
The Effects and Costs of Personalized Budgets for People with Disabilities: A Systematic Review

Abstract
:1. Introduction
2. Methods
2.1. Search Terms and Data Sources
- Health and physical well-being,
- Quality of life and psychological well-being,
- Unmet needs,
- Satisfaction with services,
- Service use,
- Costs, and
- Cost-effectiveness.
2.2. Inclusion and Exclusion Criteria
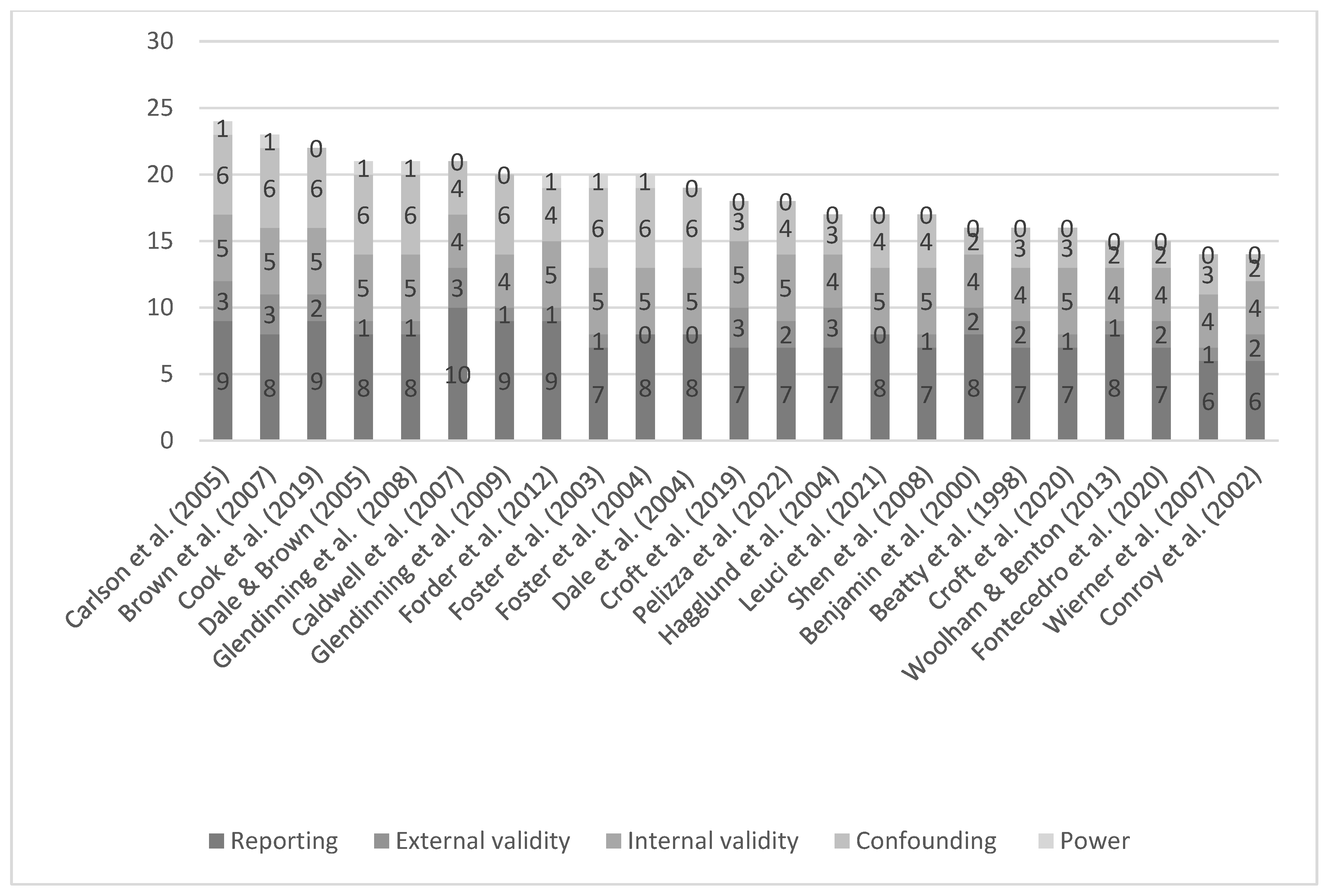
2.3. Quality Assessment
3. Results
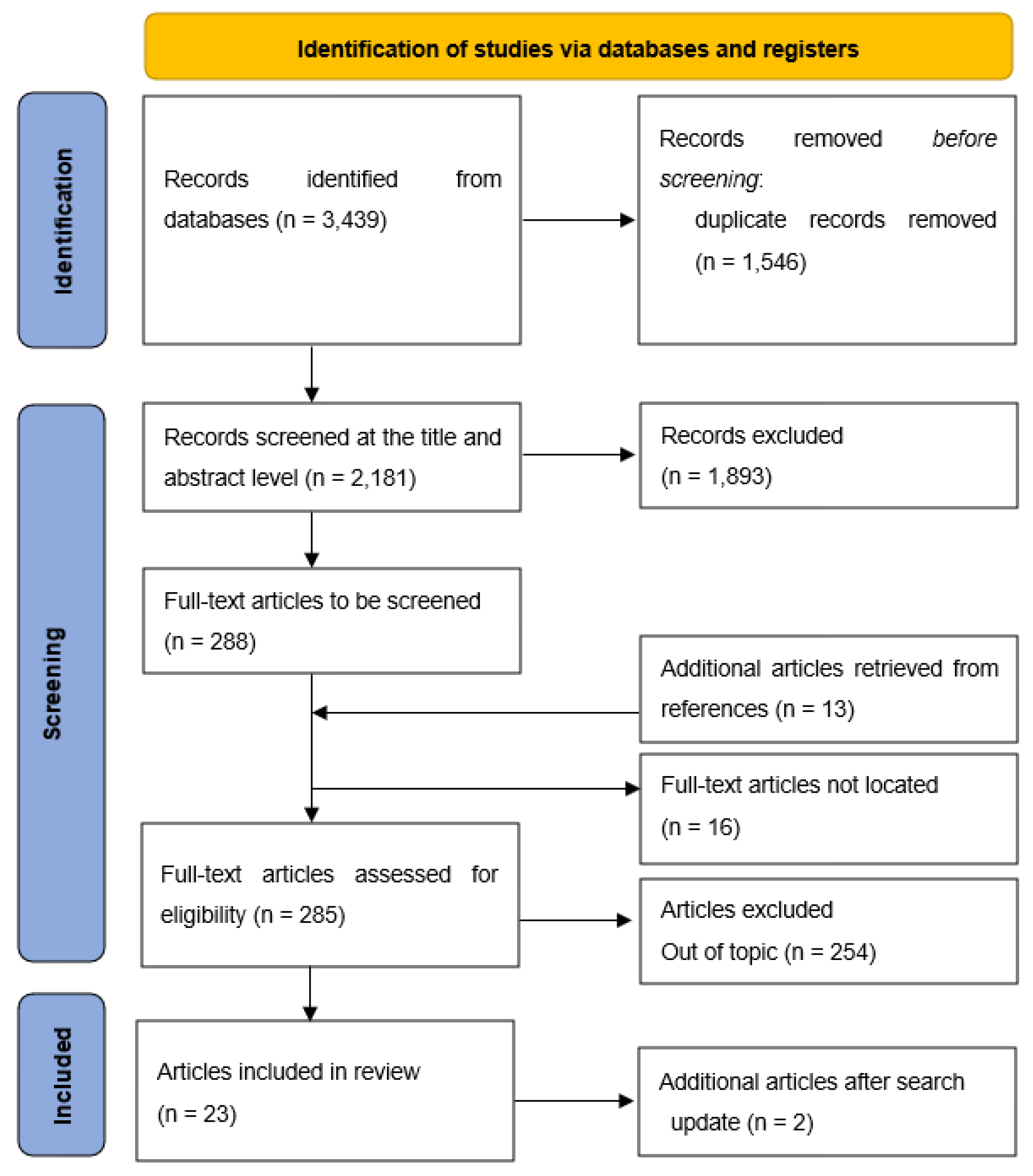
3.1. Search and Selection Results
3.2. Article Characteristics
3.3. Outcomes for Services Users
3.3.1. Physical Disabilities
3.3.2. Intellectual and Developmental Disabilities
3.3.3. Mental Health Conditions
3.3.4. Mixed Disabilities
3.4. Outcomes for Caregivers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations General Assembly. Convention on the Rights of Persons with Disabilities (CRPD); United Nations: Geneva, Switzerland, 2006; Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities/convention-on-the-rights-of-persons-with-disabilities-2.html (accessed on 30 November 2022).
- Dickinson, H.; Glasby, J. The Personalisation Agenda: Implications for the Third Sector; Working Paper; University of Birmingham: Birmingham, UK, 2010; Available online: https://www.birmingham.ac.uk/Documents/college-social-sciences/social-policy/tsrc/working-papers/working-paper-30.pdf (accessed on 30 November 2022).
