
Exploring the Digital Divide among the Bhutanese Refugee Community during COVID-19: Engaged Research in Action
 ,
,
Abstract
:1. Introduction
1.1. The Bhutanese Refugee Community
1.2. Critical Public Health Needs
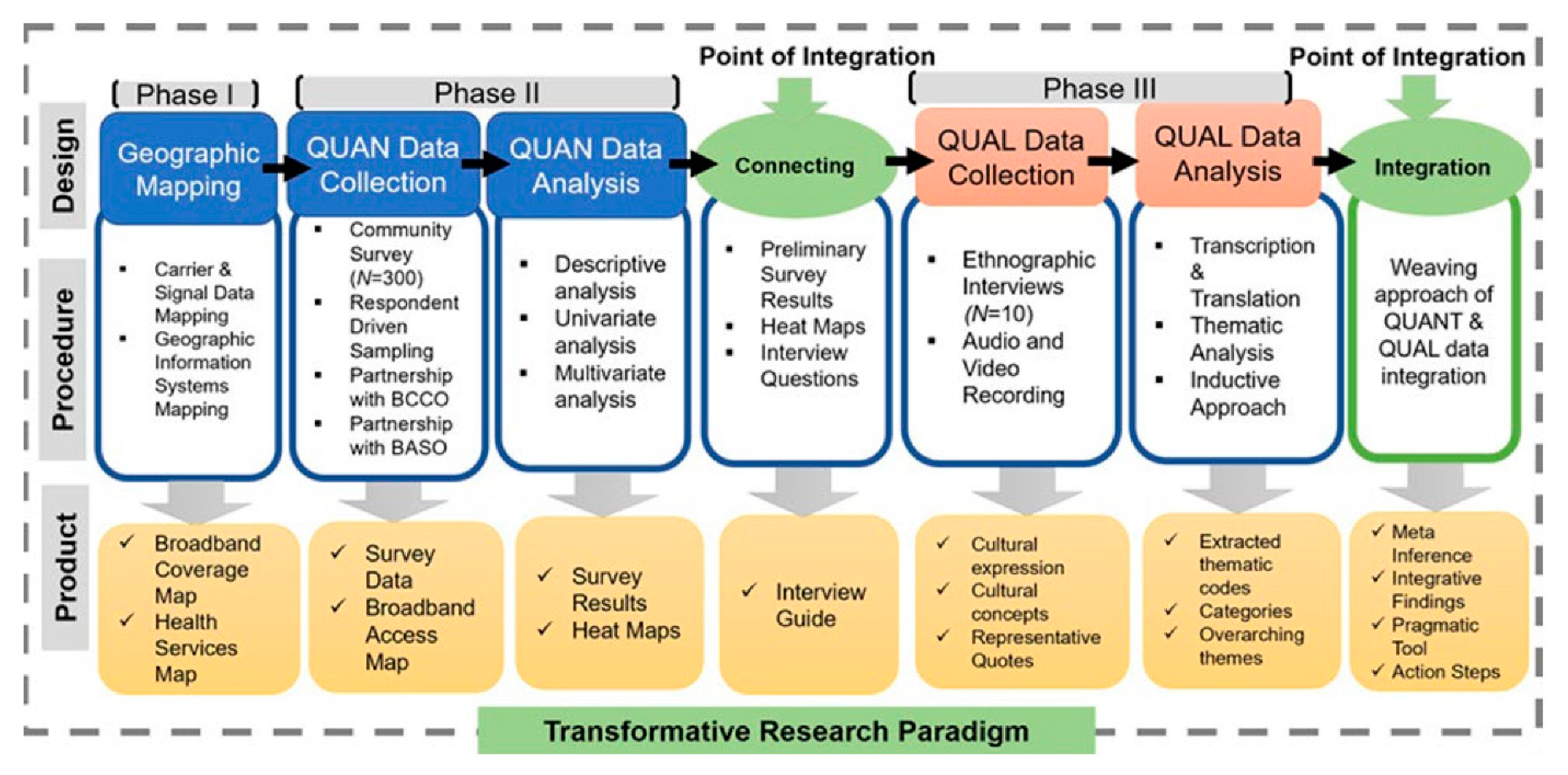
2. Materials and Methods
Research Approach
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Digital Inclusion Alliance. Available online: https://www.digitalinclusion.org/definitions/ (accessed on 16 November 2022).
