1. Introduction
Cardiovascular diseases represent one of the most widespread categories of disease in the Western world, diseases that can compromise the health and physical strength, and consequently the working capacity, of those affected [
1].
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia in adults, with an estimated prevalence of between 2% to 4%. A 2.3-fold rise is expected in the coming decades, largely owing to the extended longevity of the general population and intensifying search for undiagnosed AF [
2]. AF patients have a five-fold increased risk of ischemic stroke or systemic embolism, and oral anticoagulation therapy should be considered when the CHA2DS2Vasc Score is ≥1 in men and ≥2 in women [
3,
4,
5,
6]. Moreover, AF is associated with substantial morbidity and mortality, thus portending a significant burden on patients, societal health, and health economy [
7].
Atrial fibrillation can cause significant and permanent damage to health, resulting in the loss of working capacity, thus preventing those affected from continuing to be productive members of society [
8].
Economic aid is established by law in order to provide financial support to those with a reduced or permanent loss of working capacity. Article 38 of the Constitution of the Republic of Italy states: “Every citizen unable to work and without the necessary means of subsistence is entitled to welfare support. Workers have the right to be assured adequate means for their needs and necessities in the case of accidents, illness, disability, old age and involuntary unemployment.
Disabled and handicapped persons are entitled to receive education and vocational training. Responsibilities under this article are entrusted to entities and institutions established by or supported by the State.
Private-sector assistance may be freely provided”.
To achieve said objectives, the National Institute for Social Security (INPS) was set up as the main social security agency of the Italian public pension plan. All public and private employees, along with the majority of self-employed workers who do not have their own social security fund, are required to register with INPS. These institutions receive social security contributions from employees through the companies by whom they are employed or from self-employed workers directly, calculated on the basis of income. INPS is regulated by the Ministry of Labor and Social Policies of the Republic of Italy and is responsible for assessing the conditions of those affected by disease and providing economic aid where appropriate.
All workers registered with INPS, in the event of an accident or chronic disease, have the right to avail themselves of one of the social security benefits provided by the law: the Invalidity Allowance (IA) or Invalidity Pension (IP). The qualifications for receiving such benefits are laid down by law.
In order to qualify for an invalidity allowance, the person must prove his or her invalid or unfit for work status is due to one or more infirmities or physical/mental defects, resulting in a working capacity reduced to less than one-third. IA is granted for a period of three years and can be confirmed for periods of the same duration. After three consecutive grants, the allowance is confirmed automatically. Those who receive such benefits may continue working, if able, at a reduced capacity.
To qualify for an invalidity pension, however, absolute and permanent working incapacity, that is, 100% invalidity, must be proved, caused by particularly severe conditions, such as advanced stage diseases, which result in serious and irreversible health conditions. In this case, the beneficiary ceases all working activity. Once granted, the invalidity pension is valid for life, subject to revision.
For both social security benefits, the applicant must satisfy certain administrative requirements: five years of INPS contributions, three of which must be within the five years preceding the date of application.
Clearly, a significant percentage of public finances at the Italian government’s disposal is used by INPS to provide such economic aid and must be subject to constant monitoring. If connected to diseases, the institute’s data may serve as an important source of information on public health and the nation’s future demographic, in addition to facilitating specific epidemiological, medico-legal, and occupational medicine assessments.
The objective of this study, which is a product of collaboration between teams of research, occupational health professionals, medico-legal experts, healthcare economists, and statisticians, is to analyze trends in applications and awards for the aforementioned benefits as a result of the onset of atrial fibrillation in accord with the various classifications of professions and to evaluate the economic impact of said economic aid on the social security system. This collection is completely unpublished on the international advertising panorama also due to the fact that the Italian legislation supports a particularly broad protection for workers. For this reason, more studies like this on different diseases are needed in order to understand their social, occupational, and economic impact on the system. These studies may be useful in order to better plan the use of economic and welfare resources, especially in the post-pandemic era.
