
Spatiotemporal Patterns of Adverse Pregnancy Outcomes in Rural Areas of Henan, China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area and Data
2.2. APO Outcomes
2.3. Variables
2.4. Geolocation
2.5. Methods of APO Analysis
3. Results
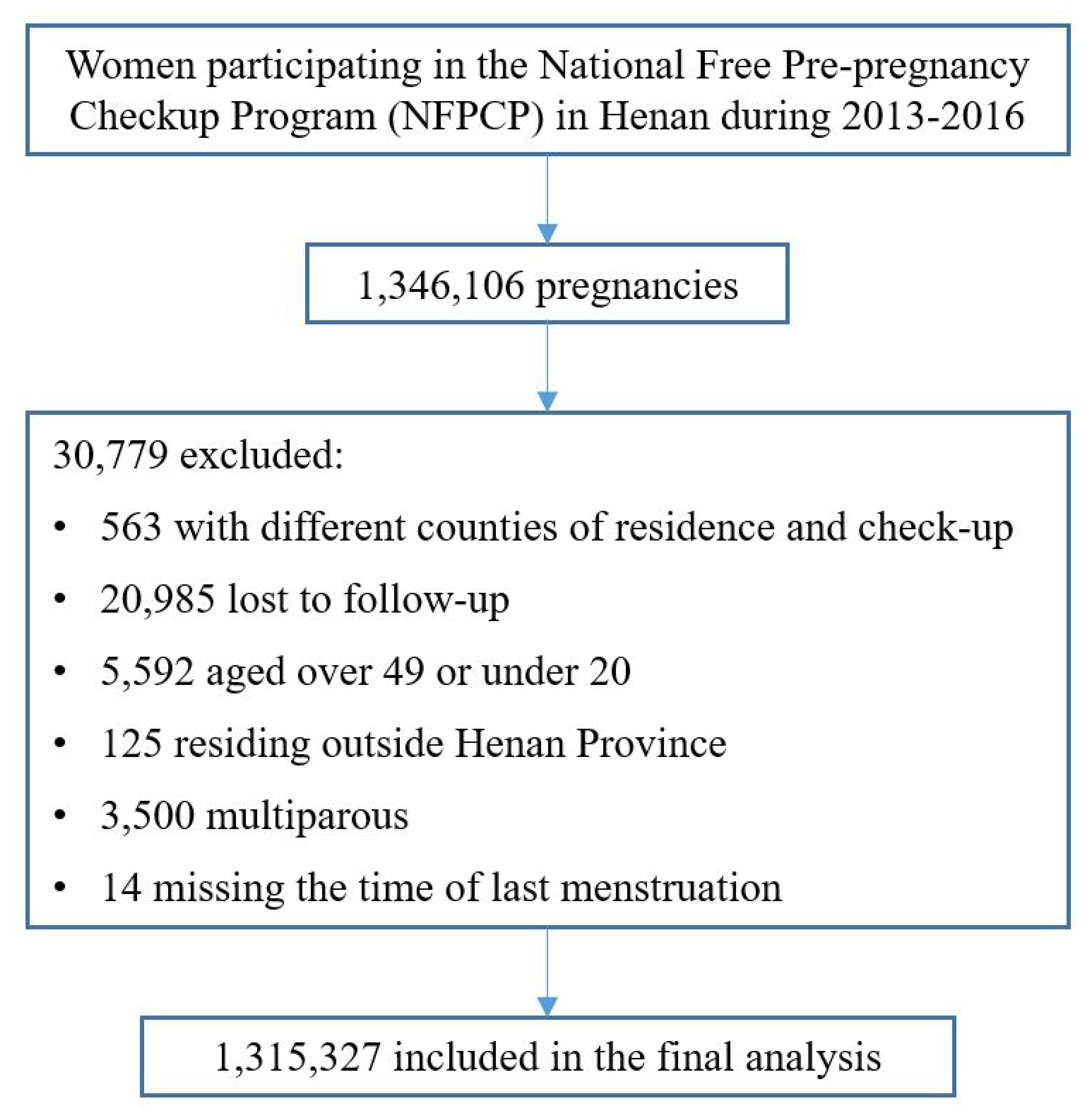
3.1. Participants
3.2. Baseline Characteristics by APOs
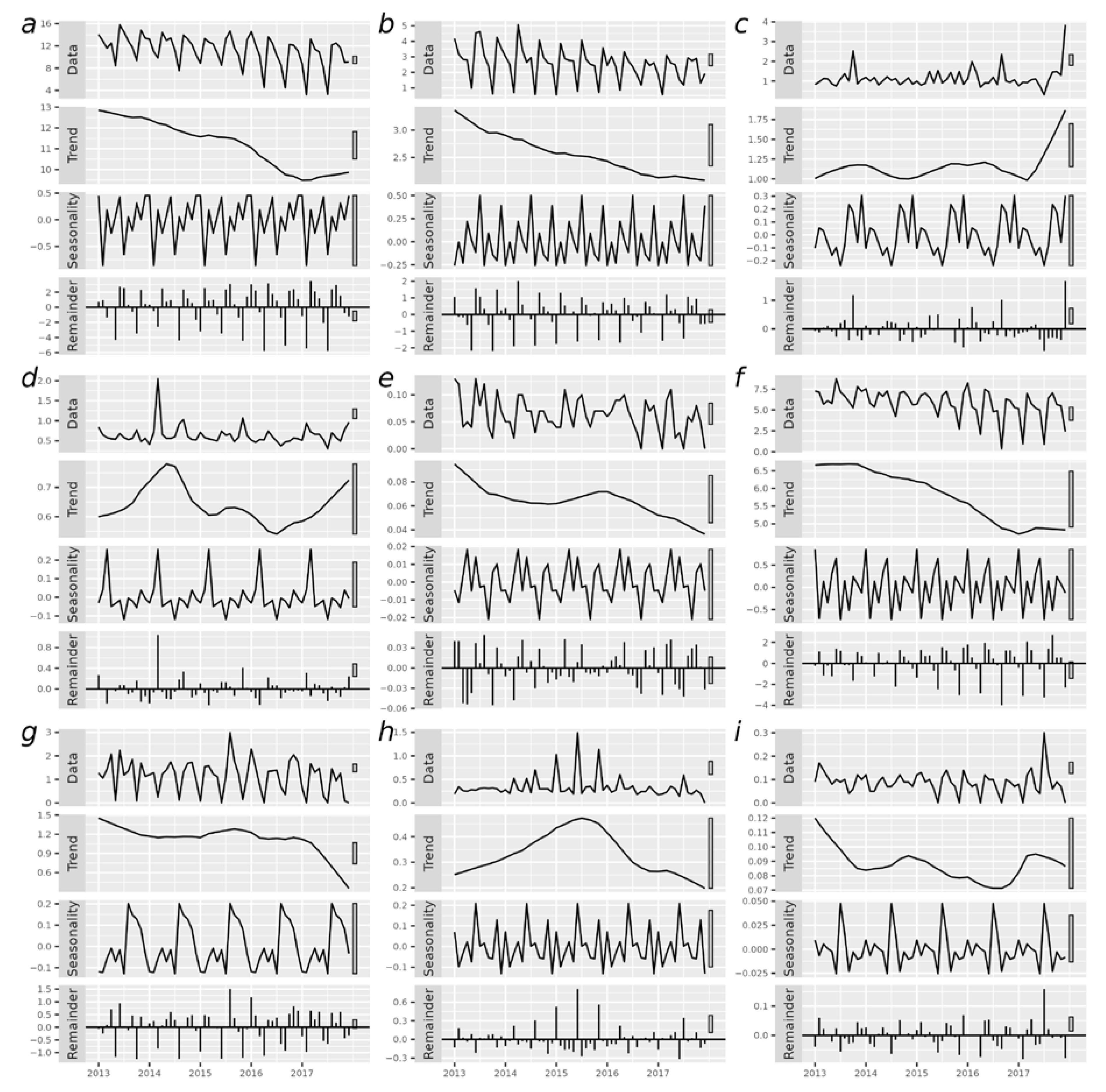
3.3. Temporal Distribution of APOs over Time
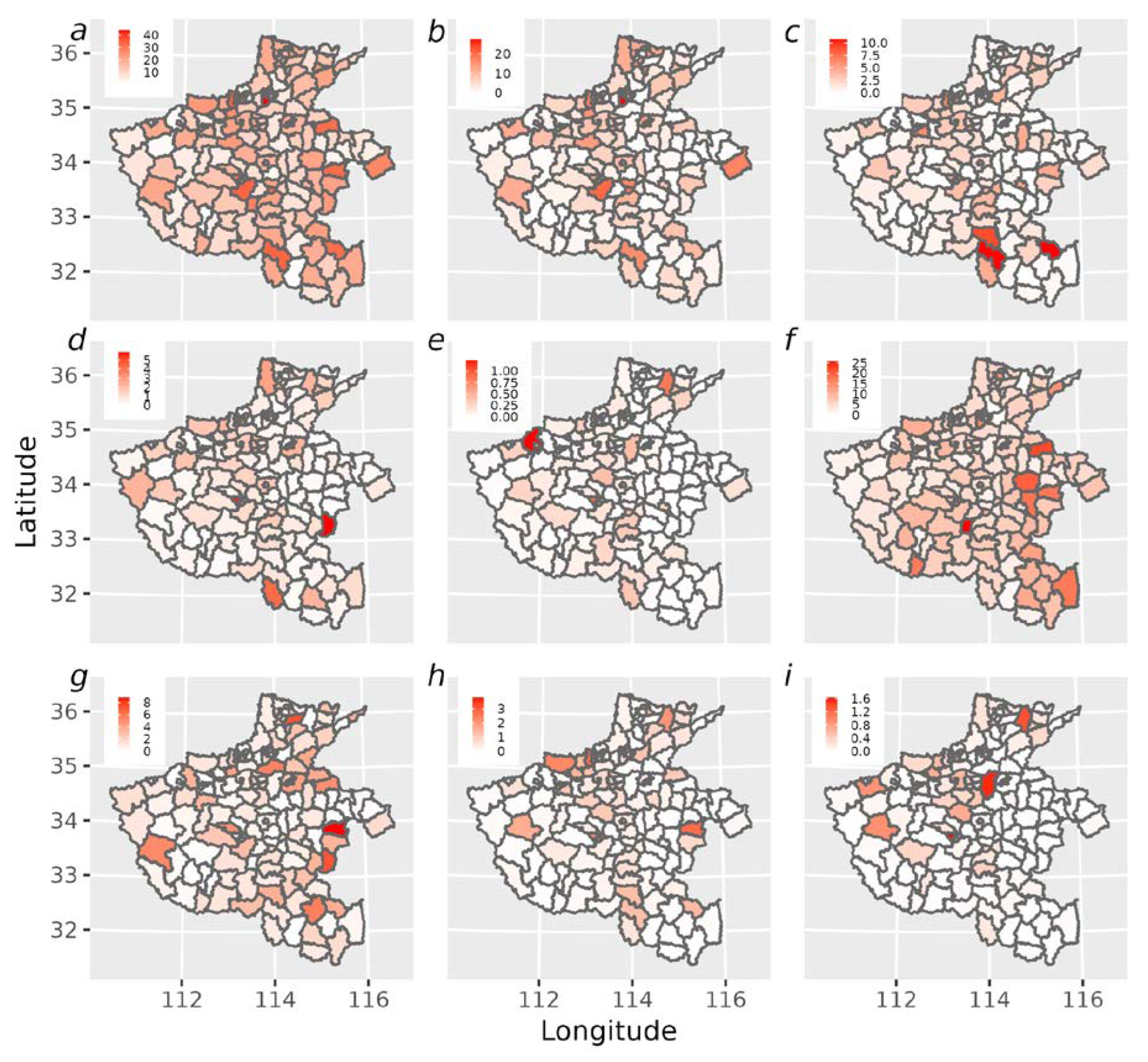
3.4. Spatial Patterns of APOs
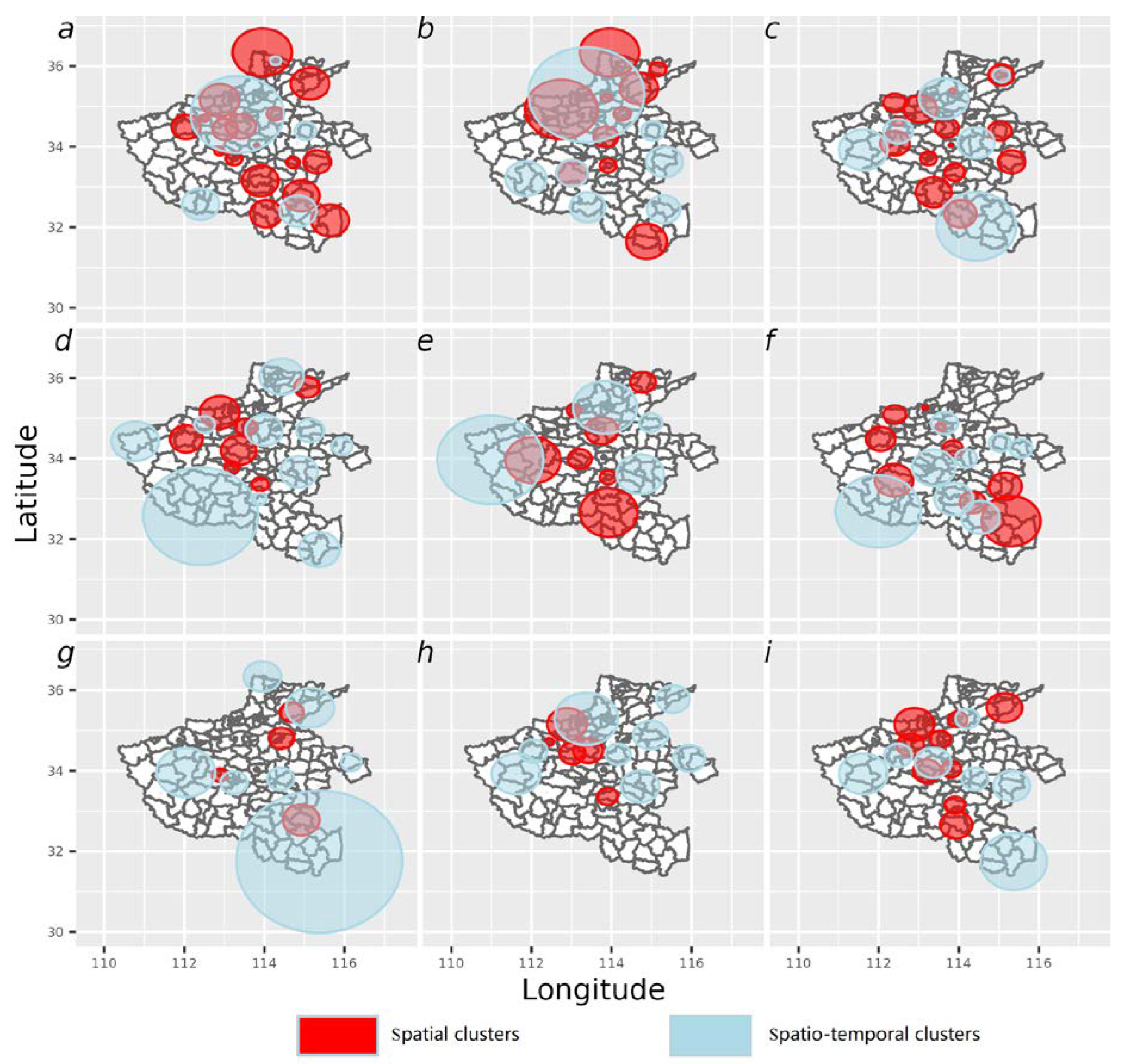
3.5. Spatio-Temporal Clustering of APOs
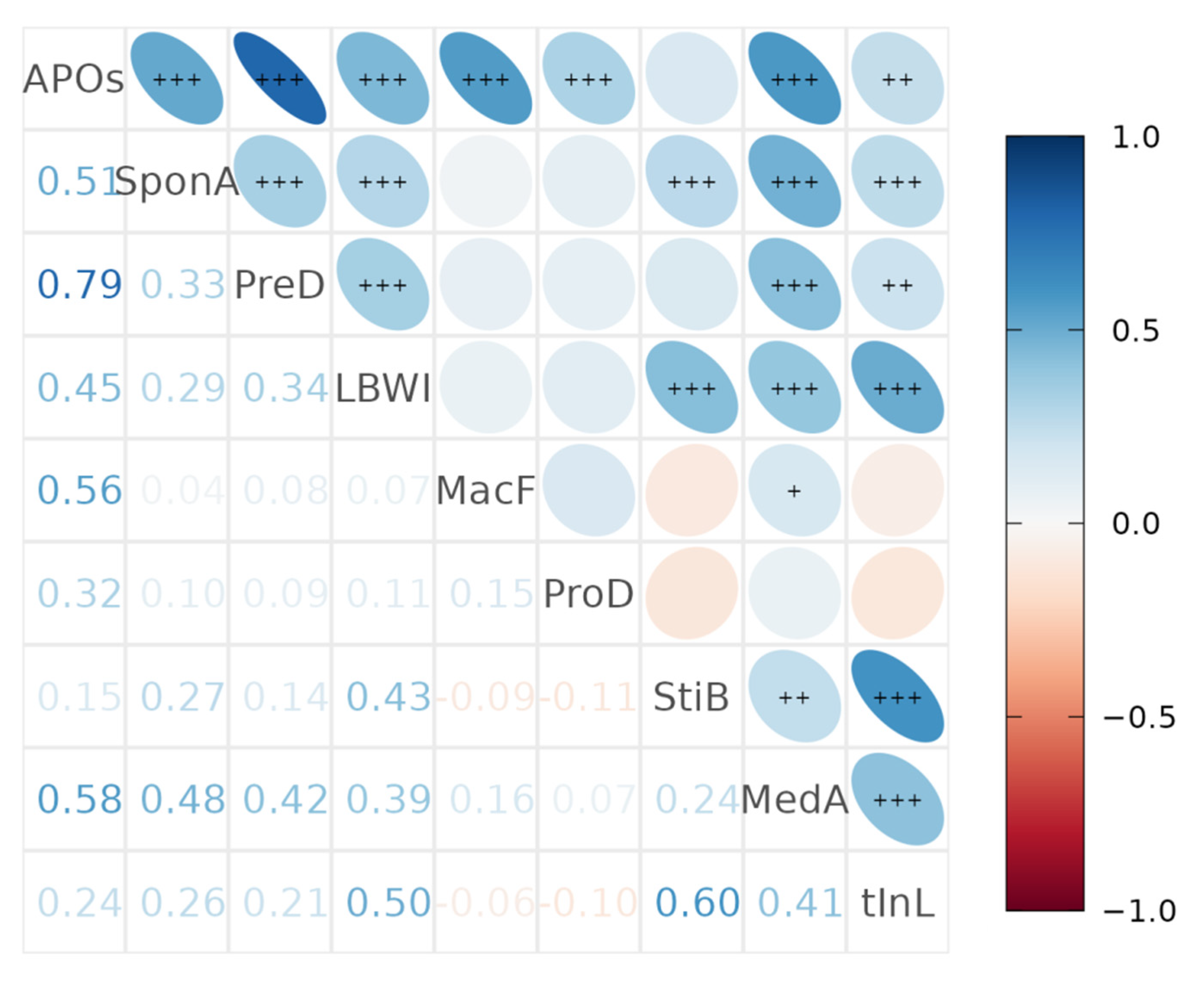
3.6. Spatio-Temporal Correlation across Eight Types of APOs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, M.Y.; Guerra, M.M.; Kaplowitz, E.; Laskin, C.A.; Petri, M.; Branch, D.W.; Lockshin, M.D.; Sammaritano, L.R.; Merrill, J.T.; Porter, T.F.; et al. Complement activation predicts adverse pregnancy outcome in patients with systemic lupus erythematosus and/or antiphospholipid antibodies. Ann. Rheum Dis. 2018, 77, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Panaitescu, A.M.; Syngelaki, A.; Prodan, N.; Akolekar, R.; Nicolaides, K.H. Chronic hypertension and adverse pregnancy outcome: A cohort study. Ultrasound Obs. Gynecol. 2017, 50, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beta, J.; Khan, N.; Fiolna, M.; Khalil, A.; Ramadan, G.; Akolekar, R. Maternal and neonatal complications of fetal macrosomia: Cohort study. Ultrasound Obs. Gynecol. 