

The Need for a Preparedness Training Model on Disaster Risk Reduction Based on Culturally Sensitive Public Health Nursing (PHN)


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Settings and Participants
2.3. Data Collection
2.4. Data Analysis
2.5. Ethical Considerations
2.6. Trustworthiness
3. Results
3.1. Document Analysis
3.2. Expert Discussions and National Seminar
- The implementation of the global target achievement of the Sendai Framework in Indonesia is carried out using the Disaster Risk Reduction (DRR) paradigm for the Disaster Resilient Village program.
- DRR is operated in the form of community empowerment.
- The steps for community empowerment in disaster management are identical to the community nursing process: assessment, diagnosis, planning, implementation, and evaluation.
- The PPNI Professional Organization believes that there is a need for community empowerment through guiding community nurses with structured disaster management training.
- Community-integrated training in disaster preparedness is needed as a DRR effort.
3.3. Focus Group Discussions (FGDs)
- The Sugih Mukti area is prone to disasters due to its geographical structure.
- No one in the community or its officials have participated in integrated disaster training in the health sector based on community needs.
- Government efforts have not been effective in community disaster management.
- A community development model in integrated disaster management that involves all components of society is needed.
- DRR efforts are not yet optimal
4. Discussion
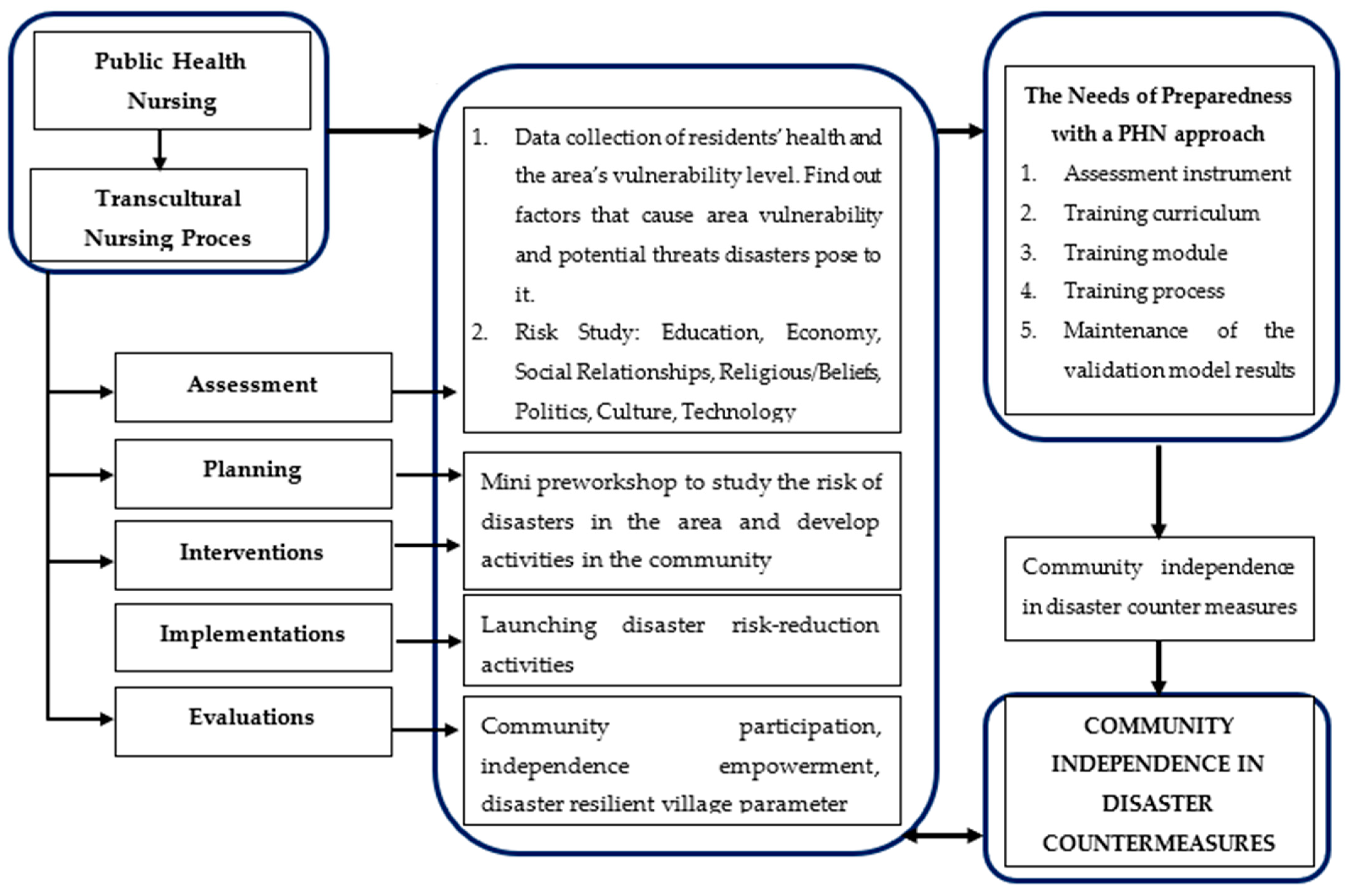
4.1. Description of Model Requirements
4.2. Constructed Model Requirements
