
Work and Family Pathways and Their Associations with Health for Young Women in Korea

Abstract
:1. Introduction
2. Background
2.1. Life Transitions and Pathways
2.2. Employment, Family, and Health of Young Women
2.3. Joint Effects of Work and Family Transitions on Women’s Health
2.4. The Case of Korea
3. Materials and Methods
3.1. Data
3.2. Measures
3.2.1. Work and Family Pathways
3.2.2. Precursor Variables
3.2.3. Health
3.2.4. Other Controls
3.3. Analytic Plan
4. Results
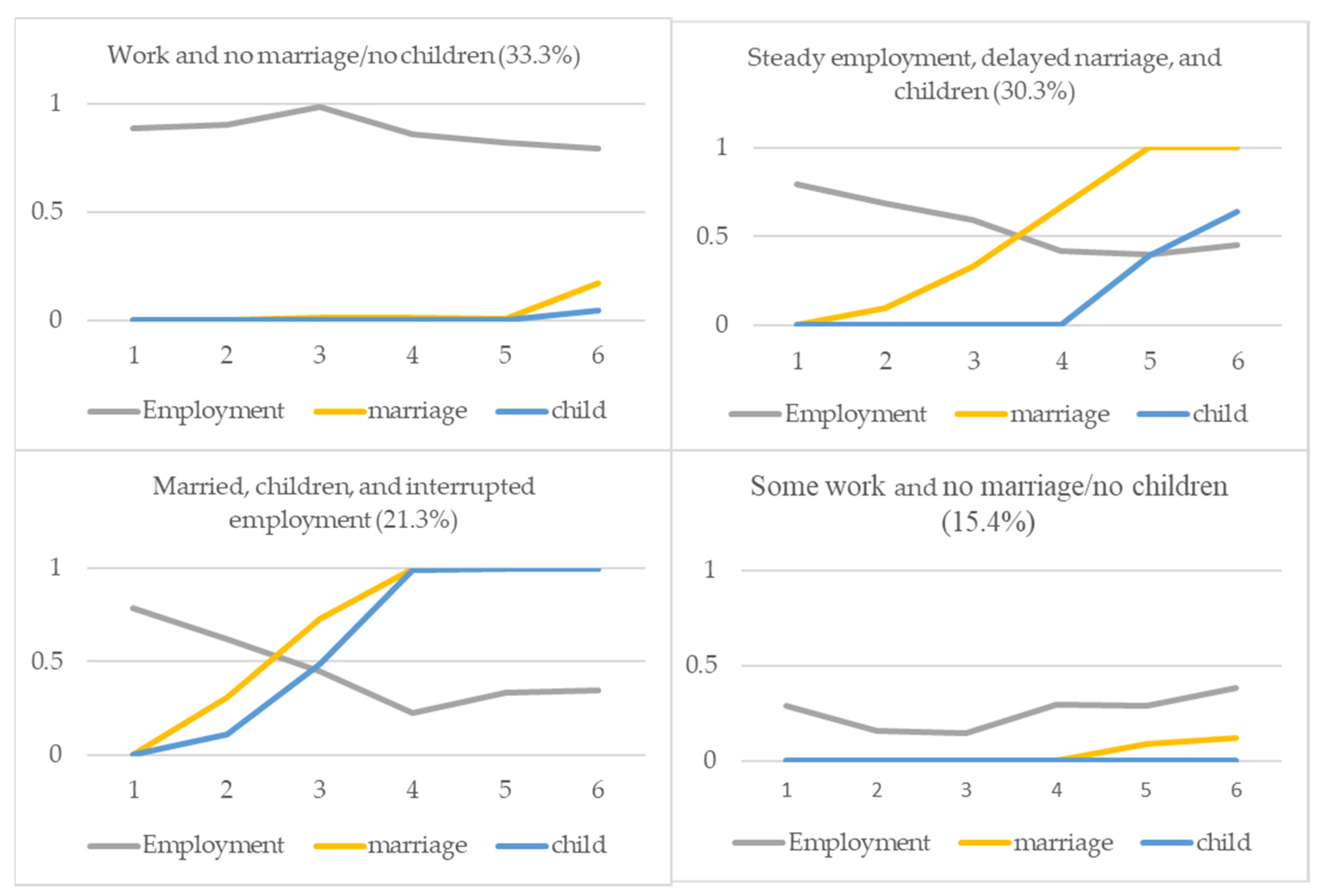
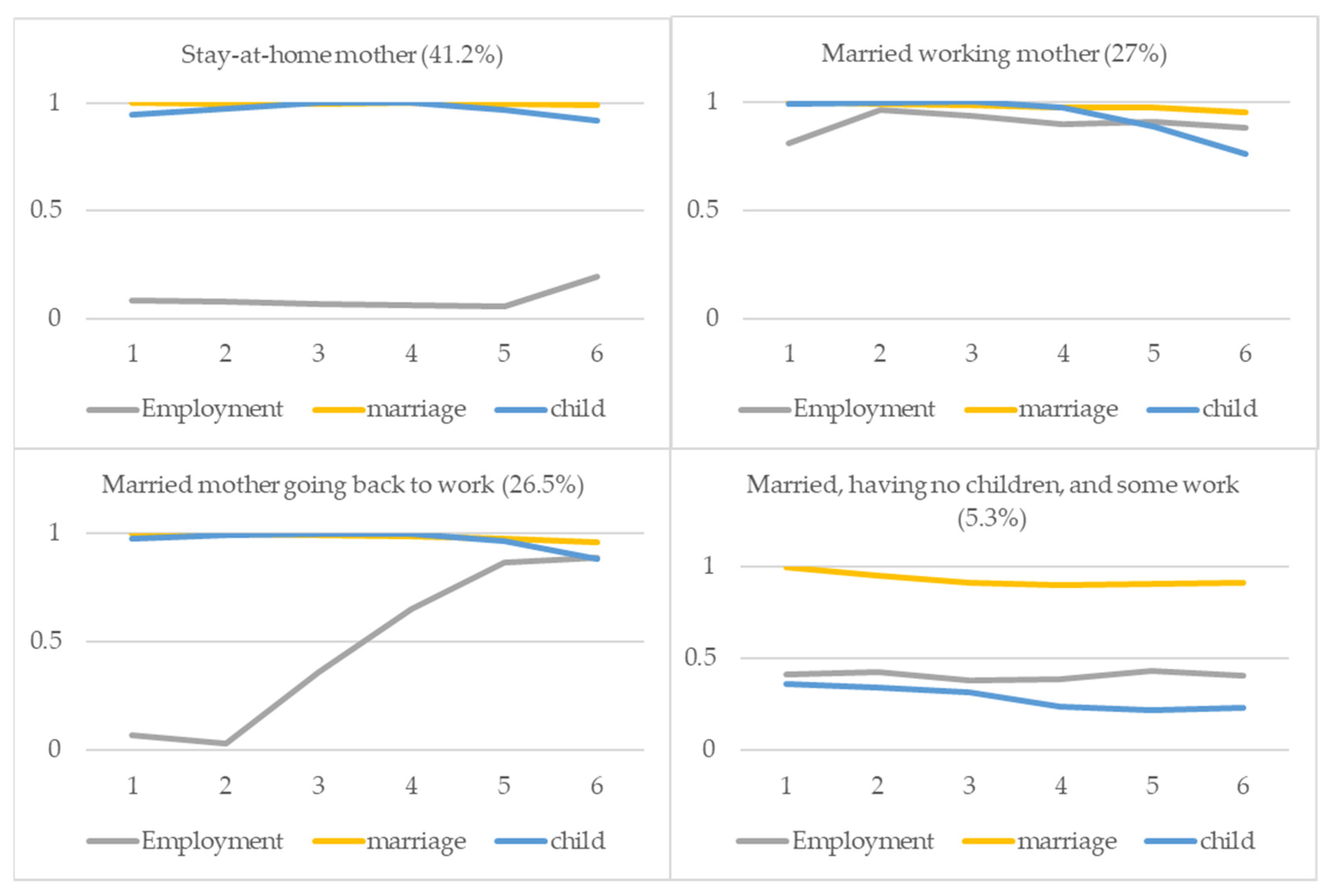
4.1. Work and Family Pathways: LCA
4.2. Precursors of Work and Family Pathways
4.3. Work and Family Pathways and Later Health
5. Discussion
Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Number of Classes | Log-Likelihood | G-Squared | AIC | BIC | Adjusted BIC | Entropy | df |
|---|---|---|---|---|---|---|---|
| 1 | −14960.93 | 11387.10 | 11459.10 | 11666.93 | 11552.55 | 1.00 | 524251 |
| 2 | −12526.51 | 6518.27 | 6666.27 | 7093.48 | 6858.37 | 0.85 | 524213 |
| 3 | −11646.20 | 4757.64 | 4981.64 | 5628.24 | 5272.39 | 0.89 | 524175 |
| 4 | −11157.84 | 3780.91 | 4080.91 | 4946.89 | 4470.31 | 0.89 | 524137 |
| 5 | −10866.71 | 3198.67 | 3574.67 | 4660.03 | 4062.71 | 0.91 | 524099 |
| 6 | −10633.07 | 2731.38 | 3183.38 | 4488.11 | 3770.06 | 0.92 | 524061 |
| 7 | −10459.51 | 2384.26 | 2912.26 | 4436.38 | 3597.6 | 0.93 | 524023 |
| 8 | −10308.12 | 2081.48 | 2685.48 | 4428.98 | 3469.46 | 0.93 | 523985 |
| Work and No Marriage/No Children | Steady Employment, Delayed Marriage and Children | Marriage and Children, and Interrupted Employment | Some Work and No Marriage/No Children | Stay-at-Home Mother | Married Working Mother | Married Mother Going Back to Work | Married, No Children, and Some Work | |
