
Back Pain and Body Posture Evaluation Instrument for Children and Adolescents (BackPEI-CA): Expansion, Content Validation, and Reliability

 ,
,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire Update
2.2. Content Validity
2.3. Reliability
2.4. Sample
2.5. Statistical Analysis
3. Results
3.1. Content Validation
3.2. Reliability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kamper, S.J.; Parma, T.; Williams, C.M. The prevalence, risk factors, prognosis and treatment for back pain in children and adolescents: An overview of systematic reviews. Best Pract. Res. Clin. Rheumatol. 2017, 30, 1021–1036. [Google Scholar] [CrossRef] [PubMed]
- Alonso-García, M.; Sarría-Santamera, A. The Economic and Social Burden of Low Back Pain in Spain: A National Assessment of the Economic and Social Impact of Low Back Pain in Spain. Spine 2020, 45, E1026–E1032. [Google Scholar] [CrossRef] [PubMed]
- Fabricant, P.D.; Heath, M.R.; Schachne, J.M.; Doyle, S.M.; Green, D.W.; Widmann, R.F. The Epidemiology of Back Pain in American Children and Adolescents. Spine 2020, 45, 1135–1142. [Google Scholar] [CrossRef] [PubMed]
- Noll, M.; Candotti, C.T.; Vieira, A.; Loss, J.F. Back Pain and Body Posture Evaluation Instrument (BackPEI): Development, content validation and reproducibility. Int. J. Public Health 2013, 58, 565–572. [Google Scholar] [CrossRef]
- Noll, M.; Candotti, C.T.; Da Rosa, B.N.; Do Valle, M.B.; Antoniolli, A.; Vieira, A.; Loss, J.F. High prevalence of inadequate sitting and sleeping postures: A three-year prospective study of adolescents. Sci. Rep. 2017, 7, 14929. [Google Scholar] [CrossRef] [Green Version]
- Noll, M.; Noll, P.R.S.; Neto, J.L.R.; Leal, V.N.; Rosa, B.N.D.; Candotti, C.T. Back pain and behavioral habits of high school students: A comparative study of two Brazil’s regions. Rev. Bras. Reumatol. 2017, 57, 495–499. [Google Scholar] [CrossRef] [Green Version]
- Noll, M.; Candotti, C.T.; Rosa, B.N.D.; Vieira, A.; Loss, J.F. Back pain and its risk factors in Brazilian adolescents: A longitudinal study. Br. J. Pain 2019, 15, 16–25. [Google Scholar] [CrossRef]
- Da Rosa, B.N.; Furlanetto, T.S.; Noll, M.; Sedrez, J.A.; Schmit, E.F.D.; Candotti, C.T. 4-Year Longitudinal Study of the Assessment of Body Posture, Back Pain, Postural and Life Habits of Schoolchildren. Motricidade 2017, 13, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Miñana-Signes, V.; Monfort-Pañego, M.; Bosh-Bivià, A.H.; Noll, M. Prevalence of low back pain among primary school students from the city of Valencia (Spain). Healthcare 2021, 9, 270. [Google Scholar] [CrossRef]
- Ozdemir, S.; Gencbas, D.; Tosun, B.; Bebis, H.; Sinan, O. Musculoskeletal Pain, Related Factors, and Posture Profiles Among Adolescents: A Cross-Sectional Study from Turkey. Pain Manag. Nurs. 2021, 22, 522–530. [Google Scholar] [CrossRef]
- Gençbaş, D.; Bebiş, H. The validity and reliability of the Turkish version of Back Pain and Body Posture Evaluation Instrument (BackPEI). Acibadem Univ. Saglik Bilim. Derg. 2020, 10, 83–389. [Google Scholar] [CrossRef]
- Miñana-Signes, V.; Monfort-Pañego, M.; Morant, J.; Noll, M. Cross-Cultural Adaptation and Reliability of the Back Pain and Body Posture Evaluation Instrument (BackPEI) to the Spanish Adolescent Population. Int. J. Environ. Res. Public Health 2021, 18, 854. [Google Scholar] [CrossRef] [PubMed]
