
The Effect of Core Stabilization Exercise with the Abdominal Drawing-in Maneuver Technique on Stature Change during Prolonged Sitting in Sedentary Workers with Chronic Low Back Pain


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Participants
2.3. Sample Size Determination
2.4. Outcome Measurements
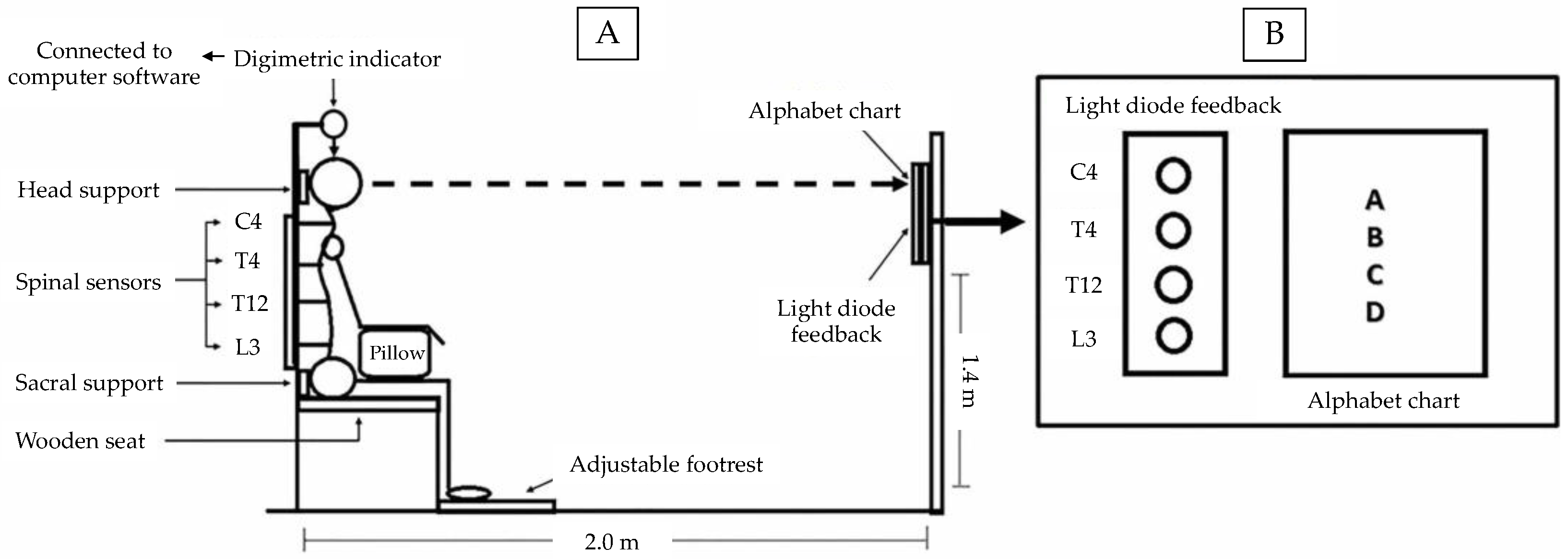
2.4.1. Stature Change Response
2.4.2. Trunk Muscle Fatigue
2.4.3. Pain Rating Scale
2.4.4. Functional Disability
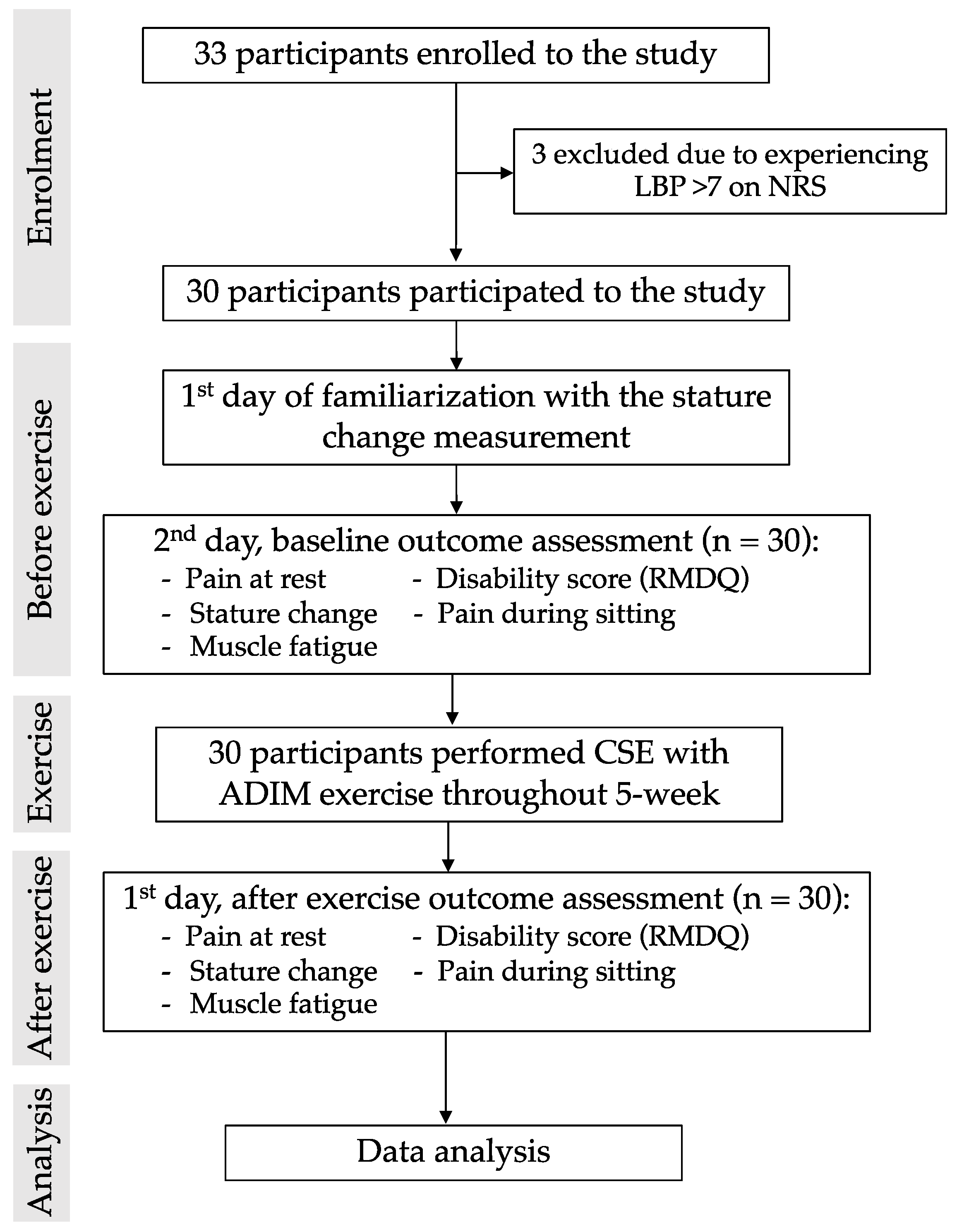
2.5. Procedure
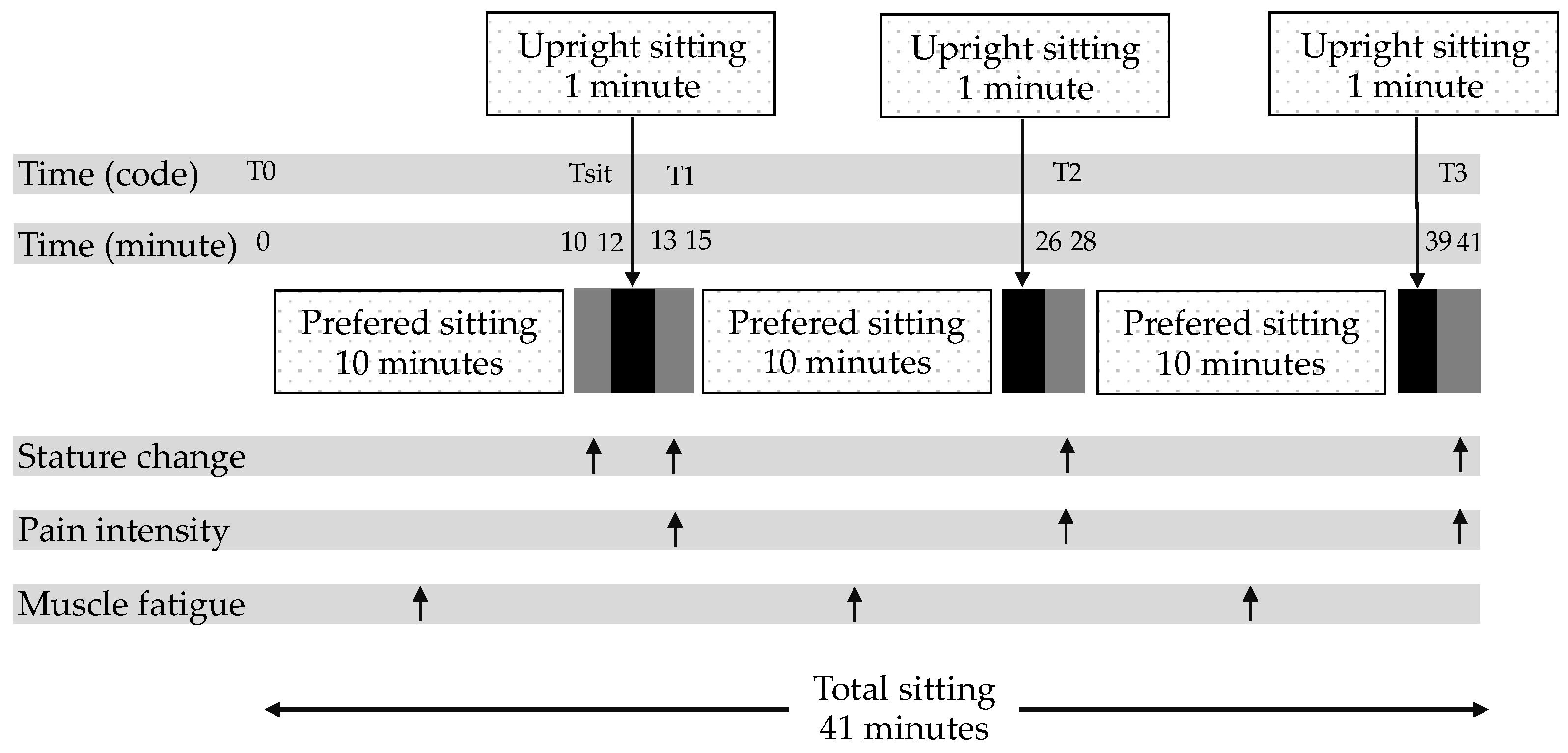
2.6. Prolonged Sitting Condition
2.7. Core Stabilization Exercise (CSE) with ADIM Technique
2.8. Data Analysis
3. Results
3.1. Participant Characteristics
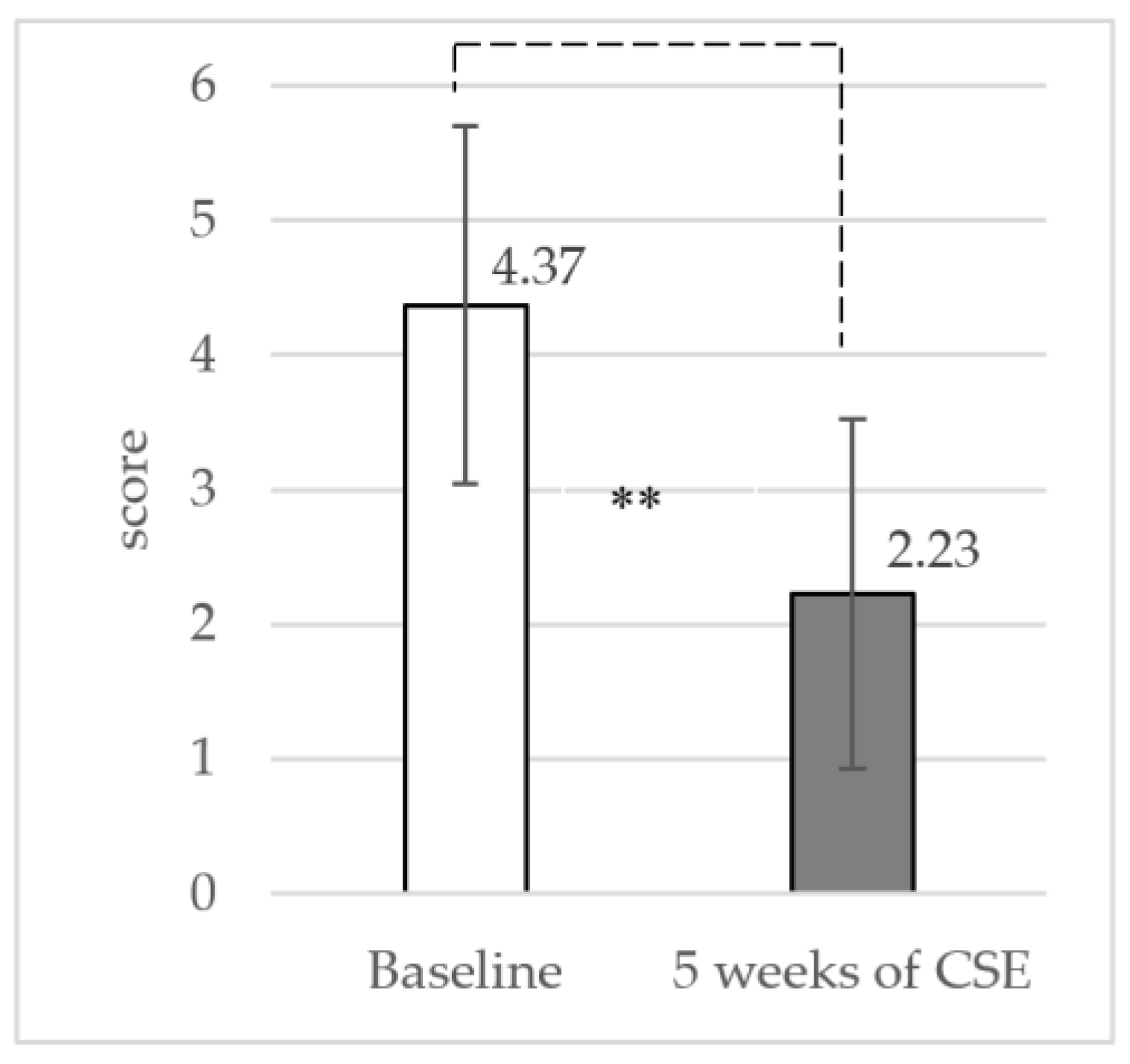
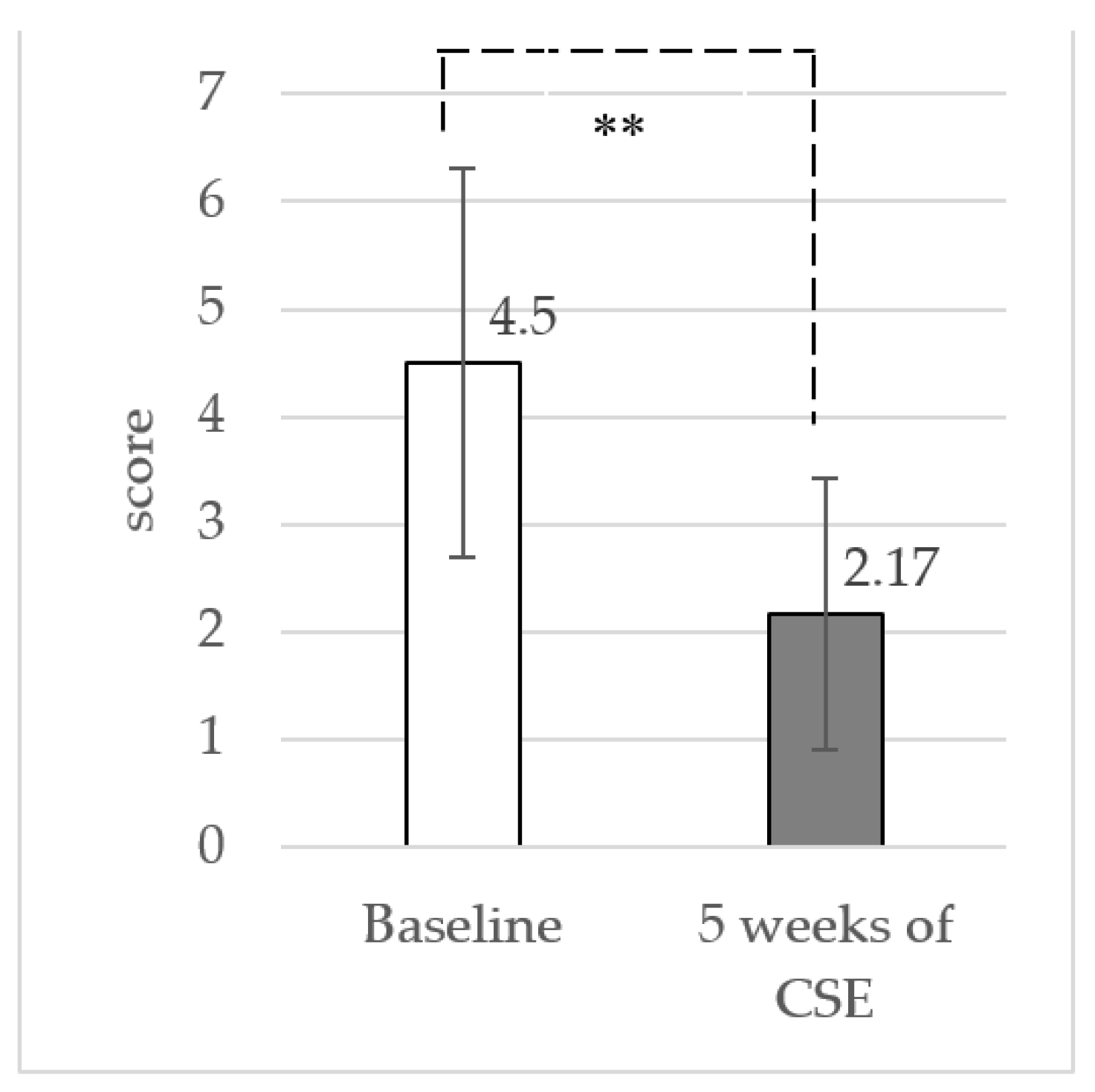
3.2. Pain Intensity at Rest and Functional Disability
3.3. Stature Changes during Sitting
3.4. Pain Intensity during Sitting
3.5. Trunk Muscle Fatigue during the Experiment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week | Exercise Protocol |
|---|---|
| 1 | The participants were given the instructions on how to isolate activation of the TrA muscles correctly. After that, they were asked to draw their lower abdomen gently in towards the spine (ADIM) with normal breathing control, and no movement of the spine and pelvis while in a prone lying position on a couch with a small pillow placed beneath their ankles. In addition, a pressure biofeedback device set at 70 mmHg was placed under the lower abdomen of the participants. If they were able to lower pressure 4 to 10 mmHg, it represented successful activation of the transversus abdominis muscle. The exercises progressed until the participants could perform muscle contractions for 10 s holds with 10 repetitions/set 10 sets/day. |
