
Caregiver Burden, Psychological Distress and Quality of Life among Informal Caregivers of Patients with Head and Neck Cancer: A Longitudinal Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Caregiver Burden, Psychological Distress and QoL in Caregivers of HNC Patients from Diagnosis to 2 Years after Treatment of HNC Cancer
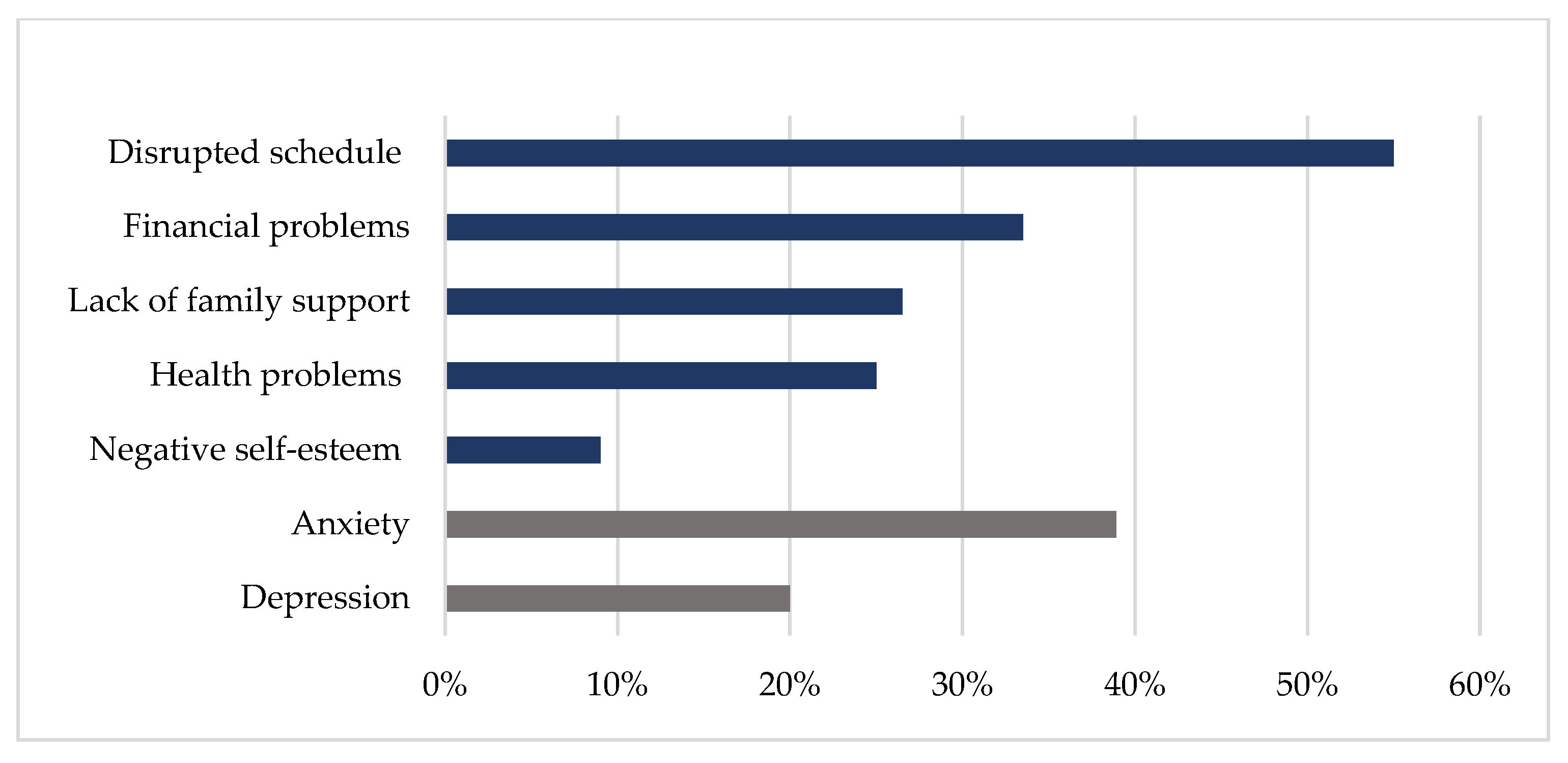
3.2.1. Baseline
3.2.2. During Follow-Up
3.3. The Relation between Caregiver Burden and Psychological Distress and QoL in Caregivers
3.4. Variables Associated with Caregiver Burden, Psychological Distress and QoL over Time in Caregivers
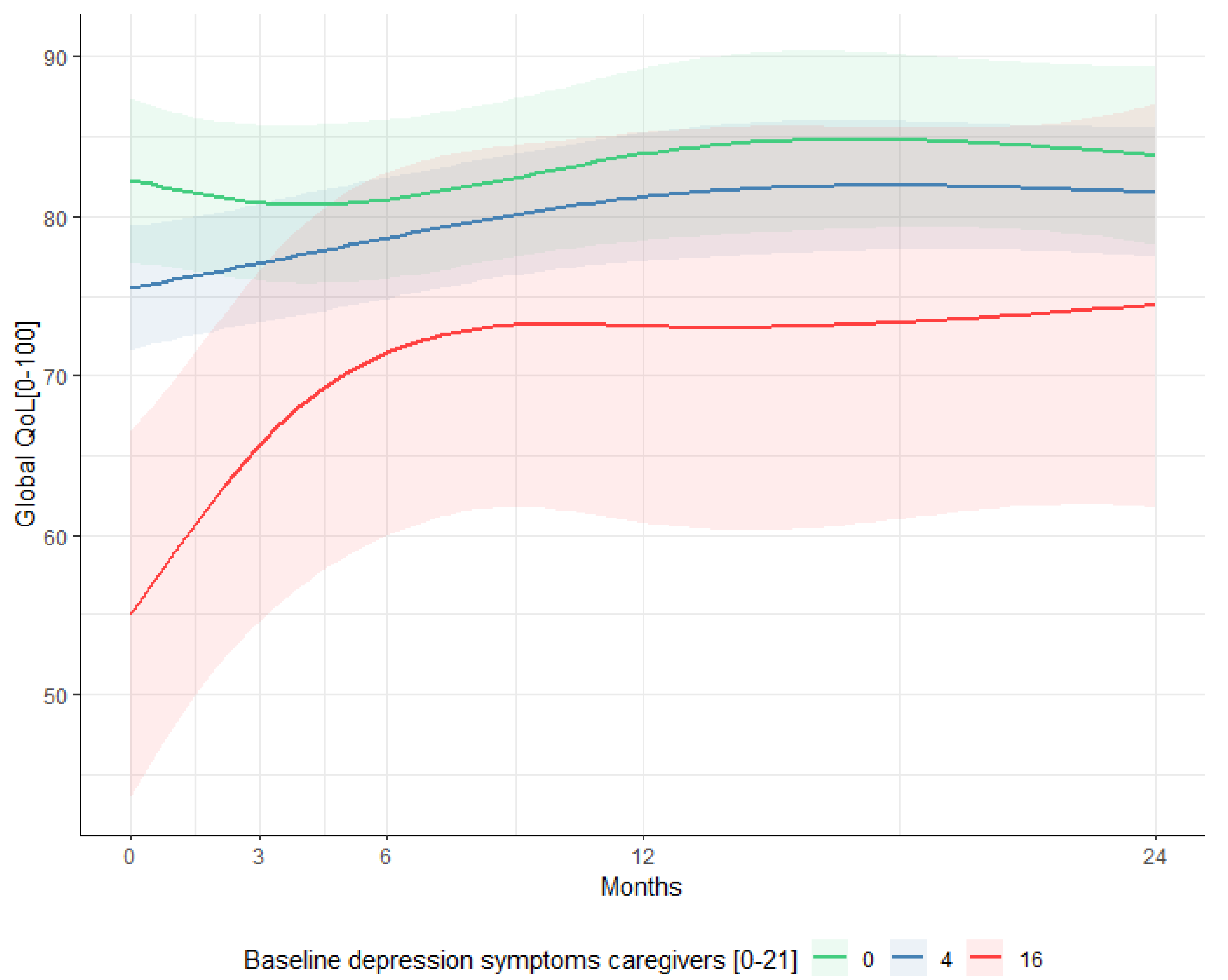
3.5. The Relationship between Caregiver Burden and Psychological Distress of Caregivers at Baseline with Psychological Distress and QoL of Their Related Patients over Time
4. Discussion
4.1. Strengths and Limitations
4.2. Clinical Implications and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
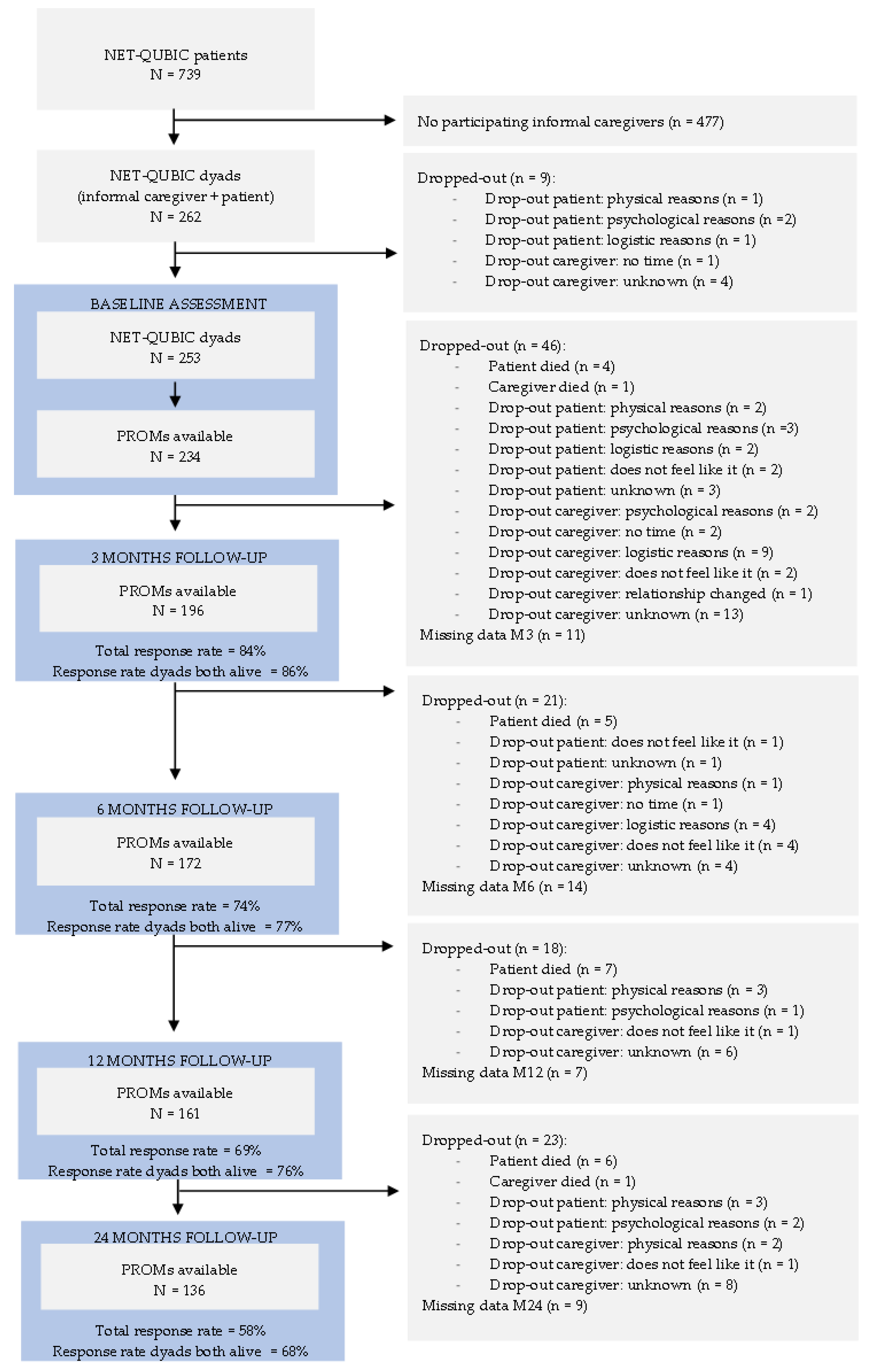
Appendix A. Flowchart of All Eligible HNC Patients and Reasons for Non-Participation

References
- Gupta, B.; Johnson, N.W.; Kumar, N. Global Epidemiology of Head and Neck Cancers: A Continuing Challenge. Oncology 2016, 91, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Hoesseini, A.; van Leeuwen, N.; Offerman, M.P.; Zhang, J.; Dronkers, E.A.; Sewnaik, A.; Lingsma, H.F.; Baatenburg de Jong, R.J. Predicting survival in head and neck cancer: External validation and update of the prognostic model OncologIQ in 2189 patients. Head Neck 2021, 43, 2445–2456. [Google Scholar] [CrossRef] [PubMed]
- Hung, T.M.; Lin, C.R.; Chi, Y.C.; Lin, C.Y.; Chen, E.Y.C.; Kang, C.J.; Huang, S.F.; Juang, Y.Y.; Huang, C.Y.; Chang, J.T.C. Body image in head and neck cancer patients treated with radiotherapy: The impact of surgical procedures. Health Qual. Life Outcomes 2017, 15, 165. [Google Scholar] [CrossRef] [Green Version]
- Richardson, A.E.; Broadbent, E.; Morton, R.P. A systematic review of psychological interventions for patients with head and neck cancer. Support Care Cancer 2019, 27, 2007–2021. [Google Scholar] [CrossRef]
- Hutcheson, K.A.; Lewin, J.S.; Barringer, D.A.; Lisec, A.; Gunn, G.B.; Moore, M.W.; Holsinger, F.C. Late dysphagia after radiotherapy-based treatment of head and neck cancer. Cancer 2012, 118, 5793–5799. [Google Scholar] [CrossRef]
- Beeken, L.; Calman, F. A return to "normal eating" after curative treatment for oral cancer. What are the long-term prospects? Eur. J. Cancer Part B Oral Oncol. 1994, 30, 387–392. [Google Scholar] [CrossRef]
