

The Effect of Dentin Contamination by Topical Anesthetics on Micro-Shear Bond Strength: An In Vitro Experiment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study 1: Micro-Shear Bond Strengths through a Universal Testing Machine in Different Dentin Preparations
2.1.1. Tooth Specimen Preparation
2.1.2. Tooth Surface Preparation
ERC Group: Etch-and-Rinse Adhesive Applied to Non-Contaminated Dentin (Control Group)
ERS Group: Etch-and-Rinse Adhesive Applied to Dentin Contaminated with Topical Anesthetic Solution
ERG Group: Etch-and-Rinse Adhesive Applied to Dentin Contaminated with Topical Anesthetic Gel
SEC Group: Self-Etch Adhesive Applied to Non-Contaminated Dentin (Control Group)
SES Group: Self-Etch Adhesive Applied to Dentin Contaminated with Topical Anesthetic Solution
SEG Group: Self-Etch Adhesive Applied to Dentin Contaminated with Topical Anesthetic Gel
2.1.3. Micro-Shear Bond Strength Test
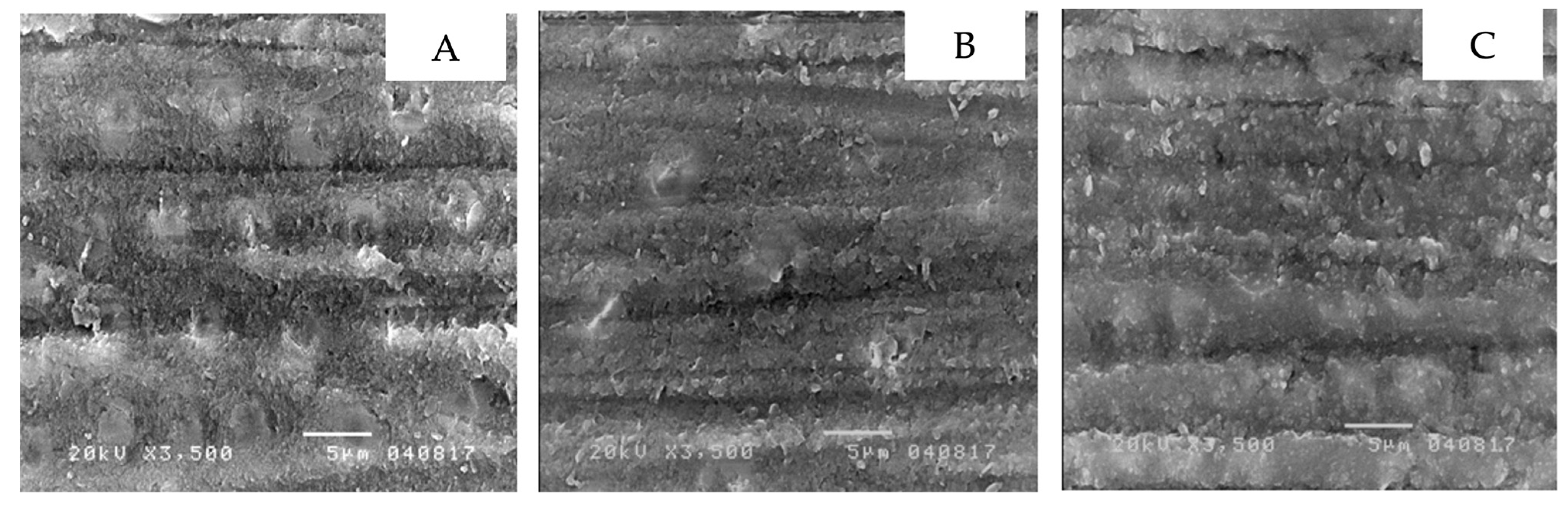
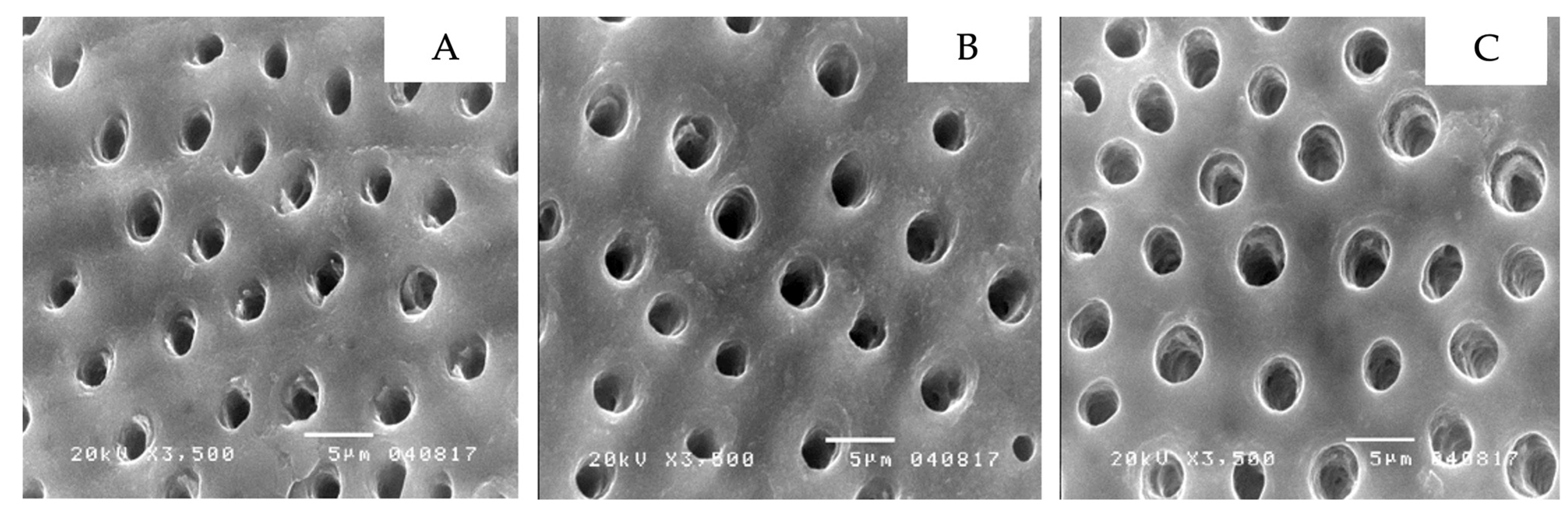
2.2. Study 2: Dentin Micro-Morphology through a Scanning Electron Microscope in Different Surface Preparations
- (1)
- Non-contaminated dentin
- (2)
- Non-contaminated dentin with 37.5 percent phosphoric acid applied on
- (3)
- Non-contaminated dentin with self-etching primer applied on
- (4)
- Dentin contaminated with topical anesthetic solution
- (5)
- Dentin contaminated with topical anesthetic solution and 37.5 percent phosphoric acid applied on
- (6)
- Dentin contaminated with topical anesthetic solution and self-etching primer applied on
- (7)
- Dentin contaminated with topical anesthetic gel
- (8)
- Dentin contaminated with topical anesthetic gel and 37.5 percent phosphoric acid applied on
- (9)
- Dentin contaminated with topical anesthetic gel and self-etching primer applied on
2.3. Statistical Analysis
2.4. Ethical Consideration
3. Results
3.1. Micro-Shear Bond Strengths in Different Dentin Preparations
3.2. Micro-Morphology of the Treated-Dentin Surfaces
