

Does Appearance Matter during Pregnancy? A Cross-Sectional Study of Body Satisfaction from Pre-Pregnancy to Late Gestation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Outcome Measures
2.4. Statistical Analyses
3. Results
3.1. Participants
3.2. Health Status and Behaviour
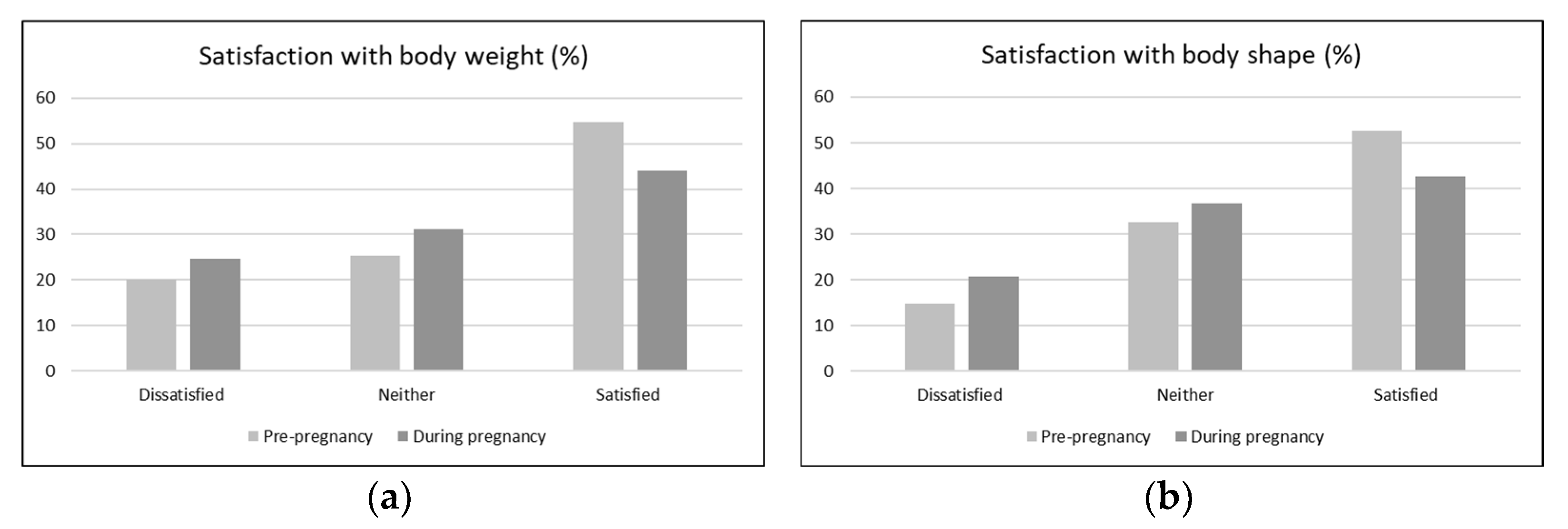
3.3. Changes in Body Satisfaction from Pre-Pregnancy to Late Pregnancy
3.4. Associations between Body Satisfaction and Health Behaviour
3.4.1. Physical Activity
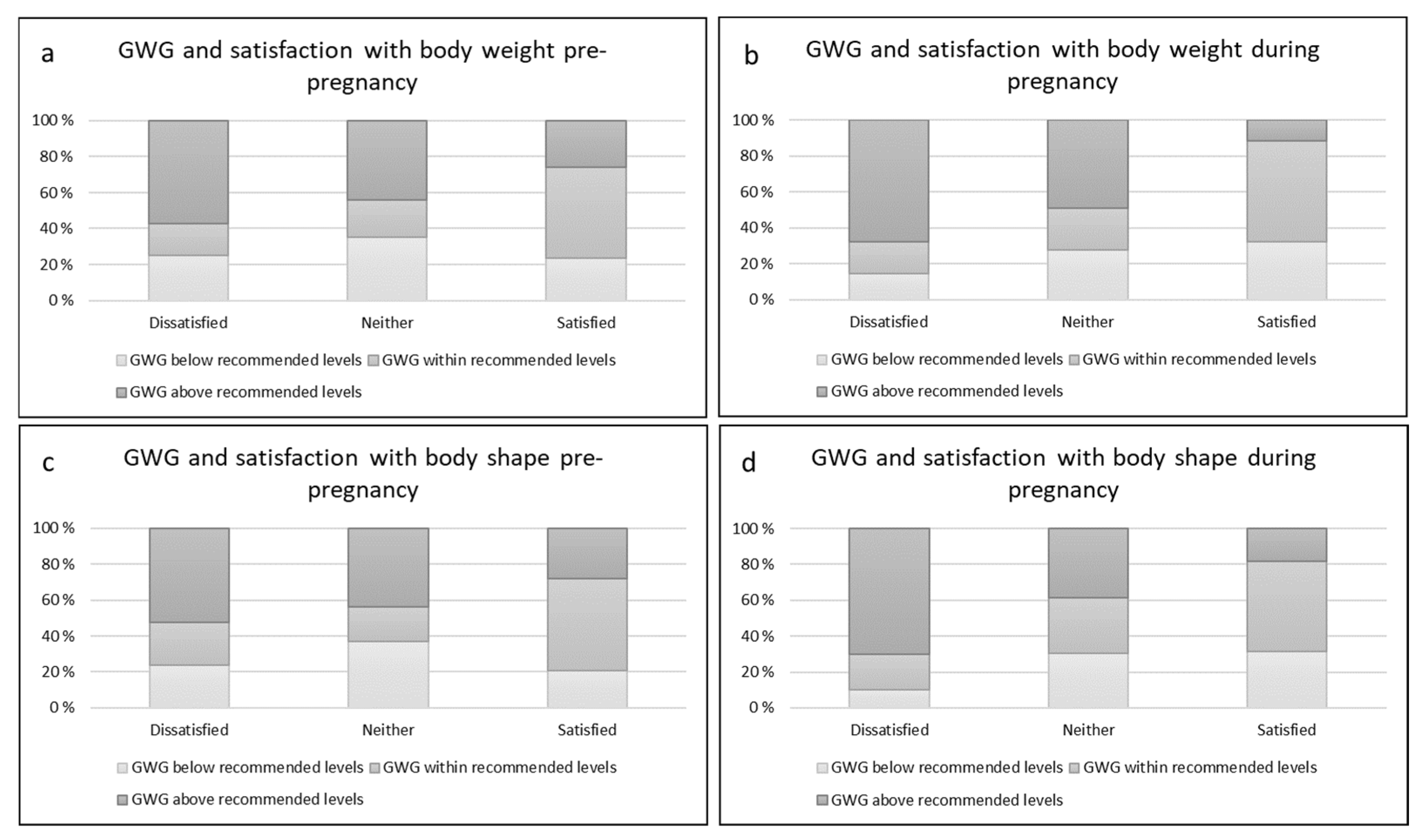
3.4.2. Gestational Weight Gain
4. Discussion
4.1. Strengths, Limitations, and Future Directions
4.2. Implications for Professional Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cash, T.F.; Smolak, L. Body Image: A Handbook of Science, Practice, and Prevention; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Frederick, D.A.; Daniels, E.A.; Bates, M.E.; Tylka, T.L. Exposure to thin-ideal media affect most, but not all, women: Results from the Perceived Effects of Media Exposure Scale and open-ended responses. Body Image 2017, 23, 188–205. [Google Scholar] [CrossRef] [PubMed]
- Hicks, S.; Brown, A. Higher Facebook use predicts greater body image dissatisfaction during pregnancy: The role of self-comparison. Midwifery 2016, 40, 132–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncombe, D.; Wertheim, E.H.; Skouteris, H.; Paxton, S.J.; Kelly, L. How well do women adapt to changes in their body size and shape across the course of pregnancy? J. Health Psychol. 2008, 13, 503–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skouteris, H. Body image issues in obstetrics and gynecology. In Body Image: A Handbook of Science, Practice, and Prevention, 2nd ed.; The Guilford Press: New York, NY, USA, 2011; pp. 342–349. [Google Scholar]
- Loth, K.A.; Bauer, K.W.; Wall, M.; Berge, J.; Neumark-Sztainer, D. Body satisfaction during pregnancy. Body Image 2011, 8, 297–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roomruangwong, C.; Kanchanatawan, B.; Sirivichayakul, S.; Maes, M. High incidence of body image dissatisfaction in pregnancy and the postnatal period: Associations with depression, anxiety, body mass index and weight gain during pregnancy. Sex. Reprod. Healthc. 2017, 13, 103–109. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 650: Physical Activity and Exercise During Pregnancy and the Postpartum Period. Obstet. Gynecol. 2015, 126, e135–e142. [Google Scholar] [CrossRef]
- Institute of Medicine. National Research Council Committee to Reexamine Institute of Medicine Pregnancy Weight Guidelines, The National Academies Collection: Reports funded by National Institutes of Health. In Weight Gain during Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academies Press (US)—National Academy of Sciences: Washington, DC, USA, 2009. [Google Scholar] [CrossRef]
