
Effects of a Diabetes Self-Management Education Program on Glucose Levels and Self-Care in Type 1 Diabetes: A Pilot Randomized Controlled Trial
 , , and
, , and
Abstract
:1. Introduction
- The control rates for blood glucose measured by the continuous glucose monitoring sensor would be higher after the educational program compared to routine-intervention levels.
- Knowledge, emotional state, and diabetes self-care activities would improve after 1 and 3 months of a nurse educational intervention compared to the control group.
- Emotional regulation, knowledge, and diabetes self-care activities would influence blood glucose control.
2. Material and Methods
2.1. Design
2.2. Participants
2.3. Randomization
2.4. Routine Intervention
2.5. Nurse-Led Health Education
2.6. Outcome Measures and Data Collection
3. Results
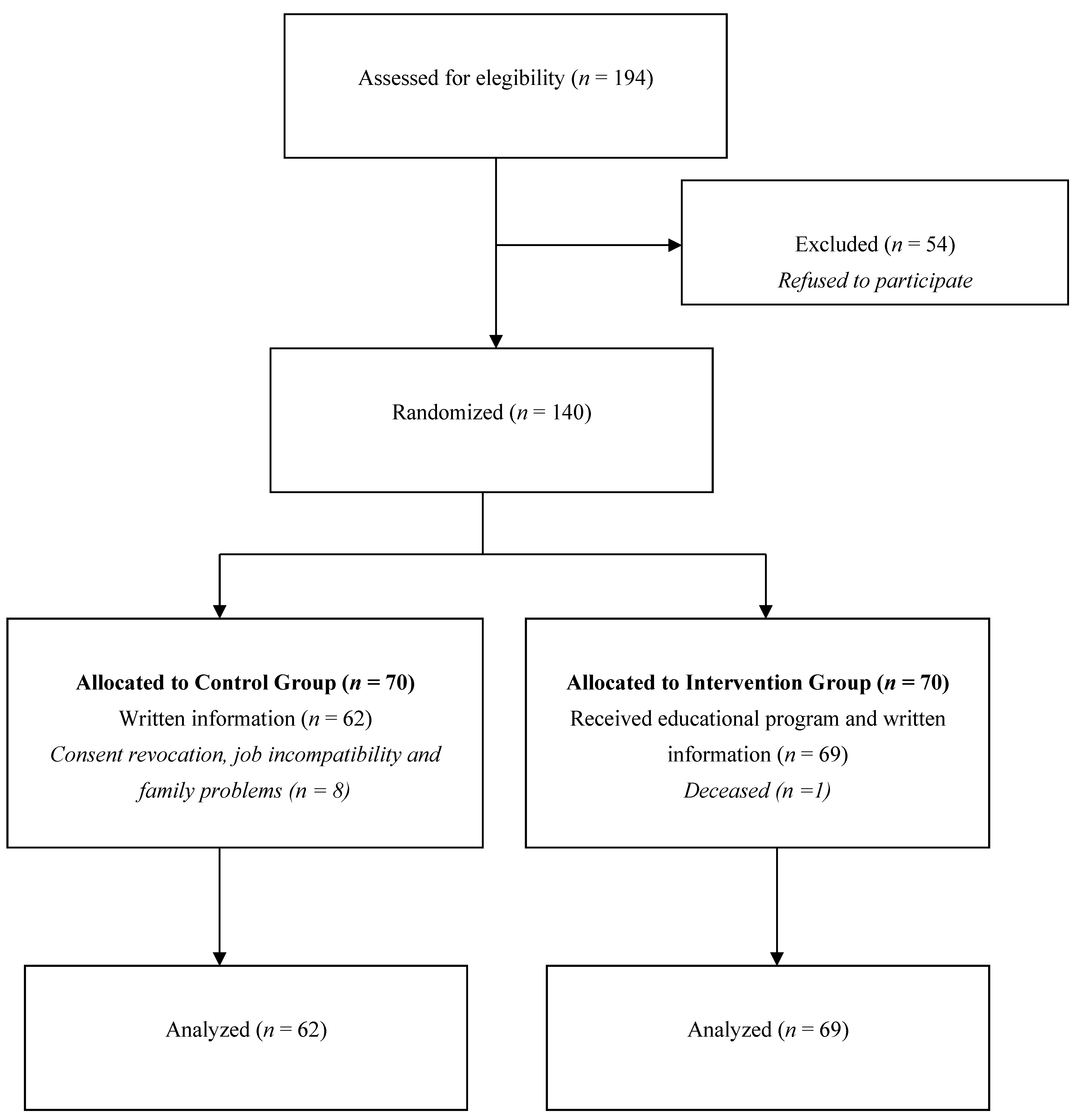
3.1. Participant Characteristics
3.2. Study Outcomes
3.3. Binary Logistic Regression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Diabetes Association. Lifestyle management: Standards of medical care in diabetes-2019. Diabetes Care 2019, 42 (Suppl. 1), S46–S60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adu, M.D.; Malabu, U.H.; Malau-Aduli, A.E.O.; Malau-Aduli, B.S. Enablers and barriers to effective diabetes self-management: A multi-national investigation. PLoS ONE 2019, 14, e0217771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickinson, J.K.; Burke, S.D.; Traficano, S. From diabetes educators to diabetes care and education specialists: Time for change. Assoc. Diabetes Care Educ. Spec. 2021, 9, 52–55. [Google Scholar] [CrossRef]
- Fain, J.A. Embracing a new vision for diabetes education and diabetes educators. Diabetes Educ. 2019, 45, 331–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, W.; Wei, W.; Wang, J.; Lyu, Y.; Li, L. Effectiveness of a nurse-led educational programme based on basic insulin therapy in patients with diabetes mellitus: A quasi-experimental trial. J. Clin. Nurs. 2021, 31, 2227–2239. [Google Scholar] [CrossRef]
- Powers, M.A.; Bardsley, J.K.; Cypress, M.; Funnell, M.M.; Harms, D.; Hess-Fischl, A.; Hooks, B.; Isaacs, D.; Mandel, E.D.; Maryniuk, M.D.; et al. Diabetes self-management education and support in adults with type 2 diabetes: A consensus report of the American Diabetes Association, the Association of Diabetes Care Education Specialists, the Academy of Nutrition and Dietetics, the American Academy of Family Physicians, the American Academy of PAs, the American Association of Nurse Practitioners, and the American Pharmacists Association. Diabetes Educ. 2020, 46, 350–369. [Google Scholar] [CrossRef]
- Bluml, B.M.; Kolb, L.E.; Lipman, R. Evaluating the impact of year-long, augmented diabetes self-management support. Popul. Health Manag. 2019, 22, 522–528. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Li, J.; Wang, B.; Yao, Q.; Li, L.; Song, R.; Shi, X.; Zhang, J. Diabetes self-management education reduces risk of all-cause mortality in type 2 diabetes patients: A systematic review and meta-analysis. Endocrine 2017, 55, 712–731. [Google Scholar] [CrossRef]
