

Comparison of Cardiorespiratory Fitness of Chinese Tibetan Adolescents with Their Han Counterparts: A Cross-Sectional Retrospective Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Measurements
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bultas, J. Mountain sickness. Cas. Lek. Cesk. 2015, 154, 280–286. [Google Scholar] [PubMed]
- Luks, A.M.; Swenson, E.R.; Bartsch, P. Acute high-altitude sickness. Eur. Respir. Rev. 2017, 26, 160096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartman-Ksycinska, A.; Kluz-Zawadzka, J.; Lewandowski, B. High altitude illness. Przegl. Epidemiol. 2016, 70, 490–499. [Google Scholar]
- Aldenderfer, M. Peopling the Tibetan plateau: Insights from archaeology. High Alt. Med. Biol. 2011, 12, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Bigham, A.W.; Wilson, M.J.; Julian, C.G.; Kiyamu, M.; Vargas, E.; Leon-Velarde, F.; Rivera-Chira, M.; Rodriquez, C.; Browne, V.A.; Parra, E.; et al. Andean and Tibetan patterns of adaptation to high altitude. Am. J. Hum. Biol. 2013, 25, 190–197. [Google Scholar] [CrossRef] [Green Version]
- Qi, X.; Cui, C.; Peng, Y.; Zhang, X.; Yang, Z.; Zhong, H.; Zhang, H.; Xiang, K.; Cao, X.; Wang, Y.; et al. Genetic evidence of paleolithic colonization and neolithic expansion of modern humans on the Tibetan plateau. Mol. Biol. Evol. 2013, 30, 1761–1778. [Google Scholar] [CrossRef] [Green Version]
- Gonggalanzi; Labasangzhu; Bjertness, E.; Wu, T.; Stigum, H.; Nafstad, P. Acute mountain sickness, arterial oxygen saturation and heart rate among Tibetan students who reascend to Lhasa after 7 years at low altitude: A prospective cohort study. BMJ Open 2017, 7, e16460. [Google Scholar]
- Dang, S.; Yan, H.; Yamamoto, S. High altitude and early childhood growth retardation: New evidence from Tibet. Eur. J. Clin. Nutr. 2008, 62, 342–348. [Google Scholar] [CrossRef] [Green Version]
- Weitz, C.A.; Garruto, R.M.; Chin, C.T.; Liu, J.C.; Liu, R.L.; He, X. Growth of Qinghai Tibetans living at three different high altitudes. Am. J. Phys. Anthropol. 2000, 111, 69–88. [Google Scholar] [CrossRef]
- Dang, S.; Yan, H.; Yamamoto, S.; Wang, X.; Zeng, L. Poor nutritional status of younger Tibetan children living at high altitudes. Eur. J. Clin. Nutr. 2004, 58, 938–946. [Google Scholar] [CrossRef]
- Yin, X.J.; Ji, C.Y. Malnutrition prevalence in Lasa Xizang children and adolescents. Biomed. Environ. Sci. 2014, 27, 614–626. [Google Scholar] [PubMed]
