1. Introduction
According to the Intergovernmental Panel on Climate Change (IPCC) report, around 30% of the global population is exposed to extreme heat for at least 20 days each year [
1]. Between 2000 and 2019, an average of six heat-related deaths per 100,000 residents each year was reported in North America [
2]. According the World Health Organization, from 1998 to 2017, more than 166,000 people died due to heat waves, and between 2000 and 2016, the number of people exposed to heat waves increased by around 125 million [
3]. More recently, 2021 experienced a record-breaking heat wave across North America [
4], and according to the U.S. National Oceanic and Atmospheric Administration, August 2022 was the hottest August recorded in North America and Europe, and the second warmest August globally [
5]. In the United States, the increase in extreme temperatures is expected to lead to a rise in heated-related deaths and illness, particularly for vulnerable populations and communities such as the elderly [
6]. Most people stay indoors during heat events, thus, developments to the built environment should consider instigating housing design practices that minimize the likelihood of overheating during hot weather events. Indoor heat exposure can lead to a cascade of illnesses including heat exhaustion, heatstroke, and hyperthermia. In addition, extreme temperatures can worsen chronic conditions such as cardiovascular and respiratory diseases. Meanwhile, climate change is increasing the potential of devastating and unpredictable extreme heat events. The Climate Action Tracker states that the world is headed for 2.4 °C of warming, despite the COP26 climate pledges [
7]. Under such conditions, it is imperative to prioritize the prevention of overheating in buildings. The first step is to understand what housing characteristics may have the biggest impact on heat-related illness (HRI).
According to the World Health Organization, heat waves rarely receive adequate attention because their death tolls and destruction are not always immediately obvious [
3]. There are also different definitions for a heat wave. The U.S. Environmental Protection Agency defines a heat wave as a period of two or more consecutive days when the daily minimum apparent temperature (the actual temperature, adjusted for humidity) in a particular city exceeds the 85th percentile of historical July and August temperatures (1981–2010) for that city (refer to the EPA’s website for the reason for this definition) [
8]. Extensive literature has focused on heat exposure in outdoor environments and its associated human health impacts, and the health impacts from extreme heat have used ambient meteorological measures [
9]. However, the available data on indoor heat exposure and its effect on human health is relatively limited compared to that of outdoor heat exposure, and most studies are on a small scale (e.g., individual buildings, a group of homes) [
10,
11]. For example, Williams and colleagues conducted a study on low-income senior residents (n = 51) in public housing in Cambridge, Massachusetts. They found that with higher indoor temperatures, sleep was more disrupted, and heart rates increased [
9]. In Detroit, Michigan, the thermal conditions of 30 different homes were monitored and analyzed, along with the housing characteristics (e.g., exterior wall materials). The findings showed that indoor exposure to heat in Detroit exceeded the comfort range among elderly occupants [
12]. In the United States, there have been only a few studies on a larger scale of a single city (e.g., Detroit) [
13], a single state (i.e., California) [
14], or multi-county [
15]. To the authors’ knowledge, there is no multistate study that has focused on the connection between heat-related illness and housing characteristics.
Indoor heat exposure potential is determined by the outdoor ambient temperature and housing characteristics (e.g., housing thermal inertia)..The majority of epidemiological studies of heat-related health effects use outdoor weather conditions as the primary indicator to estimate indoor heat exposure and/or heat stress [
16,
17,
18]. Currently, most heat-health warning systems are also based on outdoor temperatures. This reliance on outdoor conditions can mislead the interpretation of health effects and associated solutions, since most people who stay indoors are assumed to be isolated from outdoor thermal conditions [
19]. Currently, heat exposure in epidemiological studies is often estimated using an airport monitoring station and applied to residents of an entire community [
12]. As for indoor heat exposure, a WHO working group on indoor environments found that “There is no demonstrable risk to human health of healthy sedentary people living in air temperature of between 18 and 24 °C” [
20]. However, an adaptive thermal comfort model showed that thermal comfort also depends on other individual variables such as metabolism, level of activity, and clothing, among others. Therefore, a variety of indoor heat exposure ranges were found in previous literature. For example, 27 °C was used as the cut-off temperature in a survey of 57 elderly adults in the United States to study thermal conditions, reduced emotional distress, and increased hours of sleep [
21]. Conversely, a study on 113 elderly people in the Netherlands used 20.8 to 29.3 °C as the temperature range, which led to similar conclusions that an increased temperature can raise the risk of sleep disturbance [
22]. In the United States, there is no consensus on a cut-off maximum temperature for heat-related health risks; for instance, Boston uses 25 °C as an indoor maximum acceptable temperature, while New York City uses 27–28 °C [
23]. Consequently, indoor heat exposure in this study should be understood as a range of higher temperatures over an extended period of two or more consecutive days.