- Da Silva, S.G.; Ricardo, L.I.; Evenson, K.R.; Hallal, P.C. Leisure-Time Physical Activity in Pregnancy and Maternal-Child Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials and Cohort Studies. Sports Med. 2017, 47, 295–317. [Google Scholar] [CrossRef]
- Di Mascio, D.; Magro-Malosso, E.R.; Saccone, G.; Marhefka, G.D.; Berghella, V. Exercise during pregnancy in normal-weight women and risk of preterm birth: A systematic review and meta-analysis of randomized controlled trials. Am. J. Obstet. Gynecol. 2016, 215, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain With Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Sun, W.; Chen, D.; Wang, J.; Liu, N.; Zhang, W. Physical activity and body image dissatisfaction among pregnant women: A systematic review and meta-analysis of cohort studies. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 229, 38–44. [Google Scholar] [CrossRef]
- Haakstad, L.A.; Torset, B.; Bø, K. What is the effect of regular group exercise on maternal psychological outcomes and common pregnancy complaints? An assessor blinded RCT. Midwifery 2016, 32, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Hartley, E.; McPhie, S.; Skouteris, H.; Fuller-Tyszkiewicz, M.; Hill, B. Psychosocial risk factors for excessive gestational weight gain: A systematic review. Women Birth 2015, 28, e99–e109. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.Y.; Lee, A.M.; Koh, Y.W.; Lam, S.K.; Lee, C.P.; Leung, K.Y.; Tang, C.S.K. Associations of body dissatisfaction with anxiety and depression in the pregnancy and postpartum periods: A longitudinal study. J. Affect. Disord. 2020, 263, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Aittasalo, M.; Raitanen, J.; Kinnunen, T.I.; Ojala, K.; Kolu, P.; Luoto, R. Is intensive counseling in maternity care feasible and effective in promoting physical activity among women at risk for gestational diabetes? Secondary analysis of a cluster randomized NELLI study in Finland. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 104. [Google Scholar] [CrossRef] [Green Version]
- Fuller-Tyszkiewicz, M.; Skouteris, H.; Watson, B.E.; Hill, B. Body dissatisfaction during pregnancy: A systematic review of cross-sectional and prospective correlates. J. Health Psychol. 2013, 18, 1411–1421. [Google Scholar] [CrossRef]
- Dalhaug, E.M.; Haakstad, L.A.H. What the Health? Information Sources and Maternal Lifestyle Behaviors. Interact. J. Med. Res. 2019, 8, e10355. [Google Scholar] [CrossRef]
- Sagedal, L.R.; Overby, N.C.; Lohne-Seiler, H.; Bere, E.; Torstveit, M.K.; Henriksen, T.; Vistad, I. Study protocol: Fit for delivery—Can a lifestyle intervention in pregnancy result in measurable health benefits for mothers and newborns? A randomized controlled trial. BMC Public Health 2013, 13, 132. [Google Scholar] [CrossRef] [Green Version]