- Funk, G.F.; Karnell, L.H.; Christensen, A.J. Long-term health-related quality of life in survivors of head and neck cancer. Arch. Otolaryngol. Head Neck Surg. 2012, 138, 123–133. [Google Scholar] [CrossRef] [Green Version]
- Hammerlid, E.; Taft, C. Health-related quality of life in long-term head and neck cancer survivors: A comparison with general population norms. Br. J. Cancer 2001, 84, 149–156. [Google Scholar] [CrossRef]
- Offerman, M.P. Towards a Better Care for Head and Neck Cancer Patients and their Partners; Erasmus University Rotterdam: Rotterdam, The Netherlands, 2013. [Google Scholar]
- Northouse, L.L.; Katapodi, M.C.; Schafenacker, A.M.; Weiss, D. The Impact of Caregiving on the Psychological Well-Being of Family Caregivers and Cancer Patients. In Seminars in Oncology Nursing; WB Saunders: Philadelphia, PA, USA, 2012; Volume 28, pp. 236–245. [Google Scholar] [CrossRef] [PubMed]
- Vickery, L.E.; Latchford, G.; Hewison, J.; Bellew, M.; Feber, T. The impact of head and neck cancer and facial disfigurement on the quality of life of patients and their partners. Head Neck 2003, 25, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Offerman, M.P.J.; Pruyn, J.F.A.; De Boer, M.F.; Busschbach, J.J.V.; de Jong, R.B. Psychosocial consequences for partners of patients after total laryngectomy and for the relationship between patients and partners. Oral Oncol. 2015, 51, 389–398. [Google Scholar] [CrossRef]
- Li, Q.; Loke, A.Y. The positive aspects of caregiving for cancer patients: A critical review of the literature and directions for future research. Psychooncology 2013, 22, 2399–2407. [Google Scholar] [CrossRef]
- Nijboer, C.; Triemstra, M.; Tempelaar, R.; Sanderman, R.; van den Bos, G.A. Measuring both negative and positive reactions to giving care to cancer patients: Psychometric qualities of the Caregiver Reaction Assessment (CRA). Soc. Sci. Med. 1999, 48, 1259–1269. [Google Scholar] [CrossRef] [PubMed]
- Longacre, M.L.; Galloway, T.J.; Parvanta, C.F.; Fang, C.Y. Medical Communication-related Informational Need and Resource Preferences Among Family Caregivers for Head and Neck Cancer Patients. J. Cancer Educ. 2015, 30, 786–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baghi, M.; Wagenblast, J.; Hambek, M.; Radeloff, A.; Gstoettner, W.; Scherzed, A.; Spaenkuch, B.; Yuan, J.; Hornung, S.; Strebhardt, K.; et al. Demands on caring relatives of head and neck cancer patients. Laryngoscope 2007, 117, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Longacre, M.L.; Ridge, J.A.; Burtness, B.A.; Galloway, T.J.; Fang, C.Y. Psychological functioning of caregivers for head and neck cancer patients. Oral Oncol. 2012, 48, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Kent, E.E.; Mollica, M.A.; Buckenmaier, S.; Smith, A.W. The Characteristics of Informal Cancer Caregivers in the United States. In Seminars in Oncology Nursing; WB Saunders: Philadelphia, PA, USA, 2019; Volume 35, pp. 328–332. [Google Scholar] [CrossRef] [PubMed]
