
The Impact of Vitamin D Status on COVID-19 Severity among Hospitalized Patients in the Western Region of Saudi Arabia: A Retrospective Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
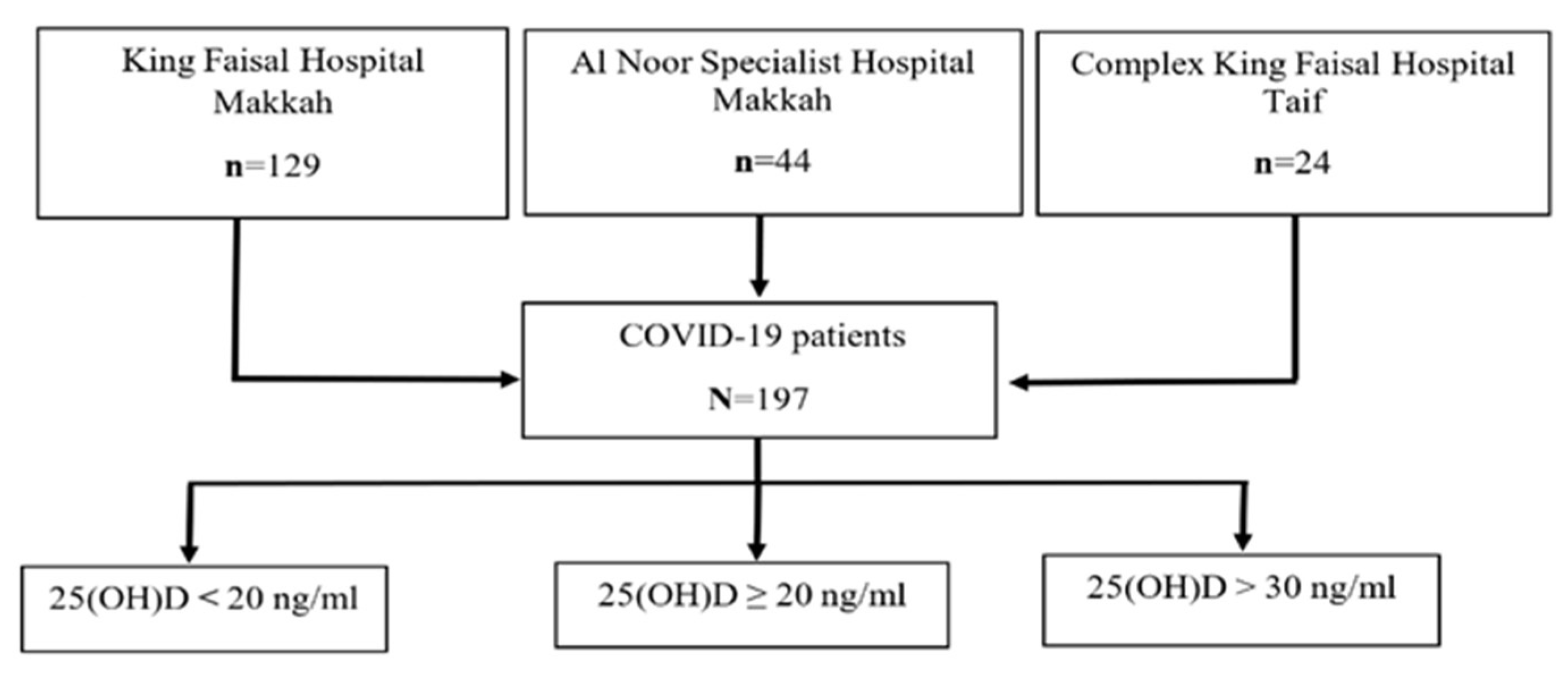
2.1. Study Design and Population
2.2. Data Collection
2.3. Laboratory Measurements
2.4. Statistical Analysis
3. Results
3.1. Clinical Features of COVID-19 Patients
3.2. The Association between Vitamin D Levels and the Severity of COVID-19
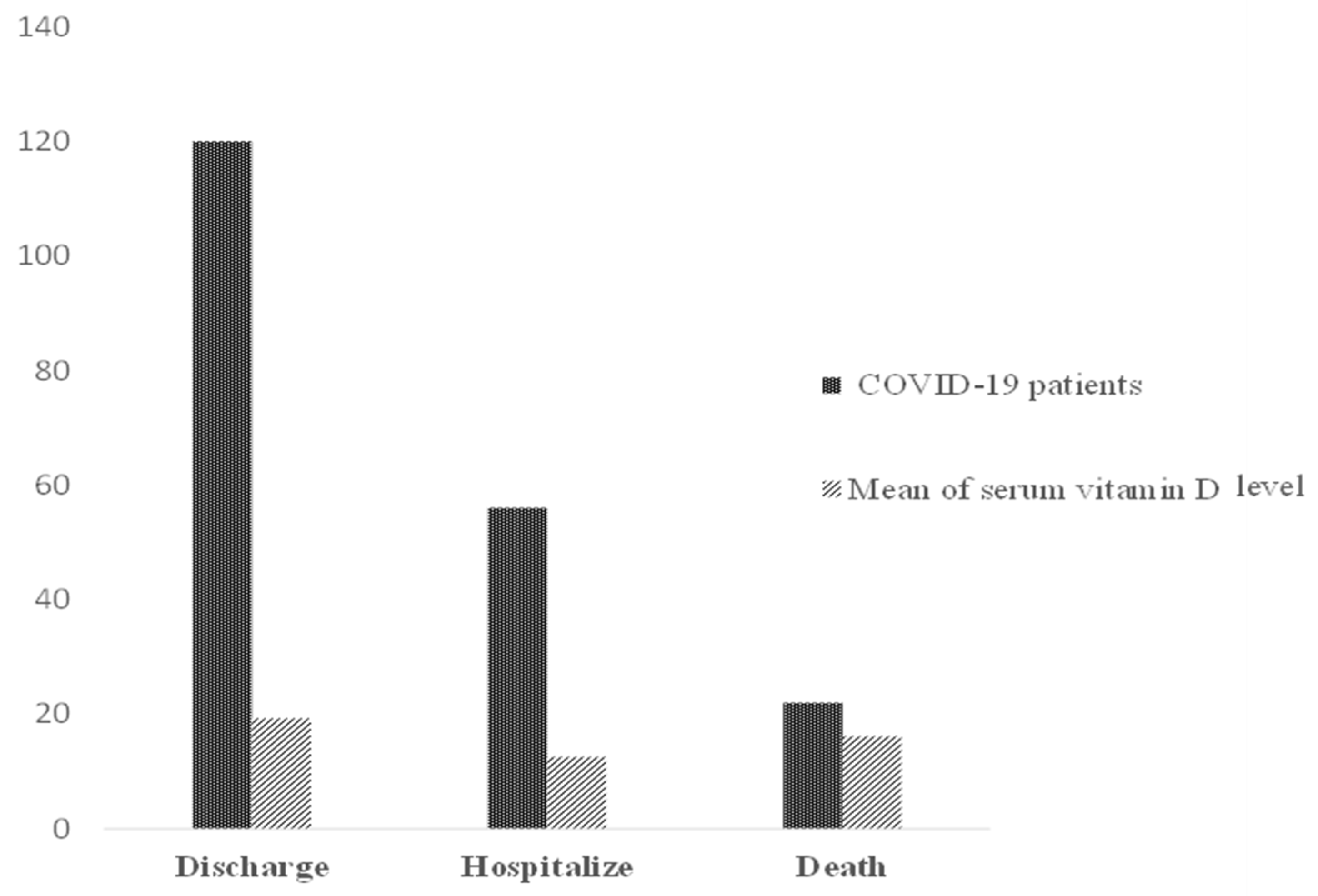
3.3. Clinical Outcome of COVID-19 Patients
4. Discussion
Strength and Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Wang, Y.; Ye, D.; Liu, Q. Review of the 2019 novel coronavirus (SARS-CoV-2) based on current evidence. Int. J. Antimicrob. Agents 2020, 55, 105948. [Google Scholar] [CrossRef] [PubMed]
- WHO. Naming the Coronavirus Disease (COVID-19) and the Virus Tthat Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(COVID-2019)-and-the-virus-that-causes-it (accessed on 7 November 2020).
