
Changes in Mental Health among Psychiatric Patients during the COVID-19 Pandemic in Hong Kong—A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Outcome Measures
2.3. Data Analysis
3. Results
3.1. Subject Demographics
3.2. Changes in Patient Satisfaction on Mental Disease Control and Self-Perceived Symptom Change
3.3. DASS-21: Assessment of Subjects’ Depression, Anxiety, and Stress Levels
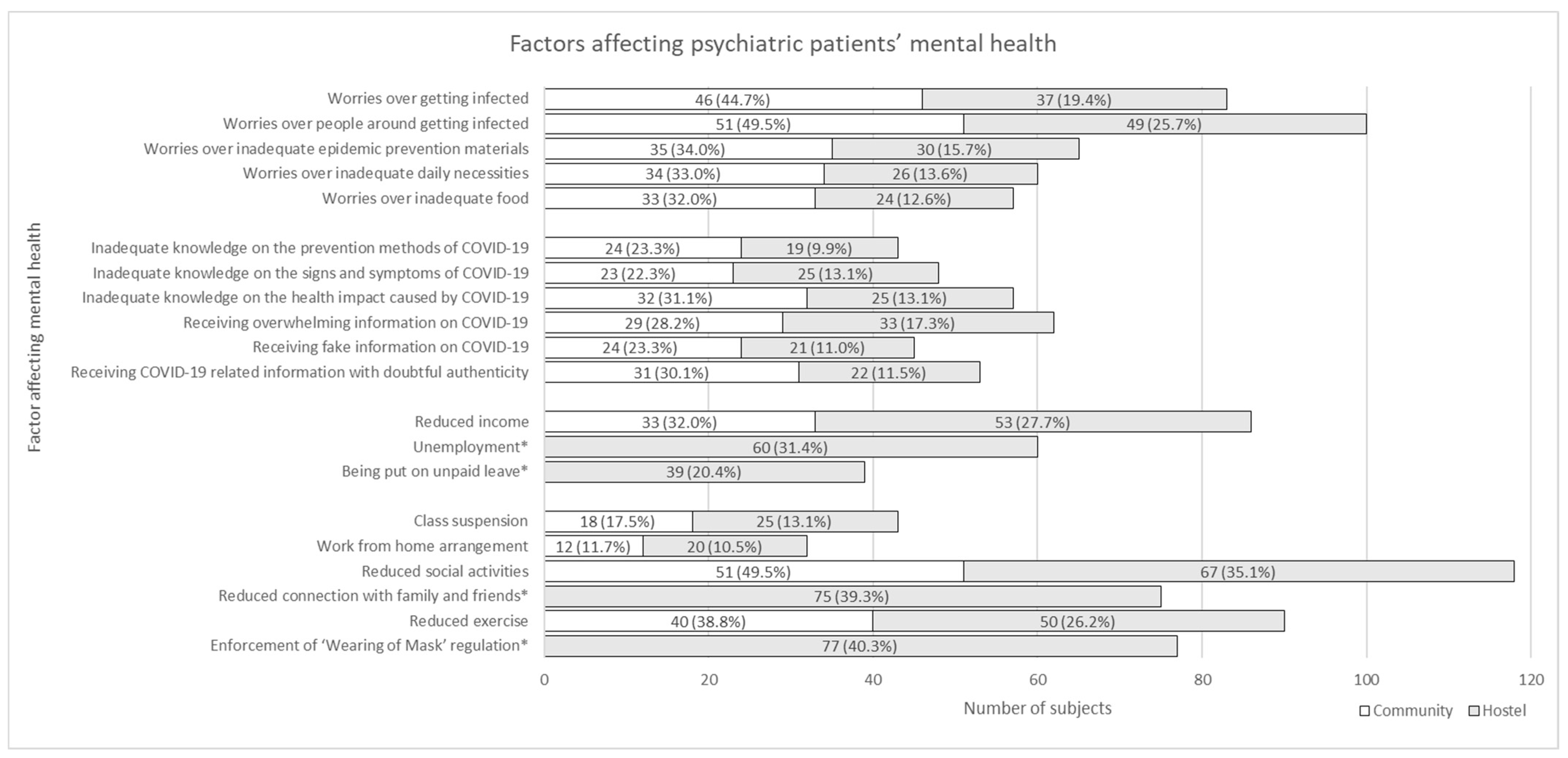
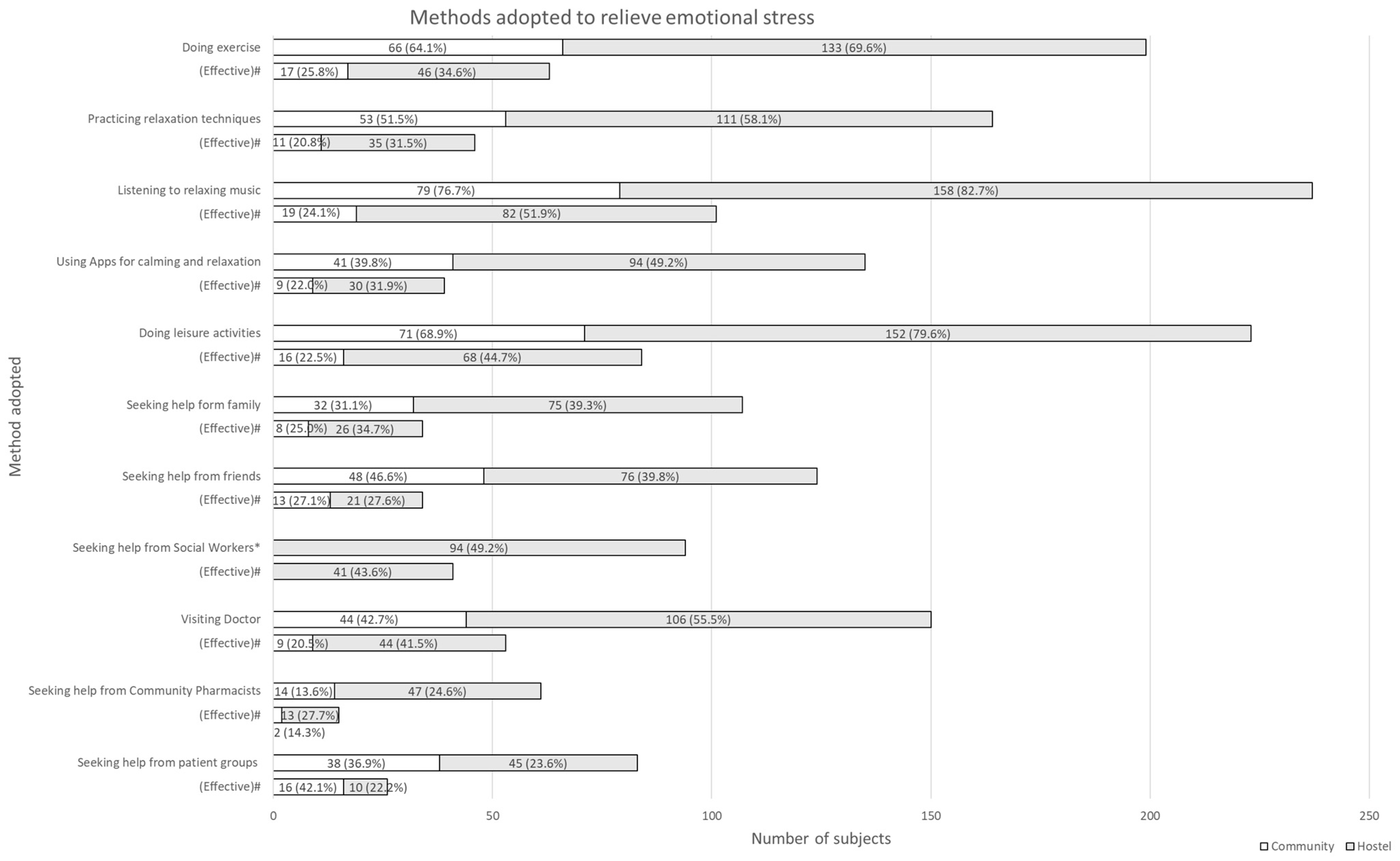
3.4. Factors Affecting Mental Health
4. Discussion
4.1. Practical Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Naming the Coronavirus Disease (COVID-19) and the Virus that Causes It. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 26 May 2021).