- Gadsby, E.W.; Segar, J.; Allen, P.; Checkland, K.; Coleman, A.; McDermott, I.; Peckham, S. Personal budgets, choice and health—A review of international evidence from 11 OECD countries: A review of international evidence from 11 OECD countries. Int. J. Public Priv. Health Manag. Econ. 2013, 3, 15–28. [Google Scholar] [CrossRef] [Green Version]
- Mladenov, T. What is good personal assistance made of? Results of a European survey. Disabil. Soc. 2020, 35, 1–24. [Google Scholar] [CrossRef]
- Camoni, L.; Picardi, A.; Venerosi, A. New mode of care. Value and limit of the person-centered care planning for people with mental disability. Ann. Ist. Super. Sanita 2020, 56, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.; Baxter, K.; Glendinning, C.; Irvine, A. Choosing health: Qualitative evidence from the experiences of personal health budget holders. J. Health Serv. Res. Policy 2013, 18, 50–58. [Google Scholar] [CrossRef]
- Webber, M.; Treacy, S.; Carr, S.; Clark, M.; Parker, G. The effectiveness of personal budgets for people with mental health problems: A systematic review. J. Ment. Health 2014, 23, 146. [Google Scholar] [CrossRef] [Green Version]
- Harkes, M.A.; Brown, M.; Horsburgh, D. Self directed support and people with learning disabilities: A review of the published research evidence. Br. J. Learn. Disabil. 2014, 42, 87–101. [Google Scholar] [CrossRef]
- Fleming, P.; McGilloway, S.; Hernon, M.; Furlong, M.; O’Doherty, S.; Keogh, F.; Stainton, T. Individualised funding interventions to improve health and social care outcomes for people with a disability: A mixed-methods systematic review. Campbell Syst. Rev. 2019, 15, e1008. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. Br. Med. J. 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 11th ed.; World Health Organization: Geneva, Switzerland, 2019; Available online: https://icd.who.int/en (accessed on 30 November 2022).
- Garritty, C.; Gartlehner, G.; Kamel, C.; King, V.J.; Nussbaumer-Streit, B.; Stevens, A.; Hamel, C.A.L. Cochrane Rapid Reviews Interim Guidance from the Cochrane; 2020. Available online: http://methods.cochrane.org/sites/methods.cochrane.org.rapidreviews/files/uploads/cochrane_rr_-_guidance-23mar2020-final.pdf (accessed on 30 November 2022).
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, S.R.; Tully, M.A.; Ryan, B.; Bradley, J.M.; Baxter, G.D.; McDonough, S.M. Failure of a numerical quality assessment scale to identify potential risk of bias in a systematic review: A comparison study. BMC Res. Notes 2015, 8, 224. [Google Scholar] [CrossRef]
- Beatty, P.W.; Richmond, G.W.; Tepper, S.; DeJong, G. Personal assistance for people with physical disabilities: Consumer- direction and satisfaction with services. Arch. Phys. Med. Rehabil. 1998, 79, 674–677. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, A.E.; Matthias, R.; Franke, T.M. Comparing Consumer-Directed and Agency Models for Providing Supportive Services at Home. Health Serv. Res. 2020, 35, 351–366. [Google Scholar]
- Brown, R.; Carlson, L.C.; Dale, S.; Foster, L.; Phillips, B.; Schore, J. Cash and Counseling: Improving the Lives of Medicaid Beneficiaries Who Need Personal Care or Home- and Community-Based Services. 2007, Volume 609, pp. 1–168. Available online: https://www.mathematica.org/publications/cash-and-counseling-improving-the-lives-of-medicaid-beneficiaries-who-need-personal-care-or-home-and-communitybased-services (accessed on 30 November 2022).
- Caldwell, J.; Heller, T.; Taylor, S.J. Longitudinal Outcomes of a Consumer-Directed Program Supporting Adults with Developmental Disabilities and Their Families. Intellect. Dev. Disabil. 2007, 45, 161–173. [Google Scholar] [CrossRef]
- Carlson, B.L.; Dale, S.; Foster, L.; Brown, R.; Phillips, B.; Schore, J. Effect of Consumer Direction on Adults’ Personal Care and Well-being in Arkansas, New Jersey and Florida; Mathematica Policy Research, Inc.: Princeton, NJ, USA, 2005; Volume 33, pp. 187–197. [Google Scholar]
- Conroy, J.; Brown, M.; Fullerton, A.; Beamer, S.; Garrow, J.; Boisot, T. Independent Evaluation of California’ s Self-Determination Pilot Projects; Eastern Los Angeles Regional Center: Alhambra, CA, USA, 2002. [Google Scholar]
- Cook, J.A.; Shore, S.; Burke-Miller, J.K.; Jonikas, J.A.; Hamilton, M.; Ruckdeschel, B.; Norris, W.; Markowitz, A.F.; Ferrara, M.; Bhaumik, D. Mental health self-directed care financing: Efficacy in improving outcomes and controlling costs for adults with serious mental illness. Psychiatr. Serv. 2019, 70, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Croft, B.; Battis, K.; Ostrow, L.; Salzer, M.S. Service costs and mental health self-direction: Findings from consumer recovery investment fund self-directed care. Psychiatr. Rehabil. J. 2019, 42, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Croft, B.; Battis, K.; Isvan, N.; Mahoney, K.J. Service utilization before and after self-direction: A quasi-experimental difference-in-differences analysis of Utah’s mental health access to recovery program. Adm. Policy Ment. Health 2020, 47, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Dale, S.; Brown, R.; Philips, B. Medicaid Costs under Consumer Direction for Florida Children with Developmental Disabilities; Mathematica Policy Research, Inc.: Princeton, NJ, USA, 2004. [Google Scholar]
- Dale, S.; Brown, R. The Effect of Cash and Counseling on Medicaid and Medicare Costs: Findings for Adults in Three States; Mathematica Policy Research, Inc.: Princeton, NJ, USA, 2005; pp. 1–64. Available online: https://www.mathematica.org/publications/the-effect-of-cash-and-counseling-on-medicaid-and-medicare-costs-findings-for-adults-in-three-states (accessed on 30 November 2022).