- Strawbridge, L.M.; Lloyd, J.T.; Meadow, A.; Riley, G.F.; Howell, B.L. One-year outcomes of diabetes self-management training among Medicare beneficiaries newly diagnosed with diabetes. Med. Care 2017, 55, 391–397. [Google Scholar] [CrossRef]
- Alotaibi, A.; Gholizadeh, L.; Al-Ganmi, A.; Perry, L. Factors influencing nurses’ knowledge acquisition of diabetes care and its management: A qualitative study. J. Clin. Nurs. 2018, 27, 4340–4352. [Google Scholar] [CrossRef]
- Luo, J.; Wang, H.; Li, X.; Zhou, Z.; Valimaki, M.; Whittemore, R.; Grey, M.; Guo, J. Factors associated with diabetes distress among adolescents with type 1 diabetes. J. Clin. Nurs. 2021, 30, 1893–1903. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, B.S.; Reis, I.A.; Torres, H.C. Evaluation of the telephone intervention in the promotion of diabetes self-care: A randomized clinical trial. Rev. Lat. Am. Enferm. 2016, 24, e2719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Storch, K.; Graaf, E.; Wunderlich, M.; Rietz, C.; Polidori, M.C.; Woopen, C. Telemedicine-assisted self-management program for type 2 diabetes patients. Diabetes Technol. 2019, 21, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Ryan, D.; Burke, S.D.; Litchman, M.L.; Bronich-Hall, L.; Kolb, L.; Rinker, J.; Yehl, K. Competencies for diabetes care and education specialists. Diabetes Educ. 2020, 46, 384–397. [Google Scholar] [CrossRef] [PubMed]
- Al Hayek, A.A.; Robert, A.A.; Al Dawish, M.A. Evaluation of FreeStyle Libre flash glucose monitoring system on glycemic control, health-related quality of life, and fear of hypoglycemia in patients with type 1 diabetes. Clin. Med. Insights Endocrinol. Diabetes 2017, 10, 1179551417746957. [Google Scholar] [CrossRef]
- Paris, I.; Henry, C.; Pirard, F.; Gerard, A.C. The new FreeStyle Libre flash glucose monitoring system improves the glycaemic control in a cohort of people with type 1 diabetes followed in real-life conditions over a period of one year. Endocrinol. Diabetes Metab. 2018, 1, 00023. [Google Scholar] [CrossRef]
- Crowea, M.; Jonesa, V.; Stoneb, M.-A.; Coeb, G. The clinical effectiveness of nursing models of diabetes care: A synthesis of the evidence. Int. J. Nurs. Stud. 2019, 93, 119–128. [Google Scholar] [CrossRef]
- Chrvala, C.A.; Sherr, D.; Lipman, R.D. Diabetes self-management education for adults with type 2 diabetes mellitus: A systematic review of the effect on glycemic control. Patient Educ. Couns. 2016, 99, 926–943. [Google Scholar] [CrossRef] [Green Version]
