
Latent Class Analysis of Health Behavior Changes Due to COVID-19 among Middle-Aged Korean Workers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Data Collection
2.3. Instruments
2.3.1. General Characteristics and Health Problems
2.3.2. Implementation of COVID-19 Quarantine Rules and Changes in Daily Life
2.3.3. Changes in Health Behavior due to COVID-19
2.4. Data Analysis
3. Results
3.1. General Characteristics of Study Participants, Characteristics of Health Problems
3.2. Implementation of COVID-19 Quarantine Rules, Changes in Daily Life, and Changes in Health Behavior of Participants
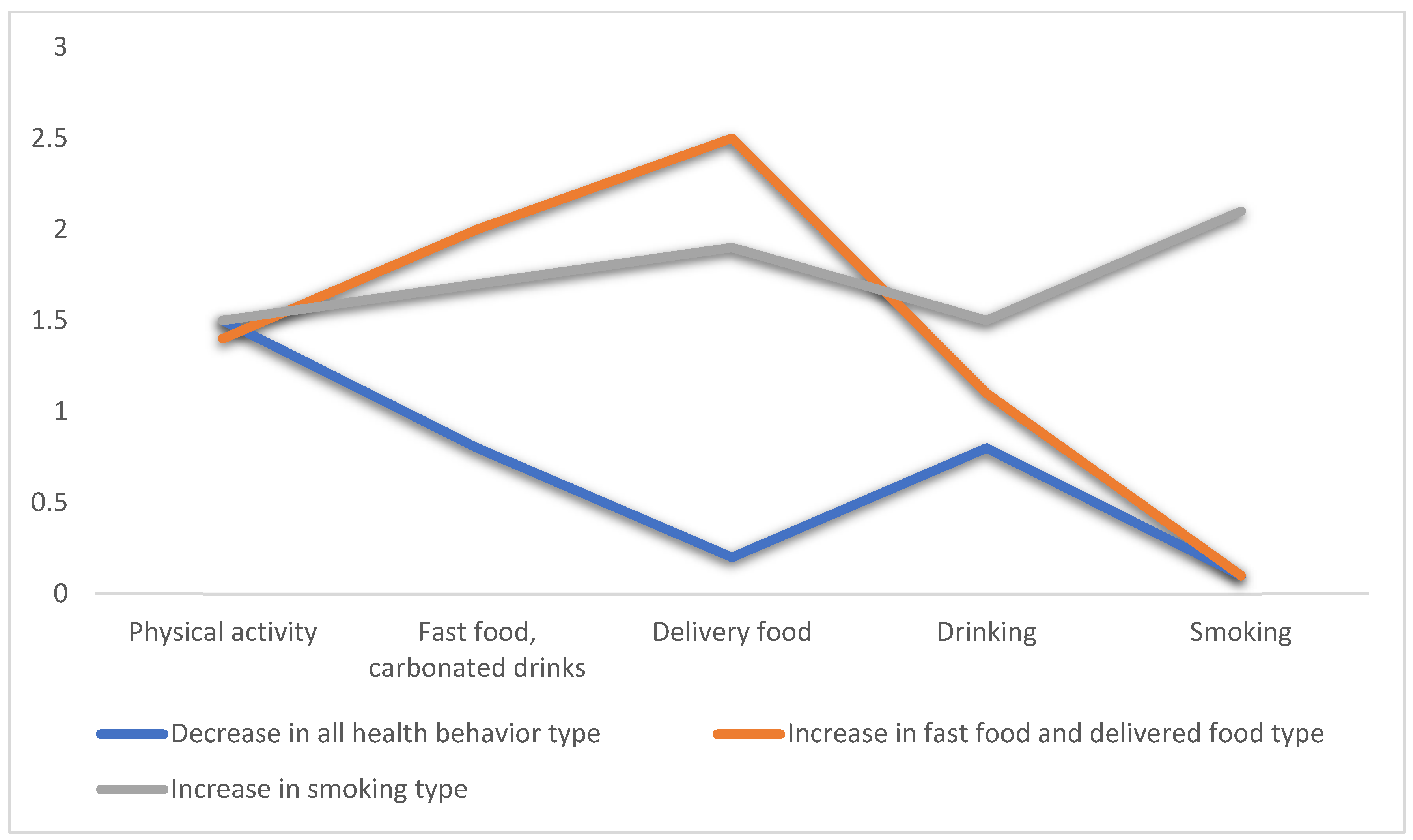
3.3. Types of Latent Classes for Changes in Health Behavior due to COVID-19
3.4. Predictive Factors by Type of Latent Class for Changes in Health Behavior due to COVID-19
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 1 November 2021).
