
The Impact of Public Health Education on Migrant Workers’ Medical Service Utilization
Abstract
:1. Introduction
1.1. Background
1.2. Literature Review
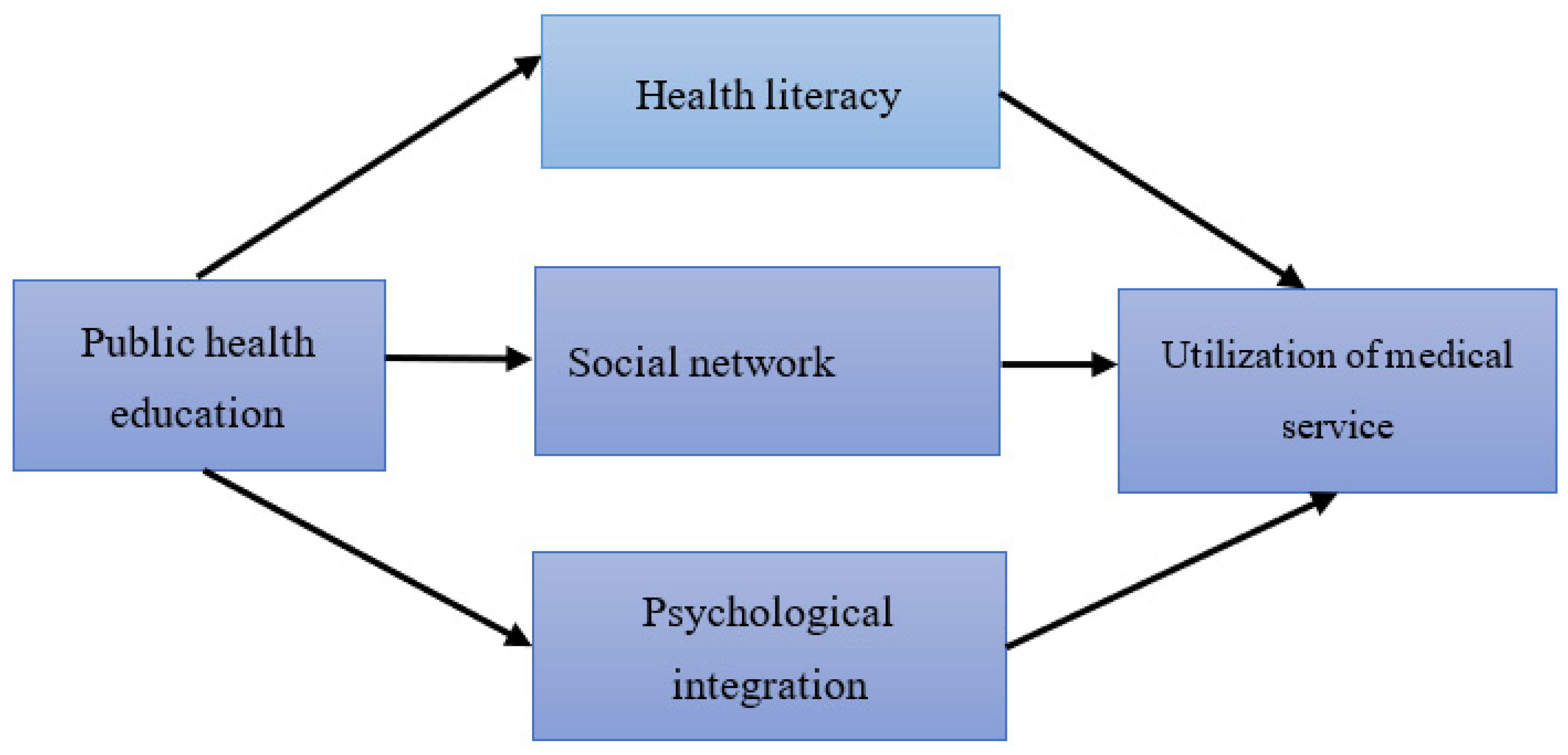
1.3. Analytical Framework
2. Methodology
2.1. Samples
2.2. Variables
2.3. Regression Method
3. Results
3.1. Baseline Regression
3.2. Robust Test
3.3. Heterogeneity Analysis
4. Discussion and Conclusions
4.1. Discussion
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leng, C.; Zhu, Z. Basic Public Health Services for Floating Population in China: Current Situation and Factor Analysis. Reform Econ. Syst. 2020, 06, 36–42. [Google Scholar]
- Sun, C. The Issues of Basic-level Health Education Public Service System and Its Perfect Path. J. Harbin Inst. Technol. 2021, 23, 9–14. [Google Scholar] [CrossRef]
- Li, W.; Liao, J.; Li, Q.; Baskota, M.; Wang, X.; Tang, Y.; Zhou, Q.; Wang, X.; Luo, X.; Ma, Y.; et al. Public health education for parents during the outbreak of COVID-19: A rapid review. Ann. Transl. Med. 2020, 8, 628. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Li, J.; Dong, T.; Cao, H.; Feng, J.; Lei, Z.; Wang, Z.; Han, X.; Lv, C.; Gan, Y. Public opinion and expectations: Development of public health education in China after COVID-19 pandemic. Front. Public Health 2021, 9, 1131. [Google Scholar] [CrossRef]
- Tannahill, A. Health promotion: The Tannahill model revisited. Public Health 2009, 123, 396–399. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, J.; Hu, X.; Wang, J.; Wang, H. Implications of health technology assessment practice in eight countries for Healthy China Initiative. Chin. J. Public Health 2021, 37, 1713–1717. [Google Scholar]
- Tian, Y.; Luo, T.; Chen, Y. The Promotional Effect of Health Education on the Medical Service Utilization of Migrants: Evidence from China. Front. Public Health 2021, 9, 818930. [Google Scholar] [CrossRef]
- Shu, Z.; Liu, Y.; Li, M.; Li, J. The effects of health system reform on medical services utilization and expenditures in China in 2004–2015. Int. Health 2021, 13, 640–647. [Google Scholar] [CrossRef]
- Wang, Y.; Porter, P.; Jin, S. Estimating effects of health insurance coverage on medical service utilization and health in rural China. Boston Mass. 2016. [Google Scholar] [CrossRef]
- Hamada, S.; Takahashi, H.; Sakata, N.; Jeon, B.; Mori, T.; Iijima, K.; Yoshie, S.; Ishizaki, T.; Tamiya, N. Household Income Relationship with Health Services Utilization and Healthcare Expenditures in People Aged 75 Years or Older in Japan: A Population-Based Study Using Medical and Long-term Care Insurance Claims Data. J. Epidemiol. 2019, 29, 377–383. [Google Scholar] [CrossRef] [Green Version]
- Du, B.; Zhou, Q.; Tan, Y.; Sang, X.; Huang, Y. Floating population: Healthy quality of life, influencing factors and paths. Chin. J. Health Policy 2019, 12, 47–53. [Google Scholar]