2019, 54, 319–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Liu, X.R.; He, C.H.; Miao, L.; Kang, L.N.; Li, X.H.; Zhu, J.; Li, Q.; Huang, Y.; Wang, Y.P. Analysis of mortality and leading causes of death in Chinese children under 5-year-old between 2010 and 2016. Chin. Prev. Med. J. 2019, 53, 411–414. [Google Scholar]
- Crump, C.; Sundquist, J.; Sundquist, K. Preterm delivery and long term mortality in women: National cohort and co-sibling study. BMJ (Clin. Res. Ed.) 2020, 370, m2533. [Google Scholar] [CrossRef]
- Wilcox, A.; Weinberg, C.; O’Connor, J.; Baird, D.; Schlatterer, J.; Canfield, R.; Armstrong, E.; Nisula, B. Incidence of early loss of pregnancy. N. Engl. J. Med. 1988, 319, 189–194. [Google Scholar] [CrossRef]
- Avalos, L.A.; Galindo, C.; Li, D. A systematic review to calculate background miscarriage rates using life table analysis. Birth Defects Res. Part A Clin. Mol. Teratol. 2012, 94, 417–423. [Google Scholar] [CrossRef]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Li, M.Y.; Wang, S.X.; Ma, M.X.; Chen, X.L.; Hu, J.H. Changing trend and cause of death of children under 5 years old in China, 2000—2017. Mod. Prev. Med. 2021, 48, 389–392+397. [Google Scholar]
- Jia, P. Spatial lifecourse epidemiology. 2022, 3, e57–e59. [Google Scholar] [CrossRef] [Green Version]