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- BNPB. Rencana Nasional Penanggulangan Bencana 2020–2024; BNPB: Jakarta, Indonesia, 2019; pp. 1–115. Available online: https://bnpb.go.id/buku/rencana-nasional-penanggulangan-bencana-20202024 (accessed on 9 January 2022).
- BNPB. Indeks Risiko Bencana Indonesia (IRBI) Tahun 2020; BNPB: Jakarta, Indonesia, 2021; p. 199. Available online: https://inarisk.bnpb.go.id/pdf/BUKUIRBI2020KP.pdf (accessed on 5 March 2022).
- Suryotomo, P. Webinar “Peran Perawat dalam Kesiapsiagaan Bencana” oleh Persatuan Perawat Nasional Indonesia (PPNI) Tahun 2022 Kesiapsiagaan dan Peran Perawat dalam Menghadapi Bencana; PPNI: Jakarta, Indonesia, 2022. [Google Scholar]
- Adi, A.; Shalih, O.; Shabrina Fathia Rizqi, A.; Putra, A. Indeks Resiko Bencana Indonesia (IRBI) Tahun 2021; Yunus, R., Ed.; Pusat Data, Informasi dan Komunikasi Kebencanaan Badan Nasional Penanggulangan Bencana 1: Jakarta, Indonesia, 2021; Volume 1, pp. 8–11. Available online: https://inarisk.bnpb.go.id/pdf/BUKU%20IRBI%202021%20(PDF).pdf (accessed on 22 September 2022).
- Mcdonald, A.; Wilcox, T.; Aslam, P.; Pannawadee, S.; Janne, P.; Animesh, K.; Calle, I.T.; Amach, O. Disaster Risk Reduction in Indonesia; Spring: Berlin/Heidelberg, Germany, 2020; p. 40. [Google Scholar]
- Supriyanto Melilano, I.; Budianto, A.; Andreas, H.; Mariany, A.; Novianto, B. Jabar Resilience Culture Province (JRCP) Cetak Biru: Jawa barat Berbudaya Tangguh Bencana; JRCP: Bandung, Indonesia, 2021. [Google Scholar]
- BNPB. Kajian Risiko Bencana Nasional Provinsi Jawa Barat 2022–2026; BNPB: Jakarta, Indonesia, 2021.
- Badan Nasional Penanggulangan Bencana (BNPB). Rencana Nasional Penanggulangan Bencana 2015-2019 RINGKASAN EKSEKUTIF; BNPB: Jakarta, Indonesia, 2014; pp. 1–115. Available online: https://www.bnpb.go.id/documents/buku-renas-pb.pdf (accessed on 13 April 2022).