Moreover, the Heat Vulnerability & Preparedness index provided by the US Centers for Disease Control and Prevention (CDC) considers 14 indicators including population demographic information and outdoor conditions, such as the percentage of forest canopy cover. However, there are no housing (building) indicators included. While outdoor weather conditions can be monitored or measured through multiple methods, such as ground monitoring, numerical models, and remote sensing data, indoor thermal conditions are not routinely monitored or reported due to privacy concerns and the time-consuming, labor-intensive traditional monitoring methods. Consequently, direct indoor heat exposure and heat stress are less studied than outdoor heat. While it is commonly perceived that buildings with little insulation, thermal mass, or shading are prone to overheating when air-conditioning is unavailable, supporting empirical studies are limited. Many practical models have been generated to predict indoor temperatures using outdoor temperatures, housing characteristics, and other variables. Some recent models, based on deep-learning computer algorithms, have reached a high accuracy of up to 98.4% [
24]. However, there is a lack of direct methods for and evidence of connecting housing characteristics and indoor heat exposure with heat-related illness, which imposes difficulties in utilizing resilient building designs (e.g., passive design) to adapt to changing climate conditions [
25]. To this extent, this study addresses these gaps by examining the association between housing characteristics and HRI.
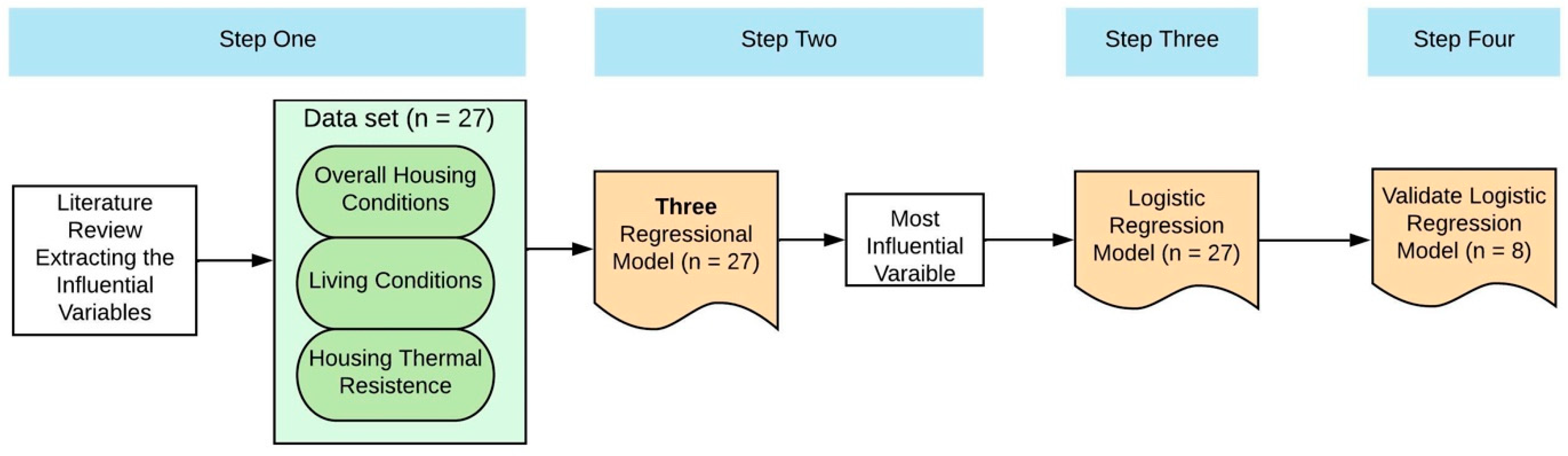
The purpose of this study is to examine the correlation between housing characteristics and HRI at a national scale using data extracted from the American Housing Survey, the American Community Survey, the ResStock database, and the CDC’s National Environmental Public Health Tracking Network on a state level in the United States. More specifically, there are three questions addressed: (1) whether HRI can be predicted based on housing characteristic variables, (2) how influential these variables are, and (3) whether the variables influencing different HRI measure differently. Additionally, we hypothesized that states with higher housing thermal inertia quality have a better mitigation effect on HRI.