| 2 | The participants performed co-contraction of the TrA and LM muscles while in a crooked lying position with both hips at 45 degrees and both knees at 90 degrees. They were asked to perform the ADIM technique with floor muscles, normal breathing control, and no movement of the spine and pelvis. Furthermore, they used their index and middle fingers to palpate contraction of the TrA muscle and opposite 2 fingers palpated contraction of LM muscle. If the participants performed correctly, they could feel the tight contraction of each muscle under their fingers. The exercises progressed until the participants could perform muscle contractions for 10 s holds with 10 repetitions/set 10 sets/day. |
| 3 | The participants performed co-contraction of the TrA and LM muscles in a crooked lying position with both hips at 45 degrees and both knees at 90 degrees. Then, they abducted one leg to 45 degrees of hip abduction and held it for 10 s. After that, they adducted their leg to the starting position. After repeating this movement 5 times, they did it with the other leg/set 10 sets/day. The next exercise in this week was to train co-contraction of these muscles in a crooked lying position with both hips at 45 degrees and both knees at 90 degrees. Then, they slid a single leg down until the knee was straight, maintained it for a 10 s hold, and then slid it back up to the starting position. After repeating this movement 10 times, they did it with the other leg/set 10 sets/day. |
| 4 | The participants performed co-contraction of the TrA and LM muscles while sitting on a chair. They were asked to perform the ADIM technique with normal breathing control, and no movement of the spine and pelvis. Furthermore, they used their index and middle fingers to palpate contraction of the TrA muscle and opposite 2 fingers palpated contraction of the LM muscle. If the participants performed correctly, they could feel the tight contraction of each muscle under their fingers. The exercises progressed until the participants could perform muscle contractions for 10 s holds with 10 repetitions/set 10 sets/day. The next exercise in this week was to train co-contraction of these muscles with the trunk forward and backward while sitting on a chair and keeping their lumbar spine and pelvis in a neutral position. The second exercise in this week required 10 s holds with 10 repetitions/set 10 sets/day. |
| 5 | The participants performed co-contraction of the TrA and LM muscles during sitting on a balance board. They were asked to perform co-contraction of the muscles with the trunk forward and backward while sitting on a balance board and keeping their lumbar spine and pelvis in a neutral position. They performed each pose for 10 s holds with 10 repetitions/set 10 sets/day. |
References
- Sedentary Behaviour Research Network. Letter to the editor: Standardized use of the terms “sedentary” and “sedentary behav- iours”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadgraft, N.T.; Lynch, B.M.; Clark, B.K.; Healy, G.N.; Owen, N.; Dunstan, D.W. Excessive sitting at work and at home: Correlates of occupational sitting and TV viewing time in working adults. BMC Public Health 2015, 15, 899. [Google Scholar] [CrossRef] [Green Version]
