I think I can clean my teeth well without using toothpaste. | □ | □ |
| 12 | I often check my teeth in a mirror after brushing. | □ | □ |
| 13 | I worry about having bad breath. | □ | □ |
| 14 | It is impossible to prevent gum disease with tooth brushing alone. | □ | □ |
| 15 | I put off going to dentist until I have a toothache. | □ | □ |
| 16 | I have used a dye to see how clean my teeth are. | □ | □ |
| 17 | I use a toothbrush which has hard bristles. | □ | □ |
| 18 | I do not feel I have brushed well unless I brush with hard strokes. | □ | □ |
| 19 | I feel I sometimes take too much time to brush my teeth. | □ | □ |
| 20 | I have had my dentist tell me that I brush very well. | □ | □ |
| 21 | I find myself using my smartphone/computer longer than I planned. | □ | □ |
| 22 | I consume tobacco at least once a week. | □ | □ |
| 23 | I drink alcohol at least once a week. | □ | □ |
| 24 | I go to the dentist/hygienist for regular check-up at least once a year. | □ | □ |
References
- Eesti Hambaarstide Liit (EHL). Inimeste suutervise paranemine on takerdunud teadmistel põhinevate riiklike otsuste nappusesse. Available online: https://ehl.ee/inimeste-suutervise-paranemine-on-takerdunud-teadmistel-pohinevate-riiklike-otsuste-nappusesse/ (accessed on 14 January 2022).
- Hambaravi Eriala Arengukava Aastani 2020. Available online: https://www.sm.ee/sites/default/files/content-editors/eesmargid_ja_tegevused/Tervis/Tervishoiususteem/Arstide_erialade_arengukavad/hambaravi_arengukava.pdf (accessed on 14 January 2022).
- World Dental Federation (FDI). Vision 2030: Delivering Optimal Oral Health for All. Available online: https://www.fdiworlddental.org/vision2030 (accessed on 14 January 2022).
- Tartu Ülikool (TU). Hambaarstiteadus. Available online: https://ut.ee/et/oppekavad/hambaarstiteadus (accessed on 14 January 2022).
- Tartu Ülikool (TU). Promotion of Oral Health. Available online: https://ois2.ut.ee/#/courses/MVST.00.006/details (accessed on 14 January 2022).
- Tartu Ülikool (TU). Health Promotion. Available online: https://ois2.ut.ee/#/courses/ARTH.04.044/details (accessed on 14 January 2022).
- Tartu Ülikool (TU). Prevention of Oral and Dental Diseases. Available online: https://ois2.ut.ee/#/courses/ARST.01.100/details (accessed on 2 February 2022).
- Peker, I.; Alkurt, M.T. Oral Health Attitudes and Behavior among a Group of Turkish Dental Students. Eur. J. Dent. 2009, 3, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawamura, M. Dental behavioral science. The relationship between perceptions of oral health and oral status in adults. J. Hiroshima Univ. Dent. Soc. 1988, 20, 273–286. [Google Scholar] [PubMed]
- Kawamura, M.; Sasahara, H.; Kawabata, K.; Iwamoto, Y.; Konishi, K.; Wright, F.A.C. Relationship between CPITN and oral health behaviour in Japanese adults. Aust. Dent. J. 1993, 38, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, M.; Wright, F.A.C.; Declerck, D.; Freire, M.C.M.; Hu, D.Y.; Honkala, E.; Lévy, G.; Kalwitzki, M.; Polychronopoulou, A.; Yip, H.K.; et al. An exploratory study on cultural variations in oral health attitudes, behaviour and values of freshman (first-year) dental students. Int. Dent. J. 2005, 55, 205–211. [Google Scholar] [CrossRef]
- Komabayashi, T.; Kawamura, M.; Kim, K.J.; Wright, F.A.C.; Declerck, D.; Freire, M.D.C.M.; Hu, D.Y.; Honkala, E.; Lévy, G.; Kalwitzki, M.; et al. The hierarchical cluster analysis of oral health attitudes and behaviour using the Hiroshima University—Dental Behavioural Inventory (HU-DBI) among final year dental students in 17 countries. Int. Dent. J. 2006, 56, 310–316. [Google Scholar] [CrossRef]
- Wieslander, V.; Leles, C.; Srinivasan, M. Evaluation of oral-health behavioral attitudes of dental students in Switzerland and Brazil. J. Oral Sci. 2021, 63, 326–329. [Google Scholar] [CrossRef]
- Ana Rita de Sousa Saraiva Dias. Atitudes E Comportamentos de Saúde Oral em Estudantes de Medicina Dentária em Portugal E Na Holanda—Um Estudo Comparativo; Universidade Católica Portuguesa: Lisboa, Portugal, 2015. [Google Scholar]
- Komabayashi, T.; Kwan, S.Y.L.; Hu, D.Y.; Kajiwara, K.; Sasahara, H.; Kawamura, M. A comparative study of oral health attitudes and behaviour using the Hiroshima University—Dental Behavioural Inventory (HU-DBI) between dental students in Britain and China. J. Oral Sci. 2005, 47, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Olszowski, T.; Walczak, A.; Janiszewska-Olszowska, J.; Milona, M.; Higieny, Z.; Zdrowia Publicznego, E.; Uniwersytet Medyczny Szczecinie, P.; Stomatologii Ogólnej, Z. Self-assessment of oral health behaviors among dental students of Pomeranian Medical University in Szczecin. Probl. Hig. Epidemiol. 2012, 93, 798–803. [Google Scholar]
- Kawamura, M.; Honkala, E.; Widström, E.; Komabayashi, T. Cross-cultural differences of self-reported oral health behaviour in Japanese and Finnish dental students. Int. Dent. J. 2000, 50, 46–50. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. UroToday Int. J. 2007, 335, 806–808. [Google Scholar] [CrossRef] [Green Version]
- Council of European Dentists (CED). The EU Manual of Dental Practice 2015; Anthony, S., Kravitz, O.B.E., Bullock, A., Cowpe, J., Barnes, E., Eds.; Council of European Dentists (CED): Brussels, Belgium, 2015. [Google Scholar]
- TÜ Statistika. Available online: https://statistika.ut.ee/ut/?_inputs_&keel=%22en%22 (accessed on 11 January 2022).