|---|---|---|---|---|---|---|---|---|
| Sample Size (n) | 101 | 95 | 66 | 48 | 862 | 569 | 530 | 105 |
| Age (W1) | ||||||||
| Mean | 29.77 | 27.34 | 27.50 | 28.67 | 33.31 | 34.81 | 33.63 | 34.04 |
| Range | 24-39 | 24-39 | 24-34 | 24-37 | 24-39 | 25-39 | 24-39 | 24-39 |
| Age (W7) | ||||||||
| Mean | 40.72 | 38.33 | 38.42 | 39.67 | 44.31 | 45.81 | 44.62 | 45.04 |
| Range | 35-50 | 35-50 | 35-45 | 35-48 | 35-50 | 36-50 | 35-50 | 35-50 |
| Education | ||||||||
| High school or below | 25.74 | 17.89 | 16.67 | 43.75 | 48.49 | 49.21 | 54.53 | 55.24 |
| Two year college | 15.84 | 24.21 | 39.39 | 18.75 | 22.74 | 18.45 | 23.96 | 15.24 |
| Four year college or above | 58.42 | 57.89 | 43.94 | 37.50 | 28.77 | 32.34 | 21.51 | 29.52 |
| Precursor Variables | ||||||||
| Structural resources | ||||||||
| Parents’ education | ||||||||
| Middle school or below | 41.58 | 46.32 | 37.88 | 47.92 | 59.51 | 68.54 | 70.00 | 59.05 |
| High school | 37.62 | 40.00 | 50.00 | 31.25 | 29.81 | 23.37 | 23.96 | 30.48 |
| College or above | 20.79 | 13.68 | 12.12 | 20.83 | 10.67 | 8.08 | 6.04 | 10.48 |
| Living Standard at age 15 | ||||||||
| Low | 20.79 | 14.74 | 15.15 | 31.25 | 27.49 | 29.17 | 27.92 | 32.38 |
| Middle | 53.47 | 62.11 | 63.64 | 52.08 | 55.22 | 54.31 | 52.83 | 47.62 |
| High | 25.74 | 23.16 | 21.21 | 16.67 | 17.29 | 16.52 | 19.25 | 20.00 |
| Living arrangement at age 15 | ||||||||
| Living with both parents | 90.10 | 91.58 | 95.45 | 83.33 | 89.68 | 90.51 | 87.74 | 90.48 |
| Others | 9.9 | 8.42 | 4.55 | 16.66 | 10.33 | 9.49 | 12.27 | 9.52 |
| Value orientations | ||||||||
| Conservative marriage norm (W1, range 1~4) | ||||||||
| Everyone must get married | 2.32 | 2.38 | 2.47 | 2.13 | 2.51 | 2.57 | 2.49 | 2.35 |