3. Results
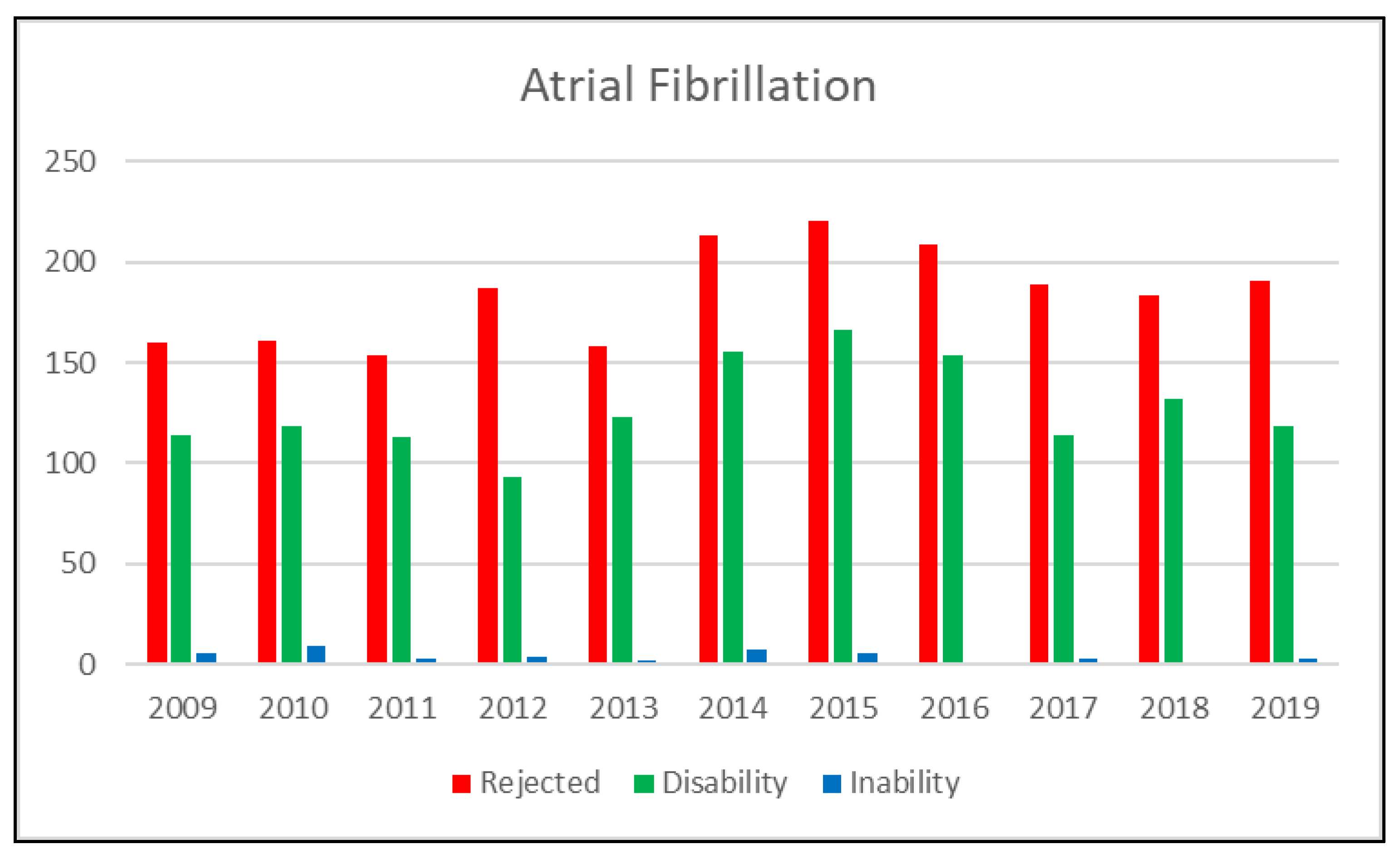
Over the period in question, a total of 3468 applications for assistance were filed throughout Italy containing a diagnosis of atrial fibrillation (
Table 1). A total of 58% of applications were rejected due to lack of the health requirements, 41% qualified for IA, and only 1.1% qualified for IP.