- Haakstad, L.A.; Gundersen, I.; Bo, K. Self-reporting compared to motion monitor in the measurement of physical activity during pregnancy. Acta Obstet. Gynecol. Scand. 2010, 89, 749–756. [Google Scholar] [CrossRef]
- Owe, K.M.; Nystad, W.; Bo, K. Correlates of regular exercise during pregnancy: The Norwegian Mother and Child Cohort Study. Scand. J. Med. Sci. Sports 2009, 19, 637–645. [Google Scholar] [CrossRef]
- Haakstad, L.A.; Bo, K. Exercise in pregnant women and birth weight: A randomized controlled trial. BMC Pregnancy Childbirth 2011, 11, 66. [Google Scholar] [CrossRef] [Green Version]
- Haakstad, L.A.H. Physical Activity and Weight Gain During Pregnancy. Ph.D. Thesis, The Norwegian School of Sports Sciences, Oslo, Norway, 2010. [Google Scholar]
- Haakstad, L.A.H.; Kissel, I.; Bo, K. Long-term effects of participation in a prenatal exercise intervention on body weight, body mass index, and physical activity level: A 6-year follow-up study of a randomized controlled trial. J. Matern.-Fetal Neonatal Med. 2019, 34, 1347–1355. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Institute of Medicine and National Research Council. Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press: Washington, DC, USA, 2009.
- Mass, E.F. Whom Do They Trust? A Cross-Sectional Study Investigating the Association between Pregnant Women’s Information Sources and Their Behaviours regarding Physical Activity, Weight Gain and Nutrition, as Well as Health Care Providers’ Practices with Respect to Giving Advice. Master’s Thesis, Norwegian School of Sports Sciences, Oslo, Norway, 2016. [Google Scholar]
- Pullmer, R.; Zaitsoff, S.; Cobb, R. Body Satisfaction During Pregnancy: The Role of Health-Related Habit Strength. Matern. Child Health J. 2018, 22, 391–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coker, E.; Abraham, S. Body weight dissatisfaction before, during and after pregnancy: A comparison of women with and without eating disorders. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2015, 20, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Nagl, M.; Jepsen, L.; Linde, K.; Kersting, A. Measuring body image during pregnancy: Psychometric properties and validity of a German translation of the Body Image in Pregnancy Scale (BIPS-G). BMC Pregnancy Childbirth 2019, 19, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boscaglia, N.; Skouteris, H.; Wertheim, E. Changes in body image satisfaction during pregnancy: A comparison of high exercising and low exercising women. Aust. N. Z. J. Obstet. Gynaecol. 2003, 43, 41–45. [Google Scholar] [CrossRef]
