
Radiological and Functional Assessment of Treatment Outcomes in Patients after Open Reduction with Internal Fixation (ORIF) of Acetabular Fractures


Abstract
:1. Introduction
2. Materials and Methods
2.1. The Clinical Group
2.2. Radiological and Functional Analysis
2.3. Statistical Analysis
3. Results
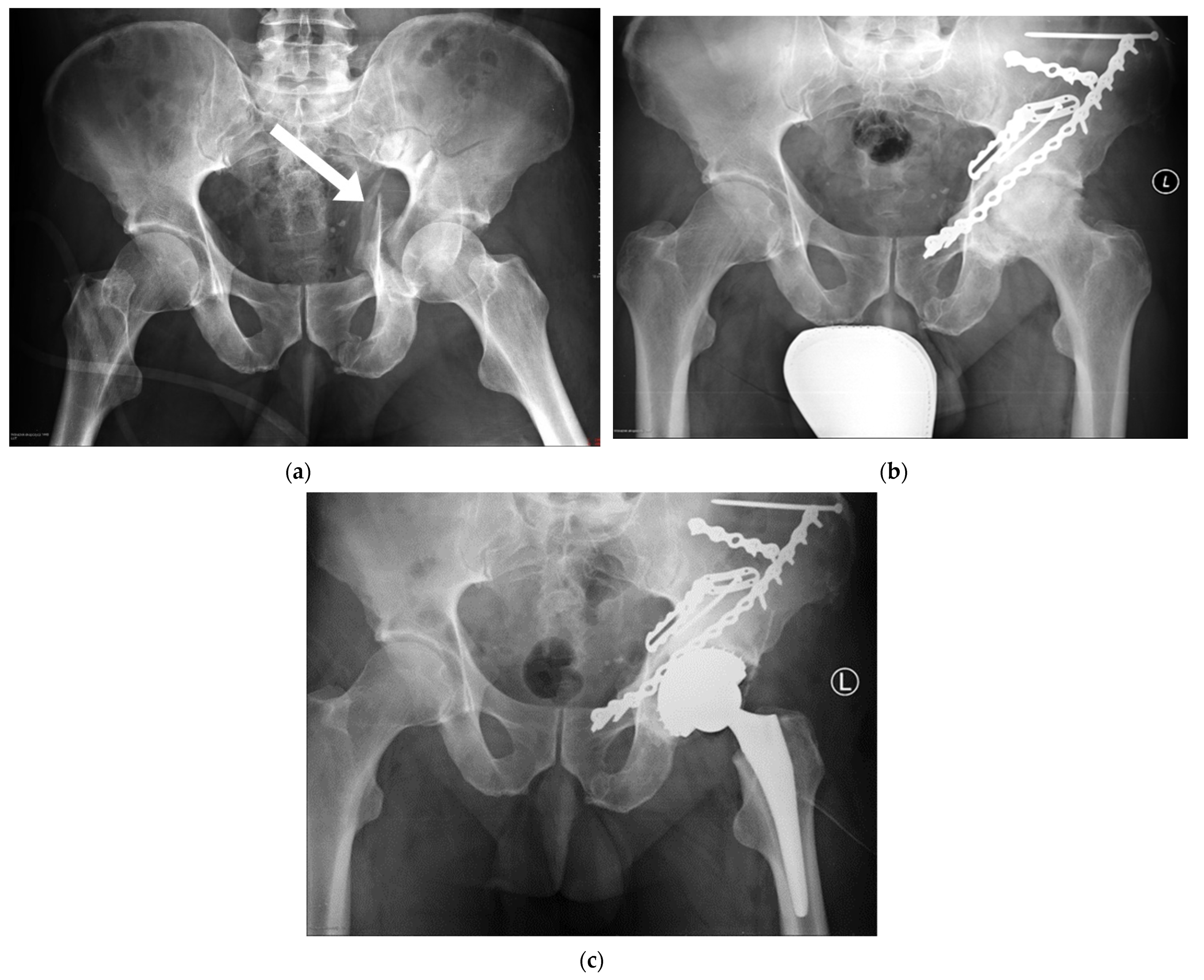
3.1. Radiological Assessment
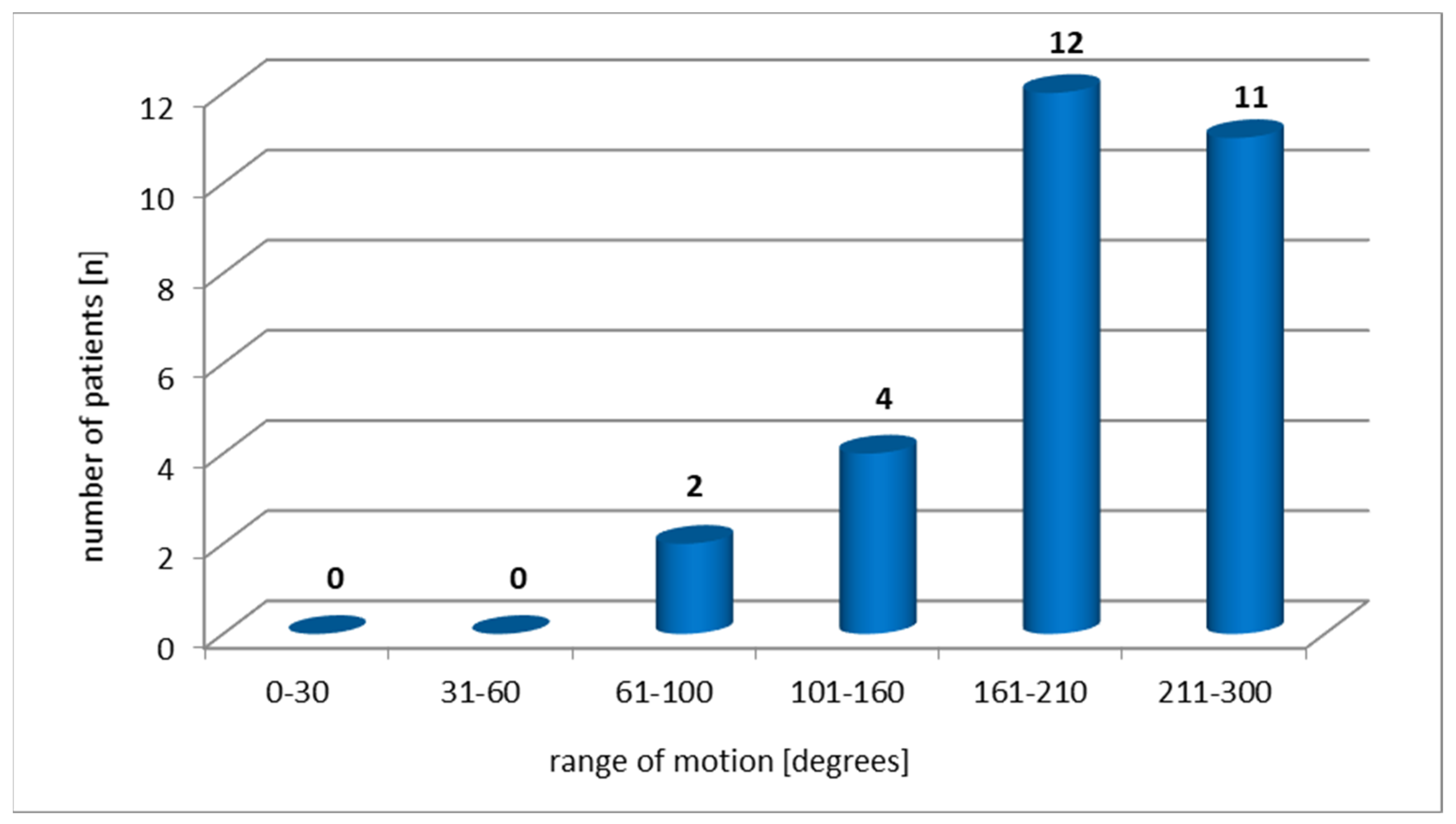
3.2. Functional Assessment
4. Discussion
4.1. Limitations of the Study
4.2. The Value of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rommens, P.M. Is there a role for percutaneous pelvic and acetabular reconstruction? Inj. Int. J. Care Inj. 2007, 38, 463–477. [Google Scholar] [CrossRef]
- Caban, A.; Zawadzki, A.; Sokólski, B.; Marczyński, W. Ocena wyników leczenia operacyjnego złamań panewki stawu biodrowego. Chir. Narządów Ruchu 2011, 76, 336–344. [Google Scholar]
- Firoozabadi, R.; Spitler, C.; Schlepp, C.; Hamilton, B.; Agel, J.; Routt, M.C.; Tornetta, P. Determining stability in posterior wall acetabular fractures. J. Orthop. Trauma 2015, 29, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Gänsslen, A.; Steinke, B.; Krettek, C. Osteosynthese von Frakturen der hinteren Wand des Azetabulums. Oper. Orthop. Traumatol. 2009, 21, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Giannoudis, P.V.; Tzioupis, C.; Papathanassopoulos, A.; Obakponovwe, O.; Roberts, C. Articular step-off and risk of post-traumatic osteoarthritis. Evidence today. Inj. Int. J. Care Inj. 2010, 41, 986–995. [Google Scholar] [CrossRef] [PubMed]
- Grubor, P.; Krupic, F.; Biscevic, M.; Grubor, M. Controversies in treatment of acetabular fracture. Med. Arch. 2015, 69, 16–20. [Google Scholar] [CrossRef]
- Magu, N.K.; Gogna, P.; Singh, A.; Singla, R.; Rohilla, R.; Batra, A.; Mukhopadhyay, R. Long term results after surgical management of posterior wall acetabular fractures. J. Orthop. Traumatol. 2014, 15, 173–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauffrey, C.; Hao, J.; Cuellar, D.O.; Herbert, B.; Chen, X.; Liu, B.; Zhang, Y.; Smith, W. The epidemiology and injury patterns of acetabular fractures. Are the USA and China comparable? Clin. Orthop. Relat. Res. 2014, 472, 3332–3337. [Google Scholar] [CrossRef] [Green Version]