- Fontecedro, E.; Furlan, M.; Tossut, D.; Pascolo-Fabrici, E.; Balestrieri, M.; Salvador-Carulla, L.; D’Avanzo, B.; Castelpietra, G. Individual health budgets in mental health: Results of its implementation in the Friuli Venezia Giulia Region, Italy. Int. J. Environ. Res. Public Health 2020, 17, 5017. [Google Scholar] [CrossRef]
- Forder, J.; Jones, K.; Glendinning, C.; Caiels, J.; Welch, E.; Baxter, K.; Davidson, J.; Windle, K.; Irvine, A.L.; King, D.; et al. Evaluation of the Personal Health Budgets Pilot Programme: Discussion Paper; Personal Social Services Research Unit: Kent, UK, 2012; Available online: http://www.york.ac.uk/inst/spru/research/pdf/phbe.pdf (accessed on 30 November 2022).
- Foster, L.; Dale, S.; Brown, R.; Phillips, B.; Schore, J.; Carlson, B.L. Do Consumer-Directed Medicaid Supportive Services Work for Children with Developmental Disabilities? Mathematica Policy Research, Inc.: Princeton, NJ, USA, 2004. [Google Scholar]
- Glendinning, C.; Moran, N.; Knapp, M.; Fernandez, J.-L.; Netten, A.; Jones, K.; Challis, D.; Wilberforce, M.; Jacobs, S.; Manthorpe, J.; et al. The National Evaluation of the Individual Budgets Pilot Programme—Final Report; IBSEN Project; University of York. Social Policy Research Unit: York, UK, 2008; Available online: http://www.york.ac.uk/inst/spru/pubs/rworks/IbsenMAINsummary.pdf (accessed on 30 November 2022).
- Hagglund, K.; Clark, M.; Farmer, J.; Sherman, A. A comparison of consumer-directed and agency-directed personal assistance services programmes. Disabil. Rehabil. 2004, 26, 518–527. [Google Scholar] [CrossRef]
- Leuci, E.; Pelizza, L.; Landi, G.; Quattrone, E.; Maestri, D.; Azzali, S.; Pelosi, A.; Ceroni, P.; Soncini, C.; Daolio, M.C.; et al. Personal health budget in patients with first episode psychosis: A new rehabilitation model based on a community care system in Italy. Early Interv. Psychiatry 2022, 16, 221–230. [Google Scholar] [CrossRef]
- Pelizza, L.; Leuci, E.; Landi, G.; Maestri, D.; Paulillo, G.; Ceroni, P.; Soncini, C.; Daolio, M.C.; Quattrone, E.; Pellegrini, P. Personal Health Budget as a new rehabilitation model for severe mental illness within a caring community: An Italian evaluation study of beneficial effects. Aust. N. Z. J. Psychiatry 2021, 55, 602–612. [Google Scholar] [CrossRef]
- Shen, C.; Smyer, M.; Mahoney, K.J.; Simon-Rusinowitz, L.; Shinogle, J.; Norstrand, J.; Mahoney, E.; Schauer, C.; Del Vecchio, P. Consumer-directed care for beneficiaries with mental illness: Lessons from New Jersey’s Cash and Counseling program. Psychiatr. Serv. 2008, 59, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Wiener, J.M.; Anderson, W.L.; Khatutsky, G. Are consumer-directed home care beneficiaries satisfied? Evidence from Washington state. Gerontologist 2007, 47, 763–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woolham, J.; Benton, C. The Costs and benefits of personal budgets for older people: Evidence from a single local authority. Br. J. Soc. Work 2013, 43, 1472–1491. [Google Scholar] [CrossRef]
- Foster, L.; Brown, R.; Phillips, B.; Carlson, B.L. Easing the burden of Caregiving: The impact of consumer direction on primary informal caregivers in Arkansas. Gerontologist 2005, 45, 474–485. [Google Scholar] [CrossRef] [PubMed]
- Glendinning, C.; Arksey, H.; Jones, K.C.; Moran, N.; Netten, A.; Rabiee, P. Individual Budgets Pilot Projects: Impact and Outcomes for Carers (Issue 2); Social Policy Research Unit, University of York: York, UK, 2009. [Google Scholar]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Language | English, German, French | All other languages |
| Location | OECD high-income countries | |
| Study type | Quantitative, mixed methods | Qualitative |
| Population | Children and adolescents Adults younger than 65 years Elderly (typically over 65 years) with the onset of disability prior to 18 years of age | Elderly people (if more than 50% of the total study population) |
| Types of disability | Mental health, Autism, Disabilities of physical, intellectual, developmental, or sensory type | Age-related disabilities such as dementia |
| Timeframe | 1985 onwards | Pre-1985 |
| Funding source | State funded | Privately funded |
| Comparator | Presence of a control group or before–after comparative study design | No comparison |
| Author(Year) | Location; Study Design; Disabilities; Duration | Sample Size; % Female; Age (Mean) | Participant Groups | Outcomes of Interest Reported | Quality Score | Intervention |