5. Conclusions
5.1. Study Contribution
Using a data set of 27 states, this study identified the correlation of housing characteristic variables in three categories, including general housing conditions, living conditions, and housing thermal inertia, with heat-related mortality (MORD), heat-related mortality rate (MOR), and heat-related emergency department visits (EDV). Out of the five identified influential variables (housing age (HA), housing energy efficiency (HEE), housing crowding ratio (HCR), roof condition (RC), and prevalence of air-conditioning (AC), RC has a statistical significance correlated with EDV; HA and HCR have a statistically significant correlation with MORD. The findings are discussed in three housing characteristic categories in the following sections.
The first two categories are closely related, with findings of the correlation between HA and HCR in line with previous studies. Moreover, the combination of these two variables can be used as predictors for the risk of MORD; these findings can help state agencies identify vulnerable communities and populations affected by extreme heat events. The regression model results of this study indicate that HA is negatively related to a higher risk of MORD. This differs from previous research and the common perception that older housing is linked to less thermal comfort. Findings from this study indicate that younger and newer housing may have less thermal inertia than older housing. This novel finding can be validated with additional data.
Although the individual correlations of HEE and AC were not found to be statistically significant to HRI, when combined with HA and HCR they were influential to MORD and EDV. This empirical evidence further supports the concept of the built environment determined health and climate change-exacerbated health outcomes.
The third category, housing thermal inertia (including RC), was not closely examined in previous research. This study contributes new findings on the role of housing thermal inertia in mitigating heat-related illness. The strong correlation between RC and EDV (from the regression model analysis) shows promise in mitigating heat stress by making roofs more thermally resistant. Relatively low-cost and low-tech solutions include adding additional insulation in the attic space or underside of the roof ceiling, or painting flat roofs in light colors and high reflective coating materials, which are readily available for most communities.
Other findings that do not align with previous research include the lack of correlation between the percentage of low-income housing (PH) and heat-related illness. This finding could help to dispel the perception that housing quality and thermal inertia equate to expensive construction. In addition, unlike RC, the exterior wall condition (EWC) did not correlate with any of the HRI indexes. There are two hypotheses: first, using an exterior condition as a proxy for thermal inertia is not reliable, and second, more indoor heat exposure is mitigated through the roof rather than the walls. Further data collection and analyses are needed to validate these hypotheses.
Overall, the results from this study provide useful insight, helping building owners and policy makers to make decisions or develop state-wide policies to support building upgrades or retrofits that adapt to extreme heat conditions. To the authors’ knowledge, this study is the first multistate study focusing on the connection between heat-related illness and housing characteristics. As climate change related, extreme heat events are projected to worsen for at least the next three decades [
46], the findings from this study provide useful information to help health systems become more heat- resilient by integrating housing physical conditions as a mitigator. The results also reinforce the benefits of using data analytics to understand the correlation between housing characteristics and HRI. Findings of some less impactful variables are unexpected, but they are useful for providing direction for future studies.