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 7 November 2020).
- Yang, Y.; Peng, F.; Wang, R.; Guan, K.; Jiang, T.; Xu, G.; Sun, J.; Chang, C. The deadly coronaviruses: The 2003 SARS pandemic and the 2020 novel coronavirus epidemic in China. J. Autoimmun. 2020, 109, 102434. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus—Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Francis, A.I.; Ghany, S.; Gilkes, T.; Umakanthan, S. Review of COVID-19 vaccine subtypes, efficacy and geographical distributions. Postgrad. Med. J. 2021, 97, 1–6. [Google Scholar] [CrossRef]
- Honardoost, M.; Ghavideldarestani, M.; Khamseh, M.E. Role of vitamin D in pathogenesis and severity of COVID-19 infection. Arch. Physiol. Biochem. 2020, 126, 1–7. [Google Scholar] [CrossRef]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [Green Version]
- Zdrenghea, M.T.; Makrinioti, H.; Bagacean, C.; Bush, A.; Johnston, S.; Stanciu, L.A. Vitamin D modulation of innate immune responses to respiratory viral infections. Rev. Med. Virol. 2016, 27, e1909. [Google Scholar] [CrossRef]
- Gombart, A.F.; Pierre, A.; Maggini, S. A Review of Micronutrients and the Immune System–Working in Harmony to Reduce the Risk of Infection. Nutrients 2020, 12, 236. [Google Scholar] [CrossRef] [Green Version]
- Lemire, J.M.; Adams, J.S.; Kermani-Arab, V.; Bakke, A.C.; Sakai, R.; Jordan, S.C. 1,25-Dihydroxyvitamin D3 suppresses human T helper/inducer lymphocyte activity in vitro. J. Immunol. 1985, 134, 3032–3035. [Google Scholar] [PubMed]
- Boonstra, A.; Barrat, F.J.; Crain, C.; Heath, V.L.; Savelkoul, H.F.J.; O’Garra, A. 1α,25-Dihydroxyvitamin D3 Has a Direct Effect on Naive CD4+ T Cells to Enhance the Development of Th2 Cells. J. Immunol. 2001, 167, 4974–4980. [Google Scholar] [CrossRef] [Green Version]
- Cui, C.; Xu, P.; Li, G.; Qiao, Y.; Han, W.; Geng, C.; Liao, D.; Yang, M.; Chen, D.; Jiang, P. Vitamin D receptor activation regulates microglia polarization and oxidative stress in spontaneously hypertensive rats and angiotensin II-exposed microglial cells: Role of renin-angiotensin system. Redox Biol. 2019, 26, 101295. [Google Scholar] [CrossRef]
- Rhodes, J.M.; Subramanian, S.; Laird, E.; Griffin, G.; Kenny, R.A. Perspective: Vitamin D deficiency and COVID-19 severity—Plausibly linked by latitude, ethnicity, impacts on cytokines, ACE2 and thrombosis. J. Intern. Med. 2021, 289, 97–115. [Google Scholar] [CrossRef]