- Caro-Bautista, J.; Kaknani-Uttumchandani, S.; García-Mayor, S.; Villa-Estrada, F.; Morilla-Herrera, J.C.; León-Campos, A.; Gómez-González, A.J.; Morales-Asencio, J.M. Impact of self-care programmes in type 2 diabetes mellitus population in primary health care: Systematic review and meta-analysis. J. Clin. Nurs. 2020, 29, 1457–1476. [Google Scholar] [CrossRef]
- Zhao, F.-F.; Suhonen, R.; Koskinen, S.; Leino-Kilpi, H. Theorybased self-management educational interventions on patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. J. Adv. Nurs. 2017, 73, 812–833. [Google Scholar] [CrossRef]
- Flood, D.; Hane, J.; Dunn, M.; Brown, S.J.; Wagenaar, B.H.; Rogers, E.A.; Heisler, M.; Rohloff, P.; Chopra, V. Health system interventions for adults with type 2 diabetes in low- and middle- income countries: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003434. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.L.; Lau, E.S.H.; Kong, A.P.S.; Davies, M.J.; Levitt, N.S.; Eliasson, B.; Aguilar-Salinas, C.A.; Ning, G.; Seino, Y.; So, W.Y.; et al. Aspects of multicomponent integrated care promote sustained improvement in surrogate clinical outcomes: A systematic review and meta-analysis. Diabetes Care 2018, 41, 1312–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, S.E.; Koh, J.J.K.; Toh, S.E.S.; Chia, K.S.; Balabonova, D.; McKee, M.; Perel, P.; Legido-Quigley, H. Assessing the influence of health systems on type 2 diabetes mellitus awareness, treatment, adherence, and control: A systematic review. PLoS ONE 2018, 13, e0195089. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Cobo, C.; Santi-Cano, M.J. Efficacy of Diabetes Education in Adults with Diabetes Mellitus Type 2 in Primary Care: A Systematic Review. J. Nurs. Sch. 2020, 52, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.B.; Potter, V.L.B.; Torensma, B.; Snoek, F.J.; Honig, A. Ethnic minorities with diabetes differ in depressive and anxiety symptoms and diabetes-distress. J. Diabetes Res. 2017, 2017, 1204237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, L.; Hessler, D.; Polonsky, W.; Strycker, L.; Masharani, U.; Peters, A. Diabetes distress in adults with type 1 diabetes: Prevalence, incidence and change over time. J. Diabetes Complicat 2016, 30, 1123–1128. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.; Hessler, D.; Polonsky, W.H.; Bowyer, V.; Strycker, L.; Ahmann, A.; Basina, M.; Blumer, I.; Chloe, C.; Kim, S.; et al. T1-REDEEM: A Randomized Controlled Trial to Reduce Diabetes Distress Among Adults with Type 1 Diabetes. Diabetes Care 2018, 41, 1862–1869. [Google Scholar] [CrossRef] [Green Version]
- Hessler, D.; Fisher, L.; Polonsky, W.H.; Masharani, U.; Strycker, L.A.; Peters, A.L.; Blumer, I.; Bowyer, V. Diabetes distress is linked with worsening diabetes management over time in adults with type 1 diabetes. Diabet. Med. 2017, 34, 1228–1234. [Google Scholar] [CrossRef]