5.2. Study Limitations
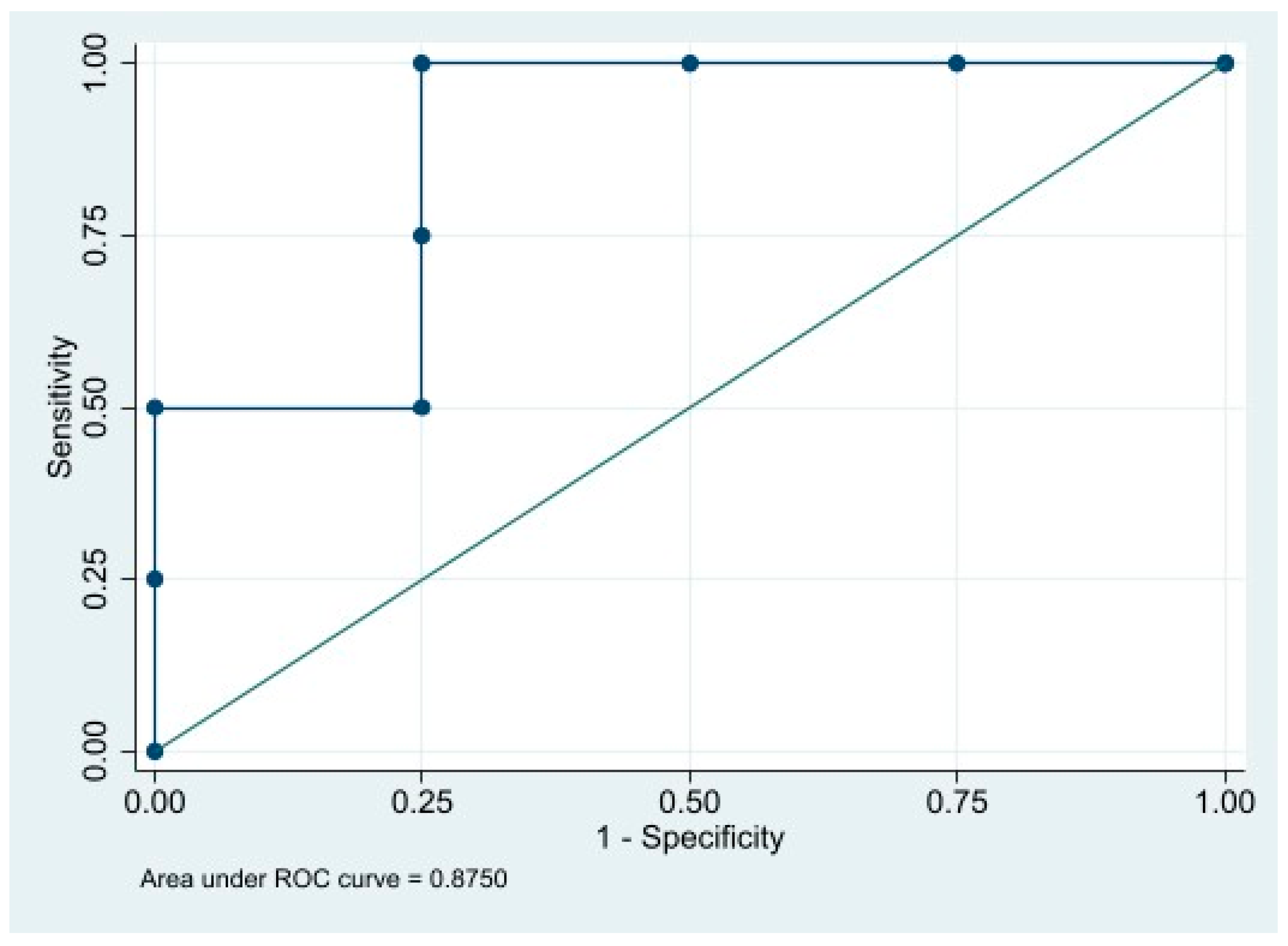
This study had four main limitations. First, our analysis data were limited to the state level. Data sets of 27 states were used for multivariable regression analysis and for building a logistic regression model. The limited data and samples may create selection bias and consequently affect the reliability of the analysis results. Therefore, the next step should be to expand the data set to include more states. Second, the selection of housing characteristic variables in this study may have influenced the findings. There are other housing variables besides the three categories in this study that impact HRI. To rule out other influencers, additional housing variables should be examined, especially variables contributing to the thermal inertia of housing, such as window (glass) areas that have direct exposure to sun and heat. A more in-depth literature review would help to extract additional variables to be included in this study. Third, data availability largely constrained the robustness of the analysis results. Since the data were collected and extracted from different sources, certain information did not match exactly. For example, EDV data from CDC was from 2015 to 2019, whereas EDV data extracted from HCUP was from 2016 to 2020. In addition, HRI data were not available for all states. It may be difficult to retrieve data for certain states with cold climates that have not tracked health data related to heat events, creating potential barriers for future research. Moreover, in the CDC database, there are no separate categories that differentiate outdoor heat-related data from indoor-heat-related data. The assumption used in this study is that during extreme heat conditions, most of the population is sheltered indoors. More granular and reliable data is needed for the specific purpose of studying indoor heat-related illness. To the authors’ knowledge, there is no such data set yet, which would be the next research step. Lastly, in this study, human factors were not included (e.g., activity level, underlying health conditions); in future studies, these variables can be used as control variables and be integrated into a regression model.






{kind=link}
{kind=link}