- Kamper, S.J.; Henschke, N.; Hestbaek, L.; Dunn, K.M.; Williams, C.M. Musculoskeletal pain in children and adolescents. Braz. J. Phys. Ther. 2016, 20, 275–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaterlaus, J.M.; Aylward, A.; Tarabochia, D.; Martin, J.D. “A smartphone made my life easier”: An exploratory study on age of adolescent smartphone acquisition and well-being. Comput. Hum. Behav. 2021, 114, 106563. [Google Scholar] [CrossRef]
- Yang, S.Y.; De Chen, M.; Huang, Y.C.; Lin, C.Y.; Chang, J.H. Association Between Smartphone Use and Musculoskeletal Discomfort in Adolescent Students. J. Community Health 2017, 42, 423–430. [Google Scholar] [CrossRef]
- Fischer-Grote, L.; Kothgassner, O.D.; Felnhofer, A. Risk factors for problematic smartphone use in children and adolescents: A review of existing literature. Neuropsychiatrie 2019, 33, 179–190. [Google Scholar] [CrossRef] [Green Version]
- Damasceno, G.M.; Ferreira, A.S.; Nogueira, L.A.C.; Reis, F.J.J.; Andrade, I.C.S.; Meziat-Filho, N. Text neck and neck pain in 18–21-year-old young adults. Eur. Spine J. 2018, 27, 1249–1254. [Google Scholar] [CrossRef]
- Gustafsson, E.; Thomée, S.; Grimby-Ekman, A.; Hagberg, M. Texting on mobile phones and musculoskeletal disorders in young adults: A five-year cohort study. Appl. Ergon. 2017, 58, 208–214. [Google Scholar] [CrossRef]
- Candotti, C.T.; Schmit, E.F.D.; Pivotto, L.R.; Raupp, E.G.; Noll, M.; Vieira, A.; Loss, J.F. Back Pain and Body Posture Evaluation Instrument for Adults: Expansion and Reproducibility. Pain Manag. Nurs. 2018, 19, 415–423. [Google Scholar] [CrossRef]
- Grant, J.S.; Davis, L.L. Selection and use of content experts for instrument development. Res. Nurs. Health 1997, 20, 269–274. [Google Scholar] [CrossRef]
- Sim, J.; Wright, C.C.; Sim, J.; Wright, C.C. The Kappa Statistic in Reliability Studies: Use, Interpretation, and Sample Size Requirements. Phys. Ther. 2005, 85, 257–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Fleiss, J.N.; Levin, B.; Paik, M.C. Statistical Methods for Rates and Proportions, 3rd ed.; Wiley: New York, NY, USA, 2004. [Google Scholar]
- Janse, A.J.; Gemke, R.J.B.J.; Uiterwaal, C.S.P.M.; Van Der Tweel, I.; Kimpen, J.L.L.; Sinnema, G. Quality of life: Patients and doctors don’t always agree: A meta-analysis. J. Clin. Epidemiol. 2004, 57, 653–661. [Google Scholar] [CrossRef]
- Schlademann, S.; Meyer, T.; Raspe, H. The test-retest reliability of a questionnaire on the occurrence and severity of back pain in a German population sample. Int. J. Public Health 2008, 53, 96–103. [Google Scholar] [CrossRef]
- Kramer, M.S.; Feinstein, A.R. Clinical biostatistics LIV. The biostatistics of concordance. Clin. Pharmacol. Ther. 1981, 29, 111–123. [Google Scholar] [CrossRef]
- Staes, F.; Stappaerts, K.; Vertommen, H.; Everaert, D.; Coppieters, M. Reproducibility of a survey questionnaire for the investigation of low back problems in adolescents. Acta Paediatr. 1999, 88, 1269–1273. [Google Scholar] [CrossRef] [PubMed]
- Lauridsen, H.H.; Hestbaek, L. Development of the young spine questionnaire. BMC Musculoskelet. Disord. 2013, 14, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Smeets, R.; Köke, A.; Lin, C.W.; Ferreira, M.; Demoulin, C. Measures of function in low back pain/disorders: Low Back Pain Rating Scale (LBPRS), Oswestry Disability Index (ODI), Progressive Isoinertial Lifting Evaluation (PILE), Quebec Back Pain Disability Scale (QBPDS), and Roland-Morris Disability Questionnaire. Arthritis Care Res. 2011, 63, 158–173. [Google Scholar] [CrossRef]
- Statista Number of Smartphone Users from 2016 to 2021. Available online: https://www.statista.com/statistics/330695/number-of-smartphone-users-worldwide/ (accessed on 20 October 2021).