- Ilie, P.C.; Stefanescu, S.; Smith, L. The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality. Aging Clin. Exp. Res. 2020, 32, 1195–1198. [Google Scholar] [CrossRef]
- Merzon, E.; Tworowski, D.; Gorohovski, A.; Vinker, S.; Cohen, A.G.; Green, I.; Frenkel-Morgenstern, M. Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: An Israeli population-based study. FEBS J. 2020, 287, 3693–3702. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Di Lecce, V.; Quaranta, V.N.; Zito, A.; Buonamico, E.; Capozza, E.; Palumbo, A.; Di Gioia, G.; Valerio, V.N.; Resta, O. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J. Endocrinol. Investig. 2021, 44, 765–771. [Google Scholar] [CrossRef]
- Panagiotou, G.; Tee, S.A.; Ihsan, Y.; Athar, W.; Marchitelli, G.; Kelly, D.; Boot, C.S.; Stock, N.; Macfarlane, J.; Martineau, A.R.; et al. Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalised with COVID-19 are associated with greater disease severity: Results of a local audit of practice. Clin. Endocrinol. 2020, 93, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Alguwaihes, A.M.; Sabico, S.; Hasanato, R.; Al-Sofiani, M.E.; Megdad, M.; Albader, S.S.; Alsari, M.H.; Alelayan, A.; Alyusuf, E.Y.; Alzahrani, S.H.; et al. Severe vitamin D deficiency is not related to SARS-CoV-2 infection but may increase mortality risk in hospitalized adults: A retrospective case–control study in an Arab Gulf country. Aging Clin. Exp. Res. 2021, 33, 1415–1422. [Google Scholar] [CrossRef] [PubMed]
- Al-Daghri, N.M. Vitamin D in Saudi Arabia: Prevalence, distribution and disease associations. J. Steroid Biochem. Mol. Biol. 2018, 175, 102–107. [Google Scholar] [CrossRef]
- Ong, L.; Saw, S.; Sahabdeen, N.B.; Tey, K.T.; Ho, C.S.; Sethi, S.K. Current 25-hydroxyvitamin D assays: Do they pass the test? Clin. Chim. Acta 2012, 413, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Al-Daghri, N.M.; Al-Saleh, Y.; Aljohani, N.; Sulimani, R.; Al-Othman, A.M.; Alfawaz, H.; Fouda, M.; Al-Amri, F.; Shahrani, A.; Alharbi, M.; et al. Vitamin D status correction in Saudi Arabia: An experts’ consensus under the auspices of the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis, and Musculoskeletal Diseases (ESCEO). Arch. Osteoporos. 2017, 12, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alguwaihes, A.M.; Al-Sofiani, M.E.; Megdad, M.; Albader, S.S.; Alsari, M.H.; Alelayan, A.; Alzahrani, S.H.; Sabico, S.; Al-Daghri, N.M.; Jammah, A.A. Diabetes and Covid-19 among hospitalized patients in Saudi Arabia: A single-centre retrospective study. Cardiovasc. Diabetol. 2020, 19, 205. [Google Scholar] [CrossRef]