- Droma, T.; Mccullough, R.G.; Mccullough, R.E.; Zhuang, J.G.; Cymerman, A.; Sun, S.F.; Sutton, J.R.; Moore, L.G. Increased vital and total lung capacities in Tibetan compared to Han residents of Lhasa (3658 m). Am. J. Phys. Anthropol. 1991, 86, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, J.; Droma, T.; Sun, S.; Janes, C.; Mccullough, R.E.; Mccullough, R.G.; Cymerman, A.; Huang, S.Y.; Reeves, J.T.; Moore, L.G. Hypoxic ventilatory responsiveness in Tibetan compared with Han residents of 3658 m. J. Appl. Physiol. 1993, 74, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.H.; Ge, R.L.; Wang, X.Z.; Chen, H.X.; Wu, T.Y.; Kobayashi, T.; Yoshimura, K. Exercise performance of Tibetan and Han adolescents at altitudes of 3417 and 4300 m. J. Appl. Physiol. 1997, 83, 661–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianba; Berntsen, S.; Andersen, L.B.; Stigum, H.; Ouzhuluobu;Nafstad, P.; Wu, T.; Bjertness, E. Exercise capacity and selected physiological factors by ancestry and residential altitude: Cross-sectional studies of 9–10-year-old children in Tibet. High Alt. Med. Biol. 2014, 15, 162–169. [Google Scholar]
- Garruto, R.M.; Chin, C.T.; Weitz, C.A.; Liu, J.C.; Liu, R.L.; He, X. Hematological differences during growth among Tibetans and Han Chinese born and raised at high altitude in Qinghai, China. Am. J. Phys. Anthropol. 2003, 122, 171–183. [Google Scholar] [CrossRef]
- Weitz, C.A.; Garruto, R.M.; Chin, C.T. Larger fvc and fev1 among Tibetans compared to Han born and raised at high altitude. Am. J. Phys. Anthropol. 2016, 159, 244–255. [Google Scholar] [CrossRef]
- Niermeyer, S.; Yang, P.; Shanmina; Drolkar; Zhuang, J.; Moore, L.G. Arterial oxygen saturation in Tibetan and Han infants born in Lhasa, Tibet. N. Engl. J. Med. 1995, 333, 1248–1252. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, N.; Tomkinson, G.; Ekelund, U. Aerobic fitness and its relationship to sport, exercise training and habitual physical activity during youth. Br. J. Sports Med. 2011, 45, 849–858. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjostrom, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Buck, S.M.; Hillman, C.H.; Castelli, D.M. The relation of aerobic fitness to stroop task performance in preadolescent children. Med. Sci. Sports Exerc. 2008, 40, 166–172. [Google Scholar] [CrossRef]
- Rodriguez-Ayllon, M.; Cadenas-Sanchez, C.; Estevez-Lopez, F.; Munoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-Garcia, P.; Henriksson, H.; Mena-Molina, A.; Martinez-Vizcaino, V.; et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: A systematic review and meta-analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef]
- de Bruijn, A.; Hartman, E.; Kostons, D.; Visscher, C.; Bosker, R.J. Exploring the relations among physical fitness, executive functioning, and low academic achievement. J. Exp. Child Psychol. 2018, 167, 204–221. [Google Scholar] [CrossRef]