- Aung, S.H.H.; White, K.; Bloomfield, J. The Experiences and the Needs of Caregivers of Patients with Head and Neck Cancer: An Integrative Review. Cancer Nurs. 2021, 44, E361–E373. [Google Scholar] [CrossRef]
- Verdonck-de Leeuw, I.M.; Eerenstein, S.E.; Van der Linden, M.H.; Kuik, D.J.; De Bree, R.; Leemans, C.R. Distress in spouses and patients after treatment for head and neck cancer. Laryngoscope 2007, 117, 238–241. [Google Scholar] [CrossRef]
- Lee, Y.; Lin, P.Y.; Chien, C.Y.; Fang, F.M.; Wang, L.J. A comparison of psychological well-being and quality of life between spouse and non-spouse caregivers in patients with head and neck cancer: A 6-month follow-up study. Neuropsychiatr. Dis. Treat. 2018, 14, 1697–1704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verdonck-de Leeuw, I.M.; Jansen, F.; Brakenhoff, R.H.; Langendijk, J.A.; Takes, R.; Terhaard, C.H.J.; de Jong, R.B.; Smit, J.H.; Leemans, C.R. Advancing interdisciplinary research in head and neck cancer through a multicenter longitudinal prospective cohort study: The NETherlands QUality of life and BIomedical Cohort (NET-QUBIC) data warehouse and biobank. BMC Cancer 2019, 19, 765. [Google Scholar]
- Van Nieuwenhuizen, A.J.; Buffart, L.M.; Smit, J.H.; Brakenhoff, R.H.; Braakhuis, B.J.; de Bree, R.; Leemans, C.R.; Verdonck-de Leeuw, I.M. A comprehensive assessment protocol including patient reported outcomes, physical tests, and biological sampling in newly diagnosed patients with head and neck cancer: Is it feasible? Support Care Cancer 2014, 22, 3321–3330. [Google Scholar] [CrossRef] [Green Version]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Piccirillo, J.F.; Tierney, R.M.; Costas, I.; Grove, L.; Spitznagel, E.L., Jr. Prognostic Importance of Comorbidity in a Hospital-Based Cancer Registry. JAMA 2004, 291, 2441–2447. [Google Scholar] [CrossRef] [Green Version]