- Total Population Sampling. Available online: https://dissertation.laerd.com/total-population-sampling.php (accessed on 11 January 2022).
- Riad, A.; Al-Khanati, N.M.; Issa, J.; Zenati, M.; Abdesslem, N.B.; Attia, S.; Krsek, M. Oral Health-Related Knowledge, Attitudes and Behaviours of Arab Dental Students: Multi-National Cross-Sectional Study and Literature Analysis 2000–2020. Int. J. Environ. Res. Public Health 2022, 19, 1658. [Google Scholar] [CrossRef]
- Al-wesabi, A.A.; Abdelgawad, F.; Sasahara, H.; El Motayam, K. Oral health knowledge, attitude and behaviour of dental students in a private university. BDJ Open 2019, 5, 1–5. [Google Scholar] [CrossRef] [Green Version]
- English Proficiency Index 2021. Available online: https://www.ef.com/wwen/epi/ (accessed on 12 January 2022).
- World Medical Association. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Proton Technologies AG General Data Protection Regulation (GDPR) Compliance Guidelines. Available online: https://gdpr.eu/ (accessed on 1 May 2020).
- SPSS Inc. IBM SPSS Statistics 28. Available online: https://www.ibm.com/support/pages/ibm-spss-statistics-28-documentation (accessed on 14 March 2021).
- Badovinac, A.; Božić, D.; Vučinac, I.; Vešligaj, J.; Vražić, D.; Plancak, D. Oral health attitudes and behavior of dental students at the University of Zagreb, Croatia. J. Dent. Educ. 2013, 77, 1171–1178. [Google Scholar] [CrossRef]
- Polychronopoulou, A.; Kawamura, M. Oral self-care behaviours: Comparing Greek and Japanese dental students. Eur. J. Dent. Educ. 2005, 9, 164–170. [Google Scholar] [CrossRef]
- Pacauskiene, I.M.; Smailiene, D.; Siudikienė, J.; Savanevskyte, J.; Nedzelskiene, I. Self-reported oral health behavior and attitudes of dental and technology students in Lithuania. Stomatologija 2014, 16, 65–71. [Google Scholar]
- Gajić, M.; Lalić, M.; Kalevski, K.; Lazić, E.; Pavlović, M.; Ivanović, M.; Milić, J.; Matijević, D.; Vojinović, J. The application of artificial intelligence algorithms for testing the correlation between the state of oral health and adolescent behavior concerning oral health. Vojnosanit. Pregl. 2021, 78, 858–864. [Google Scholar] [CrossRef] [Green Version]
- Mensi, M.; Scotti, E.; Sordillo, A.; Agosti, R.; Calza, S. Plaque disclosing agent as a guide for professional biofilm removal: A randomized controlled clinical trial. Int. J. Dent. Hyg. 2020, 18, 285–294. [Google Scholar] [CrossRef]
- Chua, H.; Sardana, D.; Turner, R.; Ting, G.; Ekambaram, M. Effectiveness of oral health education methods on oral hygiene in children and adolescents with visual impairment: A systematic review. Int. J. Paediatr. Dent. 2021, 31, 724–741. [Google Scholar] [CrossRef]
- Waldron, C.; Nunn, J.; Phadraig, C.M.G.; Comiskey, C.; Guerin, S.; van Harten, M.T.; Donnelly-Swift, E.; Clarke, M.J. Oral hygiene interventions for people with intellectual disabilities. Cochrane Database Syst. Rev. 2019, 5, CD012628. [Google Scholar] [CrossRef]
- Oliveira, L.M.; Pazinatto, J.; Zanatta, F.B. Are oral hygiene instructions with aid of plaque-disclosing methods effective in improving self-performed dental plaque control? A systematic review of randomized controlled trials. Int. J. Dent. Hyg. 2021, 19, 239–254. [Google Scholar] [CrossRef] [PubMed]
- Lujo, M.; Meštrović, M.; Malcić, A.I.; Karlović, Z.; Matijević, J.; Jukić, S. Knowledge, attitudes and habits regarding oral health in first- and final-year dental students. Acta Clin. Croat. 2016, 55, 636–643. [Google Scholar] [CrossRef] [Green Version]
- Dumitrescu, A.L.; Kawamura, M.; Sasahara, H. An assessment of oral self-care among Romanian dental students using the Hiroshima University—Dental Behavioural Inventory. Oral Health Prev. Dent. 2007, 5, 95–100. [Google Scholar] [PubMed]
