
Cardiovascular System during SARS-CoV-2 Infection


Abstract
:1. Introduction
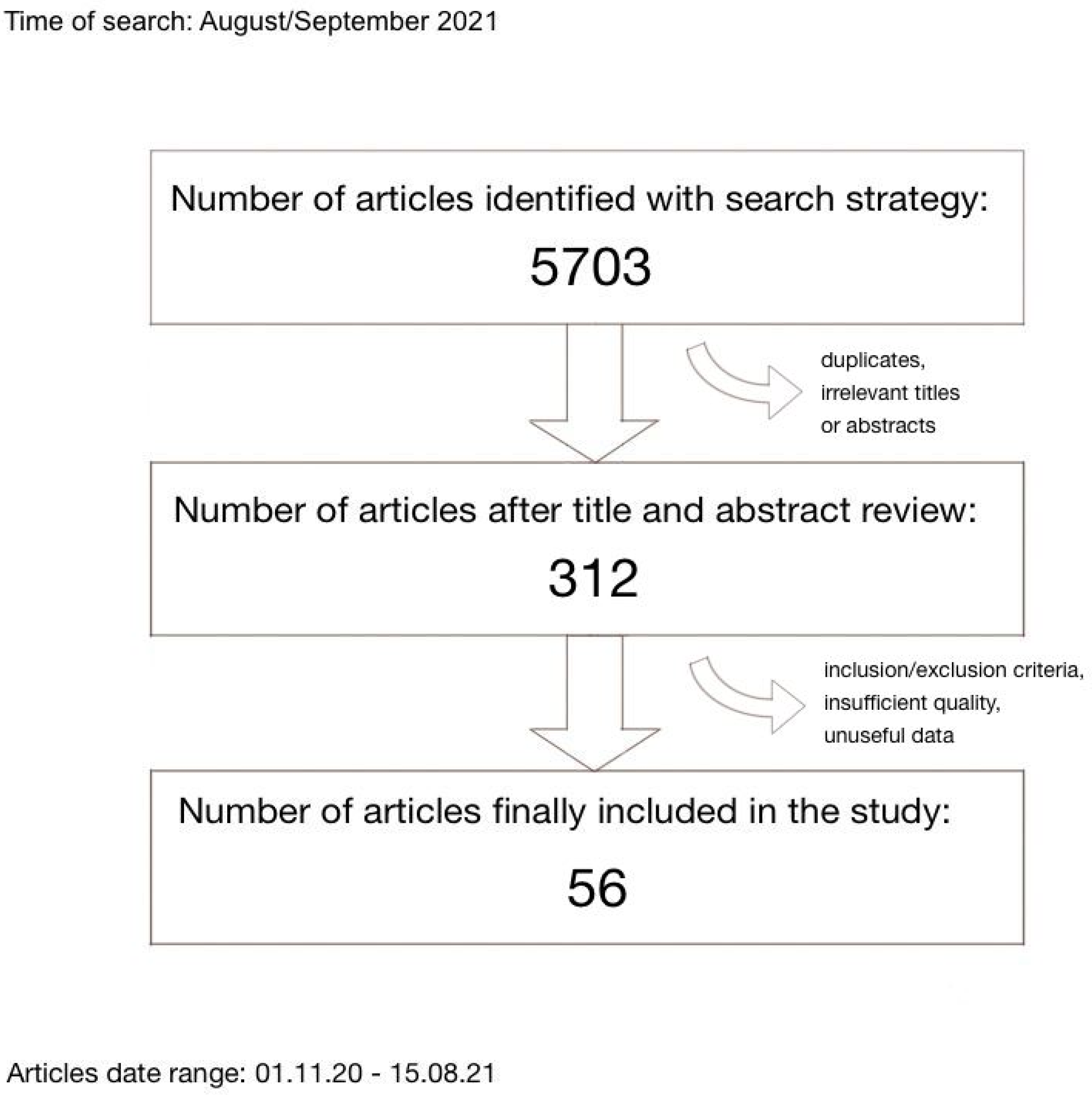
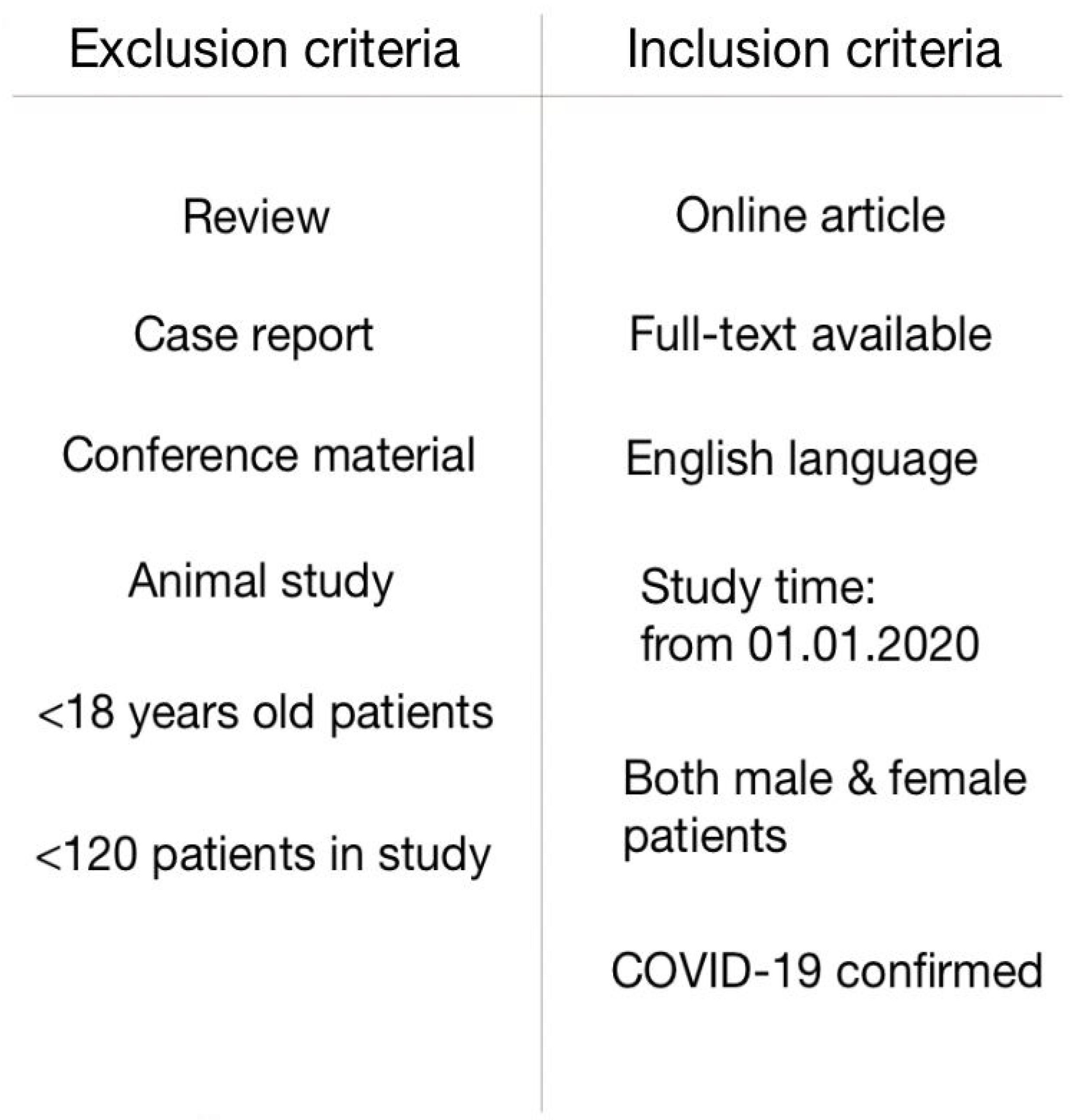
2. Materials and Methods
3. Results
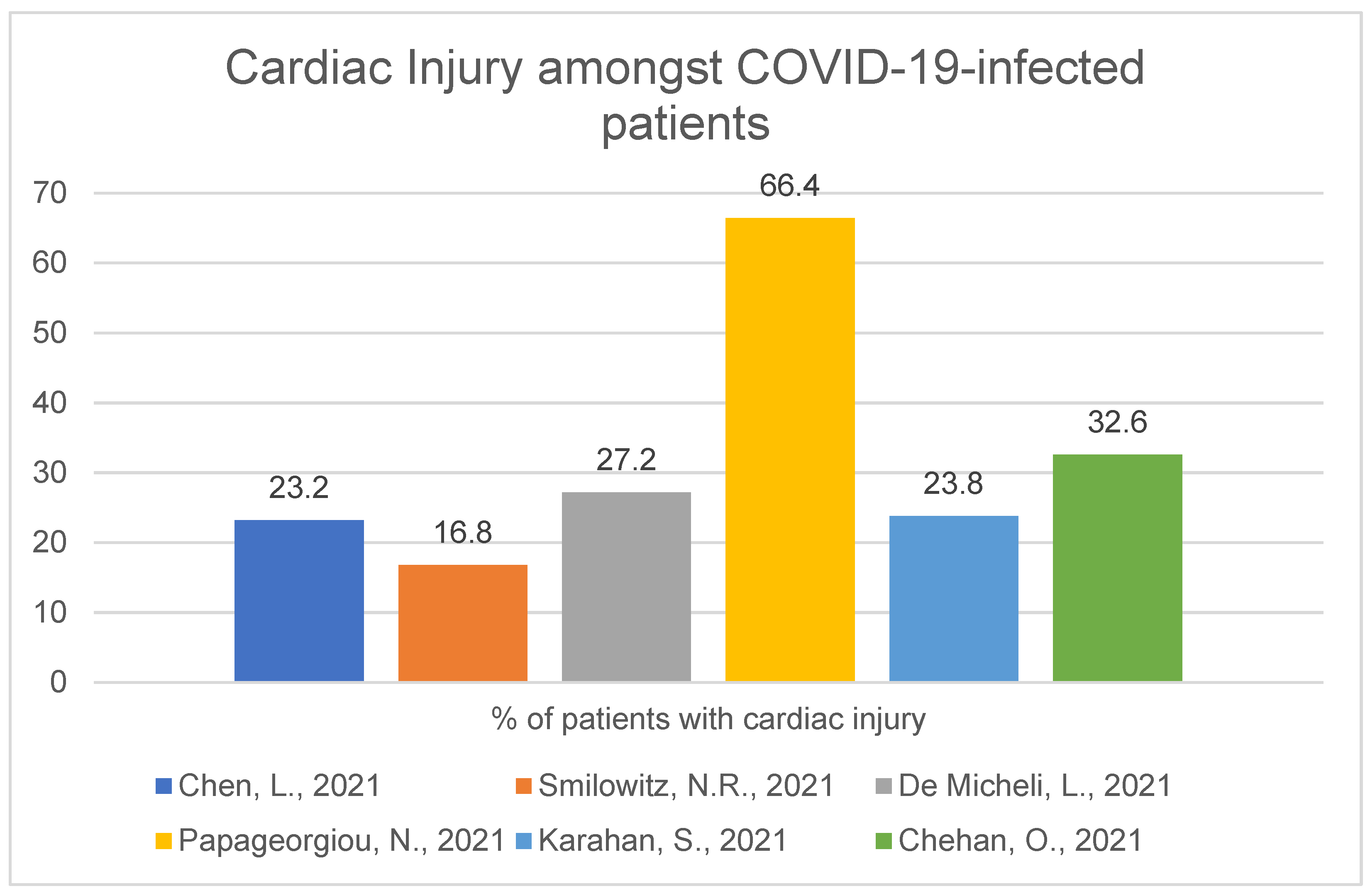
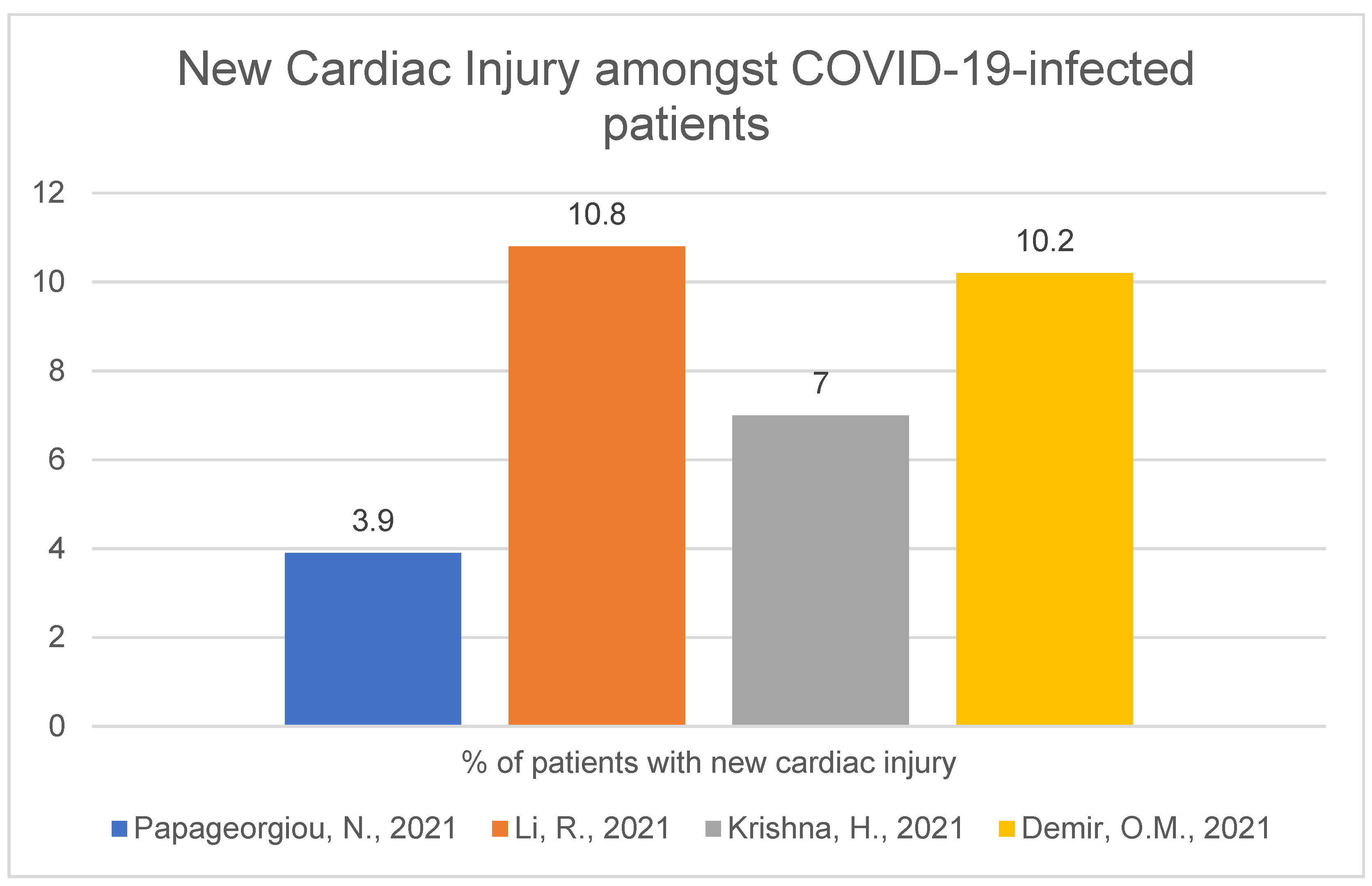
3.1. Cardiac Injury
3.1.1. Frequency and Characteristic
3.1.2. Hospitalisation and Outcome
3.1.3. Myocardial Infarction
3.1.4. Comparison of the Situation before COVID-19 Pandemic and Now
3.1.5. Myocarditis
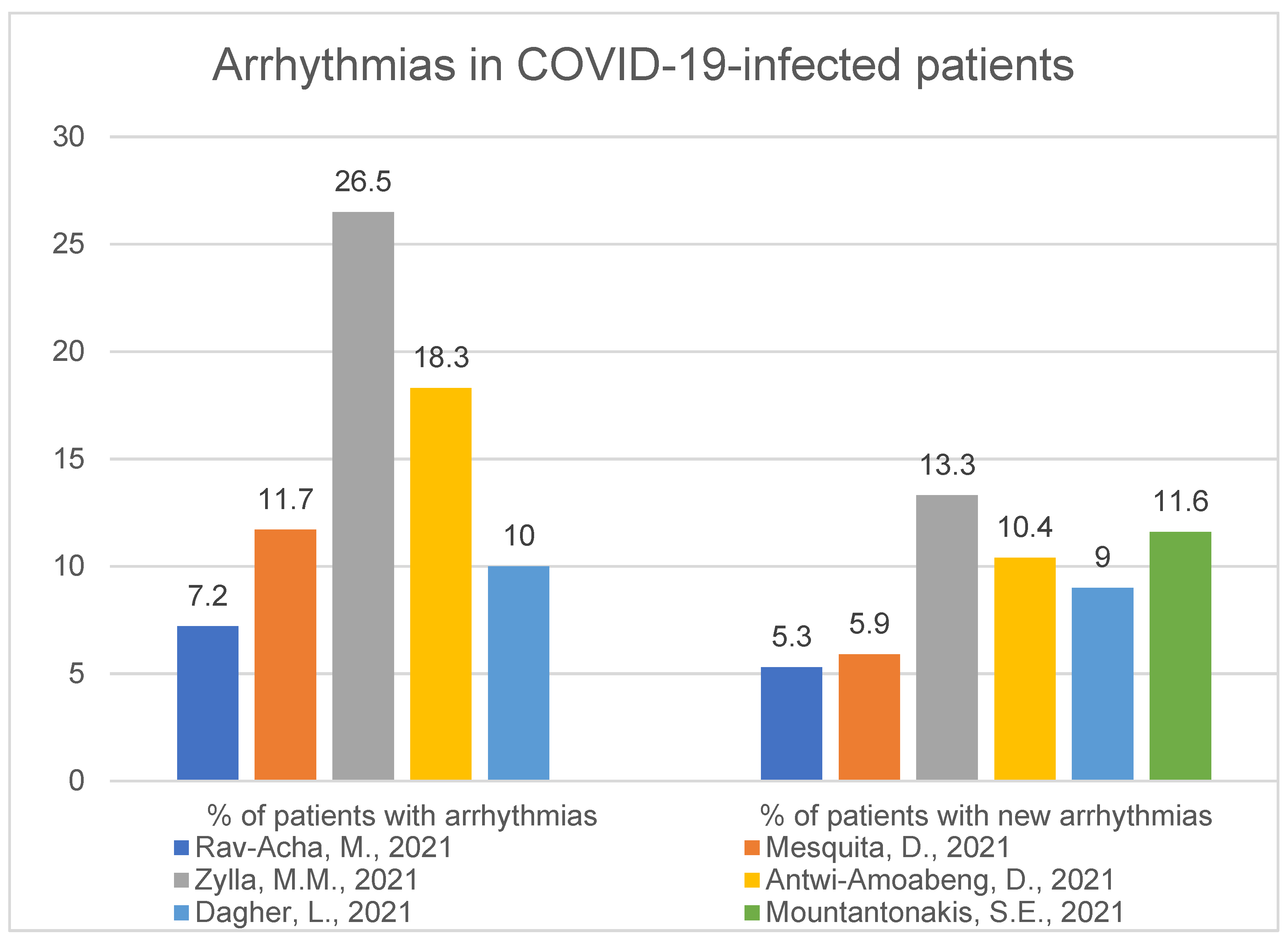
3.2. Arrhythmias
3.2.1. Frequency and Characteristic
3.2.2. Hospitalisation and Outcome
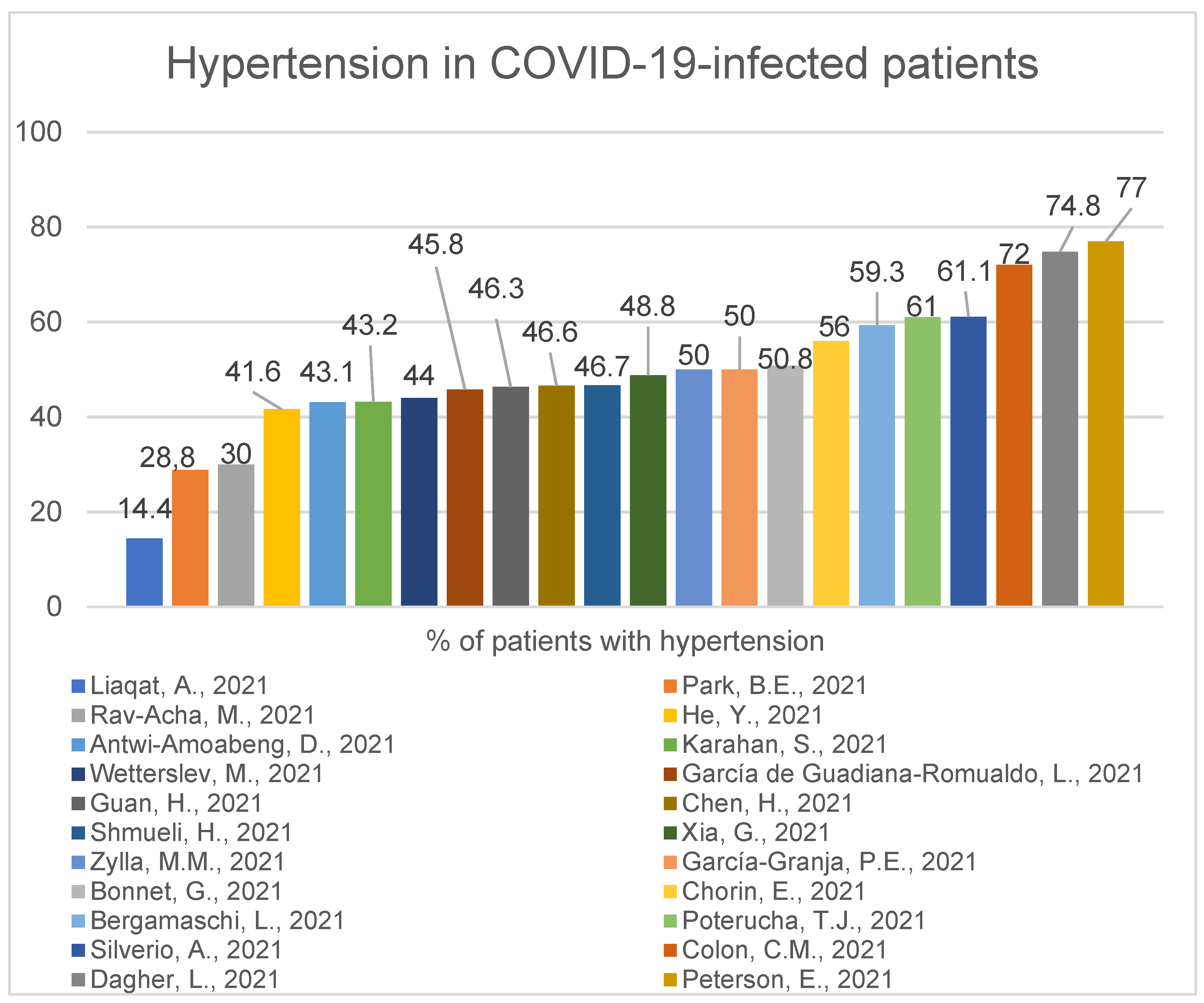
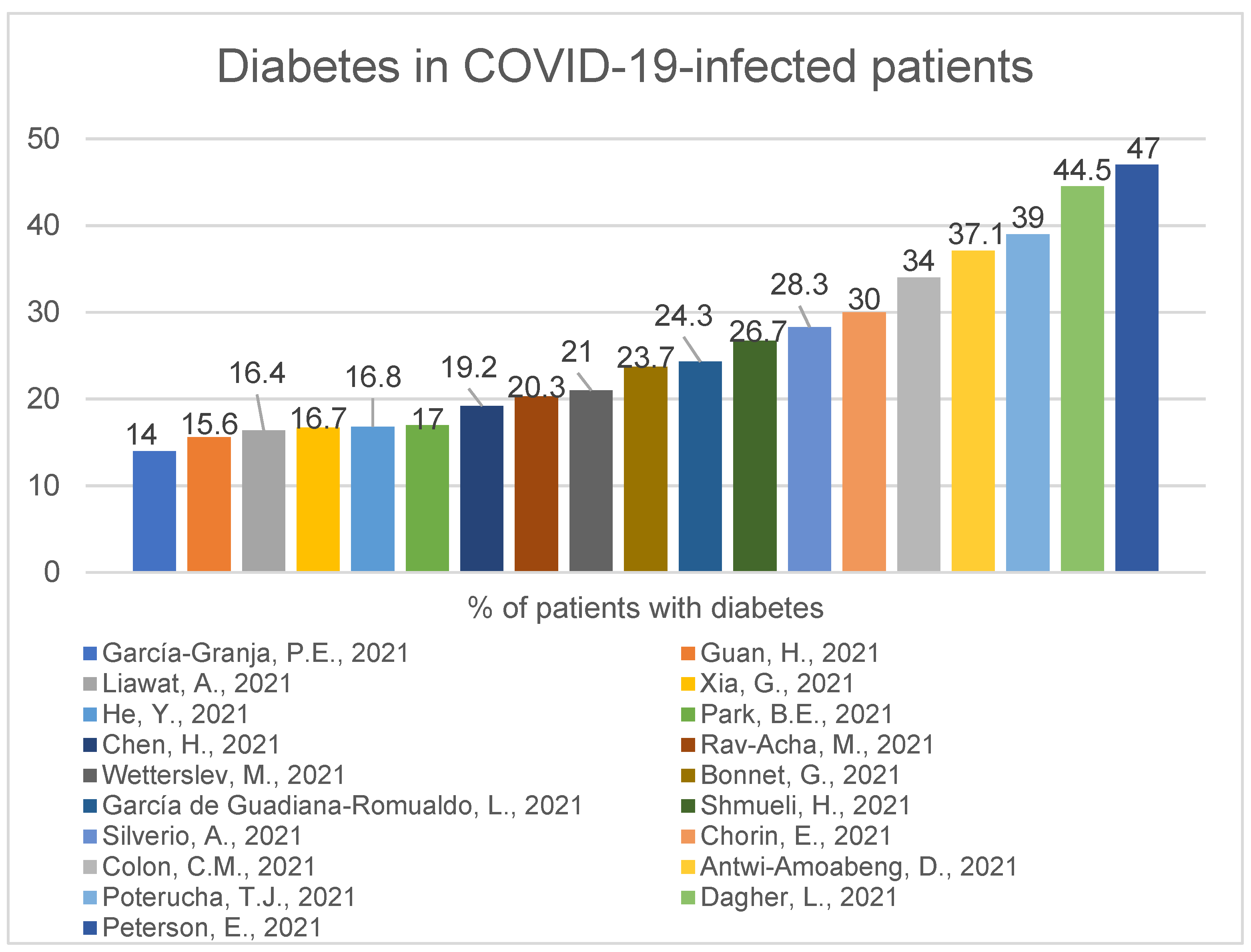
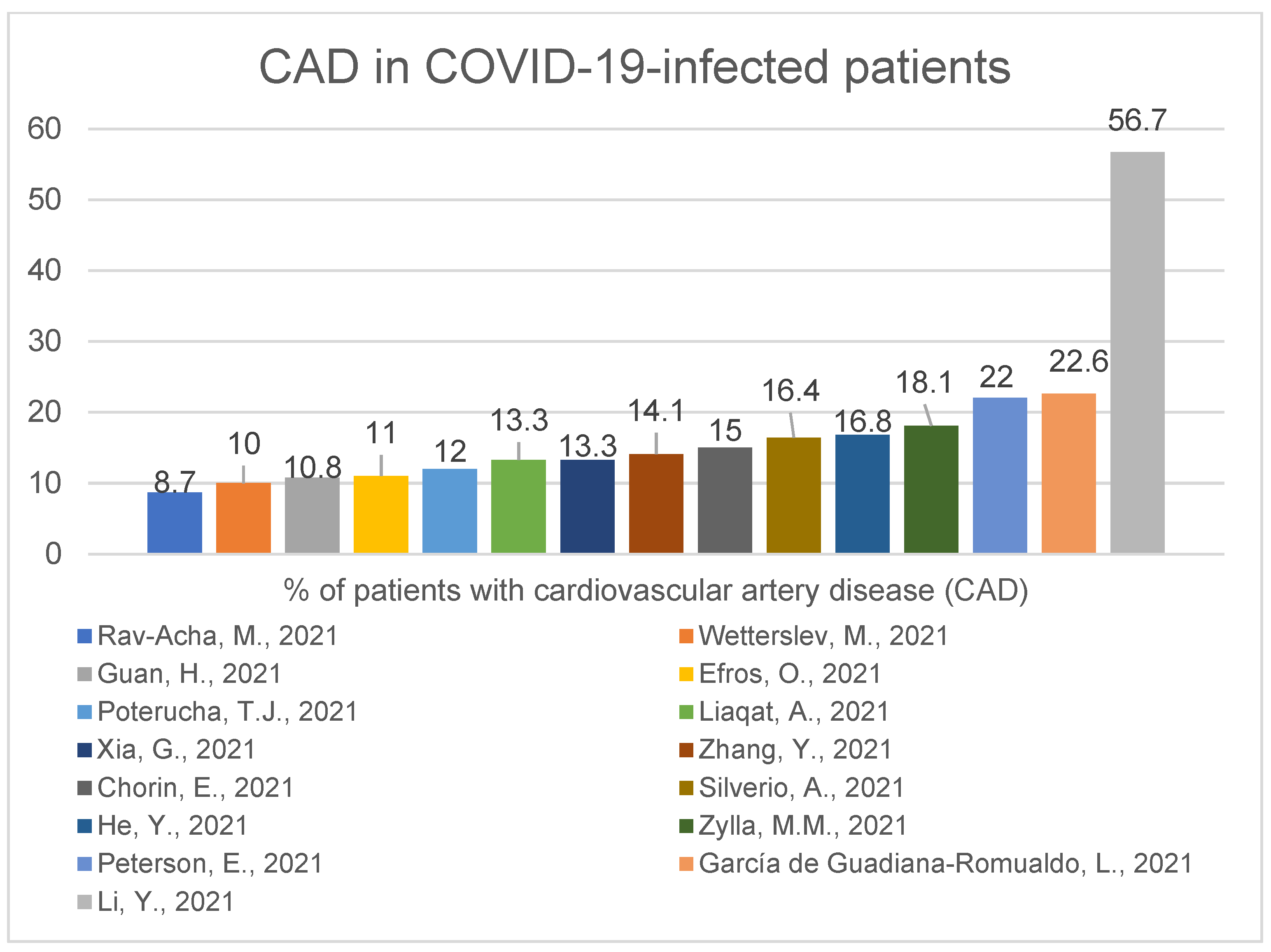
3.3. Accompanying Comorbidities
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative. Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: An international cohort study. Lancet 2020, 396, 27–38. [Google Scholar] [CrossRef]
- Whittaker, A.; Anson, M.; Harky, A. Neurological Manifestations of COVID-19: A systematic review and current update. Acta Neurol. Scand. 2020, 142, 14–22. [Google Scholar] [CrossRef]
- Maury, A.; Lyoubi, A.; Peiffer-Smadja, N.; de Broucker, T.; Meppiel, E. Neurological manifestations associated with SARS-CoV-2 and other coronaviruses: A narrative review for clinicians. Rev. Neurol. 2021, 177, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Epidemiology Working Group for NCIP Epidemic Response; Chinese Centre for Disease Control and Prevention. The epidemio logical characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 145–151. [Google Scholar]
- Chen, L.; Hu, W.; Guo, X.; Zhao, P.; Tang, J.; Gu, Y.; Huang, N.; Wang, C.; Cui, A.; Zhang, D.; et al. Association of coagulation dysfunction with cardiac injury among hospitalized patients with COVID-19. Sci. Rep. 2021, 11, 4432. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Nguy, V.; Aphinyanaphongs, Y.; Newman, J.D.; Xia, Y.; Reynolds, H.R.; Hochman, J.S.; Fishman, G.I.; Berger, J.S. Multiple Biomarker Approach to Risk Stratification in COVID-19. Circulation 2021, 143, 1338–1340. [Google Scholar] [CrossRef]
- De Michieli, L.; Babuin, L.; Vigolo, S.; De Marinis, G.B.; Lunardon, A.; Favretto, F.; Lobo, R.; Sandoval, Y.; Bryant, S.C.; Donato, D.; et al. Using high sensitivity cardiac troponin values in patients with SARS-CoV-2 infection (COVID-19): The Padova experience. Clin Biochem. 2021, 90, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, N.; Sohrabi, C.; Merino, D.P.; Tyrlis, A.; Atieh, A.E.; Saberwal, B.; Lim, W.-Y.; Creta, A.; Khanji, M.; Rusinova, R.; et al. High sensitivity troponin and COVID-19 outcomes. Acta Cardiol. 2021, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Karahan, S.; Katkat, F.; Ozcan, S.; Sahin, I.; Okuyan, E. Impact of acute myocardial injury on prognosis in patients with COVID-19. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 2425–2434. [Google Scholar] [PubMed]
- Chehab, O.; El Zein, S.; Kanj, A.; Moghrabi, A.; Sebastian, J.; Halboni, A.; Alkassis, S.; El-Hor, N.; Briasoulis, A.; Liberman, R.; et al. SARS-CoV-2 Viral Load and Cardiac Injury are Independent and Incremental Predictors of Adverse Outcome. Mayo Clin. Proc. Innov. Qual. Outcomes 2021, 5, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Liaqat, A.; Ali-Khan, R.S.; Asad, M.; Rafique, Z. Evaluation of myocardial injury patterns and ST changes among critical and non-critical patients with coronavirus-19 disease. Sci Rep. 2021, 11, 4828. [Google Scholar] [CrossRef]