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, H.S. Recent advances in topical anesthesia. J. Dent. Anesth. Pain Med. 2016, 16, 237–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, M.; Chawla, R.; Goyal, M. Topical anesthesia. J. Anaesthesiol. Clin. Pharmacol. 2015, 31, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, J.; Meechan, J.G.; Lawrence, H.P.; Grad, H.A.; Haas, D.A. Effect of time on clinical efficacy of topical anesthesia. Anesth. Prog. 2009, 56, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logothetis, D.D. Local Anesthesia for the Dental Hygienist-E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Berde, C.B.S.G. Local Anesthetics, 5th ed.; Churchill Livingstone: Philadelphia, PA, USA, 2000; pp. 491–521. [Google Scholar]
- Eakle, W.S.; Bastin, K.G. Dental Materials: Clinical Applications for Dental Assistants and Dental Hygienists; Elsevier Health Sciences: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Bonsor, S.J.; Pearson, G. A Clinical Guide to Applied Dental Materials; Elsevier Health Sciences: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Pashley, D.H.; Tay, F.R.; Breschi, L.; Tjäderhane, L.; Carvalho, R.M.; Carrilho, M.; Tezvergil-Mutluay, A. State of the art etch-and-rinse adhesives. Dent. Mater. 2011, 27, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Perdigão, J.; Reis, A.; Loguercio, A.D. Dentin adhesion and MMPs: A comprehensive review. J. Esthet. Restor. Dent. 2013, 25, 219–241. [Google Scholar] [CrossRef]
- Carrilho, E.; Cardoso, M.; Marques Ferreira, M.; Marto, C.M.; Paula, A.; Coelho, A.S. 10-MDP Based Dental Adhesives: Adhesive Interface Characterization and Adhesive Stability-A Systematic Review. Materials 2019, 12, 790. [Google Scholar] [CrossRef] [Green Version]
- Taskonak, B.; Sertgöz, A. Shear bond strengths of saliva contaminated ‘one-bottle’ adhesives. J. Oral Rehabil. 2002, 29, 559–564. [Google Scholar] [CrossRef]
- Koppolu, M.; Gogala, D.; Mathew, V.B.; Thangala, V.; Deepthi, M.; Sasidhar, N. Effect of saliva and blood contamination on the bond strength of self-etching adhesive system- An in vitro study. J. Conserv. Dent. 2012, 15, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Yoo, H.M.; Pereira, P.N. Effect of blood contamination with 1-step self-etching adhesives on microtensile bond strength to dentin. Oper. Dent. 2006, 31, 660–665. [Google Scholar] [CrossRef]