- Kissler, S.M.; Tedijanto, C.; Lipsitch, M.; Grad, Y. Social distancing strategies for curbing the COVID-19 epidemic. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Guidance for Unvaccinated People. Social Distancing, Keep a Safe Distance to Slow the Spread. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/social-distancing.html (accessed on 1 October 2021).
- Naughton, F.; Ward, E.; Khondoker, M.; Belderson, P.; Marie Minihane, A.; Dainty, J.; Hanson, S.; Holland, R.; Brown, T.; Notley, C. Health behaviour change during the UK COVID-19 lockdown: Findings from the first wave of the C-19 health behaviour and well-being daily tracker study. Br. J. Health Psychol. 2021, 26, 624–643. [Google Scholar] [CrossRef]
- Arora, T.; Grey, I. Health behaviour changes during COVID-19 and the potential consequences: A mini-review. J. Health Psychol. 2020, 25, 1155–1163. [Google Scholar] [CrossRef]
- Choi, E.P.H.; Hui, B.P.H.; Wan, E.Y.F. Depression and Anxiety in Hong Kong during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3740. [Google Scholar] [CrossRef]
- Cénat, J.M.; Blais-Rochette, C.; Kokou-Kpolou, C.K.; Noorishad, P.G.; Mukunzi, J.N.; McIntee, S.E.; Dalexis, R.D.; Goulet, M.A.; Labelle, P.R. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 295, 113599. [Google Scholar] [CrossRef]
- Evanoff, B.A.; Strickland, J.R.; Dale, A.M.; Hayibor, L.; Page, E.; Duncan, J.G.; Kannampallil, T.; Gray, D.L. Work-Related and Personal Factors Associated With Mental Well-Being During the COVID-19 Response: Survey of Health Care and Other Workers. J. Med. Int. Res. 2020, 22, e21366. [Google Scholar] [CrossRef]
- Health and Safety Executive (HSE). Working Safely during the Coronavirus (COVID-19) Pandemic. 2021. Available online: https://www.hse.gov.uk/coronavirus/working-safely/index.htm (accessed on 5 October 2021).
- Lee, H.J. Health Promotion Strategy in the Era of New Infectious Diseases. J. Korea Soc. Wellness 2020, 15, 169–180. [Google Scholar] [CrossRef]
- Bosworth, H.B.; Bastian, L.A.; Kuchibhatla, M.N.; Steffens, K.C.; McBride, C.M.; Skinner, C.S.; Rimer, B.K.; Siegler, I.C. Depressive symptoms, menopausal status, and climacteric symptoms in women at midlife. Psychosom. Med. 2001, 63, 603–608. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Cho, Y.T. Comparison of Health Behaviors, Disease Prevalence between Middle Aged One-Person Households and Multi-Member Households in South Korea. Korea Inst. Health Soc. Aff. 2019, 39, 380–409. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, M.I.; Chan, S.J.; Moon, K.J. Identification and Prediction of Patterns of Health Promoting Behaviors among the Elderly. Health Soc. Welf. Rev. 2017, 37, 251–286. [Google Scholar] [CrossRef]
- Kim, H.S.; Kim, S.S.; Park, M.H. A Converged Study on the Influence on the Quality of Life for Early and Late Middle-aged Men. J. Korea Converg. Soc. 2018, 9, 133–145. [Google Scholar]
- Korea Centers for Disease Control and Prevention. Community Health Survey. 2020. Available online: https://chs.kdca.go.kr/chs/index.do (accessed on 29 November 2021).