- Xia, G.; Fan, D.; Ma, C.; He, Y.; Wang, M.; Zhu, Y.; Zheng, Q. Hyper-Inflammatory Response Involves in Cardiac Injury Among Patients With Coronavirus Disease 2019. Am. J. Med. Sci. 2021, 361, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Metkus, T.S.; Sokoll, L.J.; Barth, A.S.; Czarny, M.J.; Hays, A.G.; Lowenstein, C.J.; Michos, E.D.; Nolley, E.P.; Post, W.S.; Resar, J.R.; et al. Myocardial Injury in Severe COVID-19 Compared with Non-COVID-19 Acute Respiratory Distress Syndrome. Circulation 2021, 143, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, G.; Weizman, O.; Trimaille, A.; Pommier, T.; Cellier, J.; Geneste, L.; Panagides, V.; Marsou, W.; Deney, A.; Attou, S.; et al. Characteristics and outcomes of patients hospitalized for COVID-19 in France: The Critical COVID-19 France (CCF) study. Arch. Cardiovasc. Dis. 2021, 114, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Wang, H.; Ma, F.; Cui, G.-L.; Peng, L.-Y.; Li, C.-Z.; Zeng, H.-S.; Marian, A.J.; Wang, D.-W. Widespread myocardial dysfunction in COVID-19 patients detected by myocardial strain imaging using 2-D speckle-tracking echocardiography. Acta Pharmacol. Sin. 2021, 28, 1–8. [Google Scholar] [CrossRef]
- Krishna, H.; Ryu, A.J.; Scott, C.G.; Mandale, D.R.; Naqvi, T.Z.; Pellikka, P.A. Cardiac Abnormalities in COVID-19 and Relationship to Outcome. Mayo Clin. Proc. 2021, 96, 932–942. [Google Scholar] [CrossRef] [PubMed]
- Demir, O.M.; Ryan, M.; Cirillo, C.; Desai, N.; Pericao, A.; Sinclair, H.; Stylianidis, V.; Victor, K.; Alaour, B.; Jones, A.; et al. Impact and Determinants of High-Sensitivity Cardiac Troponin-T Concentration in Patients with COVID-19 Admitted to Critical Care. Am. J. Cardiol. 2021, 147, 129–136. [Google Scholar] [CrossRef]
- Hendrickson, B.S.; Stephens, R.E.; Chang, J.V.; Amburn, J.M.; Pierotti, L.L.; Johnson, J.L.; Hyden, J.C.; Johnson, J.N.; Philip, R.R. Cardiovascular Evaluation After COVID-19 in 137 Collegiate Athletes: Results of an Algorithm-Guided Screening. Circulation 2021, 143, 1926–1928. [Google Scholar] [CrossRef]
- Xie, Y.; Wang, L.; Li, M.; Li, H.; Zhu, S.; Wang, B.; He, L.; Zhang, D.; Zhang, Y.; Yuan, H.; et al. Biventricular Longitudinal Strain Predict Mortality in COVID-19 Patients. Front. Cardiovasc. Med. 2021, 7, 632434. [Google Scholar] [CrossRef]
- He, J.; Zhang, B.; Zhou, Q.; Yang, W.; Xu, J.; Liu, T.; Zhang, H.; Wu, Z.; Li, D.; Zhou, Q.; et al. The Prognostic Value of Myocardial Injury in COVID-19 Patients and Associated Characteristics. Immun. Inflamm. Dis. 2021, 9, 1358–1369. [Google Scholar] [CrossRef]
- Zhang, Y.; Sun, W.; Wu, C.; Zhang, Y.; Cui, L.; Xie, Y.; Wang, B.; He, L.; Yuan, H.; Zhang, Y.; et al. Prognostic Value of Right Ventricular Ejection Fraction Assessed by 3D Echocardiography in COVID-19 Patients. Front. Cardiovasc. Med. 2021, 8, 641088. [Google Scholar] [CrossRef]
- Silverio, A.; Di Maio, M.; Scudiero, F.; Russo, V.; Esposito, L.; Attena, E.; Pezzullo, S.; Parodi, G.; D’Andrea, A.; Damato, A.; et al. Clinical conditions and echocardiographic parameters associated with mortality in COVID-19. Eur. J. Clin. Investig. 2021, 51, e13638. [Google Scholar] [CrossRef]
- Zhou, Z.; Ryan, J.; Ernst, M.E.; Zoungas, S.; Tonkin, A.M.; Woods, R.L.; McNeil, J.J.; Reid, C.M.; Curtis, A.J.; Wolfe, R.; et al. Effect of Statin Therapy on Cognitive Decline and Incident Dementia in Older Adults. J. Am. Coll. Cardiol. 2021, 77, 3145–3156. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Wang, W.-J.; Yu, H.; Xu, J.; Wu, H.; Wang, C.; Gu, C.-H.; Li, H.-J.; Li, M.; Liu, C.; et al. Pre-existing Health Conditions and Epicardial Adipose Tissue Volume: Potential Risk Factors for Myocardial Injury in COVID-19 Patients. Front. Cardiovasc. Med. 2021, 7, 585220. [Google Scholar]