- Centre for Health Protection, Department of Health. Frequently Asked Questions on Coronavirus Disease 2019 (COVID-19). 2020. Available online: https://www.chp.gov.hk/en/features/102624.html#FAQ4 (accessed on 26 May 2021).
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Announces COVID-19 Outbreak a Pandemic. 2020. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 26 May 2021).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 26 May 2021).
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef] [PubMed]
- Prime, H.; Wade, M.; Browne, D.T. Risk and resilience in family well-being during the COVID-19 pandemic. Am. Psychol. 2020, 75, 631–643. [Google Scholar] [CrossRef]
- Together We Fight the Virus—Useful Information. The Government of the Hong Kong Special Administrative Region. 2021. Available online: https://www.coronavirus.gov.hk/eng/index.html#Useful_Information (accessed on 26 May 2021).
- Leung, K.; Lum, A. Hong Kong face mask prices soar as residents scramble to stock up amid Wuhan coronavirus fears. South China Morning Post, 24 January 2020. [Google Scholar]
- Chan, H.H.; Sum, L.K. Long queues at outlets across Hong Kong selling masks, as panic buying continues amid Wuhan coronavirus outbreak. South China Morning Post, 29 January 2020. [Google Scholar]
- A scramble for face masks. Mingpao, 19 February 2020.
- Coronavirus fears lead to panic buying of essentials in Hong Kong. CBS News, 7 February 2020.
- Wang, Z.; Wang, D. The influence and enlightenment of five public health emergencies on public psychology since new century: A systematic review. Int. J. Soc. Psychiatry 2021, 67, 878–891. [Google Scholar] [CrossRef]
- Abdelrahman, Z.; Li, M.; Wang, X. Comparative Review of SARS-CoV-2, SARS-CoV, MERS-CoV, and Influenza A Respiratory Viruses. Front Immunol. 2020, 11, 552909. [Google Scholar] [CrossRef]
- Stuijfzand, S.; Deforges, C.; Sandoz, V.; Sajin, C.-T.; Jaques, C.; Elmers, J.; Horsch, A. Psychological impact of an epidemic/pandemic on the mental health of healthcare professionals: A rapid review. BMC Public Health 2020, 20, 1230. [Google Scholar] [CrossRef] [PubMed]
- Esterwood, E.; Saeed, S.A. Past Epidemics, Natural Disasters, COVID19, and Mental Health: Learning from History as we Deal with the Present and Prepare for the Future. Psychiatr. Q. 2020, 91, 1121–1133. [Google Scholar] [CrossRef] [PubMed]
- Yip, P.S.; Cheung, Y.T.; Chau, P.H.; Law, Y.W. The impact of epidemic outbreak: The case of severe acute respiratory syndrome (SARS) and suicide among older adults in Hong Kong. Crisis 2010, 31, 86–92. [Google Scholar] [CrossRef]
- Gan, Y.; Ma, J.; Wu, J.; Chen, Y.; Zhu, H.; Hall, B.J. Immediate and delayed psychological effects of province-wide lockdown and personal quarantine during the COVID-19 outbreak in China. Psychol. Med. 2020, 1–12, published online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Francisco, R.; Pedro, M.; Delvecchio, E.; Espada, J.P.; Morales, A.; Mazzeschi, C.; Orgilés, M. Psychological Symptoms and Behavioral Changes in Children and Adolescents During the Early Phase of COVID-19 Quarantine in Three European Countries. Front. Psychiatry 2020, 11, 570164. [Google Scholar] [CrossRef]