|---|---|---|---|---|---|---|
| Beatty et al. (1998) [15] | Virginia, US; Quasi-experimental longitudinal comparative study; Physical; n/a cross-sectional study design | 92, (T) 60, (C) 32; (T) 47%, (C) 42%; (T) 41.7, (C) 43.7 | (T) Consumer-directed personal assistance service, in which users could hire, fire, and train their attendants. (C) On the waiting list for consumer-directed care. | Satisfaction with services. | Fair | Personal Assistance Services Program (PAS) |
| Benjamin et al. (2000) [16] | California, US; Controlled cross-sectional study; Mixed; n/a cross-sectional study | 1095, (T) 511, (C) 584; (T) 69.9%, (C) 76.8%; Mean age not reported, (T) 53.6% ≥65 yrs, (C) 50% ≥65 yrs. | (T) Consumer-directed in-home supportive services (IHSS), where users could hire anyone they chose to provide care. (C) Receiving care under the professional home-care agency model. | Service satisfaction, unmet needs. | Fair | In-Home Supportive Services (IHSS) |
| Brown et al. (2007) [17] | Arkansas, New Jersey, Florida, US.; RCT; Mixed; 9 months; | 2825: Arkansas (T) 243, (C) 230, New Jersey (T) 345, (C) 337, Florida adults (T) 419, (C) 392, Florida children (T) 441, (C) 418; Arkansas 67.6%, New Jersey 66.1%, Florida children 37%, Florida adults 45.4%; Mean age not reported, Arkansas 18–39 yrs 27.5%, 40–64 yrs 72.5%, New Jersey 18–39 yrs 33.8%, 40–64 yrs 66.2%, Florida children 3–12 yrs 71.2%, 13–17 yrs 28.8%, Florida adults 18–39 yrs 75.5%, 40–59 yrs 24.5%; | (T) Consumer-directed care where participants receive a monthly allowance to hire workers of their own choosing and to purchase care-related services and goods. (C) Received personal care services or home- and community-based services as usual. | Satisfaction with services, unmet needs, costs. | Good | Cash and Counseling (C&C) |
| Caldwell et al. (2007) [18] | Illinois, US; Longitudinal comparative before-after study; Developmental; 9 years | 87, (T) 38, (C) 49; 49.4%; (T) 36.59, (C) 27.78 | (T) Consumer-directed program where families were provided with an individualised budget and decided what services and supports to purchase. (C) Families on the waiting list for the program. | Service satisfaction, unmet needs. | Good | Home Based Support Services Program (HBSSP) |
| Carlson et al. (2005) [19] | Arkansas, New Jersey, Florida, US; RCT; Mixed; 9 months; | 1966: Arkansas (T) 243, (C) 230, New Jersey (T) 345, (C) 337, Florida adults (T) 419, (C) 392; Arkansas 67.6%, New Jersey 65.1%, Florida adults 45.4%; Mean age not reported, Arkansas 18–39 yrs 27.1%, 40–64 yrs 72.9%, New Jersey 18–39 yrs 34.9%, 40–64 yrs 65.1%, Florida adults 18–39 yrs 75%, 40–59 yrs 25%; | (T) Consumer-directed care where participants receive a monthly allowance to hire workers of their own choosing and to purchase care related services and goods. (C) Received personal care services or home- and community-based services as usual. | Service satisfaction, quality-of-life, unmet needs. | Excellent | Cash and Counseling (C&C) |
| Conroy et al. (2002) [20] | California, US; Controlled before-after study; Intellectual disabilities; 2 years | 77, (T) 63, (C) 14; (T) 28.6%, (C) 35.7%; (T) 25.4, (C) 27.9 | (T) Self-determination program in which participants received an individual budget. (C) A group of people who wanted to participate, receiving traditional services | Choice, perception of quality-of-life, adaptive and challenging behaviours. | Fair | Pilot project on self-determination |
| Cook et al. (2019) [21] | Texas, US; Randomised controlled trial; Mental illness; 24 months | 216, (T) 114, (C) 102; 62%; 41.6 yrs | (T) Received self-directed care by means of an individual budget for the purchase of services and goods corresponding to plan goals. (C) Services as usual | Self-perceived recovery, psychosocial status, psychiatric and somatic symptoms, satisfaction with services, costs of services. | Good | Self-Directed Care Program (SDC) |
| Croft et al. (2019) [22] | Pennsylvania, US; Uncontrolled pre-post study; Mental health conditions; 3 years | 45; 71.1%; 51.5 yrs | (T) Self-directed care in which participants banked funds by intentionally reducing their use of some mental health services and applying the cost savings towards flexible spending of approved nonclinical goods and services. | Service use, costs. | Fair | Consumer Recovery Investment Fund Self-Directed Care II (CRIF-SDF II) |