- Given, C.W.; Given, B.; Stommel, M.; Collins, C.; King, S.; Franklin, S. The caregiver reaction assessment (CRA) for caregivers to persons with chronic physical and mental impairments. Res. Nurs. Health 1992, 15, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Sandstedt, P.; Littorin, S.; Cröde Widsell, G.; Johansson, S.; Gottberg, K.; Ytterberg, C.; Olsson, M.; Widén Holmqvist, L.; Kierkegaard, M. Caregiver experience, health-related quality of life and life satisfaction among informal caregivers to patients with amyotrophic lateral sclerosis: A cross-sectional study. J. Clin. Nurs. 2018, 27, 4321–4330. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Scott, N. EORTC-QLQ-C30 Reference Values; EORTC Quality of Life Group: Brussels, Belgium, 2008. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. 2020. Available online: https://www.R-project.org/ (accessed on 2 December 2021).
- Erler, N.S.; Rizopoulos, D.; Lesaffre, E.M.E.H. JointAI: Joint Analysis and Imputation of Incomplete Data in R. arXiv 2019, arXiv:1907.10867. [Google Scholar] [CrossRef]
- Hinz, A.; Brähler, E. Normative values for the hospital anxiety and depression scale (HADS) in the general German population. J. Psychosom. Res. 2011, 71, 74–78. [Google Scholar] [CrossRef]
- Hodges, L.J.; Humphris, G.M. Fear of recurrence and psychological distress in head and neck cancer patients and their carers. Psychooncology 2009, 18, 841–848. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Naar-King, S.; Ellis, D.; Kolmodin, K.; Cunningham, P.; Jen, K.L.C.; Saelens, B.; Brogan, K. A randomized pilot study of multisystemic therapy targeting obesity in African-American adolescents. J. Adolesc. Health 2009, 45, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Milbury, K.; Badr, H.; Fossella, F.; Pisters, K.M.; Carmack, C.L. Longitudinal associations between caregiver burden and patient and spouse distress in couples coping with lung cancer. Support Care Cancer 2013, 21, 2371–2379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La, I.S.; Johantgen, M.; Storr, C.L.; Zhu, S.; Cagle, J.G.; Ross, A. Caregiver burden and related factors during active cancer treatment: A latent growth curve analysis. Eur. J. Oncol. Nurs. 2021, 52, 101962. [Google Scholar] [CrossRef] [PubMed]
- Nijboer, C.; Triemstra, M.; Tempelaar, R.; Mulder, M.; Sanderman, R.; van den Bos, G.A. Patterns of caregiver experiences among partners of cancer patients. Gerontologist 2000, 40, 738–746. [Google Scholar] [CrossRef] [Green Version]
- Astrup, G.L.; Hofsø, K.; Bjordal, K.; Rustøen, T. Cancer patients' diagnosis and symptoms and their family caregivers' self-efficacy and social support are associated with different caregiver reactions. Eur. J. Cancer Care 2020, 29, e13311. [Google Scholar] [CrossRef]
- Langenberg, S.M.C.H. Caring for a Patient with Cancer—The Psychosocial Impact on Informal Caregivers. Doctoral Dissertation, Radboud University Nijmegen, Nijmegen, The Netherlands, 2021. [Google Scholar]
