
Lessons Learned from the COVID-19 Pandemic in Nursing Homes: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Eligibility Criteria
2.3. Sources of Information and Search Strategy
2.4. Data Extraction and Analysis
3. Results
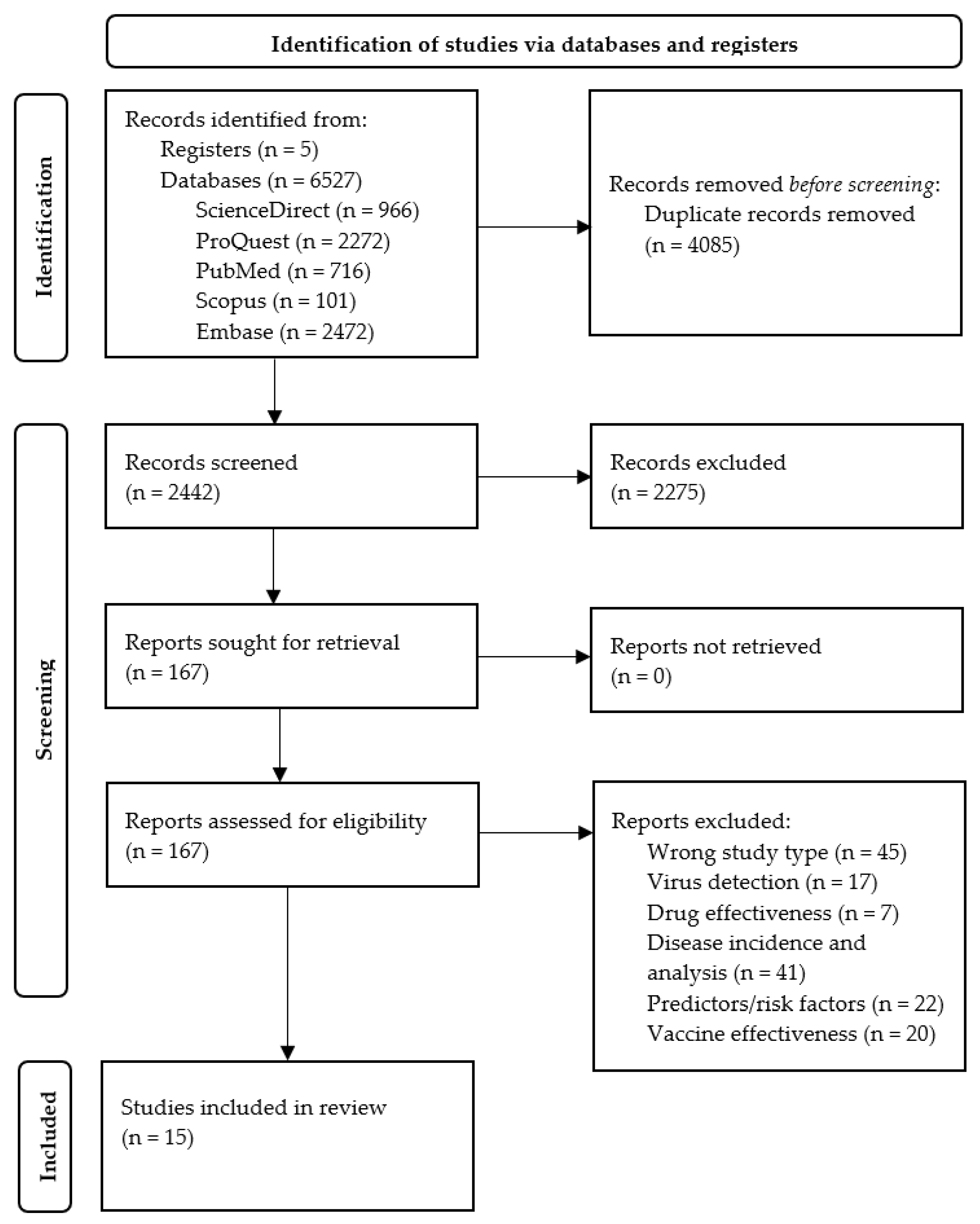
3.1. Study Selection
3.2. Description of Included Studies
3.3. Identification and Classification of Lessons Learned According to IDEF Methodology
3.4. Narrative Synthesis of Studies about Lessons Learned in Care Homes during the COVID-19 Pandemic
3.4.1. Good Practices Incorporated into the Strategic Processes of Care Homes during Pandemic
3.4.2. Good Practices Incorporated into Care Home Operational Processes during Pandemic
3.4.3. Good Practices Incorporated into Care Home Support Processes during Pandemic
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Palacios Cruz, M.; Santos, E.; Velázquez Cervantes, M.A.; León Juárez, M. COVID-19, una emergencia de salud pública mundial [COVID-19, a worldwide public health emergency]. Rev. Clin. Esp. 2021, 221, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Institut National d’Études Démographiques (INED) [National Institute for Demographic Studies]. Demography of COVID-19 Deaths. Available online: https://covid-19-apport-demographie.site.ined.fr/en/research-projects/demography-of-covid-19-deaths (accessed on 5 December 2020).
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.J.; Díez-Villanueva, P.; Ayesta, A.; Sanchis Forés, J.; Vidán-Austiz, M.T.; Formiga, F.; Ariza-Solé, A.; Martínez-Sellés, M. Coronavirus: La emergencia geriátrica de 2020. Documento conjunto de la Sección de Cardiología Geriátrica de la Sociedad Española de Cardiología y la Sociedad Española de Geriatría y Gerontología [Coronavirus: The Geriatric Emergency of 2020. Joint Document of the Section on Geriatric Cardiology of the Spanish Society of Cardiology and the Spanish Society of Geriatrics and Gerontology]. Rev. Clin. Esp. 2020, 73, 569–576. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Pan American Health Organization (PAHO). People over 60 Have Been Hardest Hit by COVID-19 in the Americas. Available online: https://www.paho.org/en/news/30-9-2020-people-over-60-have-been-hardest-hit-covid-19-americas (accessed on 30 September 2020).
- Lithander, F.E.; Neumann, S.; Tenison, E.; Lloyd, K.; Welsh, T.J.; Rodrigues, J.C.; Higgins, J.P.; Scourfield, L.; Christensen, H.; Haunton, V.J.; et al. COVID-19 in older people: A rapid clinical review. Age Aging 2020, 49, 501–515. [Google Scholar] [CrossRef]