| Croft et al. (2020) [23] | Utah, US; Quasi-experimental before-after comparative study; Mental health conditions; Enrolment average of 199 days | 623, (T) 94, (C) 529; (T) 38.3%, (C) 38.37%; (T) 42.38, (C) 42.85 | (T) Self-direction in which funds were allocated from a flexible budget to meet recovery goals. (C) Received traditional Medicaid-funded and state-funded services. | Service use. | Fair | Mental Health Access to Recovery (MHATR) |
| Dale et al. (2004) [24] | Florida, US; RCT; Children, Developmental; 9 months | 1002, (T) 501, (C) 501; (T) 38.1%, (C) 35.9%; <12 yrs (T) 63.5%, (C) 64.1%; | (T) Parents of treatment group members were given the opportunity to receive a monthly allowance they could use to hire their choice of caregivers or to buy other services or goods to meet their child’s care needs. (C) Received traditional waiver services. | Costs. | Good | Cash and Counseling (C&C) |
| Dale & Brown (2005) [25] | Arkansas, New Jersey, Florida, US; RCT; Mixed; 1 to 2 years; | 2282: Arkansas 556, New Jersey 813, Florida adults 913; Arkansas 67.6%, New Jersey 66.1%, Florida adults 45.3%; Mean age not reported, Arkansas 18–39 yrs 27.5%, 40–64 yrs 72.5%, New Jersey 18–39 yrs 33.7%, 40–64 yrs 66.31%, Florida adults 18–39 yrs 75.5%, 40–59 yrs 24.5%; | (T) Consumer-directed care where participants receive a monthly allowance to hire workers of their own choosing and to purchase care related services and goods. (C) Received personal care services or home- and community-based services as usual. | Costs, satisfaction with care, unmet needs. | Good | Cash and Counseling (C&C) |
| Fontecedro et al. (2020) [26] | Italy; Observational comparative cross- sectional study; Mental health conditions; n/a cross-sectional study design | 128, (T) 67, (C) 61; (T) 37.3%, (C) 45.9%; Mean age not reported. 20–59 yrs (T) 74.6%, (C) 65.4% | (T) Received an individual budget. (C) Care maintained as usual. | Health of the Nation Outcome Scale | Fair | Individual Health Budget (IHB) |
| Forder et al. (2012) [27] | England; RCT; Mental health conditions; 12 months | 197, (T) 105, (C) 92; (T) 49%, (C) 50%; (T) 45 yrs, 11% ≥75 yrs, (C) 53 yrs, 10% ≥75 yrs | (T) Received a personal health budget. (C) Continued conventional support arrangement. | Care-related quality-of-life, health-related quality-of-life, psychological well-being, subjective well-being, costs, cost-effectiveness. | Good | Personal HealthBudget Pilot Programme (PHB) |
| Foster et al. (2004) [28] | Florida, US; RCT; Children, Developmental; 9 months | 859, (T) 441, (C) 418; (T) 38.5%, (C) 35.2%; < 12 yrs (T) 63.3%, (C) 63.4%; | (T) Consumer-directed care where parents could use the allowance to hire their choice of caregivers and to buy other services and goods to meet their child’s care needs. (C) Received personal care services or home- and community-based services as usual. | Satisfaction with child’s care, child’s unmet needs, child’s quality of life. | Good | Cash and Counseling (C&C) |
| Glendinning et al. (2008) [29] | UK; Randomised controlled trial; Mixed; 6 months | 959, (T) 510, (C) 449; 56%; 57 yrs | (T) Participants received an individual budget in addition to traditional social care services. (C) Continued to receive traditional social care support. | Perceived quality of life, psychological well-being, social care outcomes, self-perceived health, satisfaction with services, costs, cost-effectiveness. | Good | Individual Budgets Pilot Programme (IBPP) |
| Hagglund et al. (2004) [30] | Missouri, US; Controlled cross-sectional study; Physical; Enrolled for a minimum of 1 month | 114, (T) 61, (C) 53; 32%; 48 yrs | (T) Consumer-directed personal assistance services in which consumers hired and managed their own personal assistants. (C) Received services through an agency-directed model. | Unmet needs, satisfaction, quality-of-life | Fair | Assistance Services programme (PAS) |
| Leuci et al. (2021) [31] | Parma, Italy; Longitudinal comparative before-after study; Mental health conditions; 2 years | 104, (T) 49, (C) 55; 36%, (T) 26.5%; (C) 43.6; 28 yrs, (T) 26 yrs, (C) 31 yrs. | (T) Received a personal health budget as a part of a specific program. (C) Care maintained in the specific program without a personal budget. | Brief Psychiatric Rating Scale, Global Assessment of Functioning, Health of the Nation Outcome Scale | Fair | Personal Health Budget (PHB) |
