
Relationship between Oral Function and Support/Care-Need Certification in Japanese Older People Aged ≥ 75 Years: A Three-Year Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
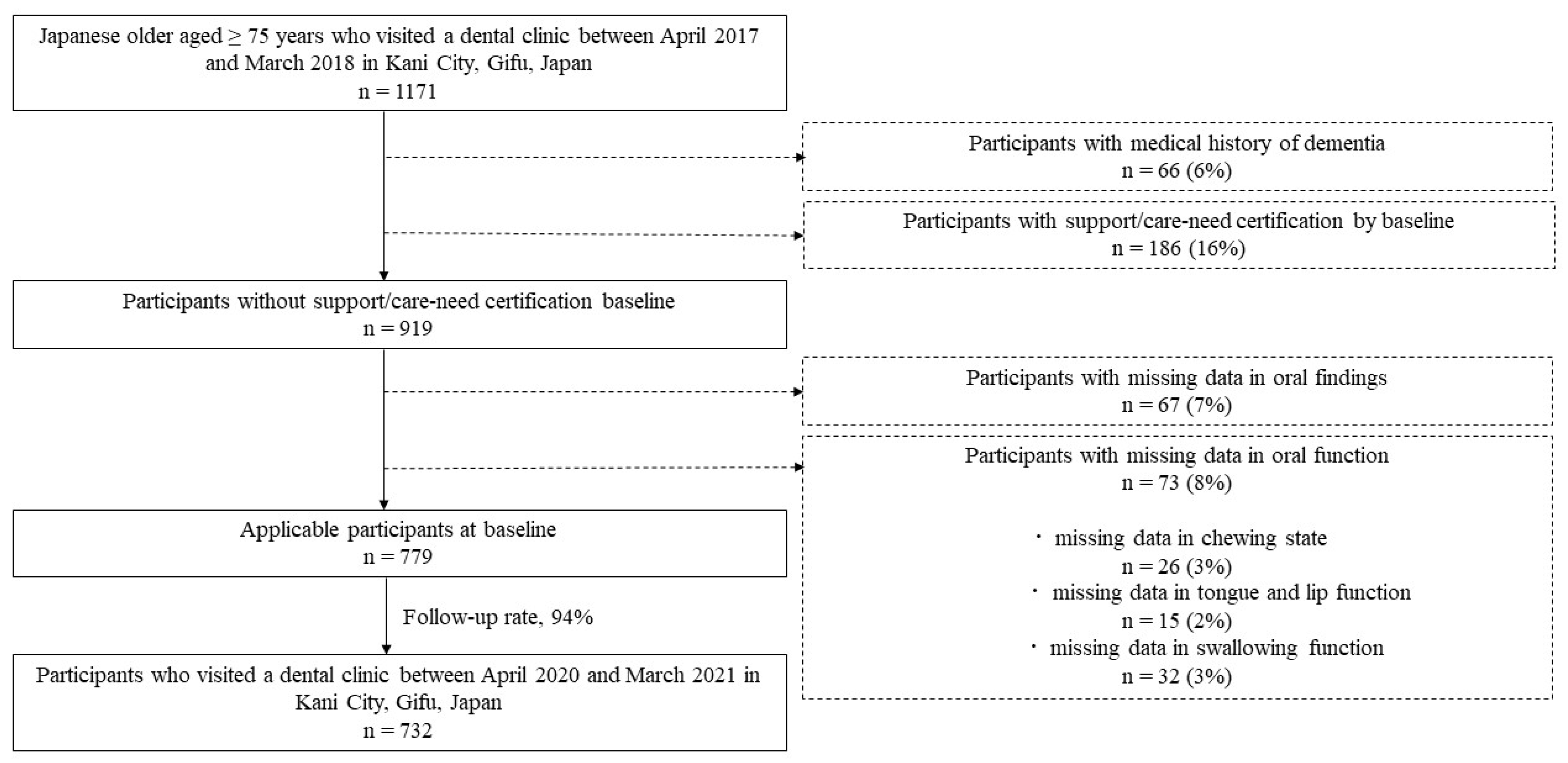
2.1. Participants
2.2. Survey Items in the National Health Insurance Database System
2.3. Oral Items
2.4. Statistical Analysis
2.5. Research Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat. World Population Prospects. Available online: https://population.un.org/wpp/ (accessed on 24 October 2022).
- The United Nations Secretariat. Population and Vital Statistics Report. Available online: https://www.un.org/en/desa/population-and-vital-statistics-report (accessed on 24 October 2022).