- Soares, C.J.; Branco, C.A.; Soares, P.B.F.; Fonseca, R.B.; Carlo, H.L.; Fernandes Neto, A.J. Effect of blood contamination during adhesive restorative procedures on dentin-resin cement shear bond strength. Braz. J. Oral Sci. 2016, 6, 1320–1325. [Google Scholar] [CrossRef]
- Erdogan, Y.; Karayilmaz, H.; Unal, M.; Gungor, O.; Ciftci, Z.Z. Effects of blood contamination and hemostatic agents on bond strength in primary teeth dentin. Niger. J. Clin. Pract. 2020, 23, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Kuphasuk, W.; Harnirattisai, C.; Senawongse, P.; Tagami, J. Bond strengths of two adhesive systems to dentin contaminated with a hemostatic agent. Oper. Dent. 2007, 32, 399–405. [Google Scholar] [CrossRef] [Green Version]
- Serra-Negra, J.; Paiva, S.M.; Oliveira, M.; Ferreira, E.; Freire-Maia, F.; Pordeus, I. Self-Reported Dental Fear among Dental Students and Their Patients. Int. J. Environ. Res. Public Health 2012, 9, 44–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayyan, M.R.; El Elagra, M.; Alqahtani, A.M.; Alhomoud, S.A.; Almutair, A.M.; Bin Razin, K.I.; Aldossary, M.F.; Alanazi, A.A. Stress levels among senior dental students in Saudi Arabia during fixed prosthodontics procedures. J. Fam. Med. Prim. Care 2022, 11, 1716–1720. [Google Scholar] [CrossRef]
- Shimada, Y.; Yamaguchi, S.; Tagami, J. Micro-shear bond strength of dual-cured resin cement to glass ceramics. Dent. Mater. 2002, 18, 380–388. [Google Scholar] [CrossRef]
- Roberts, H.W.; Vandewalle, K.S.; Charlton, D.G.; Leonard, D.L. Effect of handpiece maintenance method on bond strength. Oper. Dent. 2005, 30, 528–532. [Google Scholar]
- Townsend, R.D.; Dunn, W.J. The effect of saliva contamination on enamel and dentin using a self-etching adhesive. J. Am. Dent. Assoc. 2004, 135, 895–901, quiz 1036, 1038. [Google Scholar] [CrossRef]
- Chen, L.; Hammond, B.D.; Alex, G.; Suh, B.I. Effect of silane contamination on dentin bond strength. J. Prosthet. Dent. 2017, 117, 438–443. [Google Scholar] [CrossRef]
- Soontornvatin, V.; Prasansuttiporn, T.; Thanatvarakorn, O.; Jittidecharaks, S.; Hosaka, K.; Foxton, R.M.; Nakajima, M. Bond strengths of three-step etch-and-rinse adhesives to silane contaminated dentin. Dent. Mater. J. 2021, 40, 385–392. [Google Scholar] [CrossRef]