- Shao, S.; Zhang, H.; Chen, X.; Xu, X.; Zhao, Y.; Wang, M.; Du, J. Health education services utilization and its determinants among migrants: A cross-sectional study in urban-rural fringe areas of Beijing, China. BMC Fam. Pract. 2021, 22, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Li, N. Differential analysis of factors influencing health education among urban and rural migrant populations. Mod. Prev. Med. 2021, 48, 3769–3773+3778. [Google Scholar]
- Luque-Fernandez, M.A.; Tobias, A. The Management of the COVID-19 Pandemic Evidences the Need to Transform Spain’s Public Health Education. Int. J. Public Health 2022, 67, 1604907. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wang, X. Does accepting public health education improve the health status of floating population:An empirical analysis based on the data of the China Migrants Dynamic Survey in 2018. J. Hunan Agric. Univ. 2020, 21, 61–67+94. [Google Scholar] [CrossRef]
- Greenberg, M.T.; Domitrovich, C.E.; Weissberg, R.P.; Durlak, J.A. Social and emotional learning as a public health approach to education. Future Child. 2017, 27, 13–32. [Google Scholar] [CrossRef]
- Lv, Z.; Qiao, L. Analysis of healthcare big data. Future Gener. Comput. Syst. 2020, 109, 103–110. [Google Scholar] [CrossRef]
- Wong, S.Y.S.; Zhang, D.; Sit, R.W.S.; Yip, B.H.K.; Chung, R.Y.N.; Wong, C.K.M.; Chan, D.C.C.; Sun, W.; Kwok, K.O.; Mercer, S.W. Impact of COVID-19 on loneliness, mental health, and health service utilisation: A prospective cohort study of older adults with multimorbidity in primary care. Br. J. Gen. Pract. 2020, 70, e817–e824. [Google Scholar] [CrossRef]
- Lv, G.; Liu, W. Mobile Payment, Medical Infrastructure and Rural Residents’ Medical Services Utilization. Soc. Sci. Bei Jing 2022, 04, 95–105. [Google Scholar] [CrossRef]
- Chen, J.; Yu, H.; Dong, H. Effect of the new rural cooperative medical system on farmers’ medical service needs and utilization in Ningbo, China. BMC Health Serv. Res. 2016, 16, 593. [Google Scholar] [CrossRef] [Green Version]
- Brownlee, S.; Chalkidou, K.; Doust, J.; Elshaug, A.G.; Glasziou, P.; Heath, I.; Nagpal, S.; Saini, V.; Srivastava, D.; Chalmers, K.; et al. Evidence for overuse of medical services around the world. Lancet 2017, 390, 156–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gui, Y. Supply and utilization of health service among migrant population in China: A comparative study. Chin. J. Public Health 2021, 37, 219–223. [Google Scholar]
- Falkenberg, M.B.; Mendes TP, L.; Moraes, E.P.; De Souza, E.M. Educação em saúde e educação na saúde: Conceitos e implicações para a saúde coletiva. Ciênc. Saúde Coletiva 2014, 19, 847–852. [Google Scholar] [CrossRef] [Green Version]