- Christensen, M.A.; Bettencourt, L.; Kaye, L.; Moturu, S.T.; Nguyen, K.T.; Olgin, J.E.; Pletcher, M.J.; Marcus, G.M. Direct measurements of smartphone screen-time: Relationships with demographics and sleep. PLoS ONE 2016, 11, e165331. [Google Scholar] [CrossRef] [Green Version]
- Popescu, A.; Lee, H. Neck Pain and Lower Back Pain. Med. Clin. N. Am. 2020, 104, 279–292. [Google Scholar] [CrossRef]
- Hogg-Johnson, S.; van der Velde, G.; Carroll, L.J.; Holm, L.W.; Cassidy, J.D.; Guzman, J.; Côté, P.; Haldeman, S.; Ammendolia, C.; Carragee, E.; et al. The Burden and Determinants of Neck Pain in the General Population. Results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. J. Manip. Physiol. Ther. 2009, 32, S46–S60. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Back Pain | Frequency (%) | Neck Pain | Frequency (%) |
|---|---|---|---|
| Presence | Presence | ||
| Yes | 71 (67.6%) | Yes | 64 (62.1%) |
| No | 27 (25.7%) | No | 36 (35%) |
| I don’t know | 7 (6.7%) | I don’t know | 3 (2.9%) |
| Total | 105 (100%) | Total | 103 (100%) |
| Frequency | Frequency | ||
| Only once | 24 (29.3%) | Only once | 15 (22.7%) |
| At least once a month | 23 (28%) | At least once a month | 22 (33.3%) |
| At least once a week | 24 (29.3%) | At least once a week | 23 (34.8%) |
| I don’t know | 11 (13.4%) | I don’t know | 6 (9.2%) |
| Total | 82 (100%) | Total | 66 (100%) |
| Absenteeism at school | Absenteeism at school | ||
| Yes | 4 (43.9%) | Yes | 5 (7.6%) |
| No | 77 (93.9%) | No | 59 (89.4%) |
| I don’t know | 1 (1.2%) | I don’t know | 2 (3%) |
| Total | 82 (100%) | Total | 66 (100%) |
| Disability | Disability | ||
| Yes | 16 (19.7%) | Yes | 12 (18.5%) |