- Prather, H.; Spitznagle, T.; Hunt, D. Benefits of exercise during pregnancy. PM R 2012, 4, 845–850. [Google Scholar]
- Downs, D.S.; DiNallo, J.M.; Kirner, T.L. Determinants of pregnancy and postpartum depression: Prospective influences of depressive symptoms, body image satisfaction, and exercise behavior. Ann. Behav. Med. 2008, 36, 54–63. [Google Scholar] [CrossRef]
- Bagheri, M.; Dorosty, A.; Sadrzadeh-Yeganeh, H.; Eshraghian, M.; Amiri, E.; Khamoush-Cheshm, N. Pre-pregnancy body size dissatisfaction and excessive gestational weight gain. Matern. Child Health J. 2013, 17, 699–707. [Google Scholar] [CrossRef]
- Rogozińska, E.; Zamora, J.; Marlin, N.; Betrán, A.P.; Astrup, A.; Bogaerts, A.; Cecatti, J.G.; Dodd, J.M.; Facchinetti, F.; Geiker, N.R.W.; et al. Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials. BMC Pregnancy Childbirth 2019, 19, 322. [Google Scholar] [CrossRef] [Green Version]
- Teede, H.J.; Bailey, C.; Moran, L.J.; Bahri Khomami, M.; Enticott, J.; Ranasinha, S.; Rogozińska, E.; Skouteris, H.; Boyle, J.A.; Thangaratinam, S.; et al. Association of Antenatal Diet and Physical Activity–Based Interventions With Gestational Weight Gain and Pregnancy Outcomes: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2022, 182, 106–114. [Google Scholar] [CrossRef]
- Liechty, T.; Coyne, S.M.; Collier, K.M.; Sharp, A.D. "It’s Just Not Very Realistic": Perceptions of Media Among Pregnant and Postpartum Women. Health Commun. 2018, 33, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Steube, F.; Löwe, B.; Weigel, A. “Belly Only Pregnancy” content on social media and in internet blogs: A qualitative analysis on its definition and potential risks and benefits. Eat. Weight Disord. 2022. [Google Scholar] [CrossRef] [PubMed]
- Holland, G.; Tiggemann, M. A systematic review of the impact of the use of social networking sites on body image and disordered eating outcomes. Body Image 2016, 17, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Mostafavi-Darani, F.; Daniali, S.S.; Azadbakht, L. Relationship of body satisfaction, with nutrition and weight control behaviors in women. Int. J. Prev. Med. 2013, 4, 467–474. [Google Scholar]
- Sinclair, M.; O’Toole, J.; Malawaraarachchi, M.; Leder, K. Comparison of response rates and cost-effectiveness for a community-based survey: Postal, internet and telephone modes with generic or personalised recruitment approaches. BMC Med. Res. Methodol. 2012, 12, 132. [Google Scholar] [CrossRef] [Green Version]
- Jones, M.K.; Calzavara, L.; Allman, D.; Worthington, C.A.; Tyndall, M.; Iveniuk, J. A Comparison of Web and Telephone Responses From a National HIV and AIDS Survey. JMIR Public Health Surveill. 2016, 2, e37. [Google Scholar] [CrossRef] [Green Version]