- Root, E.D.; Bailey, E.D.; Gorham, T.; Browning, C.; Song, C.; Salsberry, P. Geovisualization and Spatial Analysis of Infant Mortality and Preterm Birth in Ohio, 2008–2015: Opportunities to Enhance Spatial Thinking. Public Health Rep. 2020, 135, 472–482. [Google Scholar] [CrossRef]
- Tesema, G.A.; Mekonnen, T.H.; Teshale, A.B. Spatial distribution and determinants of abortion among reproductive age women in Ethiopia, evidence from Ethiopian Demographic and Health Survey 2016 data: Spatial and mixed-effect analysis. PLoS ONE 2020, 15, e0235382. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Yang, L.; Bai, X.; Du, W.; Shen, G.; Fei, J.; Wang, Y.; Chen, A.; Chen, Y.; Zhao, M. Maternal ambient air pollution exposure with spatial-temporal variations and preterm birth risk assessment during 2013–2017 in Zhejiang Province, China. Environ. Int. 2019, 133, 105242. [Google Scholar] [CrossRef] [PubMed]
- Miao, H.; Li, B.; Li, W.; Yao, F.; Chen, Y.; Chen, R.; Lin, J.; Wu, Y.; Guo, P.; Zhao, Q. Adverse birth outcomes in Guangdong province, China, 2014–2017: A spatiotemporal analysis of 2.9 million births. BMJ Open 2019, 9, e030629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, C.; Amrhein, C.; Shah, P.; Aziz, K.; Osornio-Vargas, A. Spatiotemporal Patterns of Small for Gestational Age and Low Birth Weight Births and Associations With Land Use and Socioeconomic Status. Environ. Health Insights 2019, 13, 1178630219869922. [Google Scholar] [CrossRef] [Green Version]