- Poelman, M.P.; Gillebaart, M.; Schlinkert, C.; Dijkstra, S.C.; Derksen, E.; Mensink, F.; Hermans, R.C.J.; Aardening, P.; de Ridder, D.; de Vet, E. Eating behavior and food purchases during the COVID-19 lockdown: A cross-sectional study among adults in the Netherlands. Appetite 2021, 157, 105002. [Google Scholar] [CrossRef]
- Carroll, N.; Sadowski, A.; Laila, A.; Hruska, V.; Nixon, M.; Ma, D.W.L.; Haines, J. The Impact of COVID-19 on Health Behavior, Stress, Financial and Food Security among Middle to High Income Canadian Families with Young Children. Nutrients 2020, 12, 2352. [Google Scholar] [CrossRef] [PubMed]
- Choi, J. The Effect of Early Detection of Hypertension and Diabetes on Smoking and Alcohol Drinking. Health Soc. Welf. Rev. 2007, 27, 103–130. [Google Scholar] [CrossRef]
- Oh, D.K.; Kim, Y.M.; Lim, J.Y.; Cheong, W. Hypertension and Diabetes mellitus Management Effects of Community based Chronic Disease Management Program. J. Korean Acad. Soc. Home Care Nurs. 2012, 19, 74–82. [Google Scholar]
- Bourassa, K.J.; Sbarra, D.A.; Caspi, A.; Moffitt, T.E. Social Distancing as a Health Behavior: County-Level Movement in the United States During the COVID-19 Pandemic Is Associated with Conventional Health Behaviors. Ann. Behav. Med. 2020, 54, 548–556. [Google Scholar] [CrossRef]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef] [Green Version]
- Jo, H.U.; Choi, E.H. The Impact of COVID-19 on Health Prevention Behaviors in College Students: Focusing on the Health Belief Model. J. Korean Soc. Sch. Health 2021, 34, 115–122. [Google Scholar] [CrossRef]
- Yılmaz, C.; Gökmen, V. Neuroactive compounds in foods: Occurrence, mechanism and potential health effects. Food Res. 2020, 128, 108744. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, A.B.; Van Tilburg, W.A.; Igou, E.R.; Wisman, A.; Donnelly, A.E.; Mulcaire, J.B. Eaten up by boredom: Consuming food to escape awareness of the bored self. Front. Psychol. 2015, 6, 369–379. [Google Scholar] [CrossRef]
- Rodriguez-Martin, B.C.; Meule, A. Food craving: New contributions on its assessment, moderators, and consequences. Front. Psychol. 2015, 6, 21–23. [Google Scholar] [CrossRef] [Green Version]
- Biddle, S.J.H.; Garcia, E.B.; Pedisic, Z.; Bennie, J.; Vergeer, I.; Wiesner, G. Screen time, other sedentary behaviours, and obesity risk in adults: A review of reviews. Curr Obes Rep. 2017, 6, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Chenarides, L.; Grebitus, C.; Lusk, J.L.; Printezis, I. Food consumption behavior during the COVID-19 pandemic. Agribusiness 2020, 37, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Blom, V.; Lönn, A.; Ekblom, B.; Kallings, L.V.; Väisänen, D.; Hemmingsson, E.; Andersson, G.; Wallin, P.; Stenling, A.; Ekblom, Ö.; et al. Lifestyle Habits and Mental Health in Light of the Two COVID-19 Pandemic Waves in Sweden, 2020. Int. J. Environ. Res. Public Health 2021, 18, 3313. [Google Scholar] [CrossRef] [PubMed]