- Sanders, C.K.; Scanlon, E. The Digital Divide Is a Human Rights Issue: Advancing Social Inclusion Through Social Work Advocacy. J. Hum. Rights Soc. Work 2021, 6, 130–143. [Google Scholar] [CrossRef] [PubMed]
- Sieck, C.J.; Sheon, A.; Ancker, J.S.; Castek, J.; Callahan, B.; Siefer, A. Digital inclusion as a social determinant of health. NPJ Digit. Med. 2021, 4, 52. [Google Scholar] [CrossRef] [PubMed]
- Ragnedda, M.; Muschert, G.W. The Digital Divide: The Internet and Social Inequality in International Perspective; Taylor & Francis: Oxfordshire, UK, 2013. [Google Scholar]
- van Dijk, J. The Digital Divide; Polity Press: Boston, MA, USA, 2020. [Google Scholar]
- Seckler, M.; Heinz, S.; Forde, S.; Tuch, A.N.; Opwis, K. Trust and distrust on the web: User experiences and website characteristics. Comput. Hum. Behav. 2015, 45, 39–50. [Google Scholar] [CrossRef]
- Zulman, D.M.; Kirch, M.; Zheng, K.; An, L.C. Trust in the internet as a health resource among older adults: Analysis of data from a nationally representative survey. J. Med. Internet Res. 2011, 13, e19. [Google Scholar] [CrossRef]
- Prieger, J.E. The broadband digital divide and the benefits of mobile broadband for minorities. J. Econ. Inequal. 2015, 13, 373–400. [Google Scholar] [CrossRef]
- Prieger, J.E.; Hu, W.-M. The broadband digital divide and the nexus of race, competition, and quality. Inf. Econ. Policy 2008, 20, 150–167. [Google Scholar] [CrossRef] [Green Version]
- Gurung, N.; Baidya, P.B. A Fresh Start: Refugees from Bhutan Arrive in the UK UNHCR. 2010. Available online: https://www.unhcr.org/en-us/news/latest/2010/8/4c6026059/fresh-start-refugees-bhutan-arrive-uk.html (accessed on 16 November 2022).
- Roka, K. Adjusting to the New World: A Study of Bhutanese Refugees’ Adaptation in the US. J. Soc. Soc. Work 2017, 5, 98–108. [Google Scholar] [CrossRef] [Green Version]
- Bhatta, M.; Assad, L.; Shakya, S. Socio-Demographic and Dietary Factors Associated with Excess Body Weight and Abdominal Obesity among Resettled Bhutanese Refugee Women in Northeast Ohio, United States. Int. J. Environ. Res. Public Health 2014, 11, 6639–6652. [Google Scholar] [CrossRef]
- Adhikari, D. Healthcare and happiness in the Kingdom of Bhutan. Singap. Med. J. 2016, 57, 107–109. [Google Scholar] [CrossRef] [Green Version]
- Vonnahme, L.A.; Lankau, E.W.; Ao, T.; Shetty, S.; Cardozo, B.L. Factors Associated with Symptoms of Depression among Bhutanese Refugees in the United States. J. Immigr. Minor. Health 2015, 17, 1705–1714. [Google Scholar] [CrossRef]
- Maleku, A.; Kim, Y.K.; Kagotho, N.; Lim, Y. Expanding the transformative explanatory sequential mixed methods design archetype in a cross-cultural context: The polemics of African refugee livelihoods in places of resettlement. J. Mix. Methods Res. 2021, 15, 212–239. [Google Scholar] [CrossRef]