- Skrivankova, V.; Zwahlen, M.; Adams, M.; Low, N.; Kuehni, C.; Egger, M. Spatial epidemiology of gestational age and birth weight in Switzerland: Census-based linkage study. BMJ Open 2019, 9, e027834. [Google Scholar] [CrossRef] [Green Version]
- Council, Office of the Leading Group for the 7th National Population Census of the State. Tabulation on the 2010 Population Census of the People’s Republic of China; China Statistics Press: Beijing, China, 2012. [Google Scholar]
- National Bureau of Statistics. Bulletin of the Seventh National Population Census (No. 3); National Bureau of Statistics: Beijing, China, 2021. [Google Scholar]
- Wang, L.; Yang, Y.; Liu, F.; Yang, A.; Xu, Q.; Wang, Q.; Shen, H.; Zhang, Y.; Yan, D.; Peng, Z.; et al. Paternal smoking and spontaneous abortion: A population-based retrospective cohort study among non-smoking women aged 20–49 years in rural China. J. Epidemiol. Community Health 2018, 72, 783–789. [Google Scholar] [CrossRef]
- Xu, Q.; Yang, Y.; Liu, F.; Wang, L.; Wang, Q.; Shen, H.; Xu, Z.; Zhang, Y.; Yan, D.; He, Y.; et al. Preconception Hb concentration with risk of spontaneous abortion: A population-based cohort study in over 3.9 million women across rural China. Public Health Nutr. 2020, 23, 2963–2972. [Google Scholar] [CrossRef]