- Kostoglou-Athanassiou, I.; Athanassiou, P.; Chronaiou, A.; Michou, A.; Dadiras, N.; Terzi, T.; Loi, V.; Karfi, A. Vitamin D deficiency and comorbid conditions. Bone 2010, 47, S240. [Google Scholar] [CrossRef]
- Al Zarooni, A.A.R.; Al Marzouqi, F.I.; Al Darmaki, S.H.; Prinsloo, E.A.M.; Nagelkerke, N. Prevalence of vitamin D deficiency and associated comorbidities among Abu Dhabi Emirates population. BMC Res. Notes 2019, 12, 503. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef] [PubMed]
- Szeto, B.; Zucker, J.E.; LaSota, E.D.; Rubin, M.R.; Walker, M.D.; Yin, M.T.; Cohen, A. Vitamin D Status and COVID-19 Clinical Outcomes in Hospitalized Patients. Endocr. Res. 2021, 46, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Hernández, J.L.; Nan, D.; Fernandez-Ayala, M.; García-Unzueta, M.; Hernández-Hernández, M.A.; López-Hoyos, M.; Muñoz-Cacho, P.; Olmos, J.M.; Gutiérrez-Cuadra, M.; Ruiz-Cubillán, J.J.; et al. Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection. J. Clin. Endocrinol. Metab. 2021, 106, e1343–e1353. [Google Scholar] [CrossRef] [PubMed]
- Pos, V. Deficieincy in 25-Hydroxyvitamin D and 30-Day Mortality In Patients with Severe Sepsis and Septic Shock. Am. J. Crit. Care 1978, 23, 1–6. [Google Scholar]
- Anwar, E.; Hamdy, G.; Taher, E.; Fawzy, E.; Abdulattif, S.; Attia, M.H. Burden and Outcome of Vitamin D Deficiency Among Critically Ill Patients: A Prospective Study. Nutr. Clin. Pract. 2017, 32, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Radujkovic, A.; Hippchen, T.; Tiwari-Heckler, S.; Dreher, S.; Boxberger, M.; Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020, 12, 2757. [Google Scholar] [CrossRef] [PubMed]
- Orchard, L.; Baldry, M.; Nasim-Mohi, M.; Monck, C.; Saeed, K.; Grocott, M.P.W.; Ahilanandan, D. Vitamin-D levels and intensive care unit outcomes of a cohort of critically ill COVID-19 patients. Clin. Chem. Lab. Med. 2021, 59, 1155–1163. [Google Scholar] [CrossRef]
- Demir, M.; Demir, F.; Aygun, H. Vitamin D deficiency is associated with COVID-19 positivity and severity of the disease. J. Med. Virol. 2021, 93, 2992–2999. [Google Scholar] [CrossRef]
- Castillo, M.E.; Manuel, L.; Costa, E.; Bouillon, R.; Francisco, J. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 2–7. [Google Scholar]