- Arai, H.; Ouchi, Y.; Toba, K.; Endo, T.; Shimokado, K.; Tsubota, K.; Matsuo, S.; Mori, H.; Yumura, W.; Yokode, M.; et al. Japan as the front-runner of super-aged societies: Perspectives from medicine and medical care in Japan. Geriatr. Gerontol. Int. 2015, 15, 673–687. [Google Scholar] [CrossRef]
- Statistics Division, Ministry of Internal Affairs and Communications. Population Statistics. Available online: https://www.stat.go.jp/data/index.html (accessed on 24 October 2022).
- National Institute of Population and Social Security Research. Future Population Projection Report 2019. Available online: https://www.stat.go.jp/data/jinsui/ (accessed on 24 October 2022).
- Umit, T.; Ewout, W.S.; Sita, M.A.B.Z.; Albert, H.; Bart, W.K.; Arianne, P.V. Age, gender and disability predict future disability in older people: The Rotterdam Study. BMC Geriatr. 2011, 11, 22. [Google Scholar]
- Gill, M.T.; Han, L.; Gahbauer, A.E.; Leo-Summers, L.; Allore, G.H. Prognostic effect of changes in physical function over prior year on subsequent mortality and long-term nursing home admission. J. Am. Geriatr. Soc. 2018, 66, 1587–1591. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare, Health and Welfare Division for the Elderly. Mechanism and Procedure for Support/Care-Need Certification. Available online: https://www.mhlw.go.jp/file/05-Shingikai-11901000-Koyoukintoujidoukateikyoku-Soumuka/0000126240 (accessed on 24 October 2022).
- Cabinet Office. White Paper on Aging Society 2020. Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2017/html/zenbun/s1_2_3.html (accessed on 24 October 2022).
- Kikutani, T.; Kodama, M.; Nishiwaki, K.; Fukui, T.; Inaba, S.; Yoneyama, T. The relationship of oral, physical and mental functions to the nutritional status in the frail elderly. J. Gerodontology 2003, 18, 10–16. [Google Scholar]
- Takeuchi, K.; Aida, J.; Ito, K.; Furuta, M.; Yamashita, Y.; Osaka, K. Nutritional status and dysphagia risk among community-dwelling frail older adults. J. Nutr. Health Aging 2014, 18, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Hirata, A.; Ishizaka, M.; Sawaya, Y.; Shiba, T.; Urano, T. Relationship between the swallowing function, nutritional status, and sarcopenia in elderly outpatients. J. Geriatr. Soc. 2021, 58, 134–142. [Google Scholar] [CrossRef]
- Matsue, T.; Aita, H.; Yamada, R.; Kawakami, T.; Hirai, T. Predictors of deteriorated oral function for older adults in long-term care insurance facilities: Focusing on rinsing ability and activities of daily living evaluated by care providers. J. Gerodontology 2021, 36, 227–238. [Google Scholar]
- Nakagawa, K.; Matsuo, K. Assessment of oral function and proper diet level for frail elderly individuals in nursing homes using chewing training food. J. Nutr. 2019, 23, 483–489. [Google Scholar] [CrossRef]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tsuji, T.; Akishita, M.; Iijima, K. Oral frailty as a risk factor for physical frailty and mortality in community-dwelling elderly. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1661–1667. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Oral Health Surveys, Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Yamamoto, T.; Aida, J.; Kondo, K.; Fuchida, S.; Tani, Y.; Saito, M.; Sasaki, Y. Oral health and incident depressive symptoms: JAGES project longitudinal study in older Japanese. J. Am. Geriatr. Soc. 2017, 65, 1079–1084. [Google Scholar] [CrossRef]
- Satake, A.; Kobayashi, W.; Tamura, Y.; Oyama, T.; Fukuta, H.; Inui, A.; Sawada, K.; Ihara, K.; Noguchi, T.; Murashita, K.; et al. Effects of oral environment on frailty: Particular relevance of tongue pressure. Clin. Interv. Aging 2019, 12, 1643–1648. [Google Scholar] [CrossRef] [Green Version]