- Sang, H.; González-Vallejo, C.; Zhao, J.; Long, R. Is low cost really conducive to primary care utilisation: An empirical analysis of community health centers in China. Health Soc. Care Community 2021, 29, e163–e173. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Yang, H.; Wang, H.; Liu, X. Effect of health education on healthcare-seeking behavior of migrant workers in China. Int. J. Environ. Res. Public Health 2020, 17, 2344. [Google Scholar] [CrossRef]
- Tataw, D.B.; James, F.; Bazargan, S. The Preventive Health Education and Medical Home Project: A predictive and contextual model for low-income families. Soc. Work Public Health 2009, 24, 491–510. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Health Literacy. Health Literacy: A Prescription to End Confusion; National Academies Press: Washington, DC, USA, 2004; p. 4. [Google Scholar]
- Vamos, S.; Okan, O.; Sentell, T.; Rootman, I. Making a case for “Education for health literacy”: An international perspective. Int. J. Environ. Res. Public Health 2020, 17, 1436. [Google Scholar] [CrossRef] [Green Version]
- Benjamin, R.M. Improving health by improving health literacy. Public Health Rep. 2010, 125, 784–785. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.; He, A.; Zheng, S.; Jiang, J.; Liang, J.; Shrestha, B.; Wang, P. How does health literacy affect the utilization of basic public health services in Chinese migrants? Health Promot. Int. 2022, 37, daab040. [Google Scholar] [CrossRef]
- Ford, K.; Chamratrithirong, A.; Apipornchaisakul, K.; Panichapak, P.; Pinyosinwat, T. Social integration, AIDS knowledge and factors related to HIV prevention among migrant workers in Thailand. AIDS Behav. 2014, 18, 390–397. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, J.; Zhang, Z. Interactive mechanism of the floating population’s health equity and social integration. Chin. J. Health Policy 2016, 9, 66–74. [Google Scholar]
- Berkman, L.F. The role of social relations in health promotion. Psychosom. Med. 1995, 57, 245–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, J.; Shi, Y.; Osman, M.; Shrestha, B.; Wang, P. The association between social integration and utilization of essential public health services among internal migrants in China: A multilevel logistic analysis. Int. J. Environ. Res. Public Health 2020, 17, 6524. [Google Scholar] [CrossRef] [PubMed]
- Liang, T. Residence Certificate System, Life Course and Psychological Integration of New Generation Migrant Population. J. Public Manag. 2020, 17, 96–109+172,173. [Google Scholar] [CrossRef]
- Hu, W. Research Review on the Psychology Integration of Floating Population. Qinghai Soc. Sci. 2018, 04, 130–134. [Google Scholar] [CrossRef]
- Li, T.C.; Chu, C.C.; Meng, F.C.; Li, Q.; Mo, D.; Li, B.; Tsai, S.B. Will happiness improve the psychological integration of migrant workers? Int. J. Environ. Res. Public Health 2018, 15, 900. [Google Scholar] [CrossRef]