- Voelker, M.A.; Bayne, S.C.; Liu, Y.; Walker, M.P. Catalogue of Tooth Brush Head Designs. Am. Dent. Hyg. Assoc. 2013, 87, 118–133. [Google Scholar]
- Mehta, S.; Vyaasini, C.V.S.; Jindal, L.; Sharma, V.; Jasuja, T. Toothbrush, its design and modifications: An Overview. J. Curr. Med. Res. Opin. 2020, 3, 570. [Google Scholar] [CrossRef]
- Sharma, N.C.; Qaqish, J.G.; Galustians, H.J.; Goyal, C.R.; Cugini, M.A.; Thompson, M.C.; Warren, P.R. Plaque removal efficacy of two electric toothbrushes with different brush head designs. J. Dent. 2005, 33, 17–21. [Google Scholar] [CrossRef]
- Sasan, D.; Thomas, B.; Bhat, M.; Aithal, K.; Ramesh, P. Toothbrush selection: A dilemma? Indian J. Dent. Res. 2006, 17, 167. [Google Scholar] [CrossRef]
- Cronin, M.J.; Dembling, W.Z.; Low, M.A.; Jacobs, D.M.; Weber, D.A. A comparative clinical investigation of a novel toothbrush designed to enhance plaque removal efficacy. Am. J. Dent. 2000, 13, 21A–26A. [Google Scholar]
- Ng, C.; Tsoi, J.K.H.; Lo, E.C.M.; Matinlinna, J.P. Safety and Design Aspects of Powered Toothbrush—A Narrative Review. Dent. J. 2020, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Valkenburg, C.; Slot, D.E.; Bakker, E.W.P.; Van der Weijden, F.A. Does dentifrice use help to remove plaque? A systematic review. J. Clin. Periodontol. 2016, 43, 1050–1058. [Google Scholar] [CrossRef]
- Economou, G.C. Dental Anxiety and Personality: Investigating the Relationship Between Dental Anxiety and Self-Consciousness. J. Dent. Educ. 2003, 67, 970–980. [Google Scholar] [CrossRef]
- Storjord, H.P.; Teodorsen, M.M.; Bergdahl, J.; Wynn, R.; Johnsen, J.A.K. Dental anxiety: A comparison of students of dentistry, biology, and psychology. J. Multidiscip. Healthc. 2014, 7, 413. [Google Scholar] [CrossRef] [Green Version]
- Yaghooti, K.M.; Sistani, F. Dental Fear and Anxiety among Students of Rafsanjan University of Medical Sciences; Sabzevar University of Medical Sciences: Abaresh, Iran, 2014. [Google Scholar]
- MARYAM, G.; AZAM, H. Dental Fear and Anxiety Among Dental and Medical Students of Babol University of Medical Sciences. J. Islam. Dent. Assoc. IRAN 2005, 17, 9–14. [Google Scholar]
- Kirova, D.G. Dental anxiety among dental students. J. IMAB-Annu. Proceeding 2011, 17, 137–139. [Google Scholar] [CrossRef] [Green Version]
- Farooq, I.; Ali, S. A cross sectional study of gender differences in dental anxiety prevailing in the students of a Pakistani dental college. Saudi J. Dent. Res. 2015, 6, 21–25. [Google Scholar] [CrossRef] [Green Version]
- Peretz, B.; Mann, J. Dental anxiety among Israeli dental students: A 4-year longitudinal study. Eur. J. Dent. Educ. 2000, 4, 133–137. [Google Scholar] [CrossRef]
- Langa, G.P.J.; Muniz, F.W.M.G.; Wagner, T.P.; Silva, C.F.; Rösing, C.K. Anti-Plaque and Anti-Gingivitis Efficacy of Different Bristle Stiffness and End-Shape Toothbrushes on Interproximal Surfaces: A Systematic Review with Meta-Analysis. J. Evid. Based Dent. Pract. 2021, 21, 101548. [Google Scholar] [CrossRef]
- Ranzan, N.; Muniz, F.W.M.G.; Rösing, C.K. Are bristle stiffness and bristle end-shape related to adverse effects on soft tissues during toothbrushing? A systematic review. Int. Dent. J. 2019, 69, 171–182. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health Development (NIHD). Estonian Health Statistics and Health Research Database. Available online: https://statistika.tai.ee/index.html (accessed on 14 January 2022).
- Reile, R.; Veideman, T. Eesti Täiskasvanud Rahvastiku Tervisekäitumise Uuring 2020. Available online: https://tai.ee/et/valjaanded/eesti-taiskasvanud-rahvastiku-tervisekaitumise-uuring-2020 (accessed on 14 January 2022).