- Soukenik, E.; Haran, H.; Kirsch, J.; Pyakurel, S.; Maleku, A. Barriers and Facilitators of Mental Health Service Utilisation among Bhutanese Refugees in the USA: Findings from a Mixed-Methods Study. Br. J. Soc. Work 2021, 52, 1552–1576. [Google Scholar] [CrossRef]
- Romero, M. Sociology Engaged in Social Justice. Am. Sociol. Rev. 2020, 85, 1–30. [Google Scholar] [CrossRef]
- Scharrer, E.; Ramasubramanian, S. Quantitative Research Methods in Communication: The Power of Numbers for Social Justice; Routledge: London, UK, 2020. [Google Scholar]
- Mertens, D.M. Transformative Paradigm: Mixed Methods and Social Justice. J. Mix. Methods Res. 2007, 1, 212–225. [Google Scholar] [CrossRef]
- Buick, F.; Blackman, D.; O’Flynn, J.; O’Donnell, M.; West, D. Effective Practitioner–Scholar Relationships: Lessons from a Coproduction Partnership. Public Adm. Rev. 2016, 76, 35–47. [Google Scholar] [CrossRef]
- Cooke, J.; Langley, J.; Wolstenholme, D.; Hampshaw, S. “Seeing” the Difference: The Importance of Visibility and Action as a Mark of “Authenticity” in Co-production Comment on “Collaboration and Co-production of Knowledge in Healthcare: Opportunities and Challenges”. Int. J. Health Policy Manag. 2017, 6, 345–348. [Google Scholar] [CrossRef] [Green Version]
- Lai, J.; Widmar, N.O. Revisiting the Digital Divide in the COVID-19 Era. Appl. Econ. Perspect. Policy 2021, 43, 458–464. [Google Scholar] [CrossRef]
- Maleku, A.; Soukenik, E.; Haran, H.; Kirsch, J.; Pyakurel, S. Conceptualizing mental health through the Bhutanese refugee lens: Findings from a mixed methods study. Community Ment. Health J. 2022, 58, 376–393. [Google Scholar] [CrossRef]
- Talegawkar, S.A.; Jin, Y.; Kandula, N.R.; Kanaya, A.M. Associations between Cumulative Biological Risk and Subclinical Atherosclerosis in Middle- and Older-Aged South Asian Immigrants in the United States. J. Asian Health 2021, 1, e202104. [Google Scholar]
- Reddick, C.G.; Enriquez, R.; Harris, R.J.; Sharma, B. Determinants of broadband access and affordability: An analysis of a community survey on the digital divide. Cities 2020, 106, 102904. [Google Scholar] [CrossRef]
- Dutton, W.H.; Reisdorf, B.C. Cultural divides and digital inequalities: Attitudes shaping Internet and social media divides. Inf. Commun. Soc. 2019, 22, 18–38. [Google Scholar] [CrossRef]
- Ridderbos, K. Last Hope: The Need for Durable Solutions for Bhutanese Refugees in Nepal and India; Human Rights Watch: New York, NY, USA, 2007; Volume 19, Available online: https://www.hrw.org/sites/default/files/reports/bhutan0507webwcover.pdf (accessed on 16 November 2022).
- Nelson, A.; Stam, K. Bhutanese or Nepali? The Politics of Ethnonym Ambiguity. South Asia J. South Asian Stud. 2021, 44, 772–789. [Google Scholar] [CrossRef]
- Pulla, V.; Rai, D. Resettlement Perspectives of Bhutanese Refugees: A Place Called Home with a Future. In The Lhotsampa People of Bhutan: Resilience and Survival; Pulla, V., Ed.; Palgrave Macmillan US: New York, NY, USA, 2016; pp. 79–93. [Google Scholar]