- Tamura, F.; Mizukami, M.; Ayano, R.; Mukai, Y. Analysis of feeding function and jaw stability in bedridden elderly. Dysphagia 2002, 17, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Serra-Prat, M.; Palomera, M.; Gomez, C.; Sar-Shalom, D.; Saiz, A.; Montoya, G.J.; Navajas, M.; Palomera, E.; Clavé, P. Oropharyngeal dysphagia as a risk factor for malnutrition and lower respiratory tract infection in independently living older persons: A population-based prospective study. Age Ageing 2012, 41, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Enoki, H.; Sugiyama, M.; Izawa, S.; Hirose, T.; Hasegawa, J.; Iguchi, A.; Kuzuya, M. Factors associated with malnutrition in community-dwelling disabled elderly: The Kanagawa-Aichi disabled elderly cohort (KAIDEC) study. J. Geriatr. Soc. 2014, 51, 547–553. [Google Scholar]
- Beck, M.A. Weight loss, mortality and associated potentially modifiable nutritional risk factors among nursing home residents-a danish follow-up study. J. Nutr. Health Aging 2015, 19, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Izawa, S.; Kuzuya, M.; Okada, K.; Enoki, H.; Koike, T.; Kanda, S.; Iguchi, A. The nutritional status of frail elderly with care needs according to the mini-nutritional assessment. Clin. Nutr. 2006, 25, 962–967. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, Y.; Aida, J.; Watt, G.R.; Tsuboya, T.; Koyama, S.; Sato, Y.; Kondo, K.; Osaka, K. Dental status and compression of life expectancy with disability. J. Dent. Res. 2017, 96, 1006–1013. [Google Scholar] [CrossRef] [Green Version]
- Motokawa, K.; Mikami, Y.; Shirobe, M.; Edahiro, A.; Ohara, Y.; Iwasaki, M.; Watanabe, Y.; Kawai, H.; Kera, T.; Obuchi, S.; et al. Relationship between chewing ability and nutritional status in Japanese older adults: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 1216. [Google Scholar] [CrossRef]
- Tanaka, T.; Hirano, H.; Ohara, Y.; Nishimoto, M.; Iijima, K. Oral frailty index-8 in the risk assessment of new-onset oral frailty and functional disability among community-dwelling older adults. Arch. Gerontol. Geriatr. 2021, 94, 104340. [Google Scholar] [CrossRef]
- Ohara, S.; Takada, K.; Yoshiike, N.; Sugiyama, M.; Noritake, K.; Tonami, K.; Shinada, K.; Kawaguchi, Y.; Araki, K.; Mataki, S.; et al. Nutritional improvement, denture use, and chewing in elderly patients requiring nursing care with reduced masticatory function. Health Labor Stat. 2016, 63, 37–44. (In Japanese) [Google Scholar]
- Yamada, M.; Arai, H. Self-management group exercise extends healthy life expectancy in frail community-dwelling older adults. Int. J. Environ. Res. Public Health 2017, 14, 531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, K.; Ikeda, T.; Watanabe, R.; Kondo, N.; Kawachi, I.; Kondo, K. Intensity of community-based programs by long-term care insurers and the likelihood of frailty: Multilevel analysis of older Japanese adults. Soc. Sci. Med. 2020, 245, 112701. [Google Scholar] [CrossRef] [PubMed]
- Tani, N.; Hanioka, T.; Higuchi, Y.; Ohta, M.; Yamamoto, R.; Akatsu, J. Evaluating the relationship between oral health status in male workers and question item regarding subjective chewing symptoms. Sangyo Eiseigaku Zasshi 2022, 2021027B. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, T.; Ueno, M.; Shinada, K.; Ohara, S.; Kawaguchi, Y. Validity of self reported masticatory function in a Japanese population. J. Dent. Health 2010, 60, 214–223. [Google Scholar]


{kind=link}
| Factor | Baseline | Follow Up | p-Value * |
|---|---|---|---|
| Sex † | 399 (55%) | 399 (55%) | - |
| Age (y) | 78 (76, 81) | 81 (79, 84) | - |
| Hypertension ‡ | 412 (56%) | 419 (57%) | 0.711 |
| Diabetes mellitus ‡ | 280 (38%) | 287 (39%) | 0.788 |
| Dyslipidemia ‡ | 353 (48%) | 362 (50%) | 0.637 |
| Musculoskeletal disorders ‡ | 517 (71%) | 547 (75%) | 0.078 |
| Pneumonia ‡ | 182 (25%) | 193 (26%) | 0.509 |
| Number of present teeth | 24 (19, 27) | 24 (19, 27) | 0.161 |