An average of 315 applications are filed every year, of which 184 are rejected, 127 qualify for IA, and four qualify for IP. Over the period in question, there has been an almost constant increase in the number of applications filed for this type of disease (
Figure 1).
3.1. Analysis by Classification of Profession
As a result of the job descriptions contained in the reports, it was possible to conduct an analysis of distribution by classification of profession, selecting all applications granted during the period in question.
Table 2 shows the percentage distribution by classification of profession calculated on the basis of the number of applications for atrial fibrillation granted during the 10-year period. The classification of said work-related duties follows the Italian National Institute of Statistics (Istat) rules for the Classification of Professions, 2001 edition (Cp2001), which identifies eight macro groups of professionals:
I—Legislators, top management, and entrepreneurs. This group includes professions that require experience and specific decisional and organizational abilities. Duties comprise devising government policies, laws, and regulations on a local and national level; supervising implementation thereof; representing the State; directing, managing, and defining objectives; and providing direction for the activities performed by businesses and complex organizations and management structures.
II—Intellectual, scientific, and highly specialized professions. These include all professions that require a considerable level of knowledge—usually acquired by completing a graduate or post-graduate course of education—and experience in science, humanities, and art.
III—Technical professions. This group includes professions that require the operational expertise and necessary experience in order to perform support and technical–practical activities in the areas of science, humanities, social economics, sport, and art. The knowledge required for such professions can generally be acquired by completing a high school education or first level university course.
IV—Clerical support workers. This group includes non-management level office workers and non-manual executive work, which usually require the standard high school formal education.
V—Qualified professions in business activities and services. This group comprises professions that perform management/customer service roles in business activities, accommodation/catering services, recreational/family support/social services, and public security/personal and property protection services.
VI—Craftsmen, skilled workers, and farmers. This includes specialist manual labor professions in all areas of economic activity, requiring experience, knowledge of materials, tools, machines, production processes, and properties/potential uses of the final product.
VII—Plant operators, stationary and mobile machine operators, and vehicle drivers. This group includes the set-up, maintenance, and checking of machines, automated industrial plants, and automatic assembly lines of mass products, machines, or machine parts. It also includes vehicle drivers and mobile and hoisting machine drivers.
VIII—Unskilled professions. This group consists of professions that require a sufficient level of knowledge and degree of experience to perform very simple and repetitive activities which include using hand tools, often the use of physical force and limited autonomy in decisions and initiative. Professions that fall into this category perform unskilled manual labor in farming, industry, services, gardening, doorman, and cleaning. They also provide executive support in office work and small itinerant business-related tasks.
The results show that the most effected macro group is Group VI, craftsmen, skilled workers, and farmers (35%), followed by Group VIII, unskilled professions (27%). The least affected category is Group II, intellectual and scientific professions.
3.2. Territorial Analysis: Distribution by Region of Residence
Furthermore, it is possible to analyze the territorial distribution of applications filed for the diseases in question, since the applicant’s region of residence is also indicated. In order to exclude the effect of the various occupancy rates in the different regions, calculations were based on the ratio between the applications and the number of occupants in each region separately. The application distribution by region for 2009, 2019, and the average over the period in question is shown in
Table 3.
In terms of the average number of applications filed over the 10-year period in relation to the average occupancy, Valle d’Aosta has a decidedly higher number of granted invalidity allowance and invalidity pension applications than the others. It thus qualifies for all intents and purposes as an outlier. High numbers are also reported in Molise, Basilicata, and Calabria, whereas the regions that report comparatively low numbers of accepted applications are Lombardy, Venice, and Piedmont.