- Monaghan, N. What is the role of dentists in smoking cessation? Br. Dent. J. 2002, 193, 611–612. [Google Scholar] [CrossRef]
- Stacey, F.; Heasman, P.A.; Heasman, L.; Hepburn, S.; McCracken, G.I.; Preshaw, P.M. Smoking cessation as a dental intervention—Views of the profession. Br. Dent. J. 2006, 201, 109–113. [Google Scholar] [CrossRef]
- Harada, S.; Akhter, R.; Kurita, K.; Mori, M.; Hoshikoshi, M.; Tamashiro, H.; Morita, M. Relationships between lifestyle and dental health behaviors in a rural population in Japan. Community Dent. Oral Epidemiol. 2005, 33, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacios, C.; Joshipura, K.J.; Willett, W.C. Nutrition and health: Guidelines for dental practitioners. Oral Dis. 2009, 15, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Vann, W.F.; Bouwens, T.J.; Braithwaite, A.S.; Lee, J.Y. The Childhood Obesity Epidemic: A Role for Pediatric Dentists? Health Educ. 2009, 109, 507–521. [Google Scholar] [CrossRef]
- Braithwaite, A.S.; Vann, W.F.J.; Switzer, B.R.; Boyd, K.L.; Lee, J.Y. Nutritional counseling practices: How do North Carolina pediatric dentists weigh in? Pediatr. Dent. 2008, 30, 488–495. [Google Scholar]
- Riad, A.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E. Global Prevalence and Drivers of Dental Students’ COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 566. [Google Scholar] [CrossRef]
- Kateeb, E.; Danadneh, M.; Pokorná, A.; Klugarová, J.; Abdulqader, H.; Klugar, M.; Riad, A. Predictors of Willingness to Receive COVID-19 Vaccine: Cross-Sectional Study of Palestinian Dental Students. Vaccines 2021, 9, 954. [Google Scholar] [CrossRef]
- Riad, A.; Huang, Y.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E. IADS-SCORE Universal Predictors of Dental Students’ Attitudes towards COVID-19 Vaccination: Machine Learning-Based Approach. Vaccines 2021, 9, 1158. [Google Scholar] [CrossRef]
- Vollath, S.E.; Bobak, A.; Jackson, S.; Sennhenn-Kirchner, S.; Kanzow, P.; Wiegand, A.; Raupach, T. Effectiveness of an innovative and interactive smoking cessation training module for dental students: A prospective study. Eur. J. Dent. Educ. 2020, 24, 361–369. [Google Scholar] [CrossRef]
- Reile, R.; Pärna, K. E-Cigarette Use by Smoking Status in Estonia, 2012–2018. Int. J. Environ. Res. Public Health 2020, 17, 519. [Google Scholar] [CrossRef] [Green Version]
- World Bank Prevalence of Current Tobacco Use (% of adults)—Estonia|Data. Available online: https://data.worldbank.org/indicator/SH.PRV.SMOK?locations=EE (accessed on 14 January 2022).
- Rodakowska, E.; Mazur, M.; Baginska, J.; Sierpinska, T.; La Torre, G.; Ottolenghi, L.; D’egidio, V.; Guerra, F. Smoking Prevalence, Attitudes and Behavior among Dental Students in Poland and Italy. Int. J. Environ. Res. Public Health 2020, 17, 7451. [Google Scholar] [CrossRef]
- World Bank Prevalence of Current Tobacco Use (% of adults)—Italy|Data. Available online: https://data.worldbank.org/indicator/SH.PRV.SMOK?locations=IT (accessed on 2 February 2022).
- World Bank Prevalence of Current Tobacco Use (% of adults)—Poland|Data. Available online: https://data.worldbank.org/indicator/SH.PRV.SMOK?locations=PL (accessed on 2 February 2022).
- Pärna, K.; Põld, M.; Ringmets, I. Trends in smoking behaviour among Estonian physicians in 1982-2014. BMC Public Health 2017, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Mekhemar, M.; Conrad, J.; Attia, S.; Dörfer, C. Oral Health Attitudes among Preclinical and Clinical Dental Students in Germany. Int. J. Environ. Res. Public Health 2020, 17, 4253. [Google Scholar] [CrossRef]
- Yildiz, S.; Dogan, B. Self reported dental health attitudes and behaviour of dental students in Turkey. Eur. J. Dent. 2011, 5, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Virtanen, J.I.; Filppula, M.; Maldupa, I.; Patja, K. Smoking and attitudes towards it and its cessation among dental students in Latvia. Acta Odontol. Scand. 2015, 73, 421–426. [Google Scholar] [CrossRef]
- Basudan, S.; Binanzan, N.; Alhassan, A. Depression, anxiety and stress in dental students. Int. J. Med. Educ. 2017, 8, 179. [Google Scholar] [CrossRef] [Green Version]
- Elani, H.W.; Allison, P.J.; Kumar, R.A.; Mancini, L.; Lambrou, A.; Bedos, C. A Systematic Review of Stress in Dental Students. J. Dent. Educ. 2014, 78, 226–242. [Google Scholar] [CrossRef]
- Spada, M.M. An overview of problematic Internet use. Addict. Behav. 2014, 39, 3–6. [Google Scholar] [CrossRef]
- Aboujaoude, E. Problematic Internet use: An overview. World Psychiatry 2010, 9, 85. [Google Scholar] [CrossRef] [Green Version]
- Šmahel, D.; Blinka, L. Excessive Internet Use among European Children. In Children, Risk and Safety on the Internet: Research and Policy Challenges in Comparative Perspective; The Policy Press: Bristol, UK, 2012; pp. 191–204. [Google Scholar]
- Europe Internet Stats—Population Statistics. Available online: https://www.internetworldstats.com/europa2.htm (accessed on 14 January 2022).