- Saidj, M.; Menai, M.; Charreire, H.; Weber, C.; Enaux, C.; Aadahl, M.; Kesse-Guyot, E.; Hercberg, S.; Simon, C.; Oppert, J.M. Descriptive study of sedentary behaviours in 35,444 French working adults: Cross-sectional findings from the ACTI-Cités study. BMC Public Health 2015, 15, 379. [Google Scholar] [CrossRef] [PubMed]
- Montakarn, C.; Nuttika, N. Physical activity levels and prevalence of low back pain in Thai call-center operators. Indian J. Occup. Environ. Med. 2016, 20, 125–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balagué, F.; Mannion, A.F.; Pellisé, F.; Cedraschi, C. Non-specific low back pain. Lancet 2012, 379, 482–491. [Google Scholar] [CrossRef] [Green Version]
- Jiménez, R.; Bennett, P.; García, O.; Vargas, C. Fatigue detection during sit-to-stand test based on surface electromyography and acceleration: A case study. Sensors 2019, 19, 4202. [Google Scholar] [CrossRef] [Green Version]
- Olafsson, G.; Jonsson, E.; Fritzell, P.; Hägg, O.; Borgström, F. A health economic lifetime treatment pathway model for low back pain in Sweden. J. Med. Econ. 2017, 20, 1281–1289. [Google Scholar] [CrossRef] [PubMed]
- Saiklang, P.; Puntumetakul, R.; Selfe, J.; Yeowell, G. An Evaluation of an Innovative Exercise to Relieve Chronic Low Back Pain in Sedentary Workers. Available online: https://pubmed.ncbi.nlm.nih.gov/33111563/ (accessed on 22 December 2021).