| Marriage should be with someone from a similar family background | 2.82 | 2.81 | 2.92 | 2.90 | 3.03 | 2.96 | 2.98 | 2.92 |
| It is better to get married early | 2.07 | 2.00 | 2.12 | 1.94 | 2.30 | 2.25 | 2.36 | 2.19 |
| It is good to have children early if you are married | 2.48 | 2.52 | 2.44 | 2.42 | 2.91 | 2.83 | 2.97 | 2.55 |
| Conservative gender role attitude (W1, range 1~4) | ||||||||
| Ideally, men should have a job and women should take care of the household | 2.27 | 2.16 | 2.27 | 2.25 | 2.61 | 2.37 | 2.43 | 2.39 |
| Housewives also have to go to work so that marital relations are equal | 2.49 | 2.20 | 2.15 | 2.40 | 2.50 | 2.25 | 2.44 | 2.33 |
| If housewives with preschool children work, it will have a negative impact on their children’s education | 2.52 | 2.47 | 2.26 | 2.52 | 2.72 | 2.57 | 2.75 | 2.57 |
| The house couple live in must be under the joint ownership. | 1.73 | 1.83 | 1.68 | 1.88 | 2.07 | 2.11 | 2.06 | 2.09 |
| Health and health behaviors | ||||||||
| Self-rated health (W1) | ||||||||
| Mean | 4.11 | 4.32 | 4.29 | 3.98 | 4.02 | 4.04 | 4.02 | 4.02 |
| Self-rated health (W7) | ||||||||
| Mean | 3.74 | 3.89 | 3.77 | 3.38 | 3.72 | 3.69 | 3.70 | 3.61 |
| Regular exercise per week (W7) | ||||||||
| no exercise | 63.37 | 74.74 | 74.24 | 75.00 | 65.31 | 70.12 | 74.34 | 70.48 |
| 1~2 days | 12.87 | 5.26 | 6.06 | 6.25 | 9.74 | 8.61 | 6.79 | 10.48 |
| 3~4 days | 11.88 | 10.53 | 13.64 | 10.42 | 13.46 | 12.48 | 11.89 | 12.38 |
| 5+ days | 11.88 | 9.47 | 6.06 | 8.33 | 11.48 | 8.79 | 6.98 | 6.67 |
References
- OECD. Women and Men in OECD Countries; OECD: Paris, France, 2006; Available online: https://www.oecd.org/sdd/womenandmeninoecdcountries.htm (accessed on 1 October 2022).