- Petrie, J.R.; Peters, A.L.; Bergenstal, R.M.; Holl, R.W.; Fleming, A.; Heinemann, G.A. Improving the clinical value and utility of CGM systems: Issues and recommendations. A joint statement of the European Association for the Study of Diabetes and the American Diabetes Association Diabetes Technology Working Group. Diabetes Care 2017, 40, 1614–1621. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. Declaration of Helsinki. ETHICAL Principles for Medical Research Involving Human Subjects. 2013. 64ª General Assembly. Fortaleza, Brasil. Available online: https://www.wma.net/es/policies-post/declaracion-de-helsinki (accessed on 3 October 2022).
- Caro-Bautista, J.; Morilla-Herrera, J.C.; Villa-Estrada, F.; Cuevas-Fernández-Gallego, M.; Lupiáñez-Pérez, I.; Morales-Asencio, J.M. Adaptación cultural al español y validación psicométrica del Summary of Diabetes Self-Care Activities measure (SDSCA) en personas con diabetes mellitus tipo 2. Atención Primaria 2016, 48, 458–467. [Google Scholar] [CrossRef]
- Reivan-Ortiz, G.; Pineda-García, G.; León-Parias, B.D. Psychometric Properties of the Goldberg Anxiety and Depression Scale (GADS) in ecuatorian population. Int. J. Psychol. Res. 2019, 12, 41–48. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44 (Suppl. S1), S15–S33. [Google Scholar] [CrossRef] [PubMed]
- Whitworth, S.R.; Bruce, D.G.; Starkstein, S.E.; Davis, W.A.; Davis, T.M.E.; Bucks, R.S. Lifetime depression and anxiety increase prevalent psychological symptoms and worsen glycemic control in type 2 diabetes: The Fremantle Diabetes Study Phase II. Diabetes Res. Clin. Pr. 2016, 122, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Suhonen, R.; Katajisto, J.; Leino-Kilpi, H. The association of diabetes-related self-care activities with perceived stress, anxiety, and fatigue: A cross-sectional study. Patient Prefer. Adherence 2018, 12, 1677–1686. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.J.; Lu, Y.H.; Liu, S.L.; Wang, J.P.; Tang, R.S.; Li, M.Z. The effectiveness of a self-efficacy-focused structured education programme on adults with type 2 diabetes: A multicentre randomised controlled trial. J. Clin. Nurs. 2019, 28, 3299–3309. [Google Scholar] [CrossRef]
- Hagger, V.; Hendrieckx, C.; Cameron, F.; Pouwer, F.; Skinner, T.C.; Speight, J. Diabetes distress is more strongly associated with HbA1c than depressive symptoms in adolescents with type 1 diabetes: Results from Diabetes MILES Youth-Australia. Pediatric. Diabetes 2018, 19, 840–847. [Google Scholar] [CrossRef]
- Wichit, N.; Mnatzaganian, G.; Courtney, M.; Schulz, P.; Johnson, M. Randomized controlled trial of a family oriented self-management program to improve self-efficacy, glycemic control and quality of life among Thai individuals with Type 2 diabetes. Diabetes Res. Clin. Pract. 2017, 123, 37–48. [Google Scholar] [CrossRef] [Green Version]
- Cai, C.; Hu, J. Effectiveness of a family-based diabetes selfmanagement educational intervention for Chinese adults with type 2 diabetes in Wuhan, China. Diabetes Educ. 2016, 42, 697–711. [Google Scholar] [CrossRef]