- Papadakos, N.; Pearce, R.; Bircher, M.D. Low energy fractures of the acetabulum. Ann. R. Coll. Surg. Engl. 2014, 96, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Chen, W.; Su, Y.; Li, Z.; Li, M.; Wu, Z. Thrombotic risk assessment questionary helps increase the use of thromboprophylaxis for patients with pelvic and acetabular fractures. Indian J. Orthop. 2012, 46, 413–419. [Google Scholar] [PubMed]
- Weber, K.; Kohler, H.; Vock, B.; Wentzensen, A. Lebensqualität nach Acetabulum- und Beckenringfrakturen. Orthopäde 2002, 31, 582–586. [Google Scholar] [CrossRef]
- Aprato, A.; Joeris, A.; Tosto, F.; Kalampoki, V.; Stucchi, A.; Masse, A. Direct and indirect costs of surgically treated pelvic fractures. Arch. Orthop. Trauma Surg. 2016, 136, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Holstein, J.H.; Stuby, F.M.; Herath, C.S.; Culemann, U.; Aghayev, E.; Pohlemann, T. Einfluss des Beckenregisters der DGU auf die Versorgung von Beckenringfrakturen. Unfallchirurg 2016, 119, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Culemann, U.; Tosounidis, G.; Pohlemann, T. Aktuelle Behandlungsstrategien nach Azetabulumfrakturen. Z. Orthopädie Unf. 2009, 4, 229–248. [Google Scholar] [CrossRef]
- Moliere, S.; Dosch, J.C.; Bierry, G. Pelvic, acetabular and hip fractures: What the surgeon should expect from the radiologist. Diagn. Interv. Imaging 2016, 97, 709–723. [Google Scholar] [CrossRef]
- McMaster, J.; Powell, J. Acetabular fractures. Curr. Orthop. 2005, 19, 140–154. [Google Scholar] [CrossRef]
- Hessmann, M.H.; Ingelfinger, P.; Dietz, S.O.; Rommens, P.M. Osteosynthese der Frakturen der Vorderwand und des vorderen Pfeilers des Azetabulums über einen ilioinguinalen Zugang. Oper. Orthop. Traumatol. 2009, 21, 236–250. [Google Scholar] [CrossRef]
- Quadir, R.I.; Bukhari, S.I. Outcome of operative treatment of acetabular fractures: Short term follow-up. J. Ayub Med. Coll. Abbottabad 2015, 27, 287–291. [Google Scholar]
- Missaoui, B.; Portero, P.; Bendaya, S.; Hanktie, O.; Thoumie, P. Posture and equilibrium in orthopedic and rheumatologic diseases. Neurophysiol. Clin. 2008, 38, 447–457. [Google Scholar] [CrossRef]
- Sziver, E.; Nagya, E.; Preszner-Domján, A.; Pósa, G.; Horvath, G.; Balog, A.; Tóth, K. Postural control in degenerative diseases of the hip joint. Clin. Biomech. 2016, 35, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Arokoski, J.P.A.; Leinonen, V.; Arokoski, M.H.; Aalto, H.; Valtonen, H. Postural control in male patients with hip osteoarthritis. Gait Posture 2006, 23, 45–50. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Nikolau, V.S.; Kheir, E.; Mehta, S.; Stengel, D.; Roberts, C.S. Factors determining quality of life and level of sporting activity after internal fixation of an isolated acetabular fracture. J. Bone Jt. Surg. 2009, 91, 1354–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, P.; Schnegelberger, A.; Riesner, H.J.; Stuby, F.; Friemert, B.; Palm, H.G. Einfluss von operativ versorgten Beckenring- und Azetabulumfrakturen auf die posturale Kontrolle. Z. Orthop. Unf. 2016, 154, 174–180. [Google Scholar] [CrossRef]
- Judet, R.; Judet, J.; Letournel, E. Fractures of the acetabulum: Classification and surgical approaches for open reduction. Preliminary report. J. Bone Jt. Surg. Am. 1964, 46, 1615–1646. [Google Scholar] [CrossRef]
- Harris, W.H. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J. Bone Jt. Surg. Am. 1969, 51, 737–755. [Google Scholar] [CrossRef]
- D’Aubigne, R.M.; Postel, M. The Classic: Functional results of hip arthroplasty with acrylic prosthesis. Clin. Orthop. Relat. Res. 2009, 467, 7–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triantaphillopoulos, P.G.; Panagiotopoulos, E.C.; Mousafiris, C.; Tyllianakis, M.; Dimakopoulos, P.; Lambiris, E.E. Long-term results in surgically treated acetabular fractures through the posterior approaches. J. Trauma 2007, 62, 378–382. [Google Scholar] [PubMed]
- Floris, I.; Bodzay, T.; Vendegh, Z.; Gloviczki, B.; Balazs, P. Short-term results of total hip replacement due to acetabular fractures. Eklem Hastalik. Cerrahisi 2013, 24, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Fölsch, C.; Alwani, M.M.; Jurow, V.; Stiletto, R. Operative Therapie der Acetabulumfraktur beim älteren Patienten. Osteosynthese oder Endoprothese. Unfallchirurg 2015, 118, 146–154. [Google Scholar] [CrossRef]
- Matta, J.M. Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J. Bone Jt. Surg. Am. 1996, 78, 1632–1645. [Google Scholar] [CrossRef]
- Maia, M.S.; Santos, D.C.; de Queiroga, D.M.; de Oliveira Castro, C.; Silva, R.M.; Reis, A.C.; Ducatti, A.C. Epidemiological analysis on acetabular fractures. Rev. Bras. Ortop. 2011, 46, 23–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchida, K.; Kokubo, Y.; Yayama, T.; Nakajima, H.; Miyazaki, T.; Negoro, K.; Takeno, K.; Sawaguchi, T.; Watanabe, S.; Sugita, D.; et al. Fracture of the acetabulum: A retrospective review of ninety-one patients treated at a single institution. Eur. J. Orthop. Surg. Traumatol. 2013, 23, 155–163. [Google Scholar] [CrossRef]