- Klemperer, E.M.; West, J.C.; Peasley-Miklus, C.; Villanti, A.C. Change in Tobacco and Electronic Cigarette Use and Motivation to Quit in Response to COVID-19. Nicotine Tob Res. 2020, 22, 1662–1663. [Google Scholar] [CrossRef]
- Bar-Zeev, Y.; Shauly, M.; Lee, H.; Neumark, Y. Changes in Smoking Behaviour and Home-Smoking Rules during the Initial COVID-19 Lockdown Period in Israel. Int. J. Environ. Res. Public Health 2021, 18, 1931. [Google Scholar] [CrossRef]
- Sprang, G.; Silman, M. Posttraumatic stress disorder in parents and youth after health-related disasters. Disaster Med. Public Health Prep. 2013, 7, 105–110. [Google Scholar] [CrossRef]
- Wang, G.; Zhang, Y.; Zhao, J.; Zhang, J.; Jiang, F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet 2020, 395, 945–947. [Google Scholar] [CrossRef]
- Waring, J.J.C.; Hébert, E.T.; Alexander, A.C.; Kendzor, D.E.; Businelle, M.S. Evaluating the influences of social support and smoking cues on daily smoking abstinence among socioeconomically disadvantaged adults. Addict. Behav. 2020, 100, 106107. [Google Scholar] [CrossRef]
- Masho, S.W.; Do, E.; Adekoya, S. Social Support and Smoking during Pregnancy. J. Womens Health Care. 2014, 3, 1000179. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.O.; Song, J.A.; Lee, S.J. Types of Smoking in Adult Smokers and Influential Variables Related to Smoking. J. Korean Acad. Soc. Adult Nurs. 2008, 20, 77–90. [Google Scholar]
- Sussman, S.; Brannon, B.R.; Dent, C.W.; Hansen, W.B.; Johnson, C.A.; Flay, B.R. Relations of coping effort, coping strategies, perceived stress, and cigarette smoking among adolescents. Int. J. Addict. 1993, 28, 599–612. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Romano, L.; Di Renzo, L.; Di Lorenzo, N.; Cenname, G.; Gualtieri, P. Obesity: A preventable, treatable, but relapsing disease. Nutrition 2020, 71, 110615. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.I.; Lee, H.S.; Lee, S.W.; Shim, K.W.; Rhou, I.; Jeoon, Y.H. Hand Grip Strength according to the Smoking Status in Korean Adults: The 7th Korea National Health and Nutrition Examination Survey 2016–2017. Korean J. Fam. Pract. 2020, 10, 355–363. [Google Scholar] [CrossRef]
- Lima, S.; Teixeira, L.; Esteves, R.; Ribeiro, F.; Pereira, F.; Teixeira, A.; Magalhaes, C. Spirituality and quality of life in older adults: A path analysis model. BMC Geriatr. 2020, 20, 259. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Categories | N | % | |
|---|---|---|---|---|
| General characteristics | Age group | 40–44 | 2801 | 22.2 |
| 45–49 | 3521 | 27.9 | ||
| 50–54 | 3408 | 27.0 | ||
| 55–60 | 2891 | 22.9 | ||
| M (SD) | 49.5 (5.6) | |||
| Gender | Male | 7086 | 56.1 | |
| Female | 5535 | 43.9 | ||
| Household type | One-person households | 1032 | 8.2 | |
| Married couples | 1683 | 13.3 | ||
| Parents + children | 8347 | 66.1 | ||
| Other cohabitation households | 1559 | 12.4 | ||