- Setiawan, A.; Sofyana, H.; Suhanda, P. Health Notions, Volume 1 Issue 1 (January–March 2017) ISSN 2580-4936 Empowering Village Cluster as Task Force in The Normalization of Disaster Victims ’ Physical Problems 22; Humanistic Network for Science and Technology Health Notions: Ponorogo, Indonesia, 2017; Volume 1, pp. 22–28. ISSN 2580-4936. [Google Scholar]
- Salasa, S.; Murni, T.W.; Emaliyawati, E. Pemberdayaan pada Kelompok Remaja melalui Pendekatan Contingency Planning dalam Meningkatkan Kesiapsiagaan terhadap Ancaman Kematian Akibat Bencana. J. Pendidik Keperawatan Indones. 2017, 3, 154–166. [Google Scholar] [CrossRef] [Green Version]
- Kulatunga, U. Impact of culture towards disaster risk reduction. Int. J. Strateg. Prop. Manag. 2010, 14, 304–313. [Google Scholar] [CrossRef] [Green Version]
- Marutani, M.; Kodama, S.; Harada, N. Japanese public health nurses’ culturally sensitive disaster nursing for small island communities. Isl. Stud. J. 2020, 15, 371–386. [Google Scholar] [CrossRef]
- Covan, E.K.; Fugate-Whitlock, E. Emergency planning and long-term care: Least paid, least powerful, most responsible. Health Care Women Int. 2010, 31, 1028–1043. [Google Scholar] [CrossRef] [PubMed]
- United Nations. 2009 UNISDR Terminologi on Disaster Risk Reductions. In Handbook of Rural Aging; Routledge: Oxfordshire, UK, 2021; pp. 111–115. [Google Scholar]
- Paton, D. Disaster risk reduction: Psychological perspectives on preparedness. Aust. J. Psychol. 2019, 71, 327–341. [Google Scholar] [CrossRef]
- Gonzalo, A. Madeleine Leininger: Transcultural Nursing Theory. 20191–26. Available online: https://nurseslabs.com/madeleine-leininger-transcultural-nursing-theory/ (accessed on 13 April 2022).
- Murdiyanti, D. Keperawatan Transkultural Pengetahuan Praktik Berdasarkan Budaya [Internet], 1st ed.; Elzha, E., Dianawati, L., Eds.; Keperawatan Transkultural; Pustaka Baru Press: Yogyakarta, Indonesia, 2017; pp. 285–287. Available online: http://repository.akperykyjogja.ac.id/102/1/BukuKeperawatanTranskulturalLengkap.pdf (accessed on 13 April 2022).
- Badriah, S. Model Keperawatan Keluarga Peka Budaya Sunda dalam meningkatkan Pengetahuan Keluarga dan menurunkan Kadar Hula darah Pada Diabetisi Lansia. J. Keperawatan Silampari 2021, 4, 6. [Google Scholar] [CrossRef]
- Amri, M.R.; Yulianti, G.; Yunus, R.; Wiguna, S.; Adi, A.W.; Ichwana, A.N.; Septian, R.T. Risiko Bencana Indonesia (Disasters Risk of Indonesia); Badan Nasional Penanggulangan Bencana: Jakarta, Indonesia, 2016; pp. 9–140.