- Heslehurst, N.; Vieira, R.; Hayes, L.; Crowe, L.; Jones, D.; Robalino, S.; Slack, E.; Rankin, J. Maternal body mass index and post-term birth: A systematic review and meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2017, 18, 293–308. [Google Scholar] [CrossRef] [Green Version]
- Bromwich, P. Late abortion. Br. Med. J. (Clin. Res. Ed.) 1987, 294, 527–528. [Google Scholar] [CrossRef] [Green Version]
- Tu, J.; Tu, W.; Tedders, S. Spatial variations in the associations of term birth weight with ambient air pollution in Georgia, USA. Environ. Int. 2016, 92, 146–156. [Google Scholar] [CrossRef]
- Association, Family Planning Branch of Chinese Medical. Clinical Diagnosis and Treatment Guide and Technical Operation Specification Family Planning Volume; People’s Medical Publishing House: Beijing, China, 2017. [Google Scholar]
- Liang, Z.; Yang, Y.; Yi, J.; Qian, Z.; Zhang, Z.; McMillin, S.; Liu, E.; Lin, H.; Liu, G. Maternal PM exposure associated with stillbirth: A large birth cohort study in seven Chinese cities. Int. J. Hyg. Environ. Health 2021, 236, 113795. [Google Scholar] [CrossRef] [PubMed]
- Xu, M. mapchina: China Administrative Divisions Geospatial Shapefile Data. 2020. Available online: https://github.com/xmc811/mapchina (accessed on 29 August 2022).
- Cleveland, R.B.; Cleveland, W.S.; McRae, J.E.; Terpenning, I. STL: A seasonal-trend decomposition. J. Off. Stat. 1990, 6, 3–73. [Google Scholar]