- OECD. Why Do More Young Women than Men Go on to Tertiary Education? In Education Indicators in Focus 79; OECD: Paris, France, 2021. [Google Scholar] [CrossRef]
- Sewell, W.H., Jr. A theory of structure: Duality, agency, and transformation. Am. J. Sociol. 1992, 98, 1–29. [Google Scholar] [CrossRef]
- Barban, N. Family trajectories and health: A life course perspective. Eur. J. Population. 2013, 29, 357–385. [Google Scholar] [CrossRef]
- Carr, D.; Springer, K.W. Advances in Families and Health Research in the 21st Century. J. Marriage Fam. 2010, 72, 743–761. [Google Scholar] [CrossRef]
- Evenson, R.J.; Simon, R.W. Clarifying the relationship between parenthood and depression. J. Health Soc. Behav. 2005, 46, 341–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, T. Parenthood and happiness: A review of folk theories versus empirical evidence. Soc. Indic. Res. 2012, 108, 29–64. [Google Scholar] [CrossRef] [Green Version]
- Nomaguchi, K.M.; Milkie, M.A. Costs and rewards of children: The effects of becoming a parent on adults’ lives. J. Marriage Fam. 2003, 65, 356–374. [Google Scholar] [CrossRef]
- O’Flaherty, M.; Baxter, J.; Haynes, M.; Turrell, G. The family life course and health: Partnership, fertility histories, and later-life physical health trajectories in Australia. Demography 2016, 53, 777–804. [Google Scholar] [CrossRef]
- Ross, C.E.; Mirowsky, J.; Goldsteen, K. The impact of the family on health: The decade in review. J. Marriage Fam. 1990, 52, 1059–1078. [Google Scholar] [CrossRef] [Green Version]
- Ennis, L.R. Intensive Mothering: The Cultural Contradictions of Modern Motherhood; Demeter Press: Toronto, ON, Canada, 2014. [Google Scholar]
- Amato, P.R.; Kane, J.B. Life-course pathways and the psychosocial adjustment of young adult women. J. Marriage Fam. 2011, 73, 279–295. [Google Scholar] [CrossRef]
- Bird, C.E.; Rieker, P.P. Gender and Health; Cambridge University Press: New York, NY, USA, 2008. [Google Scholar]
- OECD. Education at a Glance, OECD Indicator; OECD: Paris, France, 2021; Available online: https://www.oecd-ilibrary.org/docserver/b35a14e5-en.pdf?expires=1657600153&id=id&accname=guest&checksum=D4C616FE6C86F1C1AFE3A93DD8F72246 (accessed on 1 October 2022).
- OECD. Labor Force Statistics by Sex and Age; OECD: Paris, France, 2019; Available online: https://stats.oecd.org/Index.aspx?QueryId=64196 (accessed on 1 October 2022).
- Elder, G.H., Jr. The life course as developmental theory. Child Dev. 1998, 69, 1–12. [Google Scholar] [CrossRef]
- Macmillan, R.; Copher, R. Families in the life course: Interdependency of roles, role configurations, and pathways. J. Marriage Fam. 2005, 67, 858–879. [Google Scholar] [CrossRef]
- Amato, P.R.; Landale, N.S.; Havasevich, T.C.; Booth, A.; Eggebeen, D.J.; Schoen, R.; McHale, S.M.; Pennsylvania State University. Precursors of young women’s family formation pathways. J. Marriage Fam. 2008, 70, 1271–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arber, S. Comparing inequalities in women’s and men’s health: Britain in the 1990s. Soc. Sci. Med. 1997, 44, 773–787. [Google Scholar] [CrossRef] [PubMed]
- Passannante, M.R.; Nathanson, C.A. Female labor force participation and female mortality in Wisconsin 1974–1