- Chen, H.; Li, X.; Marmar, T.; Xu, Q.; Tu, J.; Li, T.; Han, J.; Xu, D.; Shen, T. Cardiac Troponin I association with critical illness and death risk in 726 seriously ill COVID-19 patients: A retrospective cohort study. Int. J. Med. Sci. 2021, 18, 1474–1483. [Google Scholar] [CrossRef] [PubMed]
- García de Guadiana-Romualdo, L.; Morell-García, D.; Morales-Indiano, C.; Bauça, J.M.; José Alcaide Martín, M.; Del Valle, C.E.; Gutiérrez Revilla, J.I.; Urrechaga, E.; Álamo, J.M.; Hernando Holgado, A.M.; et al. Characteristics and laboratory findings on admission to the emergency department among 2873 hospitalized patients with COVID-19: The impact of adjusted laboratory tests in multicenter studies. A multicenter study in Spain (BIOCOVID-Spain study). Scand. J. Clin. Lab. Investig. 2021, 81, 187–193. [Google Scholar] [CrossRef]
- Wang, Y.; Shu, H.; Liu, H.; Li, X.; Zhou, X.; Zou, X.; Pan, S.; Xu, J.; Xu, D.; Zhao, X.; et al. The peak levels of highly sensitive troponin I predicts in-hospital mortality in COVID-19 patients with cardiac injury: A retrospective study. Eur. Heart J. Acute Cardiovasc. Care. 2021, 10, 6–15. [Google Scholar] [CrossRef]
- He, Y.; Zheng, X.; Li, X.; Jiang, X. Key factors leading to fatal outcomes in COVID-19 patients with cardiac injury. Sci. Rep. 2021, 11, 4144. [Google Scholar] [CrossRef]
- Peiró, Ó.M.; Carrasquer, A.; Sánchez-Gimenez, R.; Lal-Trehan, N.; Del-Moral-Ronda, V.; Bonet, G.; Fort-Gallifa, I.; Picó-Plana, E.; Bastón-Paz, N.; Gutiérrez, C.; et al. Biomarkers and short-term prognosis in COVID-19. Biomarkers 2021, 26, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Efros, O.; Barda, N.; Meisel, E.; Leibowitz, A.; Fardman, A.; Rahav, G.; Klempfner, R.; Grossmanet, E. Myocardial injury in hospitalized patients with COVID-19 infection-Risk factors and outcomes. PLoS ONE 2021, 16, e0247800. [Google Scholar] [CrossRef] [PubMed]
- Poterucha, T.J.; Elias, P.; Jain, S.S.; Sayer, G.; Redfors, B.; Burkhoff, D.; Rosenblum, H.; DeFilippis, E.M.; Gupta, A.; Lawlor, M.; et al. Admission Cardiac Diagnostic Testing with Electrocardiography and Troponin Measurement Prognosticates Increased 30-Day Mortality in COVID-19. J. Am. Heart Assoc. 2021, 10, e018476. [Google Scholar] [CrossRef] [PubMed]
- Briscoe, M.; Sykes, R.; Krystofiak, T.; Peck, O.; Mangion, K.; Berry, C. Clinical significance of coronavirus disease 2019 in hospitalized patients with myocardial injury. Clin. Cardiol. 2021, 44, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Primessnig, U.; Pieske, B.M.; Sherif, M. Increased mortality and worse cardiac outcome of acute myocardial infarction during the early COVID-19 pandemic. ESC Heart Fail. 2021, 8, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Salinas, P.; Travieso, A.; Vergara-Uzcategui, C.; Tirado-Conte, G.; Macaya, F.; Mejía-Rentería, H.; Nombela-Franco, L.; Núñez-Gil, I.J.; Gonzalo, N.; Jiménez-Quevedo, P.; et al. Clinical Profile and 30-Day Mortality of Invasively Managed Patients with Suspected Acute Coronary Syndrome During the COVID-19 Outbreak. Int. Heart J. 2021, 62, 274–281. [Google Scholar] [CrossRef]
- Kitahara, S.; Fujino, M.; Honda, S.; Asaumi, Y.; Kataoka, Y.; Otsuka, F.; Nakanishi, M.; Tahara, Y.; Ogata, S.; Onozuka, D.; et al. COVID-19 pandemic is associated with mechanical complications in patients with ST-elevation myocardial infarction. Open Heart 2021, 8, e001497. [Google Scholar] [CrossRef]