- Kaess, M.; Parzer, P.; Brunner, R.; Koenig, J.; Durkee, T.; Carli, V.; Wasserman, C.; Hoven, C.W.; Sarchiapone, M.; Bobes, J.; et al. Pathological Internet Use Is on the Rise Among European Adolescents. J. Adolesc. Heal. 2016, 59, 236–239. [Google Scholar] [CrossRef]



| Variable | Outcome | Frequency (n) | Percentage (%) |
|---|---|---|---|
| Gender | Female | 98 | 79% |
| Male | 26 | 21% | |
| Academic Level | First Year | 21 | 16.9% |
| Second Year | 26 | 21% | |
| Third Year | 24 | 19.4% | |
| Fourth Year | 23 | 18.5% | |
| Fifth Year | 30 | 24.2% | |
| Clinical Experience | Preclinical | 47 | 37.9% |
| Clinical | 77 | 62.1% |
| Variable | Outcome | Female (n = 98) | Male (n = 26) | α. | Preclinical (n = 47) | Clinical (n = 77) | α. | Total (n = 124) |
|---|---|---|---|---|---|---|---|---|
| Tobacco Smoking | Yes | 5 (5.1%) | 9 (34.6%) | <0.001 | 2 (4.3%) | 12 (15.6%) | 0.053 | 14 (11.3%) |
| No | 93 (94.9%) | 17 (65.4%) | 45 (95.7%) | 65 (84.4%) | 110 (88.7%) | |||
| Alcohol Drinking | Yes | 12 (12.2%) | 8 (30.8%) | 0.034 * | 4 (8.5%) | 16 (20.8%) | 0.072 | 20 (16.1%) |
| No | 86 (87.8%) | 18 (69.2%) | 43 (91.5%) | 61 (79.2%) | 104 (83.9%) | |||
| Problematic Internet Use | Yes | 85 (86.7%) | 22 (84.6%) | 0.754 * | 36 (76.6%) | 71 (92.2%) | 0.014 | 107 (86.3%) |
| No | 13 (13.3%) | 4 (15.4%) | 11 (23.4%) | 6 (7.8%) | 17 (13.7%) | |||
| Regular Check-up | Yes | 89 (90.8%) | 24 (92.3%) | 1.000 * | 45 (95.7%) | 68 (88.3%) | 0.204 * | 113 (91.1%) |
| No | 9 (9.2%) | 2 (7.7%) | 2 (4.3%) | 9 (11.7%) | 11 (8.9%) |
| Item | Outcome | 1st Year (n = 21) | 2nd Year (n = 26) | 3rd Year (n = 24) | 4th Year (n = 23) | 5th Year (n = 30) | α. | Total (n = 124) |
|---|---|---|---|---|---|---|---|---|
| No. 1 | Agree | 10 (47.6%) | 24 (92.3%) | 11 (45.8%) | 20 (87%) | 20 (66.7%) | 0.087 | 85 (68.5%) |
| No. 2 | Disagree | 20 (95.2%) | 25 (96.2%) | 23 (95.8%) | 23 (100%) | 30 (100%) | 0.114 | 121 (97.6%) |
| No. 3 | Agree | 12 (57.1%) | 12 (46.2%) | 17 (70.8%) | 12 (52.2%) | 11 (36.7%) | 0.074 | 64 (51.6%) |
| No. 4 | Agree | 4 (19%) | 5 (19.2%) | 5 (20.8%) | 6 (26.1%) | 5 (16.7%) | 0.413 | 25 (20.2%) |
| No. 5 | Agree | 3 (14.3%) | 5 (19.2%) | 0 (0%) | 1 (4.3%) | 3 (10%) | 0.320 | 12 (9.7%) |
| No. 6 | Disagree | 16 (76.2%) | 20 (76.9%) | 21 (87.5%) | 20 (87%) | 26 (86.7%) | 0.167 | 103 (83.1%) |
| No. 7 | Agree | 4 (19%) | 5 (19.2%) | 4 (16.7%) | 3 (13%) | 2 (6.7%) | 0.088 | 18 (14.5%) |
| No. 8 | Disagree | 19 (90.5%) | 24 (92.3%) | 23 (95.8%) | 21 (91.3%) | 25 (83.3%) | 0.233 | 112 (90.3%) |
| No. 9 | Agree | 19 (90.5%) | 24 (92.3%) | 24 (100%) | 22 (95.7%) | 29 (96.7%) | 0.178 | 118 (95.2%) |