| No | 64 (79.7%) | No | 52 (80%) |
| I don’t know | 1 (0.6%) | I don’t know | 1 (1.5%) |
| Total | 81 (100%) | Total | 65 (100%) |
| Daily Time of Mobile Devices Utilization | |
| 0 to 1 h | 9 (8.6%) |
| 2 to 3 h | 33 (31.4%) |
| 4 to 5 h | 24 (22.9%) |
| 6 h or more | 27 (25.7%) |
| I don’t know | 12 (11.4%) |
| Total | 105 (100%) |
| Posture Adopted to Use the Mobile Device in the Sitting Position | |
| Adequate | 34 (32.4%) |
| Inadequate | 57 (54.3%) |
| I don’t know | 14 (13.3%) |
| Total | 105 (100%) |
| Posture Adopted to Use the Mobile Device in the Standing Position | |
| Adequate | 56 (53.3%) |
| Inadequate | 43 (41%) |
| I don’t know | 6 (5.7%) |
| Total | 100 (100%) |
| BackPEI-CA Question | Item | CVI 1st Assessment | CVI 2nd Assessment |
|---|---|---|---|
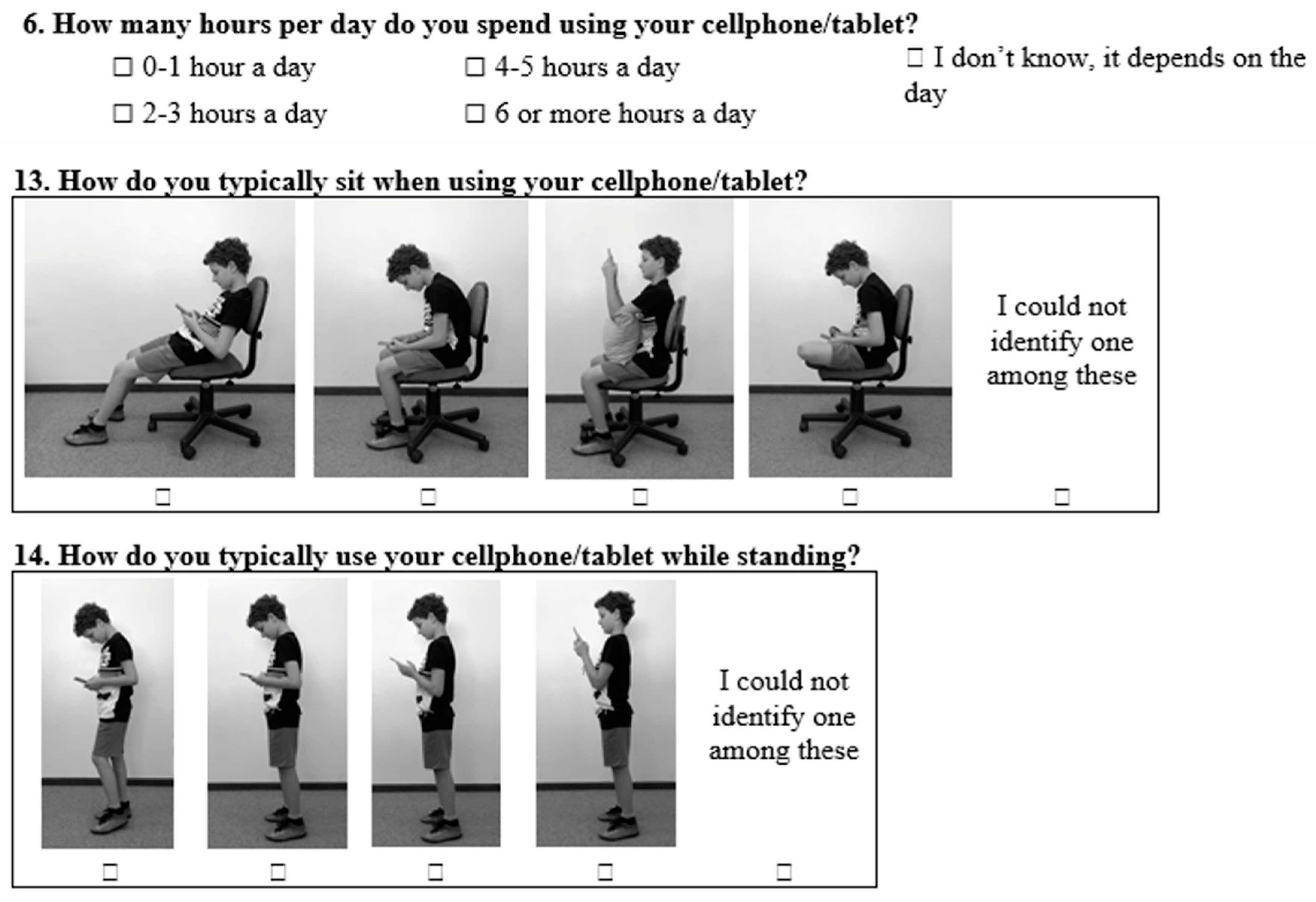
| 6, 13, and 14 | Regarding the insertion of new questions, do you think it is possible to identify behavior during smart phones/tablet use? | 0.6 | 0.9 |
| 13 and 14 | Regarding the quality of images (photos) and adequation of postures used | 0.9 | 1.0 |
| 23 and 24 | Regarding the insertion of new questions about back pain, do you think they enable assessment of the impact of back pain on children’s and adolescents’ lives? | 0.9 | 1.0 |
| 22 | Regarding the adequacy of options to answer about the back pain frequency | 0.6 | 1.0 |
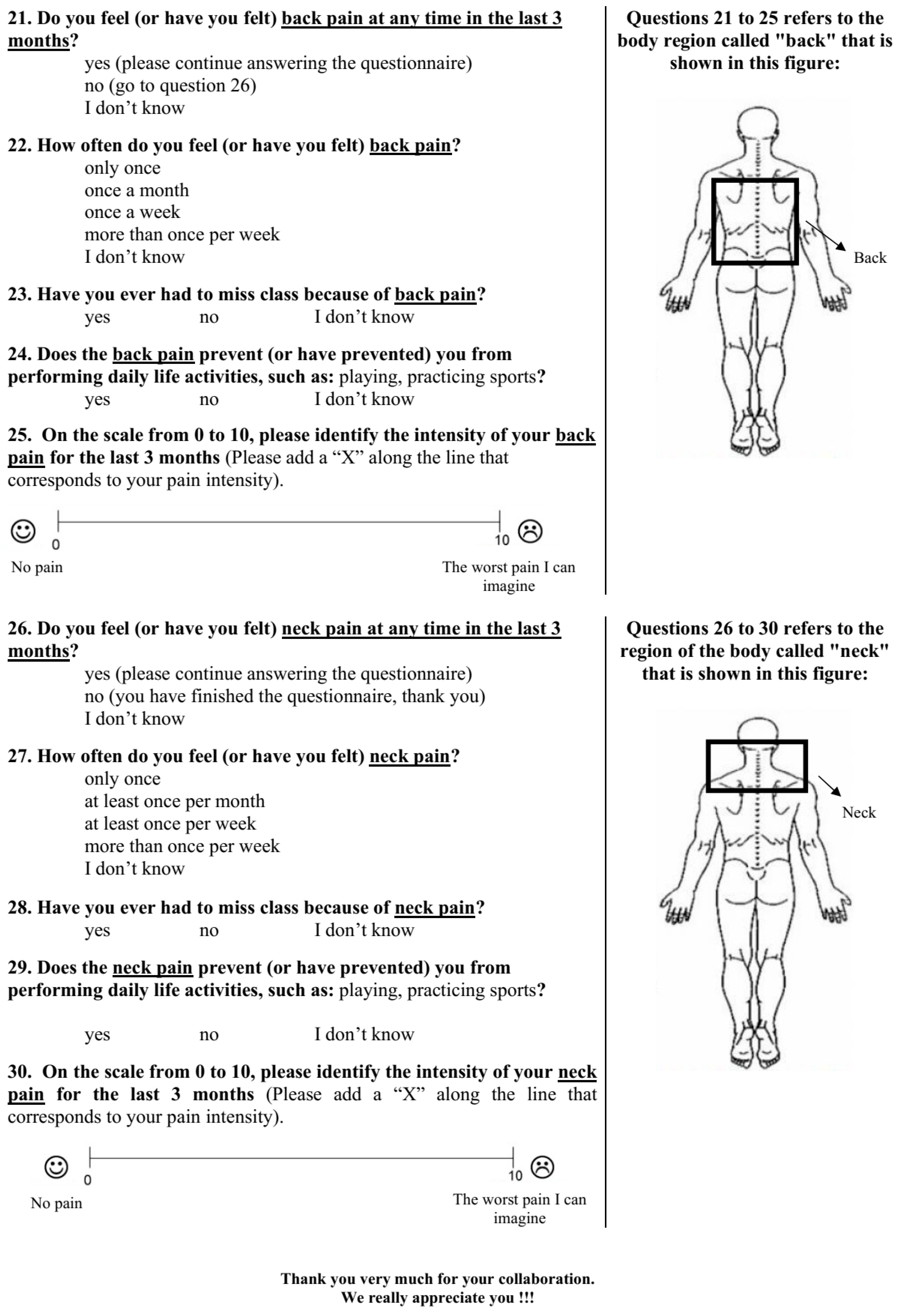
| 21–25 | Regarding the new graphic design of questions about back pain, do you think they facilitate the understanding that “back pain” refers to any thoracic and lumbar region? | 0.8 | 1.0 |