- Kourentzes, N. tsutils: Time Series Exploration, Modelling and Forecasting. 2020. Available online: https://github.com/trnnick/tsutils/ (accessed on 29 August 2022).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Pebesma, E. Simple Features for R: Standardized Support for Spatial Vector Data. R J. 2018, 10, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Han, J.; Zhu, L.; Kulldorff, M.; Hostovich, S.; Stinchcomb, D.G.; Tatalovich, Z.; Lewis, D.R.; Feuer, E.J. Using Gini coefficient to determining optimal cluster reporting sizes for spatial scan statistics. Int. J. Health Geogr. 2016, 15, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moura, M.; de Oliveira, J.; Pedreira, R.; Tavares, A.; de Souza, T.; de Lima, K.; Barbosa, I. Spatio-temporal dynamics of Aedes aegypti and Aedes albopictus oviposition in an urban area of northeastern Brazil. Trop. Med. Int. Health TM IH 2020, 25, 1510–1521. [Google Scholar]
- Santos, J.A.; Santos, D.T.; Arcencio, R.A.; Nunes, C. Space–time clustering and temporal trends of hospitalizations due to pulmonary tuberculosis: Potential strategy for assessing health care policies. Eur. J. Public Health 2021, 31, 57–62. [Google Scholar] [CrossRef]
- Kleinman, K. rsatscan: Tools, Classes, and Methods for Interfacing with SaTScan Stand-Alone Software. 2015. Available online: https://rdrr.io/cran/rsatscan/ (accessed on 29 August 2022).