- Zunzunegui, M.A. COVID-19 en centros residenciales de personas mayores: La equidad será necesaria para evitar nuevas catástrofes [COVID-19 in care homes: Equity will be needed to avoid new catastrophes]. Gac. Sanit. 2022, 36, 3–5. [Google Scholar] [CrossRef]
- Vaqué Rafart, J. Síndrome respiratorio agudo grave (SARS). An. Pediatr. 2005, 62, 6–11. [Google Scholar]
- Bratanich, A. MERS-CoV: Transmisión y el papel de nuevas especies hospederas [MERS-CoV, transmisión and the role of new host species]. Rev. Argent. Microbiol. 2015, 47, 279–281. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med. Res. Methodol. 2018, 18, 5. [Google Scholar] [CrossRef] [Green Version]
- Saturno, P.J. Diseño de Procesos. Método IDEFØ. Mapa de Procesos de una Organización. Manual del Máster en Gestión de la Calidad en Los Servicios de Salud. Módulo 5: Métodos y Herramientas Para el Diseño de la Calidad. Protocolización de Actividades Clínicas y Diseño de Procesos. Unidad Temática 30, 2nd ed.; Universidad de Murcia: Murcia, Spain, 2008; ISBN 978-84-8371-756-1. [Google Scholar]
- Vijh, R.; Prairie, J.; Otterstatter, M.; Hu, Y.; Hayden, A.; Yau, B.; Daly, P.; Lysyshyn, M.; McKee, G.; Harding, J.; et al. Evaluation of a multisectoral intervention to mitigate the risk of severe acute respiratory coronavirus virus 2 (SARS-CoV-2) transmission in long-term care facilities. Infect. Control Hosp. Epidemiol. 2021, 42, 1181–1188. [Google Scholar] [CrossRef] [PubMed]
- Morales, E.N.; Viana, L.G.; Resende, L.M.; Vasconcellos, L.S.; Moura, A.S.; Menezes, A.; Mansano, N.H.; Rabelo, R. COVID-19 in long-term care facilities for the elderly: Laboratory screening and disease dissemination prevention strategies. Cienc. Saude Coletiva 2020, 25, 3445–3458. [Google Scholar] [CrossRef]
- Schrodt, C.A.; Malenfant, J.H.; Hunter, J.C.; Slifka, K.J.; Campbell, A.; Stone, N.; Whitehouse, E.R.; Wittry, B.; Christensen, B.; Barnes, J.R.; et al. Investigation of a Suspect Severe Acute Respiratory Syndrome Coronavirus-2 and Influenza A Mixed Outbreak: Lessons Learned for Long-Term Care Facilities Nationwide. Clin. Infect. Dis. 2021, 73, S77–S80. [Google Scholar] [CrossRef] [PubMed]
- Dys, S.; Winfree, J.; Carder, P.; Zimmerman, S.; Thomas, K.S. Coronavirus Disease 2019 Regulatory Response in United States-Assisted Living Communities: Lessons Learned. Front. Public Health 2021, 9, 661042. [Google Scholar] [CrossRef] [PubMed]
- Luzón Oliver, L.; Molina Pérez de Los Cobos, E.; Novoa Jurado, A.; Pérez Martínez, E.; Martínez Monreal, D.; Grupo CORECAAS. La seguridad del paciente en las residencias sociosanitarias. La experiencia de la Comunidad Autónoma de la Región de Murcia [Patient safety in nursing homes. The experience of the Autonomous Community of the Region of Murcia]. Aten. Primaria 2021, 53, 102228. [Google Scholar] [CrossRef]