- Passos, L.; Prazeres, F.; Teixeira, A.; Martins, C. Impact on Mental Health Due to COVID-19 Pandemic: Cross-Sectional Study in Portugal and Brazil. Int. J. Environ. Res. Public Health 2020, 17, 6794. [Google Scholar] [CrossRef]
- Sachser, C.; Olaru, G.; Pfeiffer, E.; Brähler, E.; Clemens, V.; Rassenhofer, M.; Witt, A.; Fegert, J.M. The immediate impact of lockdown measures on mental health and couples’ relationships during the COVID-19 pandemic—Results of a representative population survey in Germany. Soc. Sci. Med. 2021, 278, 113954. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Sønderskov, K.M.; Dinesen, P.T.; Santini, Z.I.; Østergaard, S.D. The depressive state of Denmark during the COVID-19 pandemic. Acta Neuropsychiatr. 2020, 32, 226–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Chen, J.H.; Xu, Y.F. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry 2020, 7, e21. [Google Scholar] [CrossRef]
- Muruganandam, P.; Neelamegam, S.; Menon, V.; Alexander, J.; Chaturvedi, S.K. COVID-19 and Severe Mental Illness: Impact on patients and its relation with their awareness about COVID-19. Psychiatry Res. 2020, 291, 113265. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.Y.; Kok, A.A.L.; Eikelenboom, M.; Horsfall, M.; Jörg, F.; Luteijn, R.A.; Rhebergen, D.; Oppen, P.V.; Giltay, E.J.; Penninx, B.W.J.H. The mental health impact of the COVID-19 pandemic on people with and without depressive, anxiety, or obsessive-compulsive disorders: A longitudinal study of three Dutch case-control cohorts. Lancet Psychiatry 2021, 8, 121–129. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Chevance, A.; Gourion, D.; Hoertel, N.; Llorca, P.M.; Thomas, P.; Bocher, R.; Moro, M.R.; Laprévote, V.; Benyamina, A.; Fossati, P.; et al. Ensuring mental health care during the SARS-CoV-2 epidemic in France: A narrative review. Encephale 2020, 46, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Yang, Y.; Liu, Z.H.; Zhao, Y.-J.; Zhang, Q.; Zhang, L.; Cheung, T.; Xiang, Y.-T. Progression of Mental Health Services during the COVID-19 Outbreak in China. Int. J. Biol. Sci. 2020, 16, 1732–1738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Government of the Hong Kong Special Administrative Region. Temporary Closure of Community Halls and Community Centres. 2020. Available online: https://www.info.gov.hk/gia/general/202007/14/P2020071400505.htm (accessed on 26 May 2021).
- World Health Organization. COVID-19 Disrupting Mental Health Services in Most Countries, WHO Survey. 2020. Available online: https://www.who.int/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey (accessed on 26 May 2021).