| 26–30 | Regarding the insertion of new questions about neck pain, do you think it is possible to identify the presence, frequency, and intensity of neck pain? | 0.8 | 0.9 |
| 26–30 | Regarding graphic design of questions about neck pain, do you think they facilitate the understanding that “neck pain” refers to any region of the cervical spine? | 0.8 | 1.0 |
| Question | Question Description | n | Agreement (%) | Kappa (p) | 95%CI | Bias |
|---|---|---|---|---|---|---|
| 6 | How many hours per day do you spend using your cellphone/tablet? | 105 | 52.4 | 0.439 (<0.001) | 0.309–0.569 | −0.001 |
| 13 | How do you typically sit when using your cellphone/tablet? | 105 | 55.3 | 0.418 (<0.001) | 0.288–0.551 | −0.001 |
| 14 | How do you typically use your cellphone/tablet while standing? | 104 | 67.3 | 0.477 (<0.001) | 0.342–0.596 | −0.004 |
| 21 | Have you felt (or been feeling) back pain in the last three months? | 104 | 76 | 0.451 (<0.001) | 0.286–0.598 | −0.007 |
| 22 | How often do you feel (or have you felt) back pain? | 71 | 60.6 | 0.451 (<0.001) | 0.330–0.554 | −0.002 |
| 23 | Have you ever missed any class because of the back pain? | 71 | 81,7 | 0.559 (<0.001) | 0.380–0.711 | −0.008 |
| 24 | Does the back pain prevent (or has it prevented) you from performing daily life activities, such as playing or practicing sports? | 70 | 84.3 | 0.523 (<0.001) | 0.265–0.746 | −0.006 |
| 26 | Have you felt (or been feeling) neck pain in the last three months? | 103 | 77.5 | 0.556 (<0.001) | 0.409–0.713 | −0.001 |
| 27 | How often do you feel (or have you felt) neck pain? | 64 | 56.4 | 0.432 (<0.001) | 0.311–0.561 | −0.001 |
| 28 | Have you ever missed any class because of the neck pain? | 56 | 92.5 | 0.677 (<0.001) | 0.364–0.913 | −0.013 |