- Hansen, B.H.; Anderssen, S.A.; Steene-Johannessen, J.; Ekelund, U.; Nilsen, A.K.; Andersen, I.D.; Dalene, K.E.; Kolle, E. Physical Activity and Sedentary Time among Adults and Elderly in Norway—National Surveillance 2014–2015; Norwegian Directorate of Health: Oslo, Norway, 2015.
- Leighton, K.; Kardong-Edgren, S.; Schneidereith, T.; Foisy-Doll, C. Using Social Media and Snowball Sampling as an Alternative Recruitment Strategy for Research. Clin. Simul. Nurs. 2021, 55, 37–42. [Google Scholar] [CrossRef]
- Hart, L.M.; Cornell, C.; Damiano, S.R.; Paxton, S.J. Parents and prevention: A systematic review of interventions involving parents that aim to prevent body dissatisfaction or eating disorders. Int. J. Eat. Disord. 2015, 48, 157–169. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Dimensions Assessed | Main Variables and Questions Used | Reference |
|---|---|---|
| Sociodemographic characteristics | Age, gestation week, parity, marital status, place of residence, country of birth, educational level, occupation, and number of antenatal consultations. | Developed for this project |
| Anthropometry and gestational weight gain | Participants were asked to state their height, pre-pregnancy weight, and current weight a. | Developed for this project |
| Physical activity | Assessed using the question: “The health authorities recommend all pregnant women to perform moderate-intensity aerobic physical activity (activities that take moderate physical effort and make you breathe somewhat harder than normal, such as brisk walking, housework, etc.) for a minimum of 30 min five days a week. With this in mind, would you characterize yourself as physically active (a) pre-pregnancy and (b) in your current gestation week?” Response options: “Yes”, “No” or “I don’t know”. | Based on the ACOG recommendations [7] |
| Changes in body satisfaction from pre-pregnancy to late pregnancy | The respondents were asked to rate four statements on an 11-item scale, 0 being negative and 10 being positive. The statements were: (1) “How satisfied were you with your body weight pre-pregnancy?”, (2) “How satisfied are you with your body weight today?”, (3) “How satisfied were you with your body shape pre-pregnancy?” and (4) “How satisfied are you with your body shape today?”. | Based on questions used in previous research [24,25] |
| Habitual changes to stabilise/reduce weight gain during pregnancy. | Assessed using the question: “Over the course of pregnancy have you made habitual changes in order to stabilise/reduce further weight gain?”. Response options: “Yes” or “No”. If the respondents answered yes, they were asked to elaborate. Categorical response options: “Increased the number of exercise sessions”, “Increased the exercise intensity”, “Skipped breakfast”, “Deliberately omitted foods high in sugar and fat”, “Eaten less than usual” and “Other, please specify”. The respondents were able to choose more than one category. | Developed for this project |