- Cordellieri, P.; Barchielli, B.; Masci, V.; Viani, F.; de Pinto, I.; Priori, A.; Torriccelli, F.; Cosmo, C.; Ferracuti, S.; Giannini, A.; et al. Psychological Health Status of Psychiatric Patients Living in Treatment Communities before and during the COVID-19 Lockdown: A Brief Report. Int. J. Environ. Res. Public Health 2021, 18, 3567. [Google Scholar] [CrossRef]
- Hodžić, N.; Hasanović, M.; Pajević, I. COVID-19 Affected Mental Health of At-risk Groups of Psychiatric Patients: Two Case Reports. Psychiatr. Danub. 2020, 32, 294–299. [Google Scholar] [CrossRef]
- Rosso, G.; Teobaldi, E.; Maina, G. Did COVID-19 early lockdown actually lead to a higher rate of relapses in psychiatric patients? Psychiatry Res. 2020, 291, 113204. [Google Scholar] [CrossRef]
- Hao, F.; Tan, W.; Jiang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; Tran, B.; et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav. Immun. 2020, 87, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Huang, J.; Sun, J.; Zhao, J.; Chen, A.; Chen, J.; Wu, R.; Li, S.; Teng, Z.; Tan, Y.; et al. Prevalence of Risk Factors Associated With Mental Health Symptoms Among the Outpatient Psychiatric Patients and Their Family Members in China During the Coronavirus Disease 2019 Pandemic. Front Psychol. 2021, 12, 622339. [Google Scholar] [CrossRef]
- Burrai, J.; Roma, P.; Barchielli, B.; Biondi, S.; Cordellieri, P.; Fraschetti, A.; Pizzimenti, A.; Mazza, C.; Ferracuti, S.; Giannini, A.M. Psychological and Emotional Impact of Patients Living in Psychiatric Treatment Communities during COVID-19 Lockdown in Italy. J. Clin. Med. 2020, 9, 3787. [Google Scholar] [CrossRef]
- MacKenzie, M.; Daviskiba, S.; Dow, M.; Johnston, P.; Balon, R.; Javanbakht, A.; Arfken, C.L. The Impact of the Coronavirus Disease 2019 (COVID-19) Pandemic on Healthcare Workers with Pre-Existing Psychiatric Conditions. Psychiatr. Q. 2021, 92, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Favreau, M.; Hillert, A.; Osen, B.; Gärtner, T.; Hunatschek, S.; Riese, M.; Hewera, K.; Voderholzer, U. Psychological consequences and differential impact of the COVID-19 pandemic in patients with mental disorders. Psychiatry Res. 2021, 302, 114045. [Google Scholar] [CrossRef] [PubMed]
- Biviá-Roig, G.; La Rosa, V.L.; Gómez-Tébar, M.; Serrano-Raya, L.; Amer-Cuenca, J.J.; Caruso, S.; Commodari, E.; Barrasa-Shaw, A.; Lisón, J.F. Analysis of the Impact of the Confinement Resulting from COVID-19 on the Lifestyle and Psychological Wellbeing of Spanish Pregnant Women: An Internet-Based Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 5933. [Google Scholar] [CrossRef] [PubMed]
- Berardelli, I.; Sarubbi, S.; Rogante, E.; Cifrodelli, M.; Erbuto, D.; Innamorati, M.; Lester, D.; Pompili, M. The impact of the COVID-19 pandemic on suicide ideation and suicide attempts in a sample of psychiatric inpatients. Psychiatry Res. 2021, 303, 114072. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation of Australia: Sydney, Australia, 1995. [Google Scholar]
- Lee, J.; Lee, E.H.; Moon, S.H. Systematic review of the measurement properties of the Depression Anxiety Stress Scales-21 by applying updated COSMIN methodology. Qual. Life Res. 2019, 28, 2325–2339. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Shi, H.S.; Geng, F.L.; Zou, L.-Q.; Tan, S.-P.; Wang, Y.; Neumann, D.L.; Shum, D.H.K.; Chan, R.C.K. Cross-cultural validation of the Depression Anxiety Stress Scale-21 in China. Psychol. Assess. 2016, 28, e88–e100. [Google Scholar] [CrossRef]
- Lee, A.M.; Wong, J.G.; McAlonan, G.M.; Cheung, V.; Cheung, C.; Sham, P.C.; Chu, C.-M.; Wong, P.-C.; Tsang, K.W.; Chua, S.E. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can. J. Psychiatry 2007, 52, 233–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Govt Ready for New COVID-19 Wave. News.gov.hk. 2020. Available online: https://www.news.gov.hk/eng/2020/11/20201120/20201120_143306_589.html (accessed on 26 May 2021).
- Latest Situation of Coronavirus Disease (COVID-19) in Hong Kong. Centre for Health Protection. 2020. Available online: https://chp-dashboard.geodata.gov.hk/covid-19/en.html (accessed on 26 May 2021).