| No. 10 | Disagree | 17 (81%) | 25 (96.2%) | 17 (70.8%) | 18 (78.3%) | 26 (86.7%) | 0.290 | 103 (83.1%) |
| No. 11 | Agree | 1 (4.8%) | 6 (23.1%) | 2 (8.3%) | 3 (13%) | 5 (16.7%) | 0.097 | 17 (13.7%) |
| No. 12 | Agree | 17 (81%) | 20 (76.9%) | 20 (83.3%) | 16 (69.6%) | 22 (73.3%) | 0.264 | 95 (76.6%) |
| No. 13 | Agree | 18 (85.7%) | 13 (50%) | 17 (70.8%) | 15 (65.2%) | 20 (66.7%) | 0.062 | 83 (66.9%) |
| No. 14 | Disagree | 19 (90.5%) | 14 (53.8%) | 12 (50%) | 14 (60.9%) | 13 (43.3%) | <0.001 | 72 (58.1%) |
| No. 15 | Disagree | 20 (95.2%) | 25 (96.2%) | 24 (100%) | 22 (95.7%) | 30 (100%) | 0.114 | 121 (97.6%) |
| No. 16 | Agree | 10 (47.6%) | 14 (53.8%) | 12 (50%) | 10 (43.5%) | 22 (73.3%) | 0.031 | 68 (54.8%) |
| No. 17 | Agree | 4 (19%) | 4 (15.4%) | 2 (8.3%) | 1 (4.3%) | 1 (3.3%) | 0.032 | 12 (9.7%) |
| No. 18 | Agree | 4 (19%) | 2 (7.7%) | 2 (8.3%) | 0 (0%) | 1 (3.3%) | 0.032 | 9 (7.3%) |
| No. 19 | Agree | 10 (47.6%) | 10 (38.5%) | 10 (41.7%) | 9 (39.1%) | 9 (30%) | 0.100 | 48 (38.7%) |
| No. 20 | Agree | 14 (66.7%) | 15 (57.7%) | 20 (83.3%) | 20 (87%) | 20 (66.7%) | 0.500 | 89 (71.8%) |
| Item | Outcome | Female (n = 98) | Male (n = 26) | α. | Preclinical (n = 47) | Clinical (n = 77) | α. | Smoker (n = 14) | Nonsmoker (n = 110) | α. |
|---|---|---|---|---|---|---|---|---|---|---|
| No. 1 | Agree | 68 (69.4%) | 17 (65.4%) | 0.696 | 34 (72.3%) | 51 (66.2%) | 0.477 | 8 (57.1%) | 77 (70%) | 0.366 * |
| No. 2 | Disagree | 96 (98%) | 25 (96.2%) | 0.510 * | 45 (95.7%) | 76 (98.7%) | 0.557 * | 13 (92.9%) | 108 (98.2%) | 0.304 * |
| No. 3 | Agree | 50 (51%) | 14 (53.8%) | 0.798 | 24 (51.1%) | 40 (51.9%) | 0.924 | 12 (85.7%) | 52 (47.3%) | 0.007 |
| No. 4 | Agree | 19 (19.4%) | 6 (23.1%) | 0.677 | 9 (19.1%) | 16 (20.8%) | 0.826 | 3 (21.4%) | 22 (20%) | 1.000 * |
| No. 5 | Agree | 11 (11.2%) | 1 (3.8%) | 0.457 * | 8 (17%) | 4 (5.2%) | 0.056 * | 1 (7.1%) | 11 (10%) | 1.000 * |
| No. 6 | Disagree | 81 (82.7%) | 22 (84.6%) | 1.000 * | 36 (76.6%) | 67 (87%) | 0.133 | 13 (92.9%) | 90 (81.8%) | 0.461 * |
| No. 7 | Agree | 13 (13.3%) | 5 (19.2%) | 0.531 * | 9 (19.1%) | 9 (11.7%) | 0.253 | 2 (14.3%) | 16 (14.5%) | 1.000 * |
| No. 8 | Disagree | 89 (90.8%) | 23 (88.5%) | 0.714 * | 43 (91.5%) | 69 (89.6%) | 1.000 * | 12 (85.7%) | 100 (90.9%) | 0.625 |
| No. 9 | Agree | 93 (94.9%) | 25 (96.2%) | 1.000 * | 43 (91.5%) | 75 (97.4%) | 0.199 * | 12 (85.7%) | 106 (96.4%) | 0.137 * |
| No. 10 | Disagree | 81 (82.7%) | 22 (84.6%) | 1.000 * | 42 (89.4%) | 61 (79.2%) | 0.144 | 14 (100%) | 89 (80.9%) | 0.124 * |
| No. 11 | Agree | 16 (16.3%) | 1 (3.8%) | 0.120 * | 7 (14.9%) | 10 (13%) | 0.765 | 2 (14.3%) | 15 (13.6%) | 1.000 * |