- Waongenngarm, P.; Rajaratnam, B.S.; Janwantanakul, P. Internal oblique and transversus abdominis muscle fatigue induced by slumped sitting posture after 1 h of sitting in office workers. Saf. Health Work 2016, 7, 49–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Areeudomwong, P.; Puntumetakul, R.; Kaber, D.B.; Wanpen, S.; Leelayuwat, N.; Chatchawan, U. Effects of handicraft sitting postures on lower trunk muscle fatigue. Ergonomics 2012, 55, 693–703. [Google Scholar] [CrossRef]
- Lewis, S.E.; Fowler, N.E. Changes in intervertebral disk dimensions after a loading task and the relationship with stature change measurements. Arch. Phys. Med. Rehabil. 2009, 90, 1795–1799. [Google Scholar] [CrossRef]
- Kanlayanaphotporn, R.; Trott, P.; Williams, M.; Fulton, I. Effects of chronic low back pain, age and gender on vertical spinal creep. Ergonomics 2003, 46, 561–573. [Google Scholar] [CrossRef]
- Watanabe, S.; Kobara, K.; Yoshimura, Y.; Osaka, H.; Ishida, H. Influence of trunk muscle co-contraction on spinal curvature during sitting. J. Back Musculoskelet Rehabil. 2014, 27, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fryer, J.C.J.; Quon, J.A.; Smith, F.W. Magnetic resonance imaging and stadiometric assessment of the lumbar discs after sitting and chair-care decompression exercise: A pilot study. Spine J. 2010, 10, 297–305. [Google Scholar] [CrossRef]
- Saiklang, P.; Puntumetakul, R.; Swangnetr, M.; Boucaut, R. The immediate effect of the abdominal drawing-in maneuver technique on stature change in seated sedentary workers with chronic low back pain. Ergonomics 2020, 64, 55–68. [Google Scholar] [CrossRef]
- Holmes, M.W.R.; De Carvalho, D.E.; Karakolis, T.; Callaghan, J.P. Evaluating abdominal and lower back muscle activity while performing core exercises on a stability ball and a dynamic office chair. Hum. Factors 2015, 57, 1149–1161. [Google Scholar] [CrossRef] [PubMed]
- Gregory, D.E.; Dunk, M.N.; Callaghan, J.P. Stability ball versus office chair: Comparisonof muscle activation and lumbar spine posture during prolonged sitting. Hum. Factors 2006, 48, 142–153. [Google Scholar] [CrossRef] [Green Version]
- Panjabi, M.M. Clinical spinal instability and low back pain. J. Electromyogr. Kinesiol. J. Electromyogr. Kines 2003, 13, 371–379. [Google Scholar] [CrossRef]
- Bergmark, A. Stability of the lumbar spine: A study in mechanical engineering. Acta Orthop. Scand Suppl. 1989, 230, 1–54. [Google Scholar] [CrossRef]
- Faries, M.D.; Greenwood, M. Core Training: Stabilizing the confusion. Strength Cond J. 2007, 29, 10–25. [Google Scholar] [CrossRef]
- Kavcic, N.; Grenier, S.; McGill, S.M. Determining the stabilizing role of individual torso muscles during rehabilitation exercises. Spine 2004, 29, 1254–1265. [Google Scholar] [CrossRef] [PubMed]
- Marshell, P.W.; Murphy, B.A. Delayed abdominal muscle onsets and self-report measures of pain and disability in chronic low back pain. J. Electromyogr. Kinesiol. 2010, 20, 833–839. [Google Scholar] [CrossRef]
- Silfies, S.P.; Mehta, R.; Smith, S.S.; Karduna, A.R. Differences in feedforward trunk muscle activity in subgroups of patients with mechanical low back pain. Arch. Phys. Med. Rehabil. 2009, 90, 1159–1169. [Google Scholar] [CrossRef]
- Tsao, H.; Druitt, T.R.; Schollum, T.M.; Hodges, P.W. Motor training of the lumbar paraspinal muscles induces immediate changes in motor coordination in patients with recurrent low back pain. J. Pain 2010, 11, 1120–1128. [Google Scholar] [CrossRef] [Green Version]
- Rodacki, C.L.; Fowler, N.E.; Rodacki, A.L.; Birch, K. Stature loss and recovery in pregnant women with and without low back pain. Arch. Phys. Med. Rehabil. 2003, 84, 507–512. [Google Scholar] [CrossRef]
- Singh, R.E.; Iqbal, K.; White, G.; Hutchinson, T.E. A Systematic Review on Muscle Synergies: From Building Blocks of Motor Behavior to a Neurorehabilitation Tool. Appl. Bionics. Biomech. 2018, 22, 3165368. [Google Scholar] [CrossRef] [Green Version]