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Lei, W.; Xu, F.; Liu, H.; Yu, L. Emotional responses and coping strategies in nurses and nursing students during COVID-19 outbreak: A comparative study. PLoS ONE 2020, 15, e0237303. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.C. 16% increase in utility of JUSTONE 24-Hour Community Mental Health Support Project. Topick, 29 May 2020. (In Chinese) [Google Scholar]
- Choi, E.P.H.; Hui, B.P.H.; Wan, E.Y.F. Depression and Anxiety in Hong Kong during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3740. [Google Scholar] [CrossRef] [PubMed]
- Local Mental Health Online Support Services. Shall We Talk. 2021. Available online: https://shallwetalk.hk/en/get-help/online-support/ (accessed on 26 May 2021).
- Care & Support Networking Team. Society for Community Organization. 2021. Available online: https://soco.org.hk/en/projecthome/networking-team/ (accessed on 26 May 2021).
- Mental Illness. The Mental Health Association of Hong Kong. 2021. Available online: https://www.mhahk.org.hk/index.php/mental-illness/ (accessed on 26 May 2021).
- Alkhamees, A.A.; Alrashed, S.A.; Alzunaydi, A.A.; Almohimeed, A.S.; Aljohani, M.S. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr. Psychiatry 2020, 102, 152192. [Google Scholar] [CrossRef] [PubMed]
- Tee, M.L.; Tee, C.A.; Anlacan, J.P.; Aligam, K.J.G.; Reyes, P.W.C.; Kuruchittham, V.; Ho, R.C. Psychological impact of COVID-19 pandemic in the Philippines. J. Affect. Disord. 2020, 277, 379–391. [Google Scholar] [CrossRef]
- Leung, G.M.; Ho, L.M.; Lam, T.H.; Hedley, A.J. Epidemiology of SARS in the 2003 Hong Kong epidemic. Hong Kong Med. J. 2009, 15 (Suppl. 9), 12–16. [Google Scholar] [PubMed]
- Hung, L.S. The SARS epidemic in Hong Kong: What lessons have we learned? J. R. Soc. Med. 2003, 96, 374–378. [Google Scholar] [CrossRef]
- Li, W.; Zhao, N.; Yan, X.; Zou, S.; Wang, H.; Li, Y.; Xu, X.; Du, X.; Zhang, L.; Zhang, Q.; et al. The prevalence of depressive and anxiety symptoms and their associations with quality of life among clinically stable older patients with psychiatric disorders during the COVID-19 pandemic. Transl. Psychiatry 2021, 11, 75. [Google Scholar] [CrossRef] [PubMed]
- Solé, B.; Verdolini, N.; Amoretti, S.; Montejo, L.; Rosa, A.R.; Hogg, B.; Garcia-Rizo, C.; Mezquida, G.; Bernardo, M.; Martinez-Aran, A.; et al. Effects of the COVID-19 pandemic and lockdown in Spain: Comparison between community controls and patients with a psychiatric disorder. Preliminary results from the BRIS-MHC STUDY. J. Affect. Disord. 2021, 281, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Jose, A.L.; Harrison, M.; Roy, A.S.; Fitzpatrick, L.I.; Forsyth, K. The level of formal support received by people with severe mental illness living in supported accommodation and participation: A systematic review. Int. J. Soc. Psychiatry 2021, 67, 854–866. [Google Scholar] [CrossRef] [PubMed]
- Extending follow up intervals may increase relapse risk, serious cases should be visited every three months [Article in Chinese]. Ming Pao, 29 February 2021.