- Zhao, J.; Zhou, D. Effects of Self-employment on the Health of Migrant Workers. J. World Econ. 2021, 44, 184–204. [Google Scholar]
- Hainmueller, J. Entropy balancing for causal effects: A multivariate reweighting method to produce balanced samples in observational studies. Political Anal. 2012, 20, 25–46. [Google Scholar] [CrossRef] [Green Version]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173. [Google Scholar] [CrossRef]
- Xiao, M.; Wang, S.; Peng, H. Migration Stresses, Social Capital and Mental Health of Migrant Population: A Study Based on the Stress Process Theory. Contemp. Financ. Econ. 2019, 3, 14–24. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Variable Definition | Mean | SD |
|---|---|---|---|
| Explained Variable | |||
| Utilization of medical service | For whether go to clinic, community hospital and general hospital when ill. Yes = 1, No = 0 | 0.5136 | 0.4998 |
| Explanatory Variable | |||
| Public health education | Respondents receiving public health education. Min = 0, Max. = 9. | 3.7055 | 3.3740 |
| Intermediary variable | |||
| Health literacy | For whether know about national health projects. Yes = 1, No = 0 | 0.5852 | 0.4927 |
| Social network | |||
| - Political participation | For whether report/advise to governments. Yes = 1, No = 0 | 0.3929 | 0.4884 |
| - Activity participation | For whether join in local activities. Yes = 1, No = 0 | 0.4240 | 0.4942 |
| Psychological integration | |||
| - Admit to be native | Yes = 1, No = 0 | 0.7436 | 0.4366 |
| - Recognized by local | Yes = 1, No = 0 | 0.8178 | 0.3860 |
| Control variables | |||
| Age | Continuous variable | 36.2940 | 10.7684 |
| Gender | Male = 1, Female = 0 | 0.5199 | 0.4996 |
| Marital status | Married = 1, Unmarried = 0 | 0.9728 | 0.1626 |
| Education level | Uneducated = 1, Primary = 2, Middle school = 3, High school = 3, Vocational school = 4, University = 5, Postgraduate = 6 | 3.2297 | 1.0363 |
| Health status | Healthy = 1, Basically healthy = 2, Unhealthy = 3, Disable = 4 | 1.2069 | 0.4722 |
| Number of family member | Continuous variable | 3.2004 | 1.2133 |
| Contracted land | Have = 1, Not have = 0 | 0.5777 | 0.4939 |
| Monthly income | Continuous variable | 8.6354 | 0.5918 |
| Employment type | Self—employed = 1, Not self—employed = 0 | 0.4247 | 0.4943 |
| Working time | Continuous variable (per week) | 0.9408 | 0.2361 |
| Medical insurance | Covered = 1, Not covered = 0 | 0.1597 | 0.3663 |
| Medical access | 1–4 Ordered variable | 1.1892 | 0.4534 |
| Monthly income | Continuous variable | 2.0184 | 1.9614 |
| Employment type | Interprovincial = 1, Not = 0 | 0.5106 | 0.4999 |
| Variables | Probit Model | IVProbit Model |
|---|---|---|
| Public health education | 0.0204 *** | 0.0237 *** |
| (0.00203) | (0.00751) | |
| Age | −0.00418 *** | −0.00418 *** |
| (0.000784) | (0.000788) | |