| Pelizza et al. (2022) [32] | Parma, Italy; Uncontrolled pre-post study; Mental health conditions; 2 years | 137; 38%; 33 yrs. | (T) Received a multi-axis personal health budget. | Brief Psychiatric Rating Scale, Global Assessment of Functioning, Health of the Nation Outcome Scale | Fair | Personal Health Budget (PHB) |
| Shen et al. (2008) [33] | New Jersey, US; RCT; Mental health conditions; 9 months | 228, (T) 109, (C) 119; (T) 77%, (C) 64%; (T) 18–39 yrs 31%, 40–64 yrs 69%, (C) 18–39 yrs 29%, 40–64 yrs 71%. | (T) Consumer-directed care where participants receive a monthly allowance to hire workers of their own choosing and to purchase care related services and goods. (C) Received personal care services or home- and community-based services as usual. | Satisfaction with services, satisfaction with quality-of-life. | Fair | Cash and Counseling (C&C) |
| Wiener et al. (2007) [34] | Washington State, US; Controlled cross-sectional study; Various; n/a cross-sectional study design | 229, (T) 124, (C) 105; 62.9%; Mean age not reported. 28% ≤44 yrs, 72% aged 45–64. | (T) Consumer-directed personal assistance services where consumers are responsible for hiring, orienting, supervising, and finding replaces for the caregiver. (C) Receiving agency-directed care. | Satisfaction with services. | Fair | Home- and Community-Based Services (HCBS) |
| Woolham and Benton (2013) [35] | England; Controlled cross-sectional study; Various; n/a cross-sectional study design | 402, (T) 126, (C) 276 (under 65 yrs); (T) 66.1%, (C) 35.8%, (includes over 65 yrs); (T) 51.5 yrs, (C) 54.9 yrs (includes over 65 yrs) | (T) Received a personal budget. (C) Received traditional services. | Psychological well-being, activities of daily living, costs, cost-effectiveness. | Fair | Personal Budget (PB) |
| Foster et al. (2003) [36] | Arkansas, US; | Survey of 1433 carers; 39 or younger 22.5%, 40–64 yrs 64.1%, 65 or older 13.5%. | (T) Consumer-directed care where parents could use the allowance to hire their choice of caregivers and to buy other services and goods to meet their child’s care needs. (C) Received personal care services or home- and community-based services as usual. | Hours of care provided, satisfaction, well-being. | Good | Cash and Counseling (C&C) |
| Glendinning et al. (2009) [37] | UK; | Carers: 129, (T) 69, (C) 60, Physical disabilities (T) 8, (C) 11, Older people (T) 16, (C) 17, Learning disabilities (T) 32, (C) 38, Mental health conditions (T) 4, (C) 3 All ≥25 yrs, 45–59 yrs, (T) 57%, (C) 58%, ≥60 yrs, (T) 32%, (C) 36%. | (T) Participants received an individual budget in addition to traditional social care services. (C) Continued to receive traditional social care support | Quality-of-life, well-being, social care outcomes, self-perceived health, impact, satisfaction with services. | Good | Individual Budget Pilot Programme (IBPP) |
| Article | Age Group | Treatment (%) | Control (%) |
|---|---|---|---|
| Benjamin et al. (2000) [16] | ≥65 years | 53.6 | 50 |
| Fontecedro et al. (2020) [26] | ≥60 years | 25.4 | 34.4 |
| Forder et al. (2012) [27] | ≥75 years | 11 | 10 |
| Outcome | Article | Benefits Associated with Personal Budgets | Disadvantages Reported with Personal Budgets |
|---|---|---|---|
| Service Users’ Outcomes | |||
| Physical disabilities | |||
| Service satisfaction | Beatty et al. (1998) [15] Hagglund et al. (2004) [30] | More satisfied with the costs of care, choice, and control over care, control over assistant’s work schedule, authority to direct assistant, and the availability of assistant in both everyday care and emergency situations. Greater satisfaction with daily living and community living. | |
| Intellectual and developmental disabilities | |||
| Service satisfaction | Caldwell et al. (2007) [18] Foster et al. (2004) [28] | Increased satisfaction with services over time. Increased satisfaction with caregiver’s schedule, relationship with the caregiver, help around the house and community, and overall care arrangements. | |
| Unmet needs | Caldwell et al. (2007) [18] Foster et al. (2004) [28] | Fewer service needs for occupational therapy, social/recreational activities, educational/vocational training, assistance obtaining benefits, and assistance obtaining vocational services. Fewer unmet needs for help with daily living activities, household activities, transportation, and routine health care. | |
| Quality of life | Conroy et al. (2002) [20] Foster et al. (2004) [28] | Increased control and power over decisions. Better perception of quality of life. Some evidence of increases in adaptive behaviour. Higher child’s quality of life. | |