- Healey, E.L.; Fowler, N.E.; Burden, A.M.; McEwan, I.M. The influence of different unloading positions upon stature recovery and paraspinal muscle activity. Clin. Biomech. Bristol. Avon. 2005, 20, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Puntumetakul, R.; Areeudomwong, P.; Emasithi, A.; Yamauchi, J. Effect of 10-week core stabilization exercise training and detraining on pain-related outcomes in patients with clinical lumbar instability. Patient Prefer. Adherence 2013, 7, 1189–1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puntumetakul, R.; Saiklang, P.; Tapanya, W.; Chatprem, T.; Kanpittaya, J.; Arayawichanon, P.; Boucaut, R. The effects of core stabilization exercise with the abdominal drawing-in maneuver technique versus general strengthening exercise on lumbar segmental motion in patients with clinical lumbar instability: A randomized controlled trial with 12-month follow-up. Int. J. Environ. Res. Public Health 2021, 18, 7811. [Google Scholar] [CrossRef] [PubMed]
- Areeudomwong, P.; Puntumetakul, R.; Jirarattanaphochai, K.; Wanpen, S.; Kanpittaya, J.; Chatchawan, U.; Yamauchi, J. Core stabilization exercise improves pain intensity, functional disability and trunk muscle activity of patients with clinical lumbar instability: A pilot randomized controlled study. J. Phys. Ther. Sci. 2012, 24, 1007–1012. [Google Scholar] [CrossRef] [Green Version]
- Boonstra, M.A.; Stewart, R.E.; Köke, A.J.A.; Oosterwijk, R.F.A.; Swaan, J.L.; Schreurs, K.M.G.; Schiphorst, H.R. Cut-off points for mild, moderate, and severe pain on the numeric rating scale for pain in patients with chronic musculoskeletal pain: Variability and influence of sex and catastrophizing. Front. Psychol. 2016, 7, 1466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, S.; Holmes, P.; Woby, S.; Hindle, J.; Fowler, N. Changes in muscle activity and stature recovery after active rehabilitation for chronic low back pain. Man. Ther. 2014, 19, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.A.; Maher, C.G.; Latimer, J.; Ferreira, M.L.; Costa, L.O.P. The patient-specific functional scale is more responsive than the roland morris disability questionnaire when activity limitation is low. Eur. Spine J. 2011, 20, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phimphasak, C.; Swangnetr, M.; Puntumetakul, R.; Chatchawan, U.; Boucaut, R. Effects of seated lumbar extension postures on spinal height and lumbar range of motion during prolonged sitting. Ergonomics 2016, 59, 112–120. [Google Scholar] [CrossRef]
- Rodacki, C.L.; Fowler, N.E.; Rodacki, A.L.; Birch, K. Technical note: Repeatability of measurement in determining stature in sitting and standing postures. Ergonomics 2001, 44, 1076–1085. [Google Scholar] [CrossRef]
- Imai, A.; Kaneoka, K.; Okubo, Y.; Shiina, I.; Tatsumura, M.; Izumi, S. Trunk muscle activity during lumbar stabilization exercises on both a stable and unstable surface. J. Orthop. Sports Phys. Ther. 2010, 40, 369–375. [Google Scholar] [CrossRef] [Green Version]
- Marshall, P.; Murphy, B. The validity and reliability of surface EMG to assess the neuromuscular response of the abdominal muscles to rapid limb movement. J. Electromyogr. Kinesiol. 2003, 13, 477–489. [Google Scholar] [CrossRef]
- Danneels, L.A.; Cagnie, B.J.; Cools, A.M.; Vanderstraeten, G.G.; Cambier, D.C.; Witvrouw, E.E. Intra-operator and inter-operator reliability of surface electromyography in the clinical evaluation of back muscles. Man. Ther. 2001, 6, 145–153. [Google Scholar] [CrossRef]
- Ostelo, R.W.J.G.; de Vet, J.C.W. Clinically important outcomes in low back pain. Best Res. Clin. Rheumatol. 2005, 19, 593–607. [Google Scholar] [CrossRef]
- Roland, M.; Fairbank, J. The roland-morris disability questionnaire and the oswestry disability questionnaire. Spine 2000, 25, 3115–3124. [Google Scholar] [CrossRef] [Green Version]
- Jirarattanaphochai, K.; Jung, S.; Sumananont, C.; Saengnipanthkul, S. Reliability of the Roland-Morris Disability Questionnaire (Thai version) for the evaluation of low back pain patients. J. Med. Assoc. Thai. 2005, 88, 407–411. [Google Scholar] [PubMed]
- Healey, E.L.; Burden, A.M.; McEwan, I.M.; Fowler, N.E. Stature loss and recovery following a period of loading: Effect of time of day and presence or absence of low back pain. Clin. Biomech. Bristol. Avon. 2008, 23, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Puntumetakul, R.; Trott, P.; Williams, M.; Fulton, I. Effect of time of day on the vertical spinal creep response. Appl. Ergon. 2009, 40, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Healey, E.L.; Burden, A.M.; McEwan, I.M.; Fowler, N.E. Diurnal variation in stature: Do those with chronic low back pain differ from asymptomatic controls? Clin. Biomech. 2011, 26, 331–336. [Google Scholar] [CrossRef]