- Moed, B.R. A thirty-year perspective on posterior wall fractures of the acetabulum: Enigma or just another intra-articular injury. J. Taibah Univ. Med. Sci. 2016, 11, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Culemann, U.; Tosounidis, G.; Pohlemann, T. Die Therapie bei Azetabulumfrakturen—Aktuelle Diagnostik und Behandlungsstrategie. Zent. Chir. 2005, 130, W58–W71. [Google Scholar] [CrossRef]
- Bahat, N.A.; Kangoo, K.A.; Wani, I.H.; Wali, G.R.; Muzaffar, N.; Dar, R.A. Operative management of displacement acetabular fractures: An institutional experience with a midterm follow-up. Ortop. Traumatol. Rehabil. 2014, 3, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Schlickewei, W.; Kuner, E.H.; Elsässer, B. Langzeitergebnisse und Spätschäden nach Hüftpfannenfrakturen. Orthopäde 1997, 26, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Nusser, M.; Holstiege, J.; Kaluscha, R.; Tepohl, L.; Stuby, F.; Röderer, G.; Krischak, G. Berufliche Wiedereingliederung nach Becken- und Azetabulumfrakturen. Z. Orthop. Unf. 2015, 153, 282–288. [Google Scholar] [CrossRef]
- Ovre, S.; Sandvik, L.; Madse, J.E.; Roise, O. Modification of the Harris hip score in acetabular fracture treatment. Injury 2007, 38, 344–349. [Google Scholar] [CrossRef]
- Kalairajah, Y.; Azurza, K.; Hulme, C.; Molloy, S.; Drabu, K.J. Health outcome measures in the evaluation of total hip arthroplasties—A comparison between the Harris hip score and the Oxford hip score. J. Arthroplast. 2005, 20, 1037–1041. [Google Scholar] [CrossRef]
- Kirmit, L.; Karatosun, V.; Unver, B.; Bakirhan, S.; Sen, A.; Gocen, Z. The reliability of hip scoring systems for total hip arthroplasty candidates: Assessment by physical therapists. Clin. Rehabil. 2005, 19, 659–661. [Google Scholar] [CrossRef]
- Ugino, F.K.; Righetti, C.M.; Alves, D.P.L.; Guimarães, R.P.; Honda, E.K.; Ono, N.K. Evaluation of the reliability of the modified Merle d’Aubigné and Postel Method. Acta Ortop. Bras. 2012, 20, 213–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dindorf, C.; Teufl, W.; Taetz, B.; Becker, S. Feature extraction and gait classification in hip replacement patients on the basis of kinematic waveform data. Biomed. Hum. Kinet. 2021, 13, 177–186. [Google Scholar] [CrossRef]