- Lee, C.Y.; Lee, Y.; Wang, L.J.; Chien, C.Y.; Fang, F.M.; Lin, P.Y. Depression, anxiety, quality of life, and predictors of depressive disorders in caregivers of patients with head and neck cancer: A six-month follow-up study. J. Psychosom. Res. 2017, 100, 29–34. [Google Scholar] [CrossRef]
- Rigoni, L.; Bruhn, R.F.; De Cicco, R.; Kanda, J.L.; Matos, L.L. Quality of life impairment in patients with head and neck cancer and their caregivers: A comparative study. Braz. J. Otorhinolaryngol. 2016, 82, 680–686. [Google Scholar] [CrossRef] [Green Version]
- Lambert, S.D.; Girgis, A.; Lecathelinais, C.; Stacey, F. Walking a mile in their shoes: Anxiety and depression among partners and caregivers of cancer survivors at 6 and 12 months post-diagnosis. Support Care Cancer 2013, 21, 75–85. [Google Scholar] [CrossRef]
- Nijboer, C.; Triemstra, M.; Tempelaar, R.; Sanderman, R.; van den Bos, G.A. Determinants of caregiving experiences and mental health of partners of cancer patients. Cancer 1999, 86, 577–588. [Google Scholar] [CrossRef]
- Hanly, P.; Maguire, R.; Balfe, M.; Hyland, P.; Timmons, A.; O’Sullivan, E.; Butow, P.; Sharp, L. Burden and happiness in head and neck cancer carers: The role of supportive care needs. Support Care Cancer 2016, 24, 4283–4291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, T.; Johansson, M.; Finizia, C. Well-Being of Caregivers of Patients with Laryngeal Cancer Treated by Radiotherapy. Int. Arch. Otorhinolaryngol. 2020, 24, e170–e174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langenberg, S.M.; van Herpen, C.M.; van Opstal, C.; Wymenga, A.N.; van der Graaf, W.T.; Prins, J.B. Caregivers' burden and fatigue during and after patients' treatment with concomitant chemoradiotherapy for locally advanced head and neck cancer: A prospective, observational pilot study. Support Care Cancer 2019, 27, 4145–4154. [Google Scholar] [CrossRef] [Green Version]
- Utne, I.; Miaskowski, C.; Paul, S.M.; Rustøen, T. Association between hope and burden reported by family caregivers of patients with advanced cancer. Support Care Cancer 2013, 21, 2527–2535. [Google Scholar] [CrossRef]
- Ross, S.; Mosher, C.E.; Ronis-Tobin, V.; Hermele, S.; Ostroff, J.S. Psychosocial adjustment of family caregivers of head and neck cancer survivors. Support Care Cancer 2010, 18, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Badr, H.; Gupta, V.; Sikora, A.; Posner, M. Psychological distress in patients and caregivers over the course of radiotherapy for head and neck cancer. Oral Oncol. 2014, 50, 1005–1011. [Google Scholar] [CrossRef] [Green Version]