- Fowler, N.E.; de Lourdes Rodacki, C.; Rodacki, A.L. Spinal shrinkage and recovery in women with and without low back pain. Arch. Phys. Med. Rehabil. 2005, 86, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Corlett, E.N.; Eklund, J.A.E.; Reilly, T.; Troup, J.D.G. Assessment of workload from measurements of stature. Appl. Ergon. 1987, 18, 65–71. [Google Scholar] [CrossRef]
- Koumantakis, G.A.; Watson, P.J.; Oldham, J.A. Trunk muscle stabilization training plus general exercise versus general exercise only: Randomized controlled trial of patients with recurrent low back pain. Phys. Ther. 2005, 85, 209–225. [Google Scholar] [CrossRef] [Green Version]
- Moseley, G.L.; Hodges, P.; Gandevia, S.C. Deep and superficial fibers of the lumbar multifidus muscle are differentially active during voluntary arm movements. Spine 2002, 27, 29–36. [Google Scholar] [CrossRef]
- Goldby, L.; Moore, A.; Trew, M. A randomized controlled trial investigating the efficiency of musculoskeletal physiotherapy on chronic low back disorder. Spine 2006, 31, 1083–1093. [Google Scholar] [CrossRef]
- Schmidt, H.; Reitmaier, S.; Graichen, F.; Shirazi-Adl, A. Review of the fluid flow within intervertebral discs-How could in vitro measurements replicate in vivo? J. Biomech. 2016, 49, 3133–3146. [Google Scholar] [CrossRef]
- Vergroesen, P.P.A.; Van Der Veen, A.J.; Emanuel, K.S.; Van Dieën, J.H.; Smitm, T.H. The poro-elastic behaviour of the intervertebral disc: A new perspective on diurnal fluid flow. J. Biomech. 2016, 49, 857–863. [Google Scholar] [CrossRef]
- Munster, M.M.; Brismée, J.M.; Sizer, P.S.; Browne, K.; Dewan, B.; Litke, A.; Pape, J.L.; Sobczak, S. Can 5 min of repetitive prone press-ups and sustained prone press-ups following a period of spinal loading reverse spinal shrinkage? Physiother Theory Pract. 2018, 35, 1–9. [Google Scholar] [CrossRef]
- Pape, J.L.; Brismée, J.M.; Sizer, P.S.; Matthijs, O.C.; Browne, K.L.; Dewan, B.M.; Sobczak, S. Increased spinal height using propped slouched sitting postures: Innovative ways to rehydrate intervertebral discs. Appl. Ergon. 2018, 66, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Billy, G.G.; Lemieux, S.K.; Chow, M.X. Changes in lumbar disk morphology associated with prolonged sitting assessed by magnetic resonance imaging. PM&R 2014, 6, 790–795. [Google Scholar] [CrossRef]
- Fryer, J.; Zhang, W. Preliminary investigation into a seated unloading movement strategy for the lumbar spine: A pilot study. J. Bodyw. Mov. Ther. 2010, 14, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Søndergaard, K.H.; Olesen, C.G.; Sondergaard, E.K.; de Zee, M.; Madeleine, P. The variability and complexity of sitting postural control are associated with discomfort. J. Biomech. 2010, 43, 1997–2001. [Google Scholar] [CrossRef] [PubMed]
- Saiklang, P.; Puntumetakul, R.; Siritaratiwat, W.; Boucaut, R. Effect of Time of Day on the Magnitude of Stature Change Response Variability in Participants With Chronic Low Back Pain on Consecutive 2 Days. Trends Sci. 2021, 18, 678. [Google Scholar] [CrossRef]
- MacDonald, D.A.; Moseley, G.L.; Hodges, P.W. The lumbar multifidus: Does the evidence support clinical beliefs? Man. Ther. 2006, 11, 254–263. [Google Scholar] [CrossRef]
- Tayashiki, K.; Takai, Y.; Maeo, S.; Kanehisa, H. Intra-abdominal pressure and trunk muscular activities during abdominal bracing and hollowing. Int. J. Sports Med. 2015, 37, 134–143. [Google Scholar] [CrossRef]
- Stokes, I.A.F.; Gardner-Morse, M.G.; Henry, S.M. Intra-abdominal pressure and abdominal wall muscular function: Spinal unloading mechanism. Clin. Biomech. 2010, 25, 859–866. [Google Scholar] [CrossRef] [Green Version]
- Rodacki, C.L.; Rodacki, A.; Ugrinowitsch, C.; Zielinski, D.; Costa, R.B. Spinal unloading after abdominal exercises. Clin. Biomech. 2008, 23, 8–14. [Google Scholar] [CrossRef] [PubMed]





| Characteristics | Male (n = 15) | Female (n = 15) | Total (n = 30) |
|---|---|---|---|
| Age (years), mean ± SD | 25.67 ± 3.35 | 26.07 ± 3.37 | 25.87 ± 3.31 |
| Weight (kg), mean ± SD | 63.93 ± 7.94 | 52.80 ± 4.84 | 58.37 ± 8.59 |
| BMI (kg m−2), mean ± SD | 22.11 ± 1.90 | 20.95 ± 1.28 | 21.53 ± 1.70 |
| Sitting height (cm), mean ± SD | 87.93 ± 5.38 | 84.50 ± 3.39 | 86.22 ± 4.75 |
| Standing height (cm), mean ± SD | 169.80 ± 5.16 | 158.67 ± 4.70 | 164.23 ± 7.45 |
| Smoking status | no | no | no |
| Occupation, n (%) | |||
| -Student | 12 (80) | 13 (86.67) | 25 (83.33) |
| -Office worker | 3 (20) | 2 (13.33) | 5 (16.67) |