3.3. Estimated Number of Beneficiaries and Social Security Costs
The total number of workers who receive social security benefits is published by the INPS Statistical Watchdog and displayed below in
Table 4. Using the total number of beneficiaries per year, based on the same distribution percentage by disease of the total number of new applications, we calculated the number of beneficiaries affected by the disease in question, atrial fibrillation.
The amount awarded is dependent on the type of benefit (lesser for IAs and greater for IPs), the type of pension fund to which the worker belongs, and the sum of said worker’s contributions. Since information pertaining to individual workers is unavailable, the average monthly amounts for both social security benefits, shown in
Table 4, has been used as a reference. The total social security burden for the disease in question has been estimated using the Monte Carlo simulation method [
9].
The estimates show that each year, on average, approximately 1100 workers receive social security benefits due to a diagnosis of atrial fibrillation. The majority receive an invalidity allowance and as such can continue to work. These benefits cost approximately €10 million per year. A comparison of the data from the first observation year (2009) with the last (2019) shows a rising trend in the number of beneficiaries and consequently in expenses (
Table 5).
4. Discussion
The results of the study show that cardiac diseases such as atrial fibrillation can lead to the partial or total loss of earning capacity for a significant number of people of working age. The fact that the Italian social security system is able to provide financial support for these types of workers is a considerable social victory that benefits the population, the value of which should neither be dismissed nor underestimated. For this reason, constant monitoring of social security payment data is essential, particularly for epidemiological and preventative purposes [
10,
11].
The Italian social security system spends in the region of EUR 11.5 million per year to support these workers. Over the 10 year period analyzed, this expenditure has increased by 50%. The fact that the age of the population of Italy has and continues [
12] to increase significantly may be a contributory factor to said upsurge. This includes the ever-increasing percentage of the working age population that fall into the age bracket most associated with a higher incidence of cardiac disease.
An atrial fibrillation diagnosis can have significant repercussions on the fitness for work of those whose employment involves a high level of physical strength or creates specific risks (for example driving automobiles). In respect of driving, particularly when such involves the transport of third parties, there is concern over the risk of road traffic accidents caused by the onset of an arrhythmia. The statistics in the literature show, however, that such an event is infrequent: one recent study [
13] showed that only 1.4/1000 non-fatal accidents and 4/1000 fatal accidents were ascribable to the driver’s health condition. Moreover, the most frequently identified clinical cause of such accidents was epilepsy, with all cardiac diseases accounting for just 8%.
Moderate physical activity does not seem to affect the onset of atrial fibrillation, whereas, according to a recent study, the risk of atrial fibrillation is significantly higher in those who work more than 55 h per week (OR: 1,44 1.42, 95% CI = 1.13–1.80,
p = 0.003) [
14,
15,
16].
It may also be possible that certain sectors are more affected by occupational risks such as work-related stress or instability. Further studies and analysis will need to be conducted in that regard.
The study also highlighted irregularities in the territorial distribution of benefits, taking into account the various occupancy rates in each region, and irregularities in the classifications of professions most affected by these diseases.
Despite such discrepancies, we believe that the social security system currently in place is functional and satisfies national needs. There is an evident need for constant monitoring for financial and healthcare purposes in addition to facilitating increasingly more uniform medico-legal assessments [
17]. In our opinion, it is fundamental to provide ongoing training for and knowledge sharing between medical assessors and specialists in the various disciplines such as cardiology, occupational medicine, and legal medicine in order to identify emerging worker protection needs appropriately and accurately for the sustainability of the social security system and for the benefit of the nation.
Further studies should focus on other common diseases such as diabetes, asthma, pulmonary diseases, cardiovascular accidents, and strokes, etc., from the analysis of these data, useful elements could emerge in order to orient health policy in the field of prevention, budget disbursements due to new impacts of diseases, and projections of the impacts of diseases in the coming decades could be constructed.


 ,
, 


{kind=link}