- Lin, S.; Zhang, Y.; Wu, J.; Pei, L. Trends of Adverse Pregnancy Outcomes in a High Prevalence Region of Birth Defects—Shanxi Province, China, 2007–2019. 2021, 3, 661–664. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, X.; Li, B.; Xia, L.; Zhang, S.; Ding, W.; Gao, L.; Liu, A.; Xu, F.; Zhang, R.; et al. Changes in the live birth profile in Henan, China: A hospital registry-based study. Birth 2022, 49, 497–505. [Google Scholar] [CrossRef]
- Zeitlin, J.; Szamotulska, K.; Drewniak, N.; Mohangoo, A.; Chalmers, J.; Sakkeus, L.; Irgens, L.; Gatt, M.; Gissler, M.; Blondel, B. Preterm birth time trends in Europe: A study of 19 countries. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 1356–1365. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.Y.; Li, Q.; Guo, Y.; Zhou, H.; Wang, X.; Wang, Q.; Shen, H.; Zhang, Y.; Yan, D.; Zhang, Y.; et al. Association of Long-term Exposure to Airborne Particulate Matter of 1 mum or Less With Preterm Birth in China. JAMA Pediatr. 2018, 172, e174872. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Zhang, X.; Lei, J.; Duan, Z.; Li, J. Spatio-temporal Pattern Characteristics of Relationship Between Urbanization and Economic Development at County Level in China. Chin. Geogr. Sci. 2019, 29, 553–567. [Google Scholar] [CrossRef] [Green Version]
- Yu, S.; Yin, S.; Zhang, R.; Wang, L.; Su, F.; Zhang, Y.; Yang, J. Spatiotemporal characterization and regional contributions of O3 and NO2: An investigation of two years of monitoring data in Henan, China. J. Environ. Sci. 2020, 90, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Liu, Y.; Liu, H.; Zheng, H.; Li, X.; Zhu, L.; Wang, Z. Associations of maternal iodine status and thyroid function with adverse pregnancy outcomes in Henan Province of China. J. Trace Elem. Med. Biol. 2018, 47, 104–110. [Google Scholar] [CrossRef]
- Liu, L.; Hong, Z.; Zhang, L. Associations of prepregnancy body mass index and gestational weight gain with pregnancy outcomes in nulliparous women delivering single live babies. Sci. Rep. 2015, 5, 12863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaskins, A.J.; Hart, J.E.; Chavarro, J.E.; Missmer, S.A.; Rich-Edwards, J.W.; Laden, F.; Mahalingaiah, S. Air pollution exposure and risk of spontaneous abortion in the Nurses’ Health Study II. Hum Reprod 2019, 34, 1809–1817. [Google Scholar] [CrossRef] [PubMed]
- Leung, T.N.; Roach, V.J.; Lau, T.K. Incidence of preterm delivery in Hong Kong Chinese. Aust. N. Z. J. Obs. Gynaecol. 1998, 38, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Oksanen, T.; Kivimäki, M.; Pentti, J.; Virtanen, M.; Klaukka, T.; Vahtera, J. Self-report as an indicator of incident disease. Ann. Epidemiol. 2010, 20, 547–554. [Google Scholar] [CrossRef]
- Zhang, Y. Cross-Sectional Study on Birth Quality of Newborn Baby in Rural China. Master’s Thesis, Peking Union Medical College, National Research Institute for Family Planning, Beijing, China, 2011. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Adverse Pregnancy Outcomes | p | |
|---|---|---|---|
| Yes (n = 160,383) | No (n = 1,154,944) | ||
| Maternal age | <0.001 * | ||
| (20, 25) | 45,306 (11.80%) | 338,611 (88.20%) | |
| (25, 30) | 83,920 (12.23%) | 602,031 (87.77%) | |
| (30, 35) | 21,650 (12.42%) | 152,673 (87.58%) | |
| (35, 40) | 7276 (13.12%) | 48,170 (86.88%) | |
| (40, 45) | 1888 (13.81%) | 11,784 (86.19%) | |
| (45, 50) | 343 (17.00%) | 1675 (83.00%) | |
| Education level completed | <0.001 * | ||
| Missing | 4989 (15.25%) | 27,734 (84.75%) | |
| College or higher | 17,770 (14.50%) | 104,798 (85.50%) | |
| Senior high school | 1520 (12.68%) | 10,471 (87.32%) | |
| Junior high school | 26,395 (12.81%) | 179,693 (87.19%) | |