- Laganà, N.; Cei, M.; Evangelista, I.; Cerutti, S.; Colombo, A.; Conte, L.; Mormina, E.; Rotiroti, G.; Giovanni Versace, A.; Porta, C.; et al. Suspected myocarditis in patients with COVID-19: A multicenter case series. Medicine 2021, 100, e24552. [Google Scholar] [CrossRef]
- Kotecha, T.; Knight, D.S.; Razvi, Y.; Kumar, K.; Vimalesvaran, K.; Thornton, G.; Patel, R.; Chacko, L.; Brown, J.T.; Coyle, C.; et al. Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur. Heart J. 2021, 42, 1866–1878. [Google Scholar] [CrossRef]
- Martinez, M.W.; Tucker, A.M.; Bloom, O.J.; Green, G.; DiFiori, J.P.; Solomon, G.; Phelan, D.; Kim, J.H.; Meeuwisse, W.; Sills, A.K.; et al. Prevalence of Inflammatory Heart Disease Among Professional Athletes with Prior COVID-19 Infection Who Received Systematic Return-to-Play Cardiac Screening. JAMA Cardiol. 2021, 6, 745–752. [Google Scholar] [CrossRef]
- Clark, D.E.; Parikh, A.; Dendy, J.M.; Diamond, A.B.; George-Durrett, K.; Fish, F.A.; Slaughter, J.C.; Fitch, W.; Hughes, S.G.; Soslowet, J.H.; et al. COVID-19 Myocardial Pathology Evaluation in Athletes with Cardiac Magnetic Resonance (COMPETE CMR). Circulation 2021, 143, 609–612. [Google Scholar] [CrossRef]
- Rav-Acha, M.; Orlev, A.; Itzhaki, I.; Zimmerman, S.F.; Fteiha, B.; Bohm, D.; Kurd, R.; Samuel, T.Y.; Asher, E.; Helviz, Y.; et al. Cardiac arrhythmias amongst hospitalised Coronavirus 2019 (COVID-19) patients: Prevalence, characterisation, and clinical algorithm to classify arrhythmic risk. Int. J. Clin. Pract. 2021, 75, e13788. [Google Scholar] [CrossRef]
- Mesquita, D.; Carmo, P.; Cabanelas, N.; Santos, N.; Martins, V.; Sanfins, V.; Costa, H.C.; Fontes, J.P.; Fonseca, P.; Parreira, L.; et al. Cardiac arrhythmias in patients presenting with COVID-19 treated in Portuguese hospitals: A national registry from the Portuguese Association of Arrhythmology, Pacing and Electrophysiology. Rev. Port. Cardiol. 2021, 40, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Zylla, M.M.; Merle, U.; Vey, J.A.; Korosoglou, G.; Hofmann, E.; Müller, M.; Herth, F.; Schmidt, W.; Blessing, E.; Göggelmann, C.; et al. Predictors and Prognostic Implications of Cardiac Arrhythmias in Patients Hospitalized for COVID-19. J. Clin. Med. 2021, 10, 133. [Google Scholar] [CrossRef] [PubMed]
- Antwi-Amoabeng, D.; Beutler, B.D.; Singh, S.; Taha, M.; Ghuman, J.; Hanfy, A.; Manasewitsch, N.T.; Ulanja, M.B.; Ghuman, J.; Awad, M.; et al. Association between electrocardiographic features and mortality in COVID-19 patients. Ann. Noninvasive Electrocardiol. 2021, 26, e12833. [Google Scholar] [CrossRef]
- Dagher, L.; Shi, H.; Zhao, Y.; Wetherbie, A.; Johnsen, E.; Sangani, D.; Nedunchezhian, S.; Brown, M.; Miller, P.; Denson, J.; et al. New-onset atrial arrhythmias associated with mortality in black and white patients hospitalized with COVID-19. Pacing Clin. Electrophysiol. 2021, 44, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Northwell COVID-19 Research Consortium; Mountantonakis, S.E.; Saleh, M.; Fishbein, J.; Gandomi, A.; Lesser, M.; Chelico, J.; Gabriels, J.; Qiu, M.; Epstein, L.M. Atrial fibrillation is an independent predictor for in-hospital mortality in patients admitted with SARS-CoV-2 infection. Heart Rhythm 2021, 18, 501–507. [Google Scholar] [CrossRef]
- Yarmohammadi, H.; Morrow, J.P.; Dizon, J.; Biviano, A.; Ehlert, F.; Saluja, D.; Waase, M.; Elias, P.; Poterucha, T.J.; Berman, J.; et al. Frequency of Atrial Arrhythmia in Hospitalized Patients With COVID-19. Am. J. Cardiol. 2021, 147, 52–57. [Google Scholar] [CrossRef]