- Wang, J.; Mann, F.; Lloyd-Evans, B.; Ma, R.; Johnson, S. Associations between loneliness and perceived social support and outcomes of mental health problems: A systematic review. BMC Psychiatry 2018, 18, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathore, F.A.; Farooq, F. Information Overload and Infodemic in the COVID-19 Pandemic. J. Pak. Med. Assoc. 2020, 70 (Suppl. 3), S162–S165. [Google Scholar] [CrossRef] [PubMed]
- Choi, D.H.; Yoo, W.; Noh, G.Y.; Park, K. The impact of social media on risk perceptions during the MERS outbreak in South Korea. Comput. Human Behav. 2017, 72, 422–431. [Google Scholar] [CrossRef]
- Liu, S.; Yang, L.; Zhang, C.; Xiang, Y.-T.; Liu, Z.; Hu, S.; Zhang, B. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e17–e18. [Google Scholar] [CrossRef]
- Hu, N.; Pan, S.; Sun, J.; Wang, Z.; Mao, H. Mental health treatment online during the COVID-19 outbreak. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 270, 783–784. [Google Scholar] [CrossRef]
- Zhou, X.; Snoswell, C.L.; Harding, L.E.; Bambling, M.; Edirippulige, S.; Bai, X.; Smith, A.C. The Role of Telehealth in Reducing the Mental Health Burden from COVID-19. Telemed. J. E Health 2020, 26, 377–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, L.C.; Wong, C.S.; Wang, M.J.; Chan, W.-C.; Chen, E.; Ng, R.M.-K.; Hung, S.-F.; Cheung, E.F.-C.; Sham, P.-C.; Chiu, H.F.-K.; et al. Prevalence, psychosocial correlates and service utilization of depressive and anxiety disorders in Hong Kong: The Hong Kong Mental Morbidity Survey (HKMMS). Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1379–1388. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Total (n = 294) | Community (n = 103) | Hostel (n = 191) | ||
|---|---|---|---|---|
| Age (n = 293) | 18–29 | 32 (10.9%) | 8 (7.8%) | 24 (12.6%) |
| 30–44 | 123 (42.0%) | 37 (35.9%) | 86 (45.3%) | |
| 45–59 | 107 (36.5%) | 43 (41.7%) | 64 (33.7%) | |
| 60 or above | 31 (10.6%) | 15 (14.6%) | 16 (8.4%) | |
| Gender (n = 285) | Male | 163 (57.2%) | 68 (66.0%) | 95 (52.2%) |
| Female | 122 (42.8%) | 35 (34.0%) | 87 (47.8%) | |
| Education level (n = 285) | Never received educated | 2 (0.7%) | 1 (1.0%) | 1 (0.5%) |
| Primary or below | 27 (9.4%) | 8 (7.8%) | 19 (10.4%) | |
| Secondary | 190 (66.7%) | 60 (58.3%) | 130 (71.4%) | |
| Post-secondary | 31 (10.9%) | 11 (10.7%) | 20 (11.0%) | |
| Degree or above | 35 (12.3%) | 23 (22.3%) | 12 (6.6%) | |
| Psychiatric diagnoses (n = 294) | Anxiety disorders | 56 (19.0%) | 35 (34.0%) | 21 (11.0%) |
| Depressive disorders | 99 (33.7%) | 57 (55.3%) | 42 (22.0%) | |
| Bipolar disorders | 48 (16.3%) | 19 (18.4%) | 29 (15.2%) | |
| Schizophrenia | 173 (58.8%) | 38 (36.9) | 135 (70.7%) | |
| Duration of psychiatric illness (n = 244) | 5 years or less | 65 (26.6%) | 22 (21.8%) | 43 (30.1%) |
| 6–10 years | 63 (25.8%) | 21 (20.8%) | 42 (29.4%) | |
| 11–20 years | 64 (26.2%) | 36 (35.6%) | 28 (19.6%) | |
| More than 20 years | 52 (21.3%) | 22 (21.8%) | 30 (21.0%) | |
| Newly diagnosed with mental illness during the COVID-19 outbreak (n = 292) | Yes | 35 (12.0%) | 15 (14.6%) | 20 (10.6%) |