| Cost | Dale et al. (2004) [24] | Higher monthly costs and annual expenditures. | |
| Mental health disabilities | |||
| Quality of life | Cook et al. (2019) [21] Fontecedro et al. (2020) [26] Leuci et al. (2021) [31] Pelizza et al. (2022) [32] Shen et al. (2008) [33] | Higher perceived level of recovery, especially in the domains of goal orientation and personal confidence. Improvements in self-esteem, coping mastery, and perception of service delivery being supportive of personal autonomy. Lower somatic symptom severity. Less likely to be at risk for problems in the availability of resources for work and recreation activities. Improvements in global functioning and in the domains of impairment, psychiatric symptoms, and behavioural problems. Improvements in negative symptoms and social behaviour. Higher level of satisfaction with life. | Increased risk of severe to very severe cognitive problems and problems related to hallucinations and delusions. Higher risk for moderately severe problems with activities of daily living. |
| Service satisfaction | Cook et al. (2019) [21] Shen et al. (2008) [33] | Higher satisfaction with mental health services. Higher satisfaction with their caregiver’s schedule, help around the house and community, and overall care arrangements. | |
| Service use | Croft et al. (2020) [23] | Increased use of rehabilitation and outpatient treatment services. | |
| Cost | Croft et al. (2019) [22] Forder et al. (2012) [27] | Reduced costs for mental health clinical outpatient services. Significant reduction over time in indirect costs. Cost-effective when using ASCOT scale. | |
| Mixed disabilities | |||
| Quality of life | Glendinning et al. (2008) [29] Woolham and Benton (2013) [35] | Higher self-reported quality of life for mental health service users. More likely to feel in control of daily life. Better psychological well-being. | |
| Service satisfaction | Benjamin et al. (2000) [16] Brown et al. (2007) [17]; Carlson et al. (2005) [19] Dale and Brown (2005) [25] Glendinning et al. (2008) [29] | More positive ratings for technical quality of services, service impact, general satisfaction, and caregiver’s interpersonal manner. More satisfied with caregiver’s schedule, relationship with caregiver, help with Daily Living Activities, help around the house/community, overall care arrangements, and help with routine health care. Higher satisfaction with overall care. Higher satisfaction with quality of care for young physically disabled adults. | |
| Unmet needs | Benjamin et al. (2000) [16] Brown et al. (2007) [17] Dale and Brown (2005) [25] | Fewer unmet needs for help with daily living activities, household activities, transportation, and routine health care. Fewer unmet needs. | More ADL needs unmet. |
| Cost | Brown et al. (2007) [17] Dale and Brown (2005) [25] Glendinning et al. (2008) [29] | Lower costs for home health services, nursing facilities, and inpatient care. Lower costs for home care and Independent Living Fund.Some evidence of cost-effectiveness. | Higher monthly costs. Higher costs for personal assistance services and total care. Higher cost for personal assistants. Higher care management costs. |
| Caregivers’ outcomes | |||
| Quality of life | Foster et al. (2003) [36] Glendinning et al. (2009) [37] | Lower levels of emotional, financial, and physical strain.Higher quality of life. More likely to be fully occupied in activities of their choice. | |
| Satisfaction with services | Foster et al. (2003) [36] | More satisfied with service user’s overall care. | |
| Hours of care provided | Foster et al. (2003) [36] | Fewer hours of care provided by live-in caregivers. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robinson, M.; Blaise, M.; Weber, G.; Suhrcke, M. The Effects and Costs of Personalized Budgets for People with Disabilities: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 16225. https://doi.org/10.3390/ijerph192316225
Robinson M, Blaise M, Weber G, Suhrcke M. The Effects and Costs of Personalized Budgets for People with Disabilities: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(23):16225. https://doi.org/10.3390/ijerph192316225
Chicago/Turabian StyleRobinson, Marguerite, Marie Blaise, Germain Weber, and Marc Suhrcke. 2022. "The Effects and Costs of Personalized Budgets for People with Disabilities: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 23: 16225. https://doi.org/10.3390/ijerph192316225