- García-Granja, P.E.; Veras, C.; Aparisi, Á.; Amat Santos, I.J.; Catalá, P.; Marcos, M.; Cabezón, G.; Candela, J.; Gil, J.F.; Uribarri, A.; et al. Atrial fibrillation in patients with SARS-CoV-2 infection. Med. Clin. 2021, 157, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Wetterslev, M.; Jacobsen, P.K.; Hassager, C.; Jøns, C.; Risum, N.; Pehrson, S.; Bastiansen, A.; Andreasen, A.S.; Kristiansen, K.T.; Bestle, M.H.; et al. Cardiac arrhythmias in critically ill patients with coronavirus disease 2019: A retrospective population-based cohort study. Acta Anaesthesiol. Scand. 2021, 65, 770–777. [Google Scholar] [CrossRef]
- Pardo Sanz, A.; Salido Tahoces, L.; Ortega Pérez, R.; González Ferrer, E.; Sánchez Recalde, A.; Zamorano Gómez, J.L. New-onset atrial fibrillation during COVID-19 infection predicts poor prognosis. Cardiol. J. 2021, 28, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Guan, H.; Liu, J.; Ding, J.; Liu, W.; Feng, Y.; Bao, Y.; Li, H.; Wang, X.; Zhou, Z.; Chen, Z. Arrhythmias in patients with coronavirus disease 2019 (COVID-19) in Wuhan, China: Incidences and implications. J. Electrocardiol. 2021, 65, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Bergamaschi, L.; D’Angelo, E.C.; Paolisso, P.; Toniolo, S.; Fabrizio, M.; Angeli, F.; Donati, F.; Magnani, I.; Rinaldi, A.; Bartoli, L.; et al. The value of ECG changes in risk stratification of COVID-19 patients. Ann. Noninvasive Electrocardiol. 2021, 26, e12815. [Google Scholar] [CrossRef]
- Han, K.-Y.; Qiao, Q.; Zhu, Y.-Q.; Chen, X.-G.; Kang, X.-X.; Zhang, G.-F.; Cai, X.-C.; Du, Y.; Jin, J.; Di, R.-M.; et al. Atrial Arrhythmias in Patients with Severe COVID-19. Cardiol. Res. Pract. 2021, 2021, 8874450. [Google Scholar] [CrossRef] [PubMed]
- Park, B.E.; Lee, J.H.; Park, H.K.; Kim, H.N.; Jang, S.Y.; Bae, M.H.; Yang, D.H.; Park, H.S.; Cho, Y.; Lee, B.Y.; et al. Impact of Cardiovascular Risk Factors and Cardiovascular Diseases on Outcomes in Patients Hospitalized with COVID-19 in Daegu Metropolitan City. J. Korean Med. Sci. 2021, 36, e15. [Google Scholar] [CrossRef] [PubMed]
- Peterson, E.; Lo, K.B.; DeJoy, R.; Salacup, G.; Pelayo, J.; Bhargav, R.; Gul, F.; Albano, J.; Azmaiparashvili, Z.; Amanullah, A.; et al. The relationship between coronary artery disease and clinical outcomes in COVID-19: A single-center retrospective analysis. Coron. Artery Dis. 2021, 32, 367–371. [Google Scholar] [CrossRef]
- Bhatt, A.S.; Jering, K.S.; Vaduganathan, M.; Claggett, B.L.; Cunningham, J.W.; Rosenthal, N.; Signorovitch, J.; Thune, J.J.; Vardeny, O.; Solomon, S.D. Clinical Outcomes in Patients with Heart Failure Hospitalized with COVID-19. JACC Heart Fail. 2021, 9, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Fang, L.; Zhu, S.; Xie, Y.; Wang, B.; He, L.; Zhang, D.; Zhang, Y.; Yuan, H.; Wu, C.; et al. Echocardiographic Characteristics and Outcome in Patients With COVID-19 Infection and Underlying Cardiovascular Disease. Front. Cardiovasc. Med. 2021, 8, 642973. [Google Scholar] [CrossRef]
- Tuo, H.; Li, W.; Tang, L.; He, B.; Yao, B.; Mao, P.; Tang, Q. Cardiac Biomarker Abnormalities Are Closely Related to Prognosis in Patients with COVID-19. Int. Heart J. 2021, 62, 148–152. [Google Scholar] [CrossRef]
- Chorin, E.; Dai, M.; Kogan, E.; Wadhwani, L.; Shulman, E.; Nadeau-Routhier, C.; Knotts, R.; Bar-Cohen, R.; Barbhaiya, C.; Aizer, A.; et al. Electrocardiographic Risk Stratification in COVID-19 Patients. Front. Cardiovasc. Med. 2021, 8, 636073. [Google Scholar] [CrossRef]
- Shmueli, H.; Shah, M.; Ebinger, J.E.; Nguyen, L.C.; Chernomordik, F.; Flint, N.; Botting, P.; Siegel, R.J. Left ventricular global longitudinal strain in identifying subclinical myocardial dysfunction among patients hospitalized with COVID-19. Int. J. Cardiol. Heart Vasc. 2021, 32, 100719. [Google Scholar] [CrossRef]