- Fan, C.; Sun, R.; Nie, M.; Wang, M.; Yao, Z.; Feng, Q.; Xu, W.; Yuan, R.; Gao, Z.; Cheng, Q.; et al. The cardiorespiratory fitness of children and adolescents in Tibet at altitudes over 3,500 meters. PLoS ONE 2021, 16, e256258. [Google Scholar] [CrossRef] [PubMed]
- Mayorga-Vega, D.; Aguilar-Soto, P.; Viciana, J. Criterion-related validity of the 20-m shuttle run test for estimating cardiorespiratory fitness: A meta-analysis. J. Sport. Sci. Med. 2015, 14, 536–547. [Google Scholar]
- Metsios, G.S.; Flouris, A.D.; Koutedakis, Y.; Nevill, A. Criterion-related validity and test-retest reliability of the 20m square shuttle test. J. Sci. Med. Sport 2008, 11, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Olds, T.; Tomkinson, G.; Leger, L.; Cazorla, G. Worldwide variation in the performance of children and adolescents: An analysis of 109 studies of the 20-m shuttle run test in 37 countries. J. Sports Sci. 2006, 24, 1025–1038. [Google Scholar] [CrossRef]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S. Temporal trends in the cardiorespiratory fitness of children and adolescents representing 19 high-income and upper middle-income countries between 1981 and 2014. Br. J. Sports Med. 2019, 53, 478–486. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Bi, C.; Yin, X.; Chen, Q.; Li, Y.; Liu, Y.; Zhang, T.; Li, M.; Sun, Y.; Yang, X. Physical fitness reference standards for chinese children and adolescents. Sci. Rep. 2021, 11, 4991. [Google Scholar] [CrossRef]
- Zhang, F.; Yin, X.; Bi, C.; Li, Y.; Sun, Y.; Zhang, T.; Yang, X.; Li, M.; Liu, Y.; Cao, J.; et al. Normative reference values and international comparisons for the 20-metre shuttle run test: Analysis of 69,960 test results among chinese children and youth. J. Sport. Sci. Med. 2020, 19, 478–488. [Google Scholar]
- Leger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical power analysis for the behavioral. Sciences 1988, 67, 1007. [Google Scholar]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S.; Dale, M.; Leblanc, A.G.; Belanger, K.; Ortega, F.B.; Leger, L. International normative 20 m shuttle run values from 1 142 026 children and youth representing 50 countries. Br. J. Sports Med. 2017, 51, 1545–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.; Bi, C.; Yin, X.; Chen, Q.; Liu, Y.; Li, Y.; Sun, Y.; Zhang, T.; Yang, X.; Li, M. Roles of age, sex, and weight status in the muscular fitness of Chinese Tibetan children and adolescents living at altitudes over 3600 m: A cross-sectional study. Am. J. Hum. Biol. 2022, 34, e23624. [Google Scholar] [CrossRef]
- Quan, C.; Li, Y.; Liu, X.; Wang, Y.; Ping, J.; Lu, Y.; Zhou, G. Characterization of structural variation in Tibetans reveals new evidence of high-altitude adaptation and introgression. Genome Biol. 2021, 22, 159. [Google Scholar] [CrossRef]