- Annweiler, G.; Corvaisier, M.; Gautier, J.; Dubée, V.; Legrand, E.; Sacco, G.; Annweiler, C. Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERIA-COVID Quasi-Experimental Study. Nutrients 2020, 12, 3377. [Google Scholar] [CrossRef]
- Maruotti, N.; Cantatore, F.P. Vitamin D and the Immune System. J. Rheumatol. 2010, 37, 491–495. [Google Scholar] [CrossRef]
- Prietl, B.; Treiber, G.; Pieber, T.R.; Amrein, K. Vitamin D and Immune Function. Nutrients 2013, 5, 2502–2521. [Google Scholar] [CrossRef]
- Madden, K.; Feldman, H.A.; Chun, R.F.; Smith, E.M.; Sullivan, R.M.; Agan, A.A.; Randolph, A.G. Critically ill children have low vitamin D–binding protein, influencing bioavailability of vitamin D. Ann. Am. Thorac. Soc. 2015, 12, 1654–1661. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristic | N (%) |
|---|---|
| Hospital Admission King Faisal Hospital in Makkah Al-Noor Specialist Hospital in Makkah Complex King Faisal Hospital in Taif | 129 (65.48%) 44 (22.34%) 24 (12.18%) |
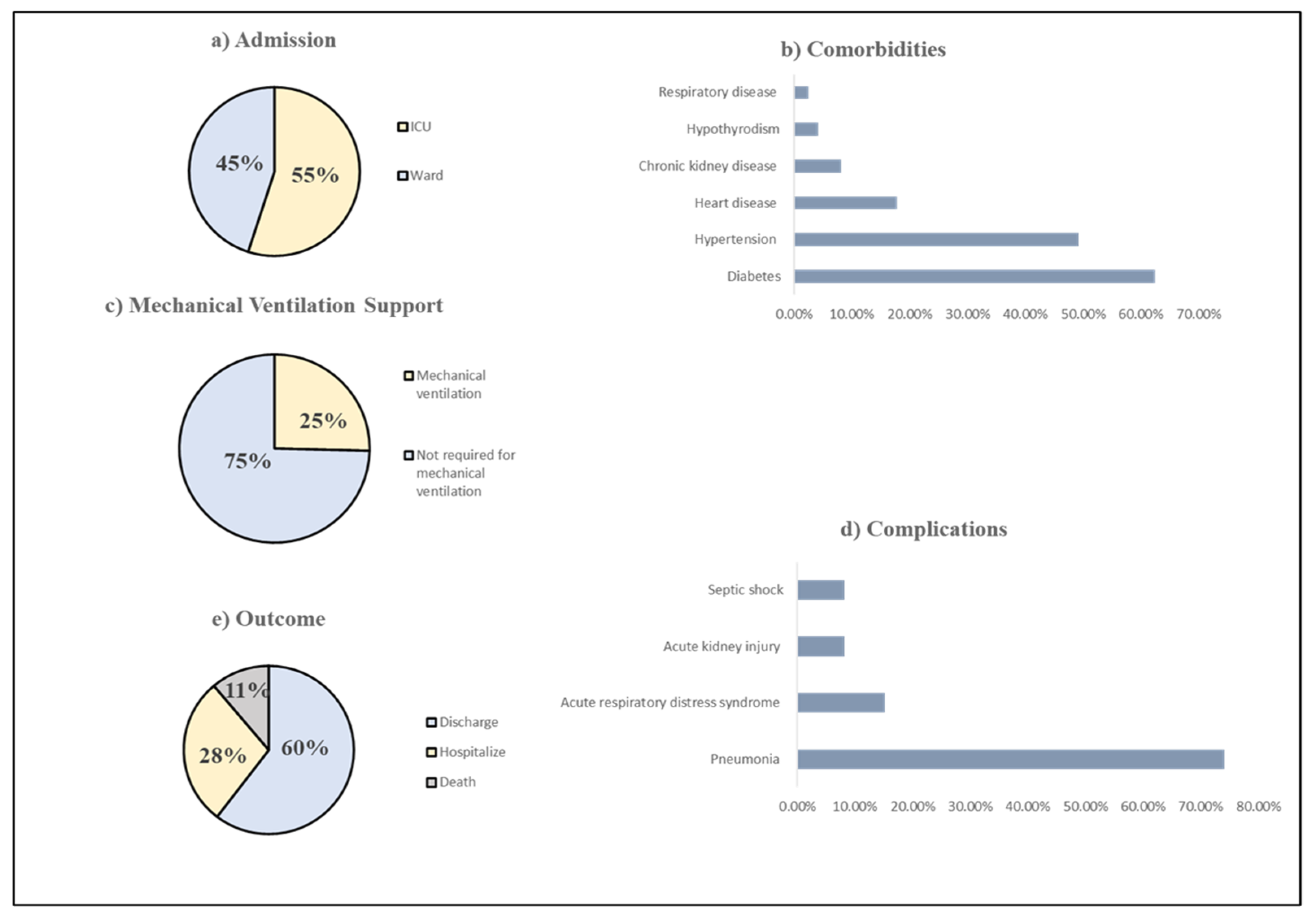
| Ward Admission General Ward ICU | 109 (55%) 88 (45%) |
| Nationality Saudi Non-Saudi | 94 (47.72%) 103 (52.28%) |
| Gender Male Female | 133 (67.51%) 64 (32.49%) |
| Age Minimum Maximum | 57. 26 ± 15.74 a 20 97 |
| Comorbidities | N (%) |
|---|---|
| Diabetes | 123 (62.44%) |
| Hypertension | 97 (49.24%) |
| Cardiovascular disease | 35 (17.77%) |
| Chronic kidney disease | 16 (8.12%) |
| Hypothyroidism | 8 (4.10%) |
| Respiratory disease | 5(2.53%) |
| Parameters | Mean ± SD | Normal Range |
|---|---|---|
| 25(OH)D | 17.04 ± 11.18 | 30–70 ng/mL |
| CRP | 17.15 ± 24.60 | 0–6 mg/L |
| Clinical Outcome | Serum Vitamin D (ng/mL) | ||||
|---|---|---|---|---|---|
| Deficiency (<20 ng/mL) N = 144 (73.10%) | Sufficient (≥20 ng/mL) N = 31 (15.74%) | Adequacy (>30 ng/mL) N = 22 (11.17%) | |||
| Ward Admission | N (%) | p-Value | |||
| General Ward | 79 | 16 | 14 | 109 (55.33%) | 0.67 |
| ICU | 65 | 15 | 8 | 88 (44.67%) | |
| Complications | |||||
| Pneumonia | 104 | 24 | 18 | 146 (74.11%) | 0.96 |
| Acute respiratory distress syndrome | 21 | 5 | 4 | 30 (15.23%) | 0.85 |
| Acute kidney injury | 11 | 3 | 2 | 16 (8.12%) | 0.76 |
| Septic shock | 12 | 2 | 2 | 16 (8.12%) | 1.00 |
| Mechanical Ventilation | |||||
| Mechanical ventilation support | 40 | 7 | 3 | 50 (25%) | 0.34 |
| No mechanical ventilation support | 104 | 24 | 19 | 147(75%) | |
| Oxygen Support | |||||