- Luz, M.; Netto, N.G.; Arana-Chavez, V. SEM study of different treatments of the smear layer on different cavity walls. Bull. GIRSO 2001, 43, 46–52. [Google Scholar]
- Beecham, G.B.; Bansal, P.; Nessel, T.A.; Goyal, A. Lidocaine. 2019. Available online: https://europepmc.org/article/nbk/nbk539881 (accessed on 1 March 2022).
- Prasad, K.D.; Hegde, C.; Agrawal, G.; Shetty, M. Gingival displacement in prosthodontics: A critical review of existing methods. J. Interdiscip. Dent. 2011, 1, 80–86. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Group | Etch-and-Rinse System | Self-Etch System |
|---|---|---|
| Non-contaminated dentin (control group) | ERC | SEC |
| Dentin contaminated with topical anesthetic solution | ERS | SES |
| Dentin contaminated with topical anesthetic gel | ERG | SEG |
| Scheme | Sum of Squares | df | Mean Squares | F | p-Value |
|---|---|---|---|---|---|
| Bonding | 7.64 | 1 | 7.64 | 0.153 | 0.697 |
| Contamination | 181.52 | 2 | 90.76 | 1.820 | 0.168 |
| Interaction (Bonding * Contamination) | 17.95 | 2 | 8.98 | 0.180 | 0.836 |
| Error | 4189.67 | 84 | 49.88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niyomsujarit, N.; Uttamang, P.; Burad, M.; Sipiyaruk, N.; Sipiyaruk, K. The Effect of Dentin Contamination by Topical Anesthetics on Micro-Shear Bond Strength: An In Vitro Experiment. Int. J. Environ. Res. Public Health 2022, 19, 16567. https://doi.org/10.3390/ijerph192416567
Niyomsujarit N, Uttamang P, Burad M, Sipiyaruk N, Sipiyaruk K. The Effect of Dentin Contamination by Topical Anesthetics on Micro-Shear Bond Strength: An In Vitro Experiment. International Journal of Environmental Research and Public Health. 2022; 19(24):16567. https://doi.org/10.3390/ijerph192416567
Chicago/Turabian StyleNiyomsujarit, Nattawit, Pathomrat Uttamang, Meghna Burad, Nadaprapai Sipiyaruk, and Kawin Sipiyaruk. 2022. "The Effect of Dentin Contamination by Topical Anesthetics on Micro-Shear Bond Strength: An In Vitro Experiment" International Journal of Environmental Research and Public Health 19, no. 24: 16567. https://doi.org/10.3390/ijerph192416567