- Alawi, M.M. Successful management of COVID-19 outbreak in a long-term care facility in Jeddah, Saudi Arabia: Epidemiology, challenges for prevention and adaptive management strategies. J. Infect. Public Health 2021, 14, 521–526. [Google Scholar] [CrossRef]
- Bernabeu-Wittel, M.; Ternero-Vega, J.E.; Nieto-Martín, M.D.; Moreno-Gaviño, L.; Conde-Guzmán, C.; Delgado-Cuesta, J.; Rincón-Gómez, M.; Díaz-Jiménez, P.; Giménez-Miranda, L.; Lomas-Cabezas, J.M.; et al. Effectiveness of a On-site Medicalization Program for Nursing Homes With COVID-19 Outbreaks. J. Gerontol. A Biol. Med. Sci. 2021, 76, 19–27. [Google Scholar] [CrossRef]
- Shrader, C.D.; Assadzandi, S.; Pilkerton, C.S.; Ashcraft, A.M. Responding to a COVID-19 Outbreak at a Long-Term Care Facility. J. Appl. Gerontol. 2021, 40, 14–17. [Google Scholar] [CrossRef]
- Japan Geriatrics Society Subcommittee on End-of-Life Issues and New Coronavirus Countermeasure Team; Kuzuya, M.; Aita, K.; Katayama, Y.; Katsuya, T.; Nishikawa, M.; Hirahara, S.; Miura, H.; Yanagawa, M.; Arai, H.; et al. The Japan Geriatrics Society consensus statement “recommendations for older persons to receive the best medical and long-term care during the COVID-19 outbreak—Considering the timing of advance care planning implementation”. Geriatr. Gerontol. Int. 2020, 20, 1112–1119. [Google Scholar] [CrossRef]
- Garibaldi, P.M.; Ferreira, N.N.; Moraes, G.R.; Mourac, J.C.; Espósito, D.L.; Volpe, G.J.; Caladoe, R.T.; Fonsecad, B.A.; Borges, M.C. Efficacy of COVID-19 outbreak management in a skilled nursing facility based on serial testing for early detection and control. Braz. J. Infect. Dis. 2021, 25, 101570. [Google Scholar] [CrossRef]
- Sacco, G.; Foucault, G.; Briere, O.; Annweiler, C. COVID-19 in seniors: Findings and lessons from mass screening in a nursing home. Maturitas 2020, 141, 46–52. [Google Scholar] [CrossRef]
- Escobar, D.J.; Lanzi, M.; Saberi, P.; Love, R.; Linkin, D.R.; Kelly, J.J.; Jhala, D.; Amorosa, V.; Hofmann, M.; Doyon, J.B. Mitigation of a Coronavirus Disease 2019 Outbreak in a Nursing Home Through Serial Testing of Residents and Staff. Clin. Infect. Dis. 2021, 72, e394–e396. [Google Scholar] [CrossRef] [PubMed]
- Murti, M.; Goetz, M.; Saunders, A.; Sunil, V.; Guthrie, J.L.; Eshaghi, A.; Zittermann, S.; Teatero, S.; Fittipaldi, N.; Rilkoff, H.; et al. Investigation of a severe SARS-CoV-2 outbreak in a long-term care home early in the pandemic. CMAJ 2021, 193, E681–E688. [Google Scholar] [CrossRef] [PubMed]