| Occupation | Professional and related occupations | 2643 | 20.9 | |
| Administrator | 834 | 6.6 | ||
| Office worker | 2356 | 18.7 | ||
| Sales and service positions | 2791 | 22.1 | ||
| Technical job | 2351 | 18.6 | ||
| Simple labor | 1646 | 13.0 | ||
| Work position | Employers and owner-operators | 3225 | 25.6 | |
| Wage workers | 9195 | 72.9 | ||
| Unpaid family workers | 201 | 1.6 | ||
| Health problems | Hypertension | Yes | 2380 | 18.9 |
| No | 10,241 | 81.1 | ||
| Diabetes | Yes | 891 | 7.1 | |
| No | 11,730 | 92.9 | ||
| PHQ-9 | Normality | 11,142 | 88.3 | |
| Mild depression | 1235 | 9.8 | ||
| Moderate depression | 190 | 1.5 | ||
| Moderately severe depression | 42 | 0.3 | ||
| Severe depression | 12 | 0.1 | ||
| M (SD) | 1.8 (2.8) | |||
| Characteristics | Categories | N | % | |
|---|---|---|---|---|
| COVID-19 quarantine rules | Social distancing | Certainly | 7812 | 61.9 |
| Yes | 3741 | 29.6 | ||
| No | 482 | 3.8 | ||
| Not applicable | 586 | 4.6 | ||
| Refrain from going out | Certainly | 7534 | 59.7 | |
| Yes | 3698 | 29.3 | ||
| No | 217 | 1.7 | ||
| Not applicable | 1172 | 9.3 | ||
| COVID-19 daily life changes | Meeting with friends or neighbors | Increased | 16 | 0.1 |
| Similar as before | 936 | 7.4 | ||
| Decreased | 11,119 | 88.1 | ||
| Not applicable | 550 | 4.4 | ||
| COVID-19 impact life score | ≥20 | 1168 | 9.3 | |
| 21–40 | 2533 | 20.1 | ||
| 41–60 | 5106 | 40.5 | ||
| 61–80 | 2973 | 23.6 | ||
| ≤81 | 841 | 6.7 | ||
| M (SD) | 53.6 (21.2) | |||
| COVID-19 health behavior changes | Physical activity | Increased | 819 | 6.5 |
| Similar as before | 4874 | 38.6 | ||
| Decreased | 6225 | 49.3 | ||
| Not applicable | 703 | 5.6 | ||
| Fast food, carbonated drinks | Increased | 2234 | 17.7 | |
| Similar as before | 6452 | 51.1 | ||
| Decreased | 1090 | 8.6 | ||
| Not applicable | 2845 | 22.5 | ||
| Delivered food | Increased | 4355 | 23.0 | |
| Similar as before | 4502 | 35.7 | ||
| Decreased | 858 | 6.8 | ||
| Not applicable | 2906 | 23.0 | ||
| Drinking | Increased | 699 | 5.5 | |
| Similar as before | 4350 | 34.5 | ||
| Decreased | 3631 | 28.8 | ||
| Not applicable | 3941 | 31.2 | ||
| Smoking | Increased | 381 | 3.0 | |
| Similar as before | 2911 | 23.1 | ||
| Decreased | 681 | 5.4 | ||
| Not applicable | 8648 | 68.5 | ||
| Number of Groups | AIC | BIC | saBIC | LMR | BLRT | Estimated Probability for Trajectory Group (%) | |||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||||||
| 1 | 170,314.599 | 170,389.031 | 170,357.252 | n/a | n/a | 100.0 | |||
| 2 | 153,083.774 | 153,202.864 | 153,152.017 | <0.001 | <0.001 | 73.9 | 26.1 | ||
| 3 | 147,906.303 | 148,070.051 | 148,000.137 | <0.001 | <0.001 | 22.1 | 51.9 | 26.1 | |
| 4 | 144,704.642 | 144,913.050 | 144,824.069 | 0.476 | 1.000 | ||||
| Group Indices | Class 1 | Class 2 | Class 3 | F | p | |||
|---|---|---|---|---|---|---|---|---|