- Watson, F. Identifying a Lhotshampa Identity: An Exploration of the Experience of Expulsion and Ongoing Third Country Resettlement among the Bhutanese Refugees. Ph.D. Thesis, Mount Allison University, Sackville, NB, Canada, 2012. [Google Scholar]
- Pulla, V.; Dhungel, O. Settlement Planning for Refugees: Australia and the United States. In The Lhotsampa People of Bhutan: Resilience and Survival; Pulla, V., Ed.; Palgrave Macmillan US: New York, NY, USA, 2016; pp. 145–163. [Google Scholar]
- Rajesh, S.K. Bhutanese Refugees in Nepal: Survival and Prospects. Econ. Polit. Wkly. 2003, 38, 285–289. [Google Scholar]
- Ramsay, G. Impossible Refuge: The Control and Constraint of Refugee Futures; Taylor & Francis: Oxfordshire, UK, 2017. [Google Scholar]
- Shrestha-Ranjit, J.; Payne, D.; Koziol-McLain, J.; Crezee, I.; Manias, E. Availability, Accessibility, Acceptability, and Quality of Interpreting Services to Refugee Women in New Zealand. Qual. Health Res. 2020, 30, 1697–1709. [Google Scholar] [CrossRef] [PubMed]
- Subedi, B.; Maleku, A. Bhutanese–Nepali Young Women’s Experiences with Racism Inside and Outside of Schools. Educ. Stud. 2021, 57, 142–165. [Google Scholar] [CrossRef]
- Bhaskar, S.; Nurtazina, A.; Mittoo, S.; Banach, M.; Weissert, R. Editorial: Telemedicine During and Beyond COVID-19. Front. Public Health 2021, 9, 662617. [Google Scholar] [CrossRef]
- Disney, L.; Mowbray, O.; Evans, D. Telemental Health Use and Refugee Mental Health Providers Following COVID-19 Pandemic. Clin. Soc. Work J. 2021, 49, 463–470. [Google Scholar] [CrossRef]
- Koonin, L.M.; Hoots, B.; Tsang, C.A.; Leroy, Z.; Farris, K.; Jolly, T.; Antall, P.; McCabe, B.; Zelis, C.B.R.; Tong, I.; et al. Trends in the Use of Telehealth During the Emergence of the COVID-19 Pandemic—United States, January–March 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1595–1599. [Google Scholar] [CrossRef]
- Baum, A.; Kaboli, P.J.; Schwartz, M.D. Reduced In-Person and Increased Telehealth Outpatient Visits During the COVID-19 Pandemic. Ann. Intern. Med. 2021, 174, 129–131. [Google Scholar] [CrossRef]
- Truong, M.; Yeganeh, L.; Cook, O.; Crawford, K.; Wong, P.; Allen, J. Using telehealth consultations for healthcare provision to patients from non-Indigenous racial/ethnic minorities: A systematic review. J. Am. Med. Inform. Assoc. 2022, 29, 970–982. [Google Scholar] [CrossRef]
- Qian, F.; Hastings, J.F.; Ahmed, R. Overcoming telemental health disparities during the COVID-19 pandemic. Int. J. Qual. Health Care 2021, 33, mzab127. [Google Scholar] [CrossRef] [PubMed]
- Bhaskar, S.; Rastogi, A.; Menon, K.V.; Kunheri, B.; Balakrishnan, S.; Howick, J. Call for Action to Address Equity and Justice Divide During COVID-19. Front. Psychiatry 2020, 11, 559905. [Google Scholar] [CrossRef] [PubMed]