- Colon, C.M.; Barrios, J.G.; Chiles, J.W.; Brown, T.M.; Pogwizd, S.M.; McElwee, S.K.; Gandotra, S.; Russell, D.W.; McElderry, H.T.; Maddox, W.R. Atrial arrhythmia related outcomes in critically ill COVID-19 patients. Pacing Clin. Electrophysiol. 2021, 44, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Seeherman, S.; Suzuki, Y.J. Viral Infection and Cardiovascular Disease: Implications for the Molecular Basis of COVID-19 Pathogenesis. Int. J. Mol. Sci. 2021, 22, 1659. [Google Scholar] [CrossRef] [PubMed]
- Kuźma, Ł.; Wańha, W.; Kralisz, P.; Kazmierski, M.; Bachórzewska-Gajewska, H.; Wojakowski, W.; Dobrzycki, S. Impact of short-term air pollution exposure on acute coronary syndrome in two cohorts of industrial and non-industrial areas: A time series regression with 6,000,000 person-years of follow-up (ACS—Air Pollution Study). Environ. Res. 2021, 197, 111154. [Google Scholar] [CrossRef]
- Ni, Z.; Guo, Z.; Chen, X.; Wang, Q.; Wang, Q.; Qiu, Y.; Wu, T.; Yang, Y.; Zhao, L. Cardiac injury in patients with pandemic 2009 influenza A (H1N1) infection. Acta Cardiol. 2011, 66, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, A.; Lucero-Obusan, C.; Schirmer, P.; Winston, C.; Holodniy, M. Acute cardiac injury events ≤30 days after laboratory-confirmed influenza virus infection among U.S. veterans, 2010–2012. BMC Cardiovasc. Disord. 2015, 15, 109. [Google Scholar] [CrossRef] [Green Version]
- Barnes, M.; Heywood, A.E.; Mahimbo, A.; Rahman, B.; Newall, A.T.; Macintyre, C.R. Acute myocardial infarction and influenza: A meta-analysis of case-control studies. Heart 2015, 101, 1738–1747. [Google Scholar] [CrossRef] [Green Version]
- Cowan, L.T.; Buck, B.; Schwind, J.S.; Lutsey, P.L.; Pankow, J.S.; Matsushita, K.; Ishigami, J.; Lakshminarayan, K. Triggering of cardiovascular disease by infection type: The Atherosclerosis Risk in Communities study (ARIC). Int. J. Cardiol. 2021, 325, 155–160. [Google Scholar] [CrossRef]
- Cowan, L.T.; Lutsey, P.L.; Pankow, J.S.; Matsushita, K.; Ishigami, J.; Lakshminarayan, K. Inpatient and Outpatient Infection as a Trigger of Cardiovascular Disease: The ARIC Study. J. Am. Heart Assoc. 2018, 7, e009683. [Google Scholar] [CrossRef] [Green Version]
- Pearce, D.C.; McCaw, J.M.; McVernon, J.; Mathews, J.D. Influenza as a trigger for cardiovascular disease: An investigation of serotype, subtype and geographic location. Environ. Res. 2017, 156, 688–696. [Google Scholar] [CrossRef]
- London, J.W.; Fazio-Eynullayeva, E.; Palchuk, M.B.; Sankey, P.; McNair, C. Effects of the COVID-19 Pandemic on Cancer-Related Patient Encounters. JCO Clin. Cancer Inform. 2020, 4, 657–665. [Google Scholar] [CrossRef]
- Oudit, G.Y.; Kassiri, Z.; Jiang, C.; Liu, P.P.; Poutanen, S.M.; Penninger, J.M.; Butany, J. SARS-coronavirus modulation of myocardial ACE2 expression and inflammation in patients with SARS. Eur. J. Clin. Investig. 2009, 39, 618–625. [Google Scholar] [CrossRef]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: Molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020, 46, 586–590. [Google Scholar] [CrossRef] [Green Version]
- Aronson, J.K.; Ferner, R.E. Drugs and the renin-angiotensin system in COVID-19. BMJ 2020, 369, m1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Li, X.; Chen, M.; Feng, Y.; Xiong, C. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc. Res. 2020, 116, 1097–1100. [Google Scholar] [CrossRef] [Green Version]