- Maurer, F.; Mutter, B.; Weise, K.; Belzl, H. Rehabilitation nach Hüftgelenkfrakturen. Orthopäde 1997, 26, 368–374. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group | Type of Fracture | Number (No.) | ∑ |
|---|---|---|---|
| Simple | posterior wall | 9 | 17 |
| posterior column | 3 | ||
| anterior wall | 1 | ||
| anterior column | 2 | ||
| transversal | 2 | ||
| Complex | posterior column and posterior wall | 3 | 14 |
| both columns | 10 | ||
| T-shaped | 1 |
| Scale | Study Population | Functional State—Norms [26,27] | ||||
|---|---|---|---|---|---|---|
| SD | Poor | Fair | Good | Excellent | ||
| HHS [points] | 68.9 | 16.3 | <70 | 70–79 | 80–89 | 90–100 |
| Merle [points] | 12.0 | 2.8 | <13 | 13–14 | 15–17 | 18 |
| Pain—HHS | n |
|---|---|
| None, or ignores it | 3 |
| Slight, occasional, no compromise in activity | 11 |
| Mild pain, no effect on average activities, rarely moderate pain with unusual activity, may take aspirin | 11 |
| Moderate pain, tolerable but makes concessions to pain. Some limitations of ordinary activity or work. May require occasional pain medication stronger than aspirin | 3 |
| Marked pain, serious limitation of activities | 1 |
| Totally disabled, crippled, pain in bed, bedridden | 0 |
| Reduction of Fracture | p ≤ 0.05 * | ||||
|---|---|---|---|---|---|
| Anatomical | Imperfect | ||||
| Scale | SD | SD | p-Value | ||
| HHS (points) | 73.74 | 15.26 | 61.33 | 15.53 | 0.05 * |
| MERLE (points) | 12.95 | 2.50 | 10.58 | 2.81 | 0.03 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dadura, E.; Truszczyńska-Baszak, A.; Szydłowski, D. Radiological and Functional Assessment of Treatment Outcomes in Patients after Open Reduction with Internal Fixation (ORIF) of Acetabular Fractures. Int. J. Environ. Res. Public Health 2022, 19, 1277. https://doi.org/10.3390/ijerph19031277
Dadura E, Truszczyńska-Baszak A, Szydłowski D. Radiological and Functional Assessment of Treatment Outcomes in Patients after Open Reduction with Internal Fixation (ORIF) of Acetabular Fractures. International Journal of Environmental Research and Public Health. 2022; 19(3):1277. https://doi.org/10.3390/ijerph19031277
Chicago/Turabian StyleDadura, Emilia, Aleksandra Truszczyńska-Baszak, and Dariusz Szydłowski. 2022. "Radiological and Functional Assessment of Treatment Outcomes in Patients after Open Reduction with Internal Fixation (ORIF) of Acetabular Fractures" International Journal of Environmental Research and Public Health 19, no. 3: 1277. https://doi.org/10.3390/ijerph19031277