| 29 | Does the neck pain prevent (or has it prevented) you from performing daily life activities, such as playing or practicing sports? | 53 | 79.2 | 0.453 (<0.001) | 0.214–0.679 | −0.004 |
| Question | Question Description | n | ICC | 95%CI | Test–Mean (SD) | Retest–Mean (SD) | SEM | MDC |
|---|---|---|---|---|---|---|---|---|
| 25 | Back pain intensity (cm) | 70 | 0.828 | 0.828–0.933 | 5.2 (1.9) | 5.1 (1.9) | 0.81 | 1.58 |
| 30 | Neck pain intensity (cm) | 56 | 0.824 | 0.700–0.897 | 4.9 (2) | 4.9 (2.3) | 0.85 | 1.66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Rosa, B.N.; Candotti, C.T.; Pivotto, L.R.; Noll, M.; Silva, M.G.; Vieira, A.; Loss, J.F. Back Pain and Body Posture Evaluation Instrument for Children and Adolescents (BackPEI-CA): Expansion, Content Validation, and Reliability. Int. J. Environ. Res. Public Health 2022, 19, 1398. https://doi.org/10.3390/ijerph19031398
da Rosa BN, Candotti CT, Pivotto LR, Noll M, Silva MG, Vieira A, Loss JF. Back Pain and Body Posture Evaluation Instrument for Children and Adolescents (BackPEI-CA): Expansion, Content Validation, and Reliability. International Journal of Environmental Research and Public Health. 2022; 19(3):1398. https://doi.org/10.3390/ijerph19031398
Chicago/Turabian Styleda Rosa, Bruna Nichele, Cláudia Tarragô Candotti, Luiza Rampi Pivotto, Matias Noll, Marcelle Guimarães Silva, Adriane Vieira, and Jefferson Fagundes Loss. 2022. "Back Pain and Body Posture Evaluation Instrument for Children and Adolescents (BackPEI-CA): Expansion, Content Validation, and Reliability" International Journal of Environmental Research and Public Health 19, no. 3: 1398. https://doi.org/10.3390/ijerph19031398