- Louie, J.K.; Scott, H.M.; DuBois, A.; Sturtz, N.; Lu, W.; Stoltey, J.; Masinde, G.; Cohen, S.; Sachdev, D.; Philip, S.; et al. Lessons From Mass-Testing for Coronavirus Disease 2019 in Long-Term Care Facilities for the elderly in San Francisco. Clin. Infect. Dis. 2021, 72, 2018–2020. [Google Scholar] [CrossRef] [PubMed]
- Morales Viera, A.; Rivas Rodriguez, R.; Otero Aguilar, P.; Briones Pérez de Blanca, E. Epidemiology of COVID-19 among health personnel in long-term care centers in Seville. Rev. Clin. Esp. 2022, 222, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.C.; Barbu, M.G.; Beiu, C.; Popa, L.G.; Mihai, M.M.; Berteanu, M.; Popescu, M.N. The Impact of COVID-19 Pandemic on Long-Term Care Facilities Worldwide: An Overview on International Issues. BioMed Res. Int. 2020, 2020, 8870249. [Google Scholar] [CrossRef]
- Zimmerman, S.; Dobbs, D.; Roth, E.G.; Goldman, S.; Peeples, A.D.; Wallace, B. Promoting and Protecting Against Stigma in Assisted Living and Nursing Homes. Gerontologist 2016, 56, 535–547. [Google Scholar] [CrossRef] [Green Version]
- Seshadri, S.; Concannon, C.; Woods, J.A.; McCullough, K.M.; Dumyati, G.K. “It’s like fighting a war with rocks”: Nursing home healthcare workers’ experiences during the COVID-19 pandemic. Infect. Control Hosp. Epidemiol. 2021, 42, 1020–1021. [Google Scholar] [CrossRef]
- Rassouli, M.; Ashrafizadeh, H.; Shirinabadi Farahani, A.; Akbari, M.E. COVID-19 Management in Iran as One of the Most Affected Countries in the World: Advantages and Weaknesses. Front. Public Health 2020, 8, 510. [Google Scholar] [CrossRef]
- Hado, E.; Friss Feinberg, L. Amid the COVID-19 Pandemic, Meaningful Communication between Family Caregivers and Residents of Long-Term Care Facilities is Imperative. J. Aging Soc. Policy 2020, 32, 410–415. [Google Scholar] [CrossRef]
- Van der Ploeg, E.S.; Eppingstall, B.; O’Connor, D.W. Internet video chat (Skype) family conversations as a treatment of agitation in nursing home residents with dementia. Int. Psychogeriatr. 2016, 28, 697–698. [Google Scholar] [CrossRef] [PubMed]
- Van der Roest, H.G.; Prins, M.; van der Velden, C.; Steinmetz, S.; Stolte, E.; van Tilburg, T.G.; de Vries, D.H. The Impact of COVID-19 Measures on Well-Being of Older Long-Term Care Facility Residents in the Netherlands. J. Am. Med. Dir. Assoc. 2020, 21, 1569–1570. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Veiga, P.; Sanchoa, M.; García, A.; Rivas, E.; Abad, E.; Suárez, N.; Mondragón, G.; Buiza, C.; Orbegozo, A.; Yangua, J. Efectos del Modelo de Atención Centrado en la Persona en la calidad de vida de personas con deterioro cognitivo de centros gerontológicos [Effects from the Person Centered-Care Model on quality of life of cognitive impaired persons from gerontological centers]. Rev. Esp. Geriatr. Gerontol. 