| No | 257 (88.0%) | 88 (85.4%) | 169 (89.4%) | |
| Current psychiatric medications (n = 274) | Sedatives/hypnotics | 89 (32.5%) | 41 (42.3%) | 48 (27.1%) |
| Anti-depressants | 134 (48.9%) | 65 (67.0%) | 69 (39.0%) | |
| Anti-psychotics | 152 (55.5%) | 33 (34.0%) | 119 (67.2%) | |
| Mood stabilizers | 104 (38.0%) | 31 (32.0%) | 73 (41.2%) | |
| Number of psychiatric medications (n = 242) | 1–2 | 151 (62.4%) | 49 (52.7%) | 102 (68.5%) |
| 3–4 | 64 (26.4%) | 31 (32.0%) | 33 (22.1%) | |
| 5–6 | 20 (8.3%) | 10 (10.8%) | 10 (6.7%) | |
| 7 or above | 7 (2.9%) | 3 (3.2%) | 4 (2.7%) | |
| Had undergone mandatory health quarantine (n = 294) | Yes | 10 (3.4%) | 0 (0.0%) | 10 (5.2%) |
| No | 284 (96.6%) | 103 (100.0%) | 181 (94.8%) | |
| Had been diagnosed with COVID-19 (n = 292) | Yes | 0 (0%) | 0 (0.0%) | 0 (0.0%) |
| No | 292 (100%) | 103 (100.0%) | 189 (100.0%) |
| Normal | Mild | Moderate | Severe | Extremely Severe | Mean Score | p-Value | Mean Score | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|---|
| DASS 21-Depression | ||||||||||
| Total | 142 (49.8%) | 32 (11.2%) | 42 (14.7%) | 31 (10.9%) | 38 (13.3%) | 12.31 ± 11.43 | Total | 12.31 ± 11.43 | ||
| Community | 35 (34.0%) | 11 (10.7%) | 21 (20.4%) | 11 (10.7%) | 25 (24.3%) | 17.0 ± 12.7 | p = 0.002 | D + A | 15.7 ± 11.7 | p = 0.024 |
| Hostel | 107 (58.8%) | 21 (11.5%) | 21 (11.5%) | 20 (11.0%) | 13 (7.1%) | 9.7 ± 9.7 | B + S | 10.1 ± 10.6 | ||
| DASS 21-Anxiety | ||||||||||
| Total | 127 (44.6%) | 22 (7.7%) | 43 (15.1%) | 30 (10.5%) | 63 (22.1%) | 11.24 ± 9.94 | Total | 11.24 ± 9.94 | ||
| Community | 32 (31.1%) | 8 (7.77%) | 14 (13.6%) | 16 (15.5%) | 33 (32.0%) | 14.9 ± 10.9 | p = 0.001 | D + A | 14.3 ± 10.6 | p = 0.006 |
| Hostel | 95 (52.2%) | 14 (7.7%) | 29 (15.9%) | 14 (7.7%) | 30 (16.5%) | 9.2 ± 8.7 | B + S | 9.1 ± 8.7 | ||
| DASS 21-Stress | ||||||||||
| Total | 169 (59.3%) | 26 (9.1%) | 36 (12.6%) | 36 (12.6%) | 18 (6.3%) | 13.80 ± 11.25 | Total | 13.80 ± 11.25 | ||
| Community | 42 (40.8%) | 9 (8.7%) | 15 (14.6%) | 23 (22.3%) | 14 (13.6%) | 19.4 ± 11.8 | p < 0.001 | D + A | 17.8 ± 10.8 | p = 0.005 |
| Hostel | 127 (69.8%) | 17 (9.3%) | 21 (11.5%) | 13 (7.1%) | 4 (2.2%) | 10.6 ± 9.6 | B + S | 11.1 ± 10.6 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.T.-S.; Lee, C.-P.; Tang, W.-K. Changes in Mental Health among Psychiatric Patients during the COVID-19 Pandemic in Hong Kong—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1181. https://doi.org/10.3390/ijerph19031181
Li JT-S, Lee C-P, Tang W-K. Changes in Mental Health among Psychiatric Patients during the COVID-19 Pandemic in Hong Kong—A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1181. https://doi.org/10.3390/ijerph19031181
Chicago/Turabian StyleLi, Joyce Tik-Sze, Chui-Ping Lee, and Wai-Kwong Tang. 2022. "Changes in Mental Health among Psychiatric Patients during the COVID-19 Pandemic in Hong Kong—A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 3: 1181. https://doi.org/10.3390/ijerph19031181