| Gender | −0.00918 | −0.00809 |
| (0.0132) | (0.0134) | |
| Marital status | 0.0868 ** | 0.0918 ** |
| (0.0415) | (0.0423) | |
| Education level | −0.0249 *** | −0.0265 *** |
| (0.00771) | (0.00797) | |
| Health status | 0.171 *** | 0.173 *** |
| (0.0136) | (0.0140) | |
| Number of family member | 0.0246 *** | 0.0240 *** |
| (0.00692) | (0.00696) | |
| Contracted land | −0.0155 | −0.0148 |
| (0.0138) | (0.0139) | |
| Monthly income (logarithm) | 0.00528 | 0.00439 |
| (0.0131) | (0.0131) | |
| Employment type | 0.00776 | 0.00751 |
| (0.0148) | (0.0149) | |
| Working time | −0.00215 *** | −0.00212 *** |
| (0.000375) | (0.000377) | |
| Medical insurance | 0.0517 *** | 0.0534 *** |
| (0.0184) | (0.0188) | |
| Medical access | −0.0411 *** | −0.0368 ** |
| (0.0155) | (0.0157) | |
| Migrancy times | −0.00183 | −0.00213 |
| (0.00329) | (0.00326) | |
| Interprovincial | 0.0429 *** | 0.0428 *** |
| (0.0155) | (0.0155) | |
| Provincial effect | Y | Y |
| Constant | −0.275 ** | −0.283 ** |
| (0.136) | (0.138) | |
| Observations | 39,841 | 39,310 |
| Variables | Replacement of Explained Variable | Replacement of Explanatory Variable | Entropy Balance Matching Method | |
|---|---|---|---|---|
| Cold Clinic | Physical Assessment | Medical Service Utilization | Medical Service Utilization | |
| Public health education | 0.0221 *** | 0.148 *** | 0.0896 *** | |
| (0.00638) | (0.0225) | (0.0129) | ||
| Public health file | 0.332 *** | 0.0349 | ||
| (0.0925) | (0.0640) | |||
| Control variable | ||||
| Constant | −0.428 *** | −1.507 *** | −0.287 * | −0.225 * |
| (0.130) | (0.452) | (0.150) | (0.132) | |
| Observations | 46,503 | 4023 | 33,705 | 42,976 |
| A (Grouped with Age) | B (Grouped with Education) | C (Grouped with City) | |||||
|---|---|---|---|---|---|---|---|
| Variables | Old Generation | New Generation | Primary Education | Middle Education | Higher Education | First-Tier | Second-Tier |
| Public health education | 0.0192 *** | 0.0217 *** | 0.0153 *** | 0.0215 *** | 0.0206 *** | 0.0239 *** | 0.0105 ** |
| (0.00274) | (0.00305) | (0.00505) | (0.00243) | (0.00616) | (0.00351) | (0.00458) | |
| Control variable | Ctrl | Ctrl | Ctrl | Ctrl | Ctrl | Ctrl | Ctrl |
| Constant | −0.115 | −0.520 ** | −0.886 *** | −0.0989 | 0.156 | −0.609 *** | 0.434 |
| (0.188) | (0.213) | (0.323) | (0.173) | (0.469) | (0.231) | (0.315) | |
| Observations | 21,584 | 18,257 | 6911 | 27,761 | 4131 | 14,214 | 8427 |
| (1) | (2) | (3) | (4) | (5) | |
|---|---|---|---|---|---|
| Disease education | 0.180 *** | ||||
| (0.0617) | |||||
| reproductive education | 0.223 *** | ||||
| (0.0763) | |||||
| Smoking control | 0.202 *** | ||||
| (0.0640) | |||||
| Mental education | 0.213 *** | ||||
| (0.0676) | |||||
| Emergency education | 0.221 *** | ||||
| (0.0700) | |||||
| Control variables | Ctrl | Ctrl | Ctrl | Ctrl | Ctrl |