| Working time (hours/day), mean ± SD | 8.60 ± 2.95 | 7.60 ± 2.13 | 8.10 ± 2.58 |
| Period of LBP (month), mean ± SD | 10.73 ± 6.18 | 10.53 ± 4.60 | 10.63 ± 5.35 |
| Disability index score, mean ± SD | 4.20 ± 1.82 | 4.80 ± 1.82 | 4.50 ± 1.81 |
| Pain scale 24 h (score), mean ± SD | 4.27 ± 1.33 | 4.47 ± 1.36 | 4.37 ± 1.33 |
| Note: SD = Standard deviation; BMI = Body mass index. | |||
| Tsit (mm) Mean ± SD (95%CI) | Mean Change from Tsit (mm) Mean ± SD (95%CI) | |||
|---|---|---|---|---|
| T1 | T2 | T3 | ||
| Baseline | −4.266 ± 2.221 (−5.095 to −3.437) | −3.999 ± 1.482 (−4.553 to −3.446) g*h** | −5.782 ± 1.605 (−6.382 to −5.183) f*h* | −7.365 ± 2.180 (−8.179 to −6.552) f**g* |
| After 5 weeks of CSE with ADIM technique | −3.864 ± 1.986 (−4.605 to −3.122) | −2.538 ± 1.004 (−2.913 to −2.163) g*h** | −4.027 ± 1.306 (−4.515 to −3.539) f**h* | −5.367 ± 1.258 (−5.837 to −4.897) f**g* |
| p-value Between | 0.458 | 0.001 | 0.001 | 0.001 |
| Conditions | Times | p-Value within Conditions | |||
|---|---|---|---|---|---|
| Tsit | (T1) | (T2) | (T3) | ||
| Baseline | 3.00 (2.00–5.00) f*g**h** | 3.00 (3.00–5.00) e*g*h* | 3.50 (3.00–6.00) e**f* | 3.50 (3.00–6.00) e**f* | 0.001 |
| After 5 weeks of CSE with ADIM technique | 1.00 (0.00–2.00) g*h** | 1.00 (0.00–2.25) g*h* | 1.50 (0.00–3.00) e*h* | 2.00 (0.00–3.00) e**f*g* | 0.001 |
| p-value Between | 0.632 | 0.001 | 0.001 | 0.001 | |
| Muscle Fatigue (Hz.) | Right | p-value | Left | p-Value | ||
|---|---|---|---|---|---|---|
| Baseline Median (Interquartile Range) | After 5 Weeks of CSE Median (Interquartile Range) | Baseline Median (Interquartile Range) | After 5 Weeks of CSE Median (Interquartile Range) | |||
| RA (0–10th min) (15th–25th min) (28th–38th min) | 25.71 (24.99–27.25) 25.70 (917.29–27.64) 25.72 (25.70–28.69) | 25.70 (25.69–25.71) 25.70 (23.91–25.71) 25.71 (25.69–25.72) | 0.713 0.992 0.144 | 25.71 (15.72–28.95) 25.71 (16.95–27.34) 25.71 (25.69–28.70) | 25.70 (25.12–25.71) 25.71 (25.69–25.72) 25.70 (24.72–25.71) | 0.128 0.926 0.130 |
| p-value | 0.177 | 0.441 | 0.852 | 0.084 | ||
| TrA & IO (0–10th min) (15th–25th min) (28th–38th min) | 42.59 (34.58–42.72) b*c* 35.99 (35.69–37.99) a* 35.71 (33.21–36.45) a* | 46.71 (46.63–48.32) 45.30 (40.80–47.96) 45.70 (41.99–48.71) | 0.001 ** 0.001 ** 0.001 ** | 42.70 (35.37–42.73) b*c* 36.15 (34.19–37.32) a* 35.95 (33.53–37.21) a* | 46.71 (44.88–48.69) 45.45 (41.49–47.23) 45.99 (43.45–48.65) | 0.001 ** 0.001 ** 0.001 ** |
| p-value | 0.001 | 0.058 | 0.001 * | 0.503 | ||
| ICLT (0–10th min) (15th–25th min) (28th–38th min) | 35.70 (33.21–36.03) 35.69 (33.28–35.72) 35.70 (33.85–35.71) | 36.14 (35.69–37.94) 35.72 (35.30–37.33) 36.70 (33.85–35.71) | 0.060 0.206 0.153 | 35.70 (34.81–35.72) 35.69 (33.66–36.21) 35.69 (33.58–35.71) | 35.71 (34.39–37.76) 35.71 (35.66–36.47) 35.71 (35.69–37.05) | 0.524 0.289 0.360 |
| p-value | 0.873 | 0.644 | 0.721 | 0.594 | ||
| LM (0–10th min) (15th–25th min) (28th–38th min) | 49.04 (46.42–52.79) 49.41 (46.96–53.57) 49.21 (47.71–55.69) | 52.65 (47.71–53.57) 52.74 (48.71–53.57) 52.34 (48.72–55.72) | 0.185 0.098 0.082 | 49.36 (45.71–52.38) 49.21 (47.71–55.70) 49.84 (48.00–55.69) | 51.90 (48.22–53.57) 52.33 (48.15–55.40) 52.42 (48.68–55.71) | 0.175 0.544 0.237 |
| p-value | 0.695 | 0.341 | 0.273 | 0.125 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saiklang, P.; Puntumetakul, R.; Chatprem, T. The Effect of Core Stabilization Exercise with the Abdominal Drawing-in Maneuver Technique on Stature Change during Prolonged Sitting in Sedentary Workers with Chronic Low Back Pain. Int. J. Environ. Res. Public Health 2022, 19, 1904. https://doi.org/10.3390/ijerph19031904
Saiklang P, Puntumetakul R, Chatprem T. The Effect of Core Stabilization Exercise with the Abdominal Drawing-in Maneuver Technique on Stature Change during Prolonged Sitting in Sedentary Workers with Chronic Low Back Pain. International Journal of Environmental Research and Public Health. 2022; 19(3):1904. https://doi.org/10.3390/ijerph19031904
Chicago/Turabian StyleSaiklang, Pongsatorn, Rungthip Puntumetakul, and Thiwaphon Chatprem. 2022. "The Effect of Core Stabilization Exercise with the Abdominal Drawing-in Maneuver Technique on Stature Change during Prolonged Sitting in Sedentary Workers with Chronic Low Back Pain" International Journal of Environmental Research and Public Health 19, no. 3: 1904. https://doi.org/10.3390/ijerph19031904