- Ren, Z.J.; Wang, H.T.; Zhang, W. Experiences in disaster-related mental health relief work: An exploratory model for the interprofessional training of psychological relief workers. J. Interprof. Care 2017, 31, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Lebowitz, A.J. Community Collaboration as a Disaster Mental Health Competency: A Systematic Literature Review. Community Ment. Health J. 2015, 51, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Pourvakhshoori, N.; Norouzi, K.; Ahmadi, F.; Hosseini, M.; Khankeh, H. Nurse in limbo: A qualitative study of nursing in disasters in Iranian context. PLoS ONE 2017, 12, e0181314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmani, I.; Seyedin, H.; Ardalan, A.; Farajkhoda, T. Correction: Conceptual model of managing health care volunteers in disasters: A mixed method study. BMC Health Serv. Res. 2019, 19, 241. [Google Scholar] [CrossRef] [PubMed]
- Kertamuda, F.E.; Chris, H. Pasrah (Surrender) and Sabar (Patience) Among Indonesia Ethnics (Javanese, Sundanese, Betawi) Through Disaster: An Indigenous Psychological Analysis. In Proceedings of the HKICEPS 2012: 2012 Hong Kong International Conference on Education, Psychology and Society, Hong Kong, China, 14–16 December 2012. [Google Scholar]
- BPBD Kab Bandung. Profil BPBD Kabupaten Bandung. 2017. Available online: https://bpbd.jabarprov.go.id/bpbd-kabupaten-dan-kota/ (accessed on 13 April 2022).
- Geodipa, P.T. Profile PT Geodipa Enenrgi, 1st ed; Bandung, Indonesia, 2020; Available online: https://www.geodipa.co.id/ (accessed on 13 April 2022).
- Walsh, L.; Subbarao, I.; Gebbie, K.; Schor, K.W.; Lyznicki, J.; Strauss-Riggs, K.; Cooper, A.; Hsu, E.B.; King, R.V.; Mitas, J.A.; et al. Core competencies for disaster medicine and public health. Disaster Med. Public Health Prep. 2012, 6, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Gulzar, S.A.; Faheem, Z.A.; Somani, R.K. Role of community health nurse in earthquake affected areas. J. Pak. Med. Assoc. 2012, 62, 1083–1086. [Google Scholar] [PubMed]
- Rush, Z.; Depriest, K.; Mccauley, L. Climate Change-Related Hurricane Impact on Puerto Rico and the U.S. Virgin Islands, Environment Risk Reduction, and the Social Determinants of Health. Nurs. Econ. 2019, 37, 13–23. [Google Scholar]
- Ahmadi, S.; Khankeh, H.; Sahaf, R.; da Lvandi, A.; Hosseini, S.A. Daily life challenges in an earthquake disaster situation in older adults: A qualitative study in Iran. J. Clin. Diagn. Res. 2018, 12, IC08–IC12. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Data | Subthemes | Theme |
|---|---|---|
| “… The people of Sugih Mukti Village often experience disasters. Especially landslides and tropical cyclones” (Respondents: 1, 2, 4, 5, 10) “Well, we’re used to it, sir. Happens very often. Especially if you’ve heard the roar from the Geo Dipa Gas Production” (Respondents: 4, 5, 6) “The location is indeed close to the drilling center, not the production process itself but very close to Patuha Mountain, which makes small earthquakes and has volcanic activity” (Respondents: 1, 2, 3, 10) “… South Bandung Regency is prone to disasters because of geological and geographical factors…” (Respondents: 1, 2, 6, 10) “often sir, even though I’m new, we’re already used to the vibrations, not because of Geodipa,… Geodipa wants to help” (Respondents: 6, 7, 11) “We know the risks, but we just do not care, the government has thought of us, if we move where will we go?” (Respondents: 5, 11) “Once, sir, there was a hurricane, there were people whose houses were partially damaged, but most often there were landslides” (Respondents: 5, 11) “The hardest thing, sir, was a flash flood, sir, there were many victims, there were 13. Wow, at that time it was like the end of the world, I was not yet a village official, but I was bewildered, sir, the people were suffering” (Respondents: 4, 11) |
| Geographically, the Sugih Mukti area is prone to natural disasters |