- Kienzler, H.; Spence, C.; Wenzel, T. A Culture-Sensitive and Person-Centered Approach: Understanding and Evaluating Cultural Factors, Social Background and History When Working with Refugees. In An Uncertain Safety: Integrative Health Care for the 21st Century Refugees; Wenzel, T., Drožđek, B., Eds.; Springer International Publishing: Cham, Switzerland; New York, NY, USA, 2019; pp. 101–116. [Google Scholar]
- Tankwanchi, A.S.; Bowman, B.; Garrison, M.; Larson, H.; Wiysonge, C.S. Vaccine hesitancy in migrant communities: A rapid review of latest evidence. Curr. Opin. Immunol. 2021, 71, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Montiel-Ishino, F.A.; Canenguez, K.M.; Cohen, J.H.; Needham, B.; Kandula, N.; Williams, F.; Shields, A.E.; Kanaya, A. Assessing profiles of cardiometabolic risk among South Asians living in the United States using a syndemic framework and acculturation. Circulation 2021, 143, A002. [Google Scholar] [CrossRef]
- Baum, F.; MacDougall, C.; Smith, D. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854–857. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Age group (N = 493) | ||
| 18–24 years | 161 | 32.7 |
| 25–44 years | 183 | 37.1 |
| 45–64 years | 104 | 21.1 |
| 65 years and older | 45 | 9.1 |
| Sex (N = 495) | ||
| Female | 240 | 48.5 |
| Male | 255 | 51.5 |
| Housing (N = 494) | ||
| Own a house | 341 | 69.0 |
| Rent a house | 48 | 9.7 |
| Rent an apartment | 90 | 18.2 |
| Other | 15 | 3.0 |
| Place of birth (N = 475) | ||
| Bhutan | 270 | 56.8 |
| Nepal | 195 | 41.1 |
| Other | 9 | 1.9 |
| Years of arrival in the US (N = 495) | ||
| 2002–2007 | 6 | 1.2 |
| 2008–2013 | 366 | 74.0 |
| 2014–2020 | 110 | 22.2 |
| Citizenship Status (N = 487) | ||
| Permanent Resident | 167 | 34.3 |
| US naturalized citizens | 317 | 64.0 |
| Other | 3 | 0.6 |
| Marital status (N = 491) | ||
| Single | 190 | 38.4 |
| Married | 270 | 54.5 |
| Separated | 6 | 1.2 |
| Divorced | 11 | 2.2 |
| Widowed | 14 | 2.8 |
| Religion (N = 489) | ||
| Hindu | 383 | 78.3 |
| Christian | 57 | 11.7 |
| Buddhist | 31 | 6.3 |
| Other | 18 | 3.6 |
| Ethnic Group (N = 491) | ||
| Dalit | 72 | 14.5 |
| Janajati | 76 | 15.3 |
| Chhetri & Brahmin | 307 | 62.5 |
| Other | 12 | 2.4 |
| Prefer not to answer | 24 | 4.9 |
| Language spoken at home (Multiple Choice) | ||
| Nepali | 489 | NA |
| English | 173 | NA |
| Hindi | 37 | NA |
| Education (N = 490) | ||
| No formal education | 120 | 24.5 |
| Primary level | 51 | 10.4 |
| High school or GED | 142 | 29.0 |
| College | 156 | 31.8 |
| Professional degree | 16 | 3.3 |
| Other | 5 | 1.0 |
| Employment status (N = 483) | ||
| Employed full-time | 243 | 50.3 |
| Employed part-time | 70 | 14.5 |
| Self-employed | 5 | 1.0 |
| Employed temporarily | 6 | 1.2 |
| Retired | 17 | 3.5 |
| Unemployed | 131 | 27.1 |
| Other | 11 | 2.3 |
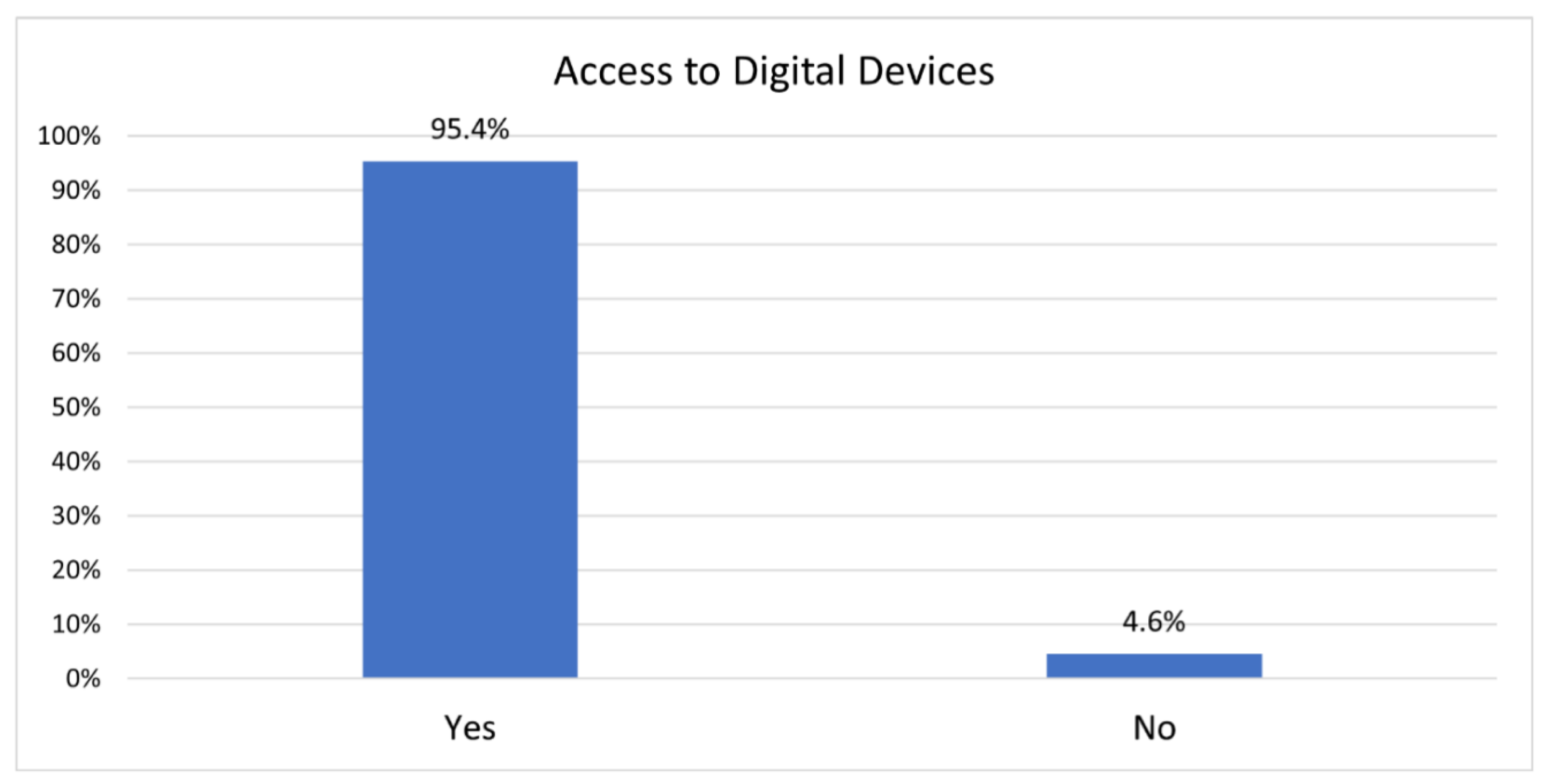
| Access to digital device (N = 482) | ||