| Constant | −0.294 ** | −0.323 ** | −0.314 ** | −0.287 ** | −0.273 ** |
| (0.131) | (0.133) | (0.140) | (0.139) | (0.138) | |
| Observations | 42,400 | 42,400 | 39,310 | 39,310 | 39,310 |
| (1) | (2) | (3) | (4) | |
|---|---|---|---|---|
| Occupational disease education | 0.229 *** | |||
| (0.0726) | ||||
| STD/AIDS prevention education | 0.191 *** | |||
| (0.0629) | ||||
| Tuberculosis education | 0.209 *** | |||
| (0.0661) | ||||
| Chronic disease education | 0.195 *** | |||
| (0.0616) | ||||
| Control variables | Ctrl | Ctrl | Ctrl | Ctrl |
| Constants | −0.257 * | −0.272 ** | −0.255 * | −0.264 * |
| (0.137) | (0.138) | (0.137) | (0.137) | |
| Observations | 39,310 | 39,310 | 39,310 | 39,310 |
| Health Literacy | Social Network | Psychological Integration | |||
|---|---|---|---|---|---|
| Variables | National Health Project | Political Participation | Social Participation | National Health Project | Political Participation |
| Public health education | 0.227 *** | 0.0789 *** | 0.0875 *** | 0.0573 *** | 0.0322 *** |
| (0.00519) | (0.00483) | (0.00481) | (0.00504) | (0.00533) | |
| Control variables | Ctrl. | Ctrl. | Ctrl. | Ctrl. | Ctrl |
| Constants | −1.129 *** | −2.553 *** | −2.600 *** | −0.255 ** | 0.368 *** |
| (0.103) | (0.0989) | (0.0996) | (0.107) | (0.111) | |
| Obsercations | 79,654 | 79,654 | 79,654 | 79,654 | 79,654 |
| (1) | (2) | (3) | |||
|---|---|---|---|---|---|
| Variables | Health Literacy | Social Network | Psychological Integration | ||
| National health project | 0.122 *** | ||||
| (0.0129) | |||||
| Political participation | 0.102 *** | ||||
| (0.0128) | |||||
| Social participation | 0.114 *** | ||||
| (0.0129) | |||||
| Admit oneself to be local | 0.0773 *** | ||||
| (0.0141) | |||||
| Be accepted by the local | 0.00208 | ||||
| (0.0155) | |||||
| Control variables | Ctrl. | Ctrl. | Ctrl. | Ctrl. | Control variables |
| Constants | −0.276 ** | −0.212 | −0.207 | −0.268 ** | −0.241 * |
| (0.129) | (0.130) | (0.129) | (0.129) | (0.130) | |
| Observations | 42,976 | 42,976 | 42,976 | 42,976 | 42,976 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, D.; Cheng, L.; Wu, H. The Impact of Public Health Education on Migrant Workers’ Medical Service Utilization. Int. J. Environ. Res. Public Health 2022, 19, 15879. https://doi.org/10.3390/ijerph192315879
Zhou D, Cheng L, Wu H. The Impact of Public Health Education on Migrant Workers’ Medical Service Utilization. International Journal of Environmental Research and Public Health. 2022; 19(23):15879. https://doi.org/10.3390/ijerph192315879
Chicago/Turabian StyleZhou, Deshui, Lanyan Cheng, and Hainan Wu. 2022. "The Impact of Public Health Education on Migrant Workers’ Medical Service Utilization" International Journal of Environmental Research and Public Health 19, no. 23: 15879. https://doi.org/10.3390/ijerph192315879