| Periodontal pockets ≥ 4 mm ‡ | 456 (62%) | 493 (67%) | 0.042 |
| Chewing state § | 77 (11%) | 79 (11%) | 0.865 |
| Tongue and lip function § | 11 (2%) | 17 (2%) | 0.331 |
| Swallowing function § | 73 (10%) | 88 (12%) | 0.275 |
| Factor | Support/Care-Need Certification at Follow Up | p-Value * | |
|---|---|---|---|
| Absent (n = 611) | Present (n = 121) | ||
| Sex † | 354 (58%) | 45 (37%) | <0.001 |
| Age (y) | 78 (76, 80) | 81 (78, 85) | <0.001 |
| Hypertension ‡ | 329 (54%) | 83 (69%) | 0.003 |
| Diabetes mellitus ‡ | 228 (37%) | 52 (43%) | 0.242 |
| Dyslipidemia ‡ | 290 (48%) | 63 (52%) | 0.355 |
| Musculoskeletal disorders ‡ | 415 (68%) | 102 (84%) | <0.001 |
| Pneumonia ‡ | 144 (23%) | 39 (32%) | 0.044 |
| Number of present teeth | 24 (19, 27) | 24 (20, 27) | 0.337 |
| Periodontal pockets ≥ 4 mm ‡ | 381 (63%) | 75 (62%) | 0.938 |
| Chewing state § | 44 (7%) | 33 (27%) | <0.001 |
| Tongue and lip function § | 8 (1%) | 3 (3%) | 0.334 |
| Swallowing function § | 52 (9%) | 21 (17%) | 0.003 |
| Factor | ORs | 95% CI | p-Value | |
|---|---|---|---|---|
| Sex | Man | 1 | (reference) | <0.001 |
| Woman | 2.326 | 1.556–3.478 | ||
| Age (y) | 1.233 | 1.171–1.297 | <0.001 | |
| Hypertension | No | 1 | (reference) | 0.003 |
| Yes | 1.872 | 1.236–2.837 | ||
| Diabetes mellitus | No | 1 | (reference) | 0.243 |
| Yes | 1.266 | 0.852–1.880 | ||
| Dyslipidemia | No | 1 | (reference) | 0.355 |
| Yes | 1.202 | 0.814–1.777 | ||
| Musculoskeletal disorders | No | 1 | (reference) | <0.001 |
| Yes | 2.535 | 1.510–4.258 | ||
| Pneumonia | No | 1 | (reference) | 0.045 |
| Yes | 1.542 | 1.009–2.358 | ||
| Number of present teeth | 0.987 | 0.960–1.014 | 0.337 | |
| Periodontal pockets ≥ 4 mm | No | 1 | (reference) | 0.938 |
| Yes | 0.984 | 0.659–1.471 | ||
| Chewing state | Well | 1 | (reference) | <0.001 |
| Poor | 4.862 | 2.935–8.054 | ||
| Tongue and lip function | Well | 1 | (reference) | 0.342 |
| Poor | 1.916 | 0.501–7.329 | ||
| Swallowing function | Well | 1 | (reference) | 0.004 |
| Poor | 2.257 | 1.303–3.911 |
| Factor | ORs | 95% CI | p-Value | |
|---|---|---|---|---|
| Sex | Man | 1 | (reference) | 0.001 |
| Woman | 2.120 | 1.354–3.317 | ||
| Age (y) | 1.203 | 1.139–1.270 | <0.001 | |
| Hypertension | No | 1 | (reference) | 0.189 |
| Yes | 1.368 | 0.857–2.182 | ||
| Musculoskeletal disorders | No | 1 | (reference) | 0.091 |
| Yes | 1.646 | 0.924–2.932 | ||
| Pneumonia | No | 1 | (reference) | 0.111 |
| Yes | 1.470 | 0.915–2.361 | ||
| Chewing state | Well | 1 | (reference) | 0.002 |
| Poor | 2.534 | 1.409–4.557 | ||
| Swallowing function | Well | 1 | (reference) | 0.008 |
| Poor | 2.372 | 1.248–4.510 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwai, K.; Azuma, T.; Yonenaga, T.; Nomura, T.; Sugiura, I.; Inagawa, Y.; Matsumoto, Y.; Nakashima, S.; Abe, Y.; Tomofuji, T. Relationship between Oral Function and Support/Care-Need Certification in Japanese Older People Aged ≥ 75 Years: A Three-Year Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 16959. https://doi.org/10.3390/ijerph192416959
Iwai K, Azuma T, Yonenaga T, Nomura T, Sugiura I, Inagawa Y, Matsumoto Y, Nakashima S, Abe Y, Tomofuji T. Relationship between Oral Function and Support/Care-Need Certification in Japanese Older People Aged ≥ 75 Years: A Three-Year Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(24):16959. https://doi.org/10.3390/ijerph192416959
Chicago/Turabian StyleIwai, Komei, Tetsuji Azuma, Takatoshi Yonenaga, Taketsugu Nomura, Iwane Sugiura, Yujo Inagawa, Yusuke Matsumoto, Seiji Nakashima, Yoshikazu Abe, and Takaaki Tomofuji. 2022. "Relationship between Oral Function and Support/Care-Need Certification in Japanese Older People Aged ≥ 75 Years: A Three-Year Cohort Study" International Journal of Environmental Research and Public Health 19, no. 24: 16959. https://doi.org/10.3390/ijerph192416959