- Hagedoorn, M.; Sanderman, R.; Bolks, H.N.; Tuinstra, J.; Coyne, J.C. Distress in couples coping with cancer: A meta-analysis and critical review of role and gender effects. Psychol. Bull. 2008, 134, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Hodges, L.J.; Humphris, G.M.; Macfarlane, G. A meta-analytic investigation of the relationship between the psychological distress of cancer patients and their carers. Soc. Sci. Med. 2005, 60, 1–12. [Google Scholar] [CrossRef]
- Hodgkinson, K.; Butow, P.; Hunt, G.E.; Wyse, R.; Hobbs, K.M.; Wain, G. Life after cancer: Couples' and partners' psychological adjustment and supportive care needs. Support Care Cancer 2007, 15, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Jansen, F.; Brakenhoff, R.H.; Baatenburg de Jong, R.J.; Langendijk, J.A.; Leemans, C.R.; Takes, R.P.; Terhaard, C.H.; Smit, J.H.; Verdonck-de Leeuw, I.M. Study retention and attrition in a longitudinal cohort study including patient-reported outcomes, fieldwork and biobank samples: Results of the Netherlands quality of life and Biomedical cohort study (NET-QUBIC) among 739 head and neck cancer patients and 262 informal caregivers. BMC Med. Res. Methodol. 2022, 22, 27. [Google Scholar]
- Gutiérrez-Colina, A.M.; Lee, J.L.; VanDellen, M.; Mertens, A.; Marchak, J.G. Family Functioning and Depressive Symptoms in Adolescent and Young Adult Cancer Survivors and Their Families: A Dyadic Analytic Approach. J. Pediatr. Psychol. 2017, 42, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Mazanec, S.R.; Voss, J.G. Needs of Informal Caregivers of Patients with Head and Neck Cancer: A Systematic Review. Oncol. Nurs. Forum. 2021, 48, 11–29. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Patients (N = 234) Mean (SD) Frequency (%) | Total no. Missing (%) | Caregivers (N = 234) Mean (SD) Frequency (%) | Total no. Missing (%) | |
|---|---|---|---|---|
| Age, years | 63.6 (9.6) | 0 (0%) | 59.4 (11.3) | 0 (0%) |
| Age, range | 35–85 | 0 (0%) | 19–88 | 0 (0%) |
| Gender | 0 (0%) | 0 (0%) | ||
| Male | 177 (75.6%) | 64 (27.4%) | ||
| Female | 57 (24.4%) | 170 (72.7%) | ||
| Caregiver type | ||||
| Spouse Daughter/son Other | 199 (85.0%) 26 (11.1%) 9 (3.8%) | 0 (0.0%) | ||
| Education level | 15 (6.4%) | 13 (5.5%) | ||
| Low Intermediate High | 83 (35.5%) 62 (26.5%) 74 (31.6%) | 82 (36.9%) 62 (27.9%) 78 (35.1%) | ||
| Tumor site | 0 (0%) | |||
| Oral cavity Oropharynx Hypopharynx Larynx Unknown primary | 68 (29.1%) 77 (32.9%) 13 (5.6%) 67 (28.6%) 9 (3.8%) | |||
| Disease stage | ||||