- Romero-Castillo, R.; Pabón-Carrasco, M.; Jiménez-Picón, N.; Ponce-Blandón, J.A. Diabetes Management after a Therapeutic Education Program: A Qualitative Study. Healthcare 2022, 10, 1375. [Google Scholar] [CrossRef]


{kind=link}
| Session Theme | Sessions Contents | Learning Methodology |
|---|---|---|
| First session. Insulin administration and blood glucose self-analysis. |
|
|
| Second session. Management of hypoglycemia and hyperglycemia. |
|
|
| Third session. Healthy diet adapted to the diabetic patient. |
|
|
| Fourth session. Physical exercise. |
|
|
| Variables | ||
|---|---|---|
| Age (years) | Range | Mean (SD) |
| 18–57 | 36.71 (12.07) | |
| Gender | Number | Percentage |
| Female | 69 | 52.7 |
| Male | 62 | 47.3 |
| Education level | ||
| Elementary | 49 | 37.41 |
| Junior high | 57 | 43.51 |
| Junior college | 9 | 6.87 |
| University or above | 16 | 12.21 |
| Marital status | ||
| Single | 36 | 27.48 |
| Married | 78 | 59.54 |
| Divorced or widowed | 17 | 12.98 |
| Current employment | ||
| No | 55 | 41.98 |
| Yes | 76 | 58.02 |
| Experimental Group (n = 69) | Control Group (n = 62) | Spearman’s Rho | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Variables | Baseline M +/− SD | 1 Month M +/− SD | 3 Months M +/− SD | Baseline M +/− SD | 1 Month M +/− SD | 3 Months M +/− SD | ||
| Sensor measurements Target range 1 | 54.805 (18.205) | 65.410 (19.345) | 62.487 (19.744) | 54.851 (18.246) | 54.238 (18.098) | 53.824 (17.218) | 0.168 | 0.027 * |
| High range 2 | 41.829 (18.942) | 31.769 (19.679) | 34.681 (20.008) | 41.693 (19.127) | 41.846 (18.976) | 41.785 (18.875) | −0.138 | 0.070 |
| Low range 3 | 3.512 (3.099) | 2.820 (2.624) | 2.931 (2.724) | 3.456 (3.078) | 3.916 (3.229) | 4.391 (4.126) | −0.036 | 0.637 |
| Average glucose | 190.024 (41.763) | 172.103 (46.703) | 176.369 (44.79) | 189.140 (40.825) | 188.458 (40.734) | 189.678 (41.287) | −0.199 | 0.009 * |
| HbA1C level | 7.778 (0.996) | 7.374 (1.019) | 7.481 (1.026) | 7.794 (0.987) | 7.806 (1.018) | 7.788 (0.948) | −0.184 | 0.015 * |
| Sensor usage (%) | 80.871 (17.601) | 87.769 (12.854) | 87.989 (13.528) | 81.745 (18.029) | 82.016 (17.549) | 81.512 (18.348) | 0.159 | 0.036 * |
| Knowledge test | 7.39 (1.32) | 8.077 (1.036) | 8.087 (1.219) | 7.28 (1.19) | 7.32 (1.275) | 7.19 (1.452) | 0.106 | 0.151 |
| Goldberg Scale Depression | 2.781 (2.067) | 2.128 (1.341) | 2.017 (1.611) | 2.812 (1.758) | 2.925 (2.025) | 2.937 (2.048) | −0.216 | 0.004 * |
| Goldberg Scale Anxiety | 4.366 (2.447) | 2.923 (1.612) | 2.894 (1.018) | 4.248 (2.126) | 4.358 (2.251) | 4.342 (2.238) | −0.166 | 0.026 * |
| Diabetes Self-Care Activities Measure | 31.268 (9.268) | 33.077 (8.174) | 33.235 (8.254) | 31.552 (10.126) | 30.947 (9.147) | 30.898 (8.474) | 0.028 | 0.705 |
| Variables | Goldberg Scale Anxiety Spearman’s Rho (p-Value) | Goldberg Scale Depression Spearman’s Rho (p-Value) | Diabetes Self-Care Activities Measure Spearman’s Rho (p-Value) | Knowledge Test Spearman’s Rho (p-Value) |