| “I don’t know what to do if there is a landslide or flood, maybe because my house is far away, but other people also don’t know yet. Those who know if an earthquake is happening run away” (Resp: 4, 5, 11) “As government officials, we are always ready for orders, instructions from commanders, there are ‘babinsa’ (army officers) and village police who monitor general security, but if we are needed, we often go down ” (Resp: 1, 2, 3, 4, 6, 10) “The residents are only focused on finding a way to get food, sir, they don’t understand how to fight a disaster, if there’s a flood we flee, if there we hear rumbling noises we just let it go, the most important thing is to pray” (Resp: 4, 5, 11) “The government has tried to explain to villages, maybe not sugih mukti village, but other parties have done it, we will help and support” (Respondents: 4, 6, 10) “There are difficulties, sir, in educating the public like money, methods and government support, as well as those who have money… well the company. In order for them to want to help, they must be given consumption, food, transportation, etc.” (Respondents: 4, 5, 6, 9, 10) “As I see it, it’s not optimal yet. We are only limited to the health sector through cadres. As for disasters, we haven’t been able to do it” (Resp: 7, 8, 10) “it’s very important, sir, we are even ready to learn, to help, after all I guide this area” (Resp: 1, 2, 7, 8) “It’s time to do more. For example, COVID, sir. For the residents, it’s normal. If you get a fever, well you just compress your forehead with cloth, you lose your sense of smell, ah, just take village medicine, we give them bandrek, or a potion, no one wears a mask, so there’s no need, the most important thing is if you are able to eat” (Respondents: 6, 11) “The government officials are the ones who are the most responsible, the people are the citizens, we just follow the government’s advice” (Respondents: 5, 11) “We will support, we know that the community must be involved, that’s why I like coordinating with villages, MSMEs, clinics, and treatments at the public health center, we will help” (Respondents: 7, 8) |
| PRB efforts have not been optimal |
| “As health workers in the community, we certainly need things like this, to train the community with disaster management, in particular” (Respondents: 7, 10) “In the community, it is very necessary. In our hospital there is a Hospital Disaster Plan (HDP) for nurses and all health workers, so they can contribute. We don’t know the HDP training method or model at the hospital yet” (Respondents: 10) “Don’t know how, need to be told how to do it or be trained, sir. So that people know. The village is ready to support…” (Respondents: 4, 5, 6, 11) “Someone has to start sir. We are ready to help. We don’t know the models and methods of training our society. Especially in the health sector. There should be guidelines so that people can be educated ” (Respondents: 7, 8, 6, 11) “In the army, there is training for soldiers, sir. If we train people, we don’t know the method yet. If using the military route is not suitable, we are ready to help and cooperate with the public health center and other health care providers” (Respondents: 1, 2, 6) “If BPBD often conducts community training, it is only selective, not for all groups, just certain villages. It’s about the budget too. Those who have been trained are in Cicalengka and Majalya. South Bandung has not been done. Every year there are only enough for 2 villages. The name of the program is Destana” (Respondents: 3, 7) “As far as the health sector is concerned, there is no such thing, I haven’t heard of it” (Respondents: 3, 7, 8, 9, 10) “Nurses are not optimal, sir, because they have a lot of activities. Those who participate in the training are also limited, there are none in the community health centers yet, we have not participated in the community development training in the field of disaster, we still have to continue with other programs” (Respondents: 9, 10) “Community Nurses are too busy with administrative work, sir, this disaster problem has not been addressed, there must be training first, so that we know how far we can train the community” (Respondents: 9, 10) |
| There needs to be a model of community development in disaster management |
| “The government’s efforts have not gone well, for example the need for heavy equipment for landslides, it is difficult and takes time if needed” (Respondents: 1, 2, 3, 11) “The government has been good. The Health Office has coordinated to meet the needs, it just needs more organization. For example, referrals to hospitals have not been optimal, difficulty in costs, treatment requirements. Because of this, there are victims who are rejected” (Respondents: 9, 10, 7) “People usually struggle when there is a disaster. Help is lacking and late and we are the ones who are blamed, sir. Especially if there are health problems that we don’t know what to do” (Respondents: 4, 5, 11) “I’m not sure about the government, but us as community partners are responsible. We will help if there is an institution that will develop the