| I II III IV | 54 (23.1%) 43 (18.4%) 37 (15.8%) 100 (42.7%) | 0 (0%) | ||
| WHO performance | 0 (0%) | |||
| 0 | 176 (75.2%) | |||
| I–II | 58 (24.8%) | |||
| Comorbidity | 16 (6.8%) | |||
| None | 65 (29.8%) | |||
| Mild | 85 (39.0%) | |||
| Moderate | 44 (20.2%) | |||
| Severe | 24 (11.0%) |
| Clinical Cut-Off * | T0 Mean (SD) | M3 Mean (SD) | M6 Mean (SD) | M12 Mean (SD) | M24 Mean (SD) | β (95% CI)/Month | OR | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Caregivers | n = 234 | n = 196 | n = 172 | n = 161 | n = 136 | ||||
| CRA ** | |||||||||
| Self-esteem | ≥4 | 4.2 (0.6) | 4.2 (0.6) | 4.1 (0.6) | 4.1 (0.6) | 4.1 (0.6) | −0.02 (−0.04 to 0.00) | 0.98 | 0.109 |
| Disrupted schedule | ≥3 | 2.6 (0.8) | 2.4 (0.8) | 2.2 (0.9) | 2.1 (0.8) | 1.9 (0.8) | −0.10 (−0.13 to −0.07) | 0.90 | <0.001 |
| Lack of family support | ≥3 | 2.1 (0.7) | 2.1 (0.8) | 2.1 (0.8) | 2.1 (0.8) | 2.2 (0.8) | 0.02 (−0.00 to 0.04) | 1.02 | 0.052 |
| Financial problems | ≥3 | 2.2 (0.8) | 1.9 (0.8) | 1.9 (0.8) | 1.9 (0.8) | 1.7 (0.8) | −0.06 (−0.09 to −0.04) | 0.94 | <0.001 |
| Health problems | ≥3 | 2.1 (0.6) | 2.1 (0.8) | 2.0 (0.7) | 1.8 (0.7) | 1.8 (0.6) | −0.07 (−0.09 to −0.05) | 0.93 | <0.001 |
| Anxiety *** | ≥8 | 7.0 (3.8) | 4.5 (3.6) | 4.1 (3.2) | 4.1 (3.2) | 3.9 (2.7) | −0.09 (−0.11 to −0.07) | - | <0.001 |
| Depression *** | ≥8 | 4.4 (3.6) | 2.7 (3.2) | 2.5 (3.0) | 2.3 (2.9) | 2.1 (2.3) | −0.07 (−0.09 to −0.05) | - | <0.001 |
| Global quality of life *** | <71.2 | 81.3 (14.9) | 82.6 (15.1) | 83.1 (15.2) | 84.3 (15.5) | 83.5 (15.2) | 0.05 (−0.02 to 0.12) | - | 0.278 |
| Physical functioning *** | <89.8 | 91.3 (13.4) | 91.0 (13.9) | 91.1 (13.1) | 91.3 (12.8) | 90.5 (13.4) | −0.03 (−0.09 to 0.02) | - | 0.216 |
| Social functioning *** | <87.5 | 94.9 (12.1) | 93.5 (15.9) | 95.2 (13.2) | 94.5 (12.9) | 95.1 (12.4) | −0.01 (−0.06 to 0.09) | - | 0.787 |
| Caregivers | Baseline Variable | β (95% CI) | p-Value | |
|---|---|---|---|---|
| Self-esteem | Caregiver type (C) | Spouse Daughter/son | “ −0.34 (−1.71 to 1.00) | 0.637 |
| Other | −2.56 (−4.53 to −0.66) | 0.007 | ||
| Disrupted schedule | WHO stage (P) | 0 I–II | “ 0.717 (0.00 to 1.43) | 0.050 |
| Tumor stage (P) | I II III IV | “ 0.75 (−0.16 to 1.69) 1.00 (0.05 to 1.93) 1.63 (0.91 to 2.42) | 0.108 0.033 <0.001 | |
| Education (C) | Low Intermediate High | “ 0.49 (−0.28 to 1.28) 0.77 (0.03 to 1.52) | 0.217 0.039 | |
| Lack of family support | WHO stage (P) | 0 I–II | “ 1.05 (0.25 to 1.83) | 0.010 |
| Caregiver type (C) | Spouse Daughter/son Other | “ −0.59 (−1.94 to 0.73) 2.14 (0.41 to 3.95) | 0.337 0.015 | |