| Yes | 460 | 95.4 |
| No | 22 | 4.6 |
| Annual family income (N = 463) | ||
| Under $15,000 | 75 | 16.2 |
| $15,000–24,999 | 80 | 17.3 |
| $25,000–34,999 | 116 | 25.1 |
| $35,000–49,999 | 82 | 17.7 |
| $50,000–74,999 | 70 | 15.1 |
| $75,000 and above | 40 | 8.6 |
| How Would You Rank Your Digital Technology Skills? | |||||
|---|---|---|---|---|---|
| Extremely Skilled | Very Skilled | Skilled | Not Very Skilled | Not Skilled | |
| n (%) | n (%) | n (%) | n (%) | n (%) | |
| Level of education | |||||
| No formal education | 1 (0.9) | 3 (2.6) | 23 (19.8) | 47 (40.5) | 42 (89.4) |
| Primary level | 1 (2.0) | 1 (2.0) | 17 (34.7) | 29 (59.2) | 1 (2.0) |
| High school or GED | 11 (7.9) | 28 (20.1) | 71 (51.1) | 27 (19.4) | 2 (1.4) |
| College | 49 (32.9) | 54 (36.2) | 42 (28.2) | 2 (1.3) | 2 (1.3) |
| Professional degree | 4 (26.7) | 6 (40.0) | 5 (33.3) | 0 (0) | 0 (0) |
| Vocational or other | 2 (40.0) | 0 (0) | 2 (40.0) | 1 (20.0) | 0 (0) |
| How Would You Rank Your Digital Technology Skills? | Access Internet at Home | Access to Digital Device | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Extremely Skilled | Very Skilled | Skilled | Not Very Skilled | Not Skilled | Never to Monthly | Weekly | Daily | No | Yes | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Age | ||||||||||
| 18–24 years | 47 (69.1) | 49 (53.3) | 45 (28.3) | 8 (7.6) | 5 (10.6) | 6 (17.1) | 10 (31.2) | 139 (34.0) | 3 (13.6) | 152 (33.2) |
| 25–44 years | 21 (30.9) | 32 (34.8) | 78 (49.1) | 39 (37.1) | 1 (2.1) | 11 (31.4) | 10 (31.2) | 153 (37.4) | 4 (18.2) | 172 (37.6) |
| 45–64 years | 0 (0) | 11 (11.9) | 31 (19.5) | 43 (41.0) | 16 (34.0) | 5 (14.3) | 6 (18.8) | 92 (22.5) | 2 (9.1) | 102 (22.3) |
| 65 years and older | 0 (0) | 0 (0) | 5 (3.1) | 15 (14.3) | 25 (53.2) | 13 (37.1) | 6 (18.8) | 25 (6.1) | 13 (59.1) | 32 (6.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cohen, J.H.; Maleku, A.; Pyakurel, S.; Suzuki, T.; Raut, S.; Montiel Ishino, F.A. Exploring the Digital Divide among the Bhutanese Refugee Community during COVID-19: Engaged Research in Action. Int. J. Environ. Res. Public Health 2022, 19, 16854. https://doi.org/10.3390/ijerph192416854
Cohen JH, Maleku A, Pyakurel S, Suzuki T, Raut S, Montiel Ishino FA. Exploring the Digital Divide among the Bhutanese Refugee Community during COVID-19: Engaged Research in Action. International Journal of Environmental Research and Public Health. 2022; 19(24):16854. https://doi.org/10.3390/ijerph192416854
Chicago/Turabian StyleCohen, Jeffrey H., Arati Maleku, Sudarshan Pyakurel, Taku Suzuki, Shambika Raut, and Francisco Alejandro Montiel Ishino. 2022. "Exploring the Digital Divide among the Bhutanese Refugee Community during COVID-19: Engaged Research in Action" International Journal of Environmental Research and Public Health 19, no. 24: 16854. https://doi.org/10.3390/ijerph192416854