| No oxygen support | 30 | 5 | 3 | 38 (19.29%) | 0.49 |
| 1–5 L/min | 37 | 7 | 9 | 53 (26.90%) | |
| 6–10 L/min | 13 | 4 | 3 | 20(10.15%) | |
| 11–15 L/min | 19 | 7 | 4 | 30 (15.23%) | |
| >15 L/min or on MV | 45 | 8 | 3 | 56 (28. 43%) | |
| Clinical Outcome | N (%) | Mean ± SD | R | p-Value * |
| Length of hospital stay | 197 (100%) | 8.65 ± 0.52 | 0.06 | 0.41 |
| CRP | 127 (64.5%) | 17.14 ± 2.18 | −0.15 | 0.11 |
| Clinical Outcome | N (%) | Serum Vitamin D (ng/mL) Mean ± SD | F | p-Value * |
| Discharge | 119 (60%) | 18.98 ± 1.12 | 3.81 | 0.02 |
| Hospitalize (transfer) | 56 (28%) | 13.23 ± 0.97 | ||
| Deceased | 22 (11%) | 16.20 ± 2.41 |
| Multiple Logistic Regression | ||||||
|---|---|---|---|---|---|---|
| Clinical Outcome | ICU Admission | Mechanical Ventilation Support | Mortality | |||
| Covariances | 95% CI | p-Value | 95% CI | p-Value | 95% CI | p-Value * |
| Age | (0.97–1.00) | 0.25 | (0.96–1.00) | 0.16 | (0.92–0.98) | 0.002 |
| Gender | (0.96–3.46) | 0.07 | (0.62–2.75) | 0.49 | (0.31–2.45) | 0.79 |
| Diabetes | (0.71–2.54) | 0.37 | (1.16–5.67) | 0.02 | (1.05–15.76) | 0.04 |
| Hypertension | (0.37–1.39) | 0.32 | (0.36–1.61) | 0.48 | (0.16–1.36) | 0.16 |
| CKD | (0.49–4.08) | 0.53 | (0.37–3.84) | 0.77 | (0.63–1.00) | 0.18 |
| Adjusted a OR vit. D | 1.25 | 3.12 | 2.39 | |||
| p–value * | 0.70 | 0.12 | 0.40 | |||
| 95% CI | (0.41–3.88) | (0.74–13.21) | (0.31–18.11) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bushnaq, T.; Algethami, F.; Qadhi, A.; Mustafa, R.; Ghafouri, K.; Azhar, W.; Malki, A.A. The Impact of Vitamin D Status on COVID-19 Severity among Hospitalized Patients in the Western Region of Saudi Arabia: A Retrospective Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1901. https://doi.org/10.3390/ijerph19031901
Bushnaq T, Algethami F, Qadhi A, Mustafa R, Ghafouri K, Azhar W, Malki AA. The Impact of Vitamin D Status on COVID-19 Severity among Hospitalized Patients in the Western Region of Saudi Arabia: A Retrospective Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1901. https://doi.org/10.3390/ijerph19031901
Chicago/Turabian StyleBushnaq, Taqwa, Fadiyah Algethami, Alaa Qadhi, Reham Mustafa, Khloud Ghafouri, Wedad Azhar, and Asma Al Malki. 2022. "The Impact of Vitamin D Status on COVID-19 Severity among Hospitalized Patients in the Western Region of Saudi Arabia: A Retrospective Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 3: 1901. https://doi.org/10.3390/ijerph19031901