| Primary school or below | 109,709 (11.65%) | 832,248 (88.35%) | |
| Maternal occupation | <0.001 | ||
| Farmer | 138,965 (11.89%) | 1,029,831 (88.11%) | |
| Other | 21,418 (14.62%) | 125,113 (85.38%) | |
| Maternal ethnicity | <0.001 | ||
| Han | 156,389 (12.15%) | 1,130,794 (87.85%) | |
| Other | 3994 (14.19%) | 24,150 (85.81%) | |
| Maternal BMI | <0.001 * | ||
| <18.5 | 15,221 (12.70%) | 104,627 (87.30%) | |
| 18.5–23.9 | 116,835 (12.01%) | 856,197 (87.99%) | |
| 24.0–27.9 | 22,540 (12.67%) | 155,357 (87.33%) | |
| ≥28.0 | 5564 (13.01%) | 37,194 (86.99%) | |
| Missing | 223 (12.44%) | 1569 (87.56%) | |
| Season of conception | <0.001 | ||
| Spring | 49,473 (12.66%) | 341,325 (87.34%) | |
| Summer | 40,332 (12.34%) | 286,477 (87.66%) | |
| Autumn | 32,561 (11.16%) | 259,263 (88.84%) | |
| Winter | 38,017 (12.43%) | 267,879 (87.57%) | |
| Maternal pre-gestational smoking | <0.001 | ||
| Missing | 616 (0.38%) | 4093 (0.35%) | |
| None | 158,573 (98.87%) | 1,142,311 (98.91%) | |
| Yes | 1184 (0.74%) | 8492 (0.74%) | |
| Maternal pre-gestational drinking | <0.001 | ||
| Missing | 616 (13.08%) | 4093 (86.92%) | |
| No | 158,573 (12.19%) | 1,142,311 (87.81%) | |
| Occasionally | 1184 (12.24%) | 8492 (87.76%) | |
| Often | 10 (17.24%) | 48 (82.76%) | |
| Paternal pre-gestational drinking | <0.001 | ||
| Missing | 1,838 (14.30%) | 11,016 (85.70%) | |
| No | 119,913 (11.93%) | 884,923 (88.07%) | |
| Occasionally | 37,929 (12.94%) | 255,161 (87.06%) | |
| Often | 703 (15.46%) | 3844 (84.54%) | |
| Paternal pre-gestational smoking | <0.001 | ||
| Missing | 1710 (14.10%) | 10,416 (85.90%) | |
| None | 123,761 (11.99%) | 908,074 (88.01%) | |
| Yes | 34,912 (12.87%) | 236,454 (87.13%) | |
| Region 1 | <0.001 | ||
| East | 49,228 (13.15%) | 325,085 (86.85%) | |
| West | 12,038 (9.46%) | 115,203 (90.54%) | |
| Middle | 23,827 (12.69%) | 163,970 (87.31%) | |
| South | 46,429 (11.36%) | 362,457 (88.65%) | |
| North | 28,861 (13.30%) | 188,229 (86.71%) | |
| Pregnancy Outcomes | Autumn | Spring | Summer | Winter | p Values | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| PreD | 7431 | 2.55 * | 12,421 | 3.18 Δ | 9626 | 2.95 | 9292 | 3.04 | <0.001 |
| LBWI | 1952 | 0.67 | 2717 | 0.70 | 2123 | 0.65 * | 2173 | 0.71 Δ | 0.015 |
| MedA | 780 | 0.27 | 1149 | 0.29 | 933 | 0.29 | 829 | 0.27 | 0.13 |
| TIL | 270 | 0.09 | 352 | 0.09 | 320 | 0.1 | 304 | 0.1 | 0.553 |
| SponD | 2828 | 0.97 * | 4024 | 1.03 | 3819 | 1.17 Δ | 3568 | 1.17 Δ | <0.001 |
| StiB | 195 | 0.07 | 269 | 0.07 | 222 | 0.07 | 231 | 0.08 | 0.568 |
| ProD | 3911 | 1.34 | 5276 | 1.35 | 4940 | 1.51 Δ | 4027 | 1.32 * | <0.001 |
| MF | 17,117 | 5.87 * | 26,268 | 6.72 Δ | 20,602 | 6.3 | 19,905 | 6.51 | <0.001 |
| APOs | 32,563 | 11.16 * | 49,474 | 12.66 Δ | 40,332 | 12.34 | 38,018 | 12.43 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chai, J.; Zhang, J.; Shi, Y.; Sun, P.; Wang, Y.; Zhou, D.; Dong, W.; Jiang, L.; Jia, P. Spatiotemporal Patterns of Adverse Pregnancy Outcomes in Rural Areas of Henan, China. Int. J. Environ. Res. Public Health 2022, 19, 15966. https://doi.org/10.3390/ijerph192315966
Chai J, Zhang J, Shi Y, Sun P, Wang Y, Zhou D, Dong W, Jiang L, Jia P. Spatiotemporal Patterns of Adverse Pregnancy Outcomes in Rural Areas of Henan, China. International Journal of Environmental Research and Public Health. 2022; 19(23):15966. https://doi.org/10.3390/ijerph192315966
Chicago/Turabian StyleChai, Jian, Junxi Zhang, Yuanyuan Shi, Panpan Sun, Yuhong Wang, Dezhuan Zhou, Wei Dong, Lifang Jiang, and Peng Jia. 2022. "Spatiotemporal Patterns of Adverse Pregnancy Outcomes in Rural Areas of Henan, China" International Journal of Environmental Research and Public Health 19, no. 23: 15966. https://doi.org/10.3390/ijerph192315966