- Weinstein, K.J. Thoracic skeletal morphology and high-altitude hypoxia in andean prehistory. Am. J. Phys. Anthropol. 2007, 134, 36–49. [Google Scholar] [CrossRef]
- Fan, J.L.; Wu, T.Y.; Lovering, A.T.; Nan, L.; Bang, W.L.; Kayser, B. Differential brain and muscle tissue oxygenation responses to exercise in Tibetans compared to Han Chinese. Front. Physiol. 2021, 12, 617954. [Google Scholar] [CrossRef]
- Yangzong; Berntsen, S.; Bjertness, E.; Stigum, H.; Gonggalanzi; Bianba; Nafstad, P. Lung function among 9- to 10-year-old Tibetan and Han Chinese schoolchildren living at different altitudes in Tibet. High Alt. Med. Biol. 2013, 14, 31–36. [Google Scholar]



{kind=link}
{kind=link}
| Gender | Age (Years) | Sample Size | Chinese Han Adolescents Born and Raised at High Altitude | Sample Size | Chinese Tibetan Adolescents | Sample Size | Chinese Han Adolescents at Sea Level |
|---|---|---|---|---|---|---|---|
| Boys | 12 | 62 | 26 ± 8 | 77 | 29 ± 13 | 79 | 34 ± 15 |
| 13 | 63 | 27 ± 10 | 69 | 34 ± 16 | 66 | 42 ± 20 | |
| 14 | 64 | 35 ± 16 | 50 | 38 ± 18 | 88 | 48 ± 18 | |
| 15 | 58 | 35 ± 13 | 51 | 40 ± 14 | 75 | 53 ± 19 | |
| 16 | 76 | 36 ± 18 | 67 | 48 ± 21 | 78 | 49 ± 22 | |
| 17 | 61 | 34 ± 16 | 60 | 50 ± 20 | 95 | 49 ± 19 | |
| 18 | 68 | 31 ± 11 | 65 | 52 ± 25 | 75 | 48 ± 20 | |
| Girls | 12 | 67 | 30 ± 13 | 52 | 23 ± 7 | 67 | 27 ± 10 |
| 13 | 64 | 24 ± 14 | 58 | 27 ± 9 | 51 | 32 ± 12 | |
| 14 | 60 | 25 ± 16 | 56 | 24 ± 11 | 55 | 33 ± 10 | |
| 15 | 62 | 24 ± 10 | 69 | 26 ± 13 | 49 | 31 ± 11 | |
| 16 | 64 | 26 ± 10 | 63 | 30 ± 10 | 90 | 30 ± 10 | |
| 17 | 62 | 19 ± 7 | 71 | 30 ± 13 | 76 | 30 ± 9 | |
| 18 | 67 | 20 ± 8 | 56 | 33 ± 12 | 42 | 30 ± 12 |
| Age | Sample Size | Chinese Han Adolescents Born and Raised at High Altitude | Sample Size | Chinese Tibetan Adolescents | Sample Size | Chinese Han Adolescents at Sea Level | F | p | |
|---|---|---|---|---|---|---|---|---|---|
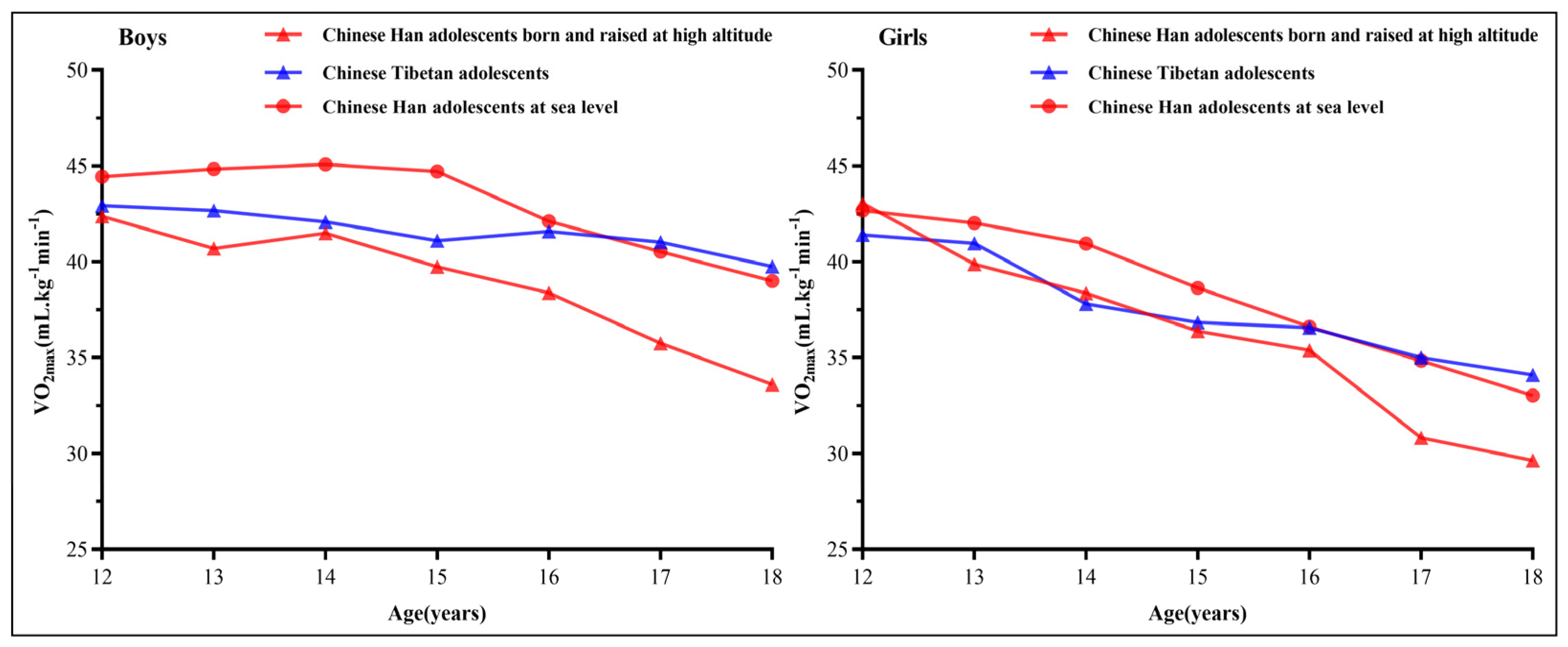
| 12 | 62 | 42.37 ± 2.38 | 77 | 42.93 ± 3.71 | 79 | 44.44 ± 4.37 bc | 6.213 | 0.002 | |
| 13 | 63 | 40.69 ± 2.96 | 69 | 42.67 ± 4.63 a | 66 | 44.84 ± 5.27 bc | 14.205 | 0.000 | |
| 14 | 64 | 41.50 ± 4.65 | 50 | 42.08 ± 5.29 | 88 | 45.07 ± 4.98 bc | 11.310 | 0.000 | |
| 15 | 58 | 39.73 ± 4.05 | 51 | 41.09 ± 3.77 | 75 | 44.71 ± 5.38 bc | 21.204 | 0.000 | |
| 16 | 76 | 38.37 ± 5.25 | 67 | 41.58 ± 6.32 a | 78 | 42.11 ± 6.10 b | 8.904 | 0.000 | |
| 17 | 61 | 35.74 ± 5.03 | 60 | 41.03 ± 6.17 a | 95 | 40.52 ± 5.53 b | 17.542 | 0.000 | |
| 18 | 68 | 33.60 ± 3.87 | 65 | 39.75 ± 7.83 a | 75 | 38.99 ± 5.61 b | 21.572 | 0.000 | |
| F | 37.749 | 2.586 | 16.504 | ||||||
| p | 0.000 | 0.018 | 0.000 |