| Satisfaction with physical and mental health | The respondents were asked to rate four statements on an 11-item scale, 0 being negative and 10 being positive. The statements were: “All in all, how satisfied are you with your physical health as pregnant?” and “All in all, how satisfied are you with your mental health as pregnant?”. | Developed for this project |
| Characteristics | n | % | |
|---|---|---|---|
| Parity | |||
| Nulliparous | 91 | 60.7 | |
| Multiparous | 59 | 39.3 | |
| Marital status | |||
| Married/living together | 147 | 98.0 | |
| Other | 3 | 2.0 | |
| Country of birth | |||
| Norway | 130 | 86.7 | |
| Other (Sweden, Denmark, Iceland, Syria, Gambia, Macedonia, Morocco, Spain, Italy, Russia, Iran) | 20 | 13.3 | |
| Education | |||
| <4 years college/university | 54 | 36.0 | |
| ≥4 years college/university | 96 | 64.0 | |
| Employment status | |||
| Employed/student | 144 | 96.0 | |
| Not employed | 6 | 4.0 | |
| Physically active | |||
| Pre-pregnancy | 132 | 88.0 | |
| During pregnancy | 73 | 48.7 | |
| Pre-pregnancy BMI category | |||
| Underweight | 2 | 1.3 | |
| Normal weight | 102 | 68.4 | |
| Overweight | 28 | 18.7 | |
| Obese | 17 | 11.4 | |
| Smoking in pregnancy | |||
| No | 149 | 99.3 | |
| Yes | 1 | 0.7 | |
| Pregnancy complaints | |||
| Pelvic girdle pain | 69 | 46.0 | |
| Back pain | 67 | 44.7 | |
| Urinary incontinence | 30 | 20.0 | |
| On sick leave | 39 | 26.0 | |
| Adherence to national nutritional guidelines | 98 | 65.3 | |
| n | % | Mean (SD) | |
|---|---|---|---|
| Within recommendations | 51 | 36.7 | - |
| Below recommendations | 37 | 26.7 | −2.6 (± 2.2) |
| Above recommendations | 51 | 36.7 | +3.0 (± 2.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalhaug, E.M.; Haakstad, L.A.H. Does Appearance Matter during Pregnancy? A Cross-Sectional Study of Body Satisfaction from Pre-Pregnancy to Late Gestation. Int. J. Environ. Res. Public Health 2022, 19, 16375. https://doi.org/10.3390/ijerph192316375
Dalhaug EM, Haakstad LAH. Does Appearance Matter during Pregnancy? A Cross-Sectional Study of Body Satisfaction from Pre-Pregnancy to Late Gestation. International Journal of Environmental Research and Public Health. 2022; 19(23):16375. https://doi.org/10.3390/ijerph192316375
Chicago/Turabian StyleDalhaug, Emilie Mass, and Lene Annette Hagen Haakstad. 2022. "Does Appearance Matter during Pregnancy? A Cross-Sectional Study of Body Satisfaction from Pre-Pregnancy to Late Gestation" International Journal of Environmental Research and Public Health 19, no. 23: 16375. https://doi.org/10.3390/ijerph192316375