2014, 49, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Pascual López, J.A.; Gil Pérez, T.; Sánchez, J.A.; Menárguez Puche, J.F. Cuestionarios de atención centrada en la persona en atención primaria. Una revisión sistemática [Questionnaires of person centered care in primary care. A systematic review]. Aten. Primaria 2020, 52, 738–749. [Google Scholar] [CrossRef] [PubMed]
- Avidor, S.; Ayalon, L. “I Didn’t Meet My Mother; I Saw My Mother”: The Challenges Facing Long-Term Care Residents and Their Families in the Age of COVID-19. J. Appl. Gerontol. 2022, 41, 22–29. [Google Scholar] [CrossRef]
- Tretteteig, S.; Eriksen, S.; Hillestad, A.H.; Julnes, S.G.; Lichtwarck, B.; Nilsen, A.; Rokstad, A.M. The Experience of Relatives of Nursing Home Residents with COVID-19: A Qualitative Study. Nurs. Res. Rev. 2022, 12, 17–27. [Google Scholar] [CrossRef]
- Vellani, S.; Boscart, V.; Escrig-Pinol, A.; Cumal, A.; Krassikova, A.; Sidani, S.; Zheng, N.; Yeung, L.; McGilton, K.S. Complexity of Nurse Practitioners’ Role in Facilitating a Dignified Death for Long-Term Care Home Residents during the COVID-19 Pandemic. J. Pers. Med. 2021, 11, 433. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Sinsky, C. From triple to quadruple aim: Care of the patient requires care of the provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Frutos, C.; Gómez-Salgado, J. Efectos de la pandemia por COVID-19 en la salud mental de la población trabajadora [Effects of the Covid-19 Pandemic on Workers’ Mental Health]. Arch. Prev. Riesgos Labor. 2021, 24, 6–11. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Database | Search Strategy | Results |
|---|---|---|
| Science Direct | (learnings [Title/Abstract]) AND (long-term care [Title/Abstract]) AND ((SARS [Title/Abstract]) OR (MERS [Title/Abstract])) NOT (hospital [Title/Abstract]) | 93 |
| (lessons [Title/Abstract]) AND (long-term care [Title/Abstract])) AND ((SARS [Title/Abstract]) OR (MERS [Title/Abstract])) NOT (hospital [Title/Abstract]) | 44 | |
| ((positive learnings [Title/Abstract]) OR (positive lessons [Title/Abstract])) AND ((nursing homes [Title/Abstract])) OR (long-term care [Title/Abstract])) AND ((SARS [Title/Abstract]) OR (MERS [Title/Abstract])) NOT (hospital [Title/Abstract]) | 829 | |
| TOTAL | 966 | |
| ProQuest | ti (learnings) AND ti (nursing homes) OR ti (long-term care) AND ti (SARS) OR ti (MERS) NOT ti (hospital) | 700 |
| ti (lessons) AND ti (nursing homes) OR ti (long-term care) AND ti (SARS) OR ti (MERS) NOT ti (hospital) | 694 | |