- García-Ortega, A.; de la Rosa, D.; Oscullo, G.; Castillo-Villegas, D.; López-Reyes, R.; Martínez-García, M.Á. Coagulation disorders and thromboembolic disease in COVID-19: Review of current evidence in search of a better approach. J. Thorac. Dis. 2021, 13, 1239–1255. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Quincy Brown, J.; Vander Heide, R.S. Pulmonary and cardiac pathology in African American patients with COVID-19: An autopsy series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Guzik, T.J.; Mohiddin, S.A.; Dimarco, A.; Patel, V.; Savvatis, K.; Marelli-Berg, F.M.; Madhur, M.S.; Tomaszewski, M.; Maffia, P.; D’Acquisto, F.; et al. COVID-19 and the cardiovascular system: Implications for risk assessment, diagnosis, and treatment options. Cardiovasc. Res. 2020, 116, 1666–1687. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.Y.; Chao, T.F.; Liu, C.J.; Chen, S.J.; Chung, F.P.; Liao, J.N.; Tuan, T.C.; Chen, T.J.; Chen, S.A. The association between influenza infection, vaccination, and atrial fibrillation: A nationwide case-control study. Heart Rhythm 2016, 13, 1189–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soto-Gomez, N.; Anzueto, A.; Waterer, G.W.; Restrepo, M.I.; Mortensen, E.M. Pneumonia: An arrhythmogenic disease? Am. J. Med. 2013, 126, 43–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badawi, A.; Ryoo, S.G. Prevalence of comorbidities in the Middle East respiratory syndrome coronavirus (MERS-CoV): A systematic review and meta-analysis. Int. J. Infect. Dis. 2016, 49, 129–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Country | Publication Date | Number of Citations | Study Time | Sample Size | Median Age (Years) | Mean Age (Years) | Males |
|---|---|---|---|---|---|---|---|---|
| 7 | China | 24.02.21 | 1 | 01.01.20–27.02.2020 | 181 | 55 (46–65) | 56.4% | |
| 8 | US | 15.02.21 | 4 | 01.03.20–16.04.2020 | 2895 | – | – | – |
| 9 | Italy/USA | 30.01.21 | 2 | 21.02.20–31.05.2020 | 313 | 66.1 (55.1–79.4) | 56.2% | |
| 10 | UK/Spain | 08.03.21 | 1 | Second half of March 2020 | 434 | 66 (56–80) | 62.9% | |
| 11 | Turkey | 25.03.21 | 0 | 15.04.20–death/discharge | 324 | 55.1 ± 12.9 | 52.8% | |
| 12 | USA | 13.08.21 | 0 | 04.04.20–05.06.2020 | 270 | 70 (57–78) | 51.1% | |
| 13 | Pakistan | 01.03.21 | 5 | 01.04.20–31.08.2020 | 201 | 44.6 ± 15.2 | 59.2% | |
| 14 | China/USA | 12.02.21 | 2 | 01.02.20–10.03.21 | 330 | 67 (range: 42–92) | 48.8% | |
| 15 | USA | 13.11.20 | 23 | 15.03.20–11.06.20 | 243 | 62.8 ± 14.9 | 60.9% | |
| 16 | France | 02.03.21 | 2 | 26.02.20–20.04.20 | 2878 | 66.6 ± 17.0 | 57.9% | |
| 17 | China/USA | 28.01.21 | 9 | 15.03.20–01.04.2020 | 218 | 62 (55–69) | 49.6% | |
| 18 | USA | 19.01.21 | 3 | 10.03.20–05.08.2020 | 179 | 59.8 ± 16.9 | 62% | |
| 19 | UK | 20.02.21 | 3 | 03.03.20–21.04.2020 | 176 | 55.1 ± 12.9 | 71% | |
| 20 | USA | 10.05.21 | 3 | 09.07.20–21.10.20 | 137 | 20 (range: 18–27) | 68% | |
| 21 | China | 18.01.21 | 6 | 11.03.20–16.03.2020 | 132 | 55.1 ± 12.9 | 51.5% | |
| 22 | China/USA/UK | 19.02.21 | 1 | 11.01.20–25.03.2020 | 304 | 65 (54.0–74.0) | 52.6% | |
| 23 | China | 09.02.21 | 5 | 29.01.20–04.03.2020 | 128 | 61.3 ± 13.1 | 47.7% | |
| 24 | Italy/Switzerland | 20.07.21 | 3 | 01.03.20–22.04.20 | 226 | 68.9 ± 13.9 | 62.4% | |
| 25 | USA | 16.04.21 | 1 | till 13.07.2020 | 367 | 61 ± 17 | 60% | |
| 26 | China | 11.01.02 | 1 | 03.01.20–26.02.2020 | 400 | 49 (37–61) | 52.2% | |
| 27 | China | 29.01.21 | 0 | 27.01.20–12.02.20 | 726 | 68 (58–77); 65 (55–71) * | 54.1% | |
| 28 | Spain | 16.02.21 | 3 | 01.03.20–30.03.20 | 2873 | 66 (54–76) | 59.1% | |
| 29 | China | 05.03.21 | 1 | 01.01.20–28.02.20 | 242 | 68 (61–75) | 62.4% | |