| No. 12 | Agree | 78 (79.6%) | 17 (65.4%) | 0.128 | 37 (78.7%) | 58 (75.3%) | 0.664 | 12 (85.7%) | 83 (75.5%) | 0.517 * |
| No. 13 | Agree | 63 (64.3%) | 20 (76.9%) | 0.223 | 31 (66%) | 52 (67.5%) | 0.856 | 13 (92.9%) | 70 (63.6%) | 0.034 * |
| No. 14 | Disagree | 58 (59.2%) | 14 (53.8%) | 0.624 | 33 (70.2%) | 39 (50.6%) | 0.032 | 7 (50%) | 65 (59.1%) | 0.516 |
| No. 15 | Disagree | 96 (98%) | 25 (96.2%) | 0.510 * | 45 (95.7%) | 76 (98.7%) | 0.557 * | 14 (100%) | 107 (97.3%) | 1.000 * |
| No. 16 | Agree | 56 (57.1%) | 12 (46.2%) | 0.317 | 24 (51.1%) | 44 (57.1%) | 0.509 | 7 (50%) | 61 (55.5%) | 0.699 |
| No. 17 | Agree | 9 (9.2%) | 3 (11.5%) | 0.714 * | 8 (17%) | 4 (5.2%) | 0.056 * | 3 (21.4%) | 9 (8.2%) | 0.136 * |
| No. 18 | Agree | 6 (6.1%) | 3 (11.5%) | 0.395 * | 6 (12.8%) | 3 (3.9%) | 0.081 * | 1 (7.1%) | 8 (7.3%) | 1.000 * |
| No. 19 | Agree | 37 (37.8%) | 11 (42.3%) | 0.672 | 20 (42.6%) | 28 (36.4%) | 0.492 | 6 (42.9%) | 42 (38.2%) | 0.735 |
| No. 20 | Agree | 69 (70.4%) | 20 (76.9%) | 0.512 | 29 (61.7%) | 60 (77.9%) | 0.052 | 10 (71.4%) | 79 (71.8%) | 1.000* |
| Variable | Outcome | Knowledge (0–5) | α. | Attitudes (0–3) | α. | Behaviours (0–4) | α. | HU-DBI Score (0–12) | α. |
|---|---|---|---|---|---|---|---|---|---|
| Gender | Female | 4.07 ± 0.68 | 0.485 | 1.58 ± 0.72 | 0.146 | 2.51 ± 0.78 | 0.114 | 8.16 ± 1.23 | 0.093 |
| Male | 4.08 ± 0.56 | 1.42 ± 0.50 | 2.31 ± 0.68 | 7.81 ± 1.13 | |||||
| Academic Level | 1st Year | 4.10 ± 0.89 | 0.245 | 1.71 ± 0.64 | 0.376 | 2.38 ± 0.81 | 0.402 | 8.19 ± 1.47 | 0.686 |
| 2nd Year | 4.19 ± 0.63 | 1.54 ± 0.91 | 2.42 ± 0.81 | 8.15 ± 1.29 | |||||
| 3rd Year | 4.04 ± 0.46 | 1.46 ± 0.59 | 2.54 ± 0.88 | 8.04 ± 1.30 | |||||
| 4th Year | 4.04 ± 0.64 | 1.61 ± 0.58 | 2.35 ± 0.83 | 8.00 ± 1.09 | |||||
| 5th Year | 4.00 ± 0.64 | 1.47 ± 0.63 | 2.60 ± 0.50 | 8.07 ± 1.05 | |||||
| Clinical Experience | Preclinical | 4.15 ± 0.75 | 0.170 | 1.62 ± 0.80 | 0.207 | 2.40 ± 0.80 | 0.235 | 8.17 ± 1.36 | 0.281 |
| Clinical | 4.03 ± 0.58 | 1.51 ± 0.60 | 2.51 ± 0.74 | 8.04 ± 1.13 | |||||
| Tobacco Smoking | Yes | 4.21 ± 0.58 | 0.195 | 1.57 ± 0.65 | 0.447 | 2.43 ± 0.76 | 0.419 | 8.21 ± 1.19 | 0.342 |
| No | 4.05 ± 0.66 | 1.55 ± 0.69 | 2.47 ± 0.76 | 8.07 ± 1.22 | |||||
| Alcohol Drinking | Yes | 4.05 ± 0.61 | 0.433 | 1.50 ± 0.61 | 0.365 | 2.45 ± 0.76 | 0.455 | 8.00 ± 1.08 | 0.362 |
| No | 4.08 ± 0.66 | 1.56 ± 0.69 | 2.47 ± 0.76 | 8.11 ± 1.25 | |||||
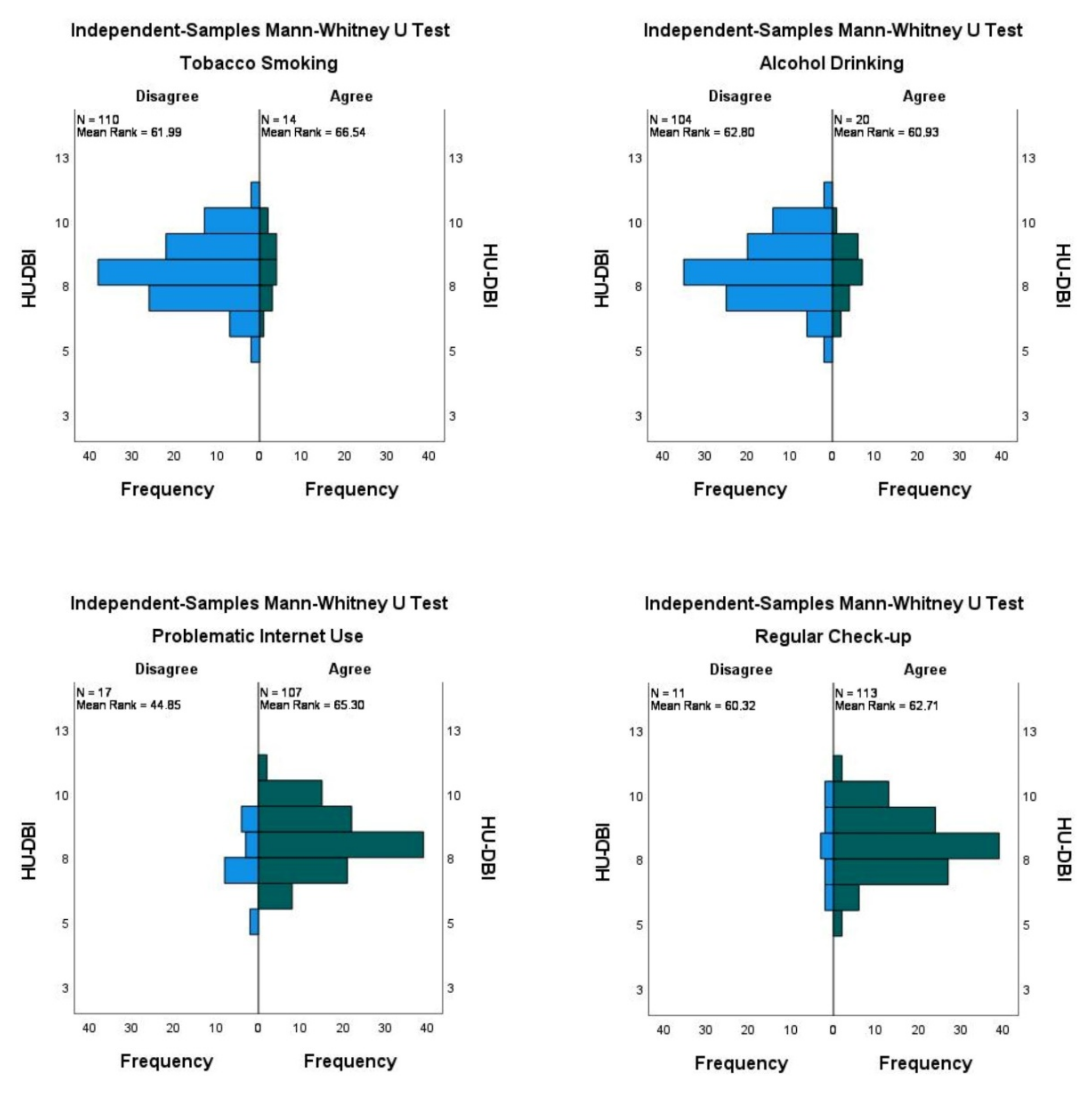
| Problematic Internet Use | Yes | 4.09 ± 0.62 | 0.187 | 1.57 ± 0.66 | 0.187 | 2.53 ± 0.74 | 0.008 | 8.20 ± 1.19 | 0.006 |