| ti (positive learnings) OR ti (positive lessons) AND ti (nursing homes) OR ti (long-term care) AND ti (SARS) OR ti (MERS) NOT ti (hospital) | 878 | |
| TOTAL | 2272 | |
| PubMed | (learnings [Title/Abstract]) AND ((nursing homes [Title/Abstract])) OR (long-term care [Title/Abstract])) AND ((SARS [Title/Abstract]) OR (MERS [Title/Abstract])) NOT (hospital [Title/Abstract]) | 252 |
| (lessons [Title/Abstract]) AND ((nursing homes [Title/Abstract])) OR (long-term care [Title/Abstract])) AND ((SARS [Title/Abstract]) OR (MERS [Title/Abstract])) NOT (hospital [Title/Abstract]) | 252 | |
| ((positive learnings [Title/Abstract]) OR (positive lessons [Title/Abstract])) AND ((nursing homes [Title/Abstract])) OR (long-term care [Title/Abstract])) AND ((SARS [Title/Abstract]) OR (MERS [Title/Abstract])) NOT (hospital [Title/Abstract]) | 212 | |
| TOTAL | 716 | |
| Scopus | (TITLE-ABS-KEY (learnings) AND TITLE-ABS-KEY (nursing AND homes) OR TITLE-ABS-KEY (long-term AND care) AND TITLE-ABS-KEY (sars) OR TITLE-ABS-KEY (mers) AND NOT TITLE-ABS-KEY (hospital)) | 49 |
| (TITLE-ABS-KEY (lessons) AND TITLE-ABS-KEY (nursing AND homes) OR TITLE-ABS-KEY (long-term AND care) AND TITLE-ABS-KEY (sars) OR TITLE-ABS-KEY (mers) AND NOT TITLE-ABS-KEY (hospital)) | 47 | |
| (TITLE-ABS-KEY (positive AND learnings) OR TITLE-ABS-KEY (positive AND lessons) AND TITLE-ABS-KEY (nursing AND homes) OR TITLE-ABS-KEY (long-term AND care) AND TITLE-ABS-KEY (sars) OR TITLE-ABS-KEY (mers) AND NOT TITLE-ABS-KEY (hospital)) | 11 | |
| TOTAL | 101 | |
| Embase | ((learnings:ab,ti AND ‘nursing homes’:ab,ti OR ‘long-term care’:ab,ti) AND sars:ab,ti OR mers:ab,ti) NOT hospital:ab,ti | 824 |
| ((lessons:ab,ti AND ‘nursing homes’:ab,ti OR ‘long-term care’:ab,ti) AND sars:ab,ti OR mers:ab,ti) NOT hospital:ab,ti | 824 | |
| ((‘positive learnings’:ab,ti OR ‘positive lessons’:ab,ti OR ‘nursing homes’:ab,ti OR ‘long-term care’:ab,ti) AND sars:ab,ti OR mers:ab,ti) NOT hospital:ab,ti | 824 | |
| TOTAL | 2472 | |
| TOTAL | 6527 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Payá, M.; Carrillo, I.; Guilabert, M. Lessons Learned from the COVID-19 Pandemic in Nursing Homes: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 16919. https://doi.org/10.3390/ijerph192416919
Martínez-Payá M, Carrillo I, Guilabert M. Lessons Learned from the COVID-19 Pandemic in Nursing Homes: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(24):16919. https://doi.org/10.3390/ijerph192416919
Chicago/Turabian StyleMartínez-Payá, Marina, Irene Carrillo, and Mercedes Guilabert. 2022. "Lessons Learned from the COVID-19 Pandemic in Nursing Homes: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 24: 16919. https://doi.org/10.3390/ijerph192416919