|---|---|---|---|---|
| Age | 0.064 (0.475) | 0.046 (0.606) | −0.167 (0.056) | −0.101 (0.249) |
| Target range | 0.110 (0.158) | 0.030 (0.700) | 0.023 (0.771) | −0.190 (0.012) * |
| High range | −0.167 (0.030) * | −0.073 (0.345) | 0.073 (0.347) | 0.269 (0.000) * |
| Low range | −0.159 (0.040) * | 0.036 (0.641) | −0.189 (0.014) * | 0.100 (0.189) |
| Average glucose | −0.197 (0.010) * | −0.167 (0.030) * | 0.239 (0.002) * | 0.255 (0.001) * |
| HbA1c level | −0.200 (0.009) * | −0.185 (0.017) * | 0.252 (0.001) * | 0.266 (0.000) * |
| Sensor usage (%) | −0.068 (0.383) | 0.116 (0.134) | −0.127 (0.100) | 0.059 (0.442) |
| Knowledge test | −0.629 (0.000) * | −0.375 (0.000) | 0.266 (0.000) * | |
| Goldberg Scale—Depression | 0.467 (0.000) * | |||
| Goldberg Scale—Anxiety | −0.472 (0.000) * | |||
| Diabetes Self-Care Activities Measure | −0.472 (0.000) * | −0.505 (0.000) * |
| Variables | B | S.E. | Wals | p | Exp (B) | EXP(B) 95% C.I. |
|---|---|---|---|---|---|---|
| Gender | −0.082 | 0.280 | 0.087 | 0.768 | 0.921 | 0.532, 1.593 |
| Age | −0.004 | 0.012 | 0.128 | 0.721 | 0.996 | 0.972, 1.020 |
| Target range | 0.101 | 0.071 | 1.979 | 0.159 | 1.106 | 0.961, 1.272 |
| High range | 0.114 | 0.073 | 2.455 | 0.117 | 1.120 | 0.972, 1.292 |
| Low range | 0.155 | 0.081 | 3.680 | 0.055 | 1.168 | 0.997, 1.368 |
| Average glucose | −0.057 | 0.033 | 2.911 | 0.088 | 0.945 | 0.886, 1.008 |
| HbA1c level | 1.996 | 1.461 | 1.868 | 0.172 | 7.362 | 0.420, 128.930 |
| Sensor usage (%) | 0.047 | 0.018 | 7.053 | 0.008 * | 1.048 | 1.012, 1.084 |
| Knowledge | 0.827 | 0.134 | 37.955 | 0.000 * | 0.438 | 0.336, 0.569 |
| Depression | 0.642 | 0.126 | 25.768 | 0.000 * | 1.901 | 1.483, 2.435 |
| Anxiety | −0.135 | 0.091 | 2.207 | 0.137 | 0.874 | 0.731, 1.044 |
| Diabetes Self-Care Activities Measure | 0.41 | 0.019 | 4.483 | 0.034 * | 1.042 | 1.003, 1.082 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Castillo, R.; Pabón-Carrasco, M.; Jiménez-Picón, N.; Ponce-Blandón, J.A. Effects of a Diabetes Self-Management Education Program on Glucose Levels and Self-Care in Type 1 Diabetes: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 16364. https://doi.org/10.3390/ijerph192316364
Romero-Castillo R, Pabón-Carrasco M, Jiménez-Picón N, Ponce-Blandón JA. Effects of a Diabetes Self-Management Education Program on Glucose Levels and Self-Care in Type 1 Diabetes: A Pilot Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(23):16364. https://doi.org/10.3390/ijerph192316364
Chicago/Turabian StyleRomero-Castillo, Rocío, Manuel Pabón-Carrasco, Nerea Jiménez-Picón, and José Antonio Ponce-Blandón. 2022. "Effects of a Diabetes Self-Management Education Program on Glucose Levels and Self-Care in Type 1 Diabetes: A Pilot Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 23: 16364. https://doi.org/10.3390/ijerph192316364