| Financial problems | Comorbidity (P) | None Mild Moderate Severe | “ 0.66 (−0.17 to 1.52) 0.57 (−0.49 to 1.65) 2.20 (−0.0.96 to 3.59) | 0.111 0.277 <0.001 |
| Education (C) | Low Intermediate High | “ −0.16 (−1.01 to 0.68) −1.30 (−2.16 to −0.41) | 0.707 0.003 | |
| Health problems | Tumor stage (P) | I II III IV | “ 0.44 (−0.52 to 1.44) 0.88 (−0.11 to 1.89) 0.83 (0.05 to 1.63) | 0.383 0.085 0.037 |
| Gender (C) | Male Female | “ 0.94 (0.20 to 1.65) | 0.013 |
| Caregivers | Baseline Variable | β (95% CI) | p-Value | |
|---|---|---|---|---|
| Anxiety | Gender (C) | Male Female | “ 0.93 (0.06 to 1.89) | 0.039 |
| Health problems (C) | 0.89 (0.10 to 1.67) | 0.027 | ||
| Depression | Health problems (C) | 1.47 (0.80 to 2.14) | <0.001 | |
| Global QoL | WHO stage (P) | 0 I–II | “ −6.10 (−9.99 to −2.20) | 0.002 |
| Health problems (C) | −9.44 (−12.83 to −6.04) | <0.001 | ||
| Education (C) | Low Intermediate High | “ −1.08 (−5.38 to 3.16) −4.70 (−8.92 to −0.44) | 0.621 0.030 | |
| Physical functioning | WHO stage (P) | 0 I–II | “ −4.17 (−7.93 to −0.54) | 0.026 |
| Age (C) | −0.33 (−0.49 to −0.16) | <0.001 | ||
| Health problems (C) | −8.22 (−11.37 to −4.88) | <0.001 | ||
| Social functioning | Health problems (C) | −9.11 (−11.89 to −6.25) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Hof, K.S.; Hoesseini, A.; Dorr, M.C.; Verdonck-de Leeuw, I.M.; Jansen, F.; Leemans, C.R.; Takes, R.P.; Terhaard, C.H.J.; Baatenburg de Jong, R.J.; Sewnaik, A.; et al. Caregiver Burden, Psychological Distress and Quality of Life among Informal Caregivers of Patients with Head and Neck Cancer: A Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 16304. https://doi.org/10.3390/ijerph192316304
Van Hof KS, Hoesseini A, Dorr MC, Verdonck-de Leeuw IM, Jansen F, Leemans CR, Takes RP, Terhaard CHJ, Baatenburg de Jong RJ, Sewnaik A, et al. Caregiver Burden, Psychological Distress and Quality of Life among Informal Caregivers of Patients with Head and Neck Cancer: A Longitudinal Study. International Journal of Environmental Research and Public Health. 2022; 19(23):16304. https://doi.org/10.3390/ijerph192316304
Chicago/Turabian StyleVan Hof, Kira S., Arta Hoesseini, Maarten C. Dorr, Irma M. Verdonck-de Leeuw, Femke Jansen, C. René Leemans, Robert P. Takes, Chris H. J. Terhaard, Robert Jan Baatenburg de Jong, Aniel Sewnaik, and et al. 2022. "Caregiver Burden, Psychological Distress and Quality of Life among Informal Caregivers of Patients with Head and Neck Cancer: A Longitudinal Study" International Journal of Environmental Research and Public Health 19, no. 23: 16304. https://doi.org/10.3390/ijerph192316304