| Age | Sample Size | Chinese Han Adolescents Born and Raised at High Altitude | Sample Size | Chinese Tibetan Adolescents | Sample Size | Chinese Han Adolescents at Sea Level | F | p | |
|---|---|---|---|---|---|---|---|---|---|
| 12 | 67 | 43.05 ± 3.89 | 52 | 41.40 ± 2.21 a | 67 | 42.67 ± 3.14 c | 4.114 | 0.018 | |
| 13 | 64 | 39.88 ± 4.22 | 58 | 40.97 ± 3.06 | 51 | 42.02 ± 3.58 b | 4.842 | 0.009 | |
| 14 | 60 | 38.36 ± 4.81 | 56 | 37.80 ± 3.80 | 55 | 40.96 ± 3.39 bc | 9.523 | 0.000 | |
| 15 | 62 | 36.38 ± 3.16 | 69 | 36.84 ± 4.47 | 49 | 38.63 ± 3.32 bc | 5.321 | 0.006 | |
| 16 | 64 | 35.39 ± 3.15 | 63 | 36.56 ± 3.82 | 90 | 36.61 ± 3.09 b | 2.925 | 0.056 | |
| 17 | 62 | 30.81 ± 2.53 | 71 | 35.00 ± 4.29 a | 76 | 34.84 ± 3.26 b | 30.586 | 0.000 | |
| 18 | 67 | 29.63 ± 3.02 | 56 | 34.09 ± 3.84 a | 42 | 33.02 ± 3.95 b | 26.156 | 0.000 | |
| F | 115.510 | 31.254 | 70.322 | ||||||
| p | 0.000 | 0.000 | 0.000 |
| Model | Independent Variable | B | Standard Error | β | t-Value | p-Value | B (95.0% CI) | |
|---|---|---|---|---|---|---|---|---|
| I | Constant Term | 64.863 | 0.743 | 87.271 | <0.01 | 63.406 | 66.320 | |
| Gender | −3.905 | 0.183 | −0.336 | −21.303 | <0.01 | −4.265 | −3.546 | |
| Age | −1.314 | 0.046 | −0.452 | −28.695 | <0.01 | −1.403 | −1.224 | |
| II | Constant Term | 66.125 | 0.723 | 91.479 | <0.01 | 64.707 | 67.542 | |
| Gender | −3.781 | 0.177 | −0.325 | −21.412 | <0.01 | −4.127 | −3.435 | |
| Age | −1.316 | 0.044 | −0.453 | −29.886 | <0.01 | −1.402 | −1.229 | |
| Chinese Han adolescents born and raised at high altitude | −3.178 | 0.213 | −0.257 | −14.913 | <0.01 | −3.596 | −2.760 | |
| Chinese Tibetan adolescents | −1.193 | 0.215 | −0.095 | −5.542 | <0.01 | −1.615 | −0.771 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, L.; Zhang, R.; Zhang, F.; Yin, X.; Liu, Y.; Guo, Y.; Sun, P. Comparison of Cardiorespiratory Fitness of Chinese Tibetan Adolescents with Their Han Counterparts: A Cross-Sectional Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 16526. https://doi.org/10.3390/ijerph192416526
Zhang L, Zhang R, Zhang F, Yin X, Liu Y, Guo Y, Sun P. Comparison of Cardiorespiratory Fitness of Chinese Tibetan Adolescents with Their Han Counterparts: A Cross-Sectional Retrospective Study. International Journal of Environmental Research and Public Health. 2022; 19(24):16526. https://doi.org/10.3390/ijerph192416526
Chicago/Turabian StyleZhang, Li, Ruming Zhang, Feng Zhang, Xiaojian Yin, Yuan Liu, Yaru Guo, and Pengwei Sun. 2022. "Comparison of Cardiorespiratory Fitness of Chinese Tibetan Adolescents with Their Han Counterparts: A Cross-Sectional Retrospective Study" International Journal of Environmental Research and Public Health 19, no. 24: 16526. https://doi.org/10.3390/ijerph192416526