community, like now. we are ready to cooperate if needed” (Respondents: 7, 8, 11) “The government has tried, there are many programs for disasters. For example, for COVID 19. This is a disaster too; it just can’t be solved as fast as turning the palm of the hand. Moreover, the community has different characters, now the government has tried very hard, the sub-district always coordinates with BPBD to map if there are locations that are threatened with landslides” (Respondents: 3, 6) “For the wider community, it has not been felt, sir, the government likes to be unfair, in other places it is fast, while in our place it takes a long time. I don’t know why, the fast ones are the army, sir. Maybe it’s because there are noncommissioned law enforcement officers, huh… And the police take action if there is a report” (Respondents: 4, 5, 11) “At BPBD, we try to maximize our efforts, sir, but it’s only limited to human resources. For example, if there is a health problem, we coordinate with the service, we cannot handle it directly. BPBD can only coordinate. That’s right, sir, we can’t do it all, especially human resources. We don’t have all professions, so we really need cooperation” (Respondents: 3) |
| Government efforts have not been effective |
| “I have never participated in any training, and indeed there has never been any in the village for our community, especially those related to the health sector” (Respondents: 4, 5, 6, 7, 10, 11) “ If we have not participated in disaster management training, and in the Army, the training is the same as military training. If you want to go to the area there has to be a special course on how to approach the community. Just not specialized in disaster management training” (Respondents: 1, 2) “As a BPBD extension worker, I have often participated in training, but I have never attended training in the community that was held by health workers. The most frequent, yes.. training with ‘PT” (a company), but the materials are usually trauma healing, soup kitchens, rarely about health…” (Respondents: 3) “To my knowledge in our area there has never been any special disaster management training for community members, including by BPBD. I feel like it’s never been done. So if the Polytechnic of Health wants to hold it, we will support and help” (Respondents: 7, 8, 6) “ I was once invited by the Geodipa representative for disaster counseling in Ring 1, our area, only so far it has not been held, but I heard that Geodipa held it themselves without coordination with us. That we don’t know for sure” (Respondents: 4) “If it is true that there will be training in our area, we have been waiting for this, actually this is included in our program too, especially in villages that are in direct contact with the mountain and gas production center, indeed there has been compensation, but there has never been training and counseling about disasters” (Respondents: 5, 6) “ In our area, there is no cadre training for nurses, let alone for the community. So we have never guided the community for disaster management, in the future, if God wills it, we will program it” (Respondents: 7, 10) “ I work at the hospital and the Disaster Hospital Plan training had been done, specifically with the emergency room team and the disaster team in each hospital, but for the surrounding community, we at the hospital have never held it” (Respondents: 9) |
| No involvement yet in an integrated disaster training program in the health sector |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sofyana, H.; Ibrahim, K.; Afriandi, I.; Herawati, E.; Wahito Nugroho, H.S. The Need for a Preparedness Training Model on Disaster Risk Reduction Based on Culturally Sensitive Public Health Nursing (PHN). Int. J. Environ. Res. Public Health 2022, 19, 16467. https://doi.org/10.3390/ijerph192416467
Sofyana H, Ibrahim K, Afriandi I, Herawati E, Wahito Nugroho HS. The Need for a Preparedness Training Model on Disaster Risk Reduction Based on Culturally Sensitive Public Health Nursing (PHN). International Journal of Environmental Research and Public Health. 2022; 19(24):16467. https://doi.org/10.3390/ijerph192416467
Chicago/Turabian StyleSofyana, Haris, Kusman Ibrahim, Irvan Afriandi, Erna Herawati, and Heru Santoso Wahito Nugroho. 2022. "The Need for a Preparedness Training Model on Disaster Risk Reduction Based on Culturally Sensitive Public Health Nursing (PHN)" International Journal of Environmental Research and Public Health 19, no. 24: 16467. https://doi.org/10.3390/ijerph192416467