| (N = 2784, 22.1%) | (N = 6545, 51.9%) | (N = 3292, 26.1%) | ||||||
| M | (SD) | M | (SD) | M | (SD) | |||
| Physical activity | 1.5 | 0.8 | 1.4 | 0.7 | 1.5 | 0.7 | 11.357 | <0.001 |
| Fast food, carbonated drinks | 0.8 | 0.9 | 2.0 | 0.8 | 1.7 | 0.9 | 1842.898 | <0.001 |
| Delivered food | 0.2 | 0.4 | 2.5 | 0.6 | 1.9 | 1.1 | 10,702.338 | <0.001 |
| Drinking | 0.8 | 0.9 | 1.1 | 0.9 | 1.5 | 0.8 | 552.132 | <0.001 |
| Smoking | 0.1 | 0.3 | 0.1 | 0.3 | 2.1 | 0.3 | 66,164.429 | <0.001 |
| Characteristics | Categories | Comparison Group (Ref = Class 1) | (Ref = Class 2) | |||||
|---|---|---|---|---|---|---|---|---|
| Class 2 | Class 3 | Class 3 | ||||||
| OR | p | OR | p | OR | p | |||
| Health problems | Hypertension (ref = none) | Existence | 1.153 | 0.023 | 1.049 | 0.513 | 0.910 | 0.125 |
| Diabetes (ref = none) | Existence | 0.743 | 0.001 | 0.788 | 0.020 | 1.060 | 0.531 | |
| Depression | 1.006 | 0.503 | 1.036 | 0.001 | 1.030 | 0.001 | ||
| COVID-19 quarantine rules | Social distancing | Certainly | 1.259 | 0.043 | 1.226 | 0.135 | 0.974 | 0.831 |
| (ref = N/A) | Yes | 1.466 | 0.001 | 1.502 | 0.004 | 1.025 | 0.848 | |
| No | 1.907 | <0.001 | 1.917 | 0.001 | 1.005 | 0.975 | ||
| Refrain from going out | Certainly | 1.569 | <0.001 | 1.171 | 0.120 | 0.746 | 0.002 | |
| (ref = N/A) | Yes | 1.547 | <0.001 | 1.182 | 0.127 | 0.764 | 0.006 | |
| No | 1.229 | 0.306 | 0.958 | 0.850 | 0.780 | 0.199 | ||
| COVID-19 daily life changes | Meeting with friends or neighbors | Decreased | 2.138 | <0.001 | 2.133 | <0.001 | 0.998 | 0.986 |
| (ref = N/A) | Similar as before | 2.455 | <0.001 | 4.076 | <0.001 | 1.660 | 0.001 | |
| Increased | 2.522 | 0.273 | 17.952 | 0.001 | 7.117 | 0.003 | ||
| COVID-19 impact life score | ≥20 | 1.432 | 0.003 | 1.385 | 0.020 | 0.967 | 0.790 | |
| (ref ≤ 81) | 21–40 | 1.507 | <0.001 | 1.068 | 0.593 | 0.709 | 0.002 | |
| 41–60 | 1.588 | <0.001 | 1.132 | 0.270 | 0.713 | 0.001 | ||
| 61–80 | 1.362 | 0.002 | 1.046 | 0.703 | 0.768 | 0.013 | ||
| −2 Log Likelihood = 20,698.541 χ2 = 4286.357 df = 56 p < 0.001 | ||||||||
| Cox and Snell R2 = 0.288 Nagelkerke R2 = 0.331 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, E.-H.; Kim, W.-J.; Baek, E.-M. Latent Class Analysis of Health Behavior Changes Due to COVID-19 among Middle-Aged Korean Workers. Int. J. Environ. Res. Public Health 2022, 19, 1832. https://doi.org/10.3390/ijerph19031832
Choi E-H, Kim W-J, Baek E-M. Latent Class Analysis of Health Behavior Changes Due to COVID-19 among Middle-Aged Korean Workers. International Journal of Environmental Research and Public Health. 2022; 19(3):1832. https://doi.org/10.3390/ijerph19031832
Chicago/Turabian StyleChoi, Eun-Hi, Won-Jong Kim, and Eun-Mi Baek. 2022. "Latent Class Analysis of Health Behavior Changes Due to COVID-19 among Middle-Aged Korean Workers" International Journal of Environmental Research and Public Health 19, no. 3: 1832. https://doi.org/10.3390/ijerph19031832