| 30 | China | 18.02.21 | 1 | 20.01.20–10.04.20 | 173 | 73.0 (64.0–80.5) | 64.2% | |
| 31 | Spain | 18.01.21 | 4 | 16.03.20–15.05.20 | 196 | 67.5 (53.5–78.0) | 59.7% | |
| 32 | Israel | 26.02.21 | 4 | 09.02.20–28.08.2020 | 320 | 73.31 (61.33–82.25); 59.83 (49.65–71.19) ** | 64.1% | |
| 33 | USA | 10.11.20 | 10 | 01.03.20–01.04.20 | 887 | 64 ± 17 | 58% | |
| 34 | UK | 27.01.21 | 3 | 01.03.20–15.04.2020 | 346 | 65 (59–74) 74 (63–83) *** | 64.8%; 43.7% ♥ | |
| 35 | Germany | 06.12.20 | 11 | 01.01.20–30.04.2020 | 147 | 70 (56.5–76); 64 (58–72) ♥♥ | 69%; 70% ♥♥♥ | |
| 36 | Spain | 17.03.21 | 2 | 01.03.20–30.04.2020 | 316 | 68 (58.8–78); 66 (56–77) ♦ | 71.2%; 70.3% ♦♦ | |
| 37 | Japan | 05.02.21 | 8 | 01.01.18–06.04.20 || 07.04.20–14.08.2020 | 422 | 72(61–80); 70 (59–79) ♦♦♦ | 72.1%; 66.7% ♣ | |
| 38 | Italy | 26.02.21 | 6 | 04.03.20–20.05.2020 | 1169 | 70.96 ± 16.71 | 48% | |
| 39 | UK/USA | 18.02.21 | 53 | 01.01.2020–31.10.20 | 148 | 64 ± 12; 64 ± 9 ♣♣ | 56 %; 88 % ♣♣♣ | |
| 40 | USA | 04.03.21 | 34 | 05.2020–10.2020 | 789 | 25 ± 3 | 98.5% | |
| 41 | UK | 17.12.20 | 35 | – | 146 | 20 (19–21); 30 (27–34); 25 (22–27) ♠ | 37%; 63%; 88% ♠♠ | |
| 42 | Israel | 30.10.20 | 5 | 01.02.20–30.05.20 | 390 | 57.5 (43–74.3) | 55.4% | |
| 43 | Portugal | 08.2021 | 0 | 12.04.20–10.05.20 | 692 | 73.5 (61–80.25) ♠♠♠ | 70.3% ☼ | |
| 44 | Germany | 02.01.21 | 11 | 05.03.20–17.06.20 | 166 | 73.6 ± 12.8; 61.6 ± 16.7 ☼☼ | 67.6%; 64.6% ☼☼☼ | |
| 45 | USA/India | 19.03.21 | 5 | 04.2020–06.2020 | 186 | 60 (range: 18–95). | 53.2% | |
| 46 | USA | 16.04.21 | 1 | 01.03.20–01.05.20 | 310 | 61.4 ± 16. | 41.3% | |
| 47 | USA | 22.01.21 | 12 | 01.03.20–27.04.20 | 9564 | 64.8 ± 16. | 58.9% | |
| 48 | USA | 20.02.21 | 0 | 01.03.20–15.04.20 | 1029 | 63.6 ± 17.4 | 57%; 56% § | |
| 49 | Spain | 28.01.21 | 1 | 10.03.20–15.04.20 | 517 | 68.1 ± 15.1 | ||
| 50 | Denmark | 13.03.21 | 3 | 01.03.20–01.06.20 | 155 | 66 (55–74) | 73% | |
| 51 | Spain | 03.11.20 | 11 | 03.2020–04.2020 | 160 | 75.9 ± 9.6; 64.9 ± 16.3 §§ | 66.7%; 59.5% §§§ | |
| 52 | China | 24.01.21 | 0 | 01.02.20–19.03.20 | 463 | 61 (51–69) | 47.9% | |
| 53 | Italy | 29.01.21 | 5 | 01.03.20–10.04.20 | 216 | 67.0 (56.75–79.0) | 66% | |
| 54 | China | 12.03.21 | 1 | 24.02.20–05.04.20 | 168 | 61.60 ± 11.30; 61.90 ± 13.90 • | 44%; 52.4% •• | |
| 55 | Korea | 29.12.20 | 4 | 15.02.20–24.04.20 | 2269 | 55.5 ± 20.2 | 35.9% | |
| 56 | USA | 01.08.21 | 8 | 01.03.20–24.04.20 | 355 | 66.21 ± 14.21 | 49% | |
| 57 | USA | 09.01.21 | 20 | 01.04.20–30.09.20 | 8383 | 71.7 ± 13.2 | 49.8% | |
| 58 | China | 16.03.21 | 4 | 12.02.20–16.03.20 | 157 | 62 ± 13 | 50.3% | |
| 59 | China | 30.01.21 | 3 | 01.02.20–26.02.20 | 148 | 57.2 ± 17.7 | 45.3% | |
| 60 | USA | 02.02.21 | 0 | – | 204 | 64 ± 13 | 76% | |
| 61 | USA/Israel | 25.01.21 | 5 | 01.01.20–08.06.20 | 589 | 66 ± 18 | 56% | |
| 62 | USA | 31.03.21 | 1 | 29.02.20–28.06.20 | 300 | 60 ± 16 | 60% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koźlik, M.; Błahuszewska, A.; Kaźmierski, M. Cardiovascular System during SARS-CoV-2 Infection. Int. J. Environ. Res. Public Health 2022, 19, 1184. https://doi.org/10.3390/ijerph19031184
Koźlik M, Błahuszewska A, Kaźmierski M. Cardiovascular System during SARS-CoV-2 Infection. International Journal of Environmental Research and Public Health. 2022; 19(3):1184. https://doi.org/10.3390/ijerph19031184
Chicago/Turabian StyleKoźlik, Maciej, Adrianna Błahuszewska, and Maciej Kaźmierski. 2022. "Cardiovascular System during SARS-CoV-2 Infection" International Journal of Environmental Research and Public Health 19, no. 3: 1184. https://doi.org/10.3390/ijerph19031184