| No | 3.94 ± 0.83 | 1.41 ± 0.80 | 2.06 ± 0.75 | 7.41 ± 1.23 | |||||
| Regular Check-up | Yes | 4.07 ± 0.66 | 0.923 | 1.54 ± 0.67 | 0.654 | 2.49 ± 0.77 | 0.374 | 8.10 ± 1.20 | 0.801 |
| No | 4.09 ± 0.54 | 1.64 ± 0.81 | 2.27 ± 0.65 | 8.00 ± 1.41 |
| Pair | Knowledge (0–5) | α. | Attitudes (0–3) | α. | Behaviours (0–4) | α. | HU-DBI Score (0–12) | α. |
|---|---|---|---|---|---|---|---|---|
| 1st Year vs. 2nd Year | 23.67/24.27 | 0.870 | 25.79/22.56 | 0.384 | 23.79/24.17 | 0.918 | 24.79/23.37 | 0.718 |
| 2nd Year vs. 3rd Year | 27.17/23.69 | 0.304 | 26.21/24.73 | 0.695 | 24.52/26.56 | 0.597 | 26.19/24.75 | 0.717 |
| 3rd Year vs. 4th Year | 23.94/24.07 | 0.968 | 22.35/25.72 | 0.341 | 25.56/22.37 | 0.396 | 23.52/24.50 | 0.798 |
| 4th Year vs. 5th Year | 27.52/26.60 | 0.805 | 28.26/26.03 | 0.556 | 23.87/29.40 | 0.152 | 26.50/27.38 | 0.829 |
| Predictor | Beta | S.E. | Wald | df | AOR | 95% CI | α. |
|---|---|---|---|---|---|---|---|
| Gender: Male | 2.18 | 0.71 | 9.35 | 1 | 8.84 | 2.19–35.70 | 0.002 |
| Experience: Clinical Students | 1.00 | 0.88 | 1.30 | 1 | 2.73 | 0.49–15.30 | 0.253 |
| Alcohol Drinking: Yes | 1.20 | 0.79 | 2.30 | 1 | 3.32 | 0.70–15.67 | 0.129 |
| Problematic Internet Use: Yes | 0.46 | 1.20 | 0.15 | 1 | 1.58 | 0.15–16.45 | 0.704 |
| Item No. 3: Agree | 1.69 | 0.90 | 3.53 | 1 | 5.41 | 0.93–31.46 | 0.060 |
| Item No. 13: Agree | 1.15 | 1.15 | 1.00 | 1 | 3.15 | 0.33–30.00 | 0.318 |
| Observed Group | Predicted Group | Correct Percentage | ||
|---|---|---|---|---|
| Nonsmoker | Smoker | |||
| Tobacco Smoking | Nonsmoker | 106 | 4 | 96.4% |
| Smoker | 8 | 6 | 42.9% | |
| Overall | 90.3% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riad, A.; Põld, A.; Olak, J.; Howaldt, H.-P.; Klugar, M.; Krsek, M.; Attia, S. Estonian Dental Students’ Oral Health-Related Knowledge, Attitudes and Behaviours (KAB): National Survey-Based Study. Int. J. Environ. Res. Public Health 2022, 19, 1908. https://doi.org/10.3390/ijerph19031908
Riad A, Põld A, Olak J, Howaldt H-P, Klugar M, Krsek M, Attia S. Estonian Dental Students’ Oral Health-Related Knowledge, Attitudes and Behaviours (KAB): National Survey-Based Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1908. https://doi.org/10.3390/ijerph19031908
Chicago/Turabian StyleRiad, Abanoub, Ave Põld, Jana Olak, Hans-Peter Howaldt, Miloslav Klugar, Martin Krsek, and Sameh Attia. 2022. "Estonian Dental Students’ Oral Health-Related Knowledge, Attitudes and Behaviours (KAB): National Survey-Based Study" International Journal of Environmental Research and Public Health 19, no. 3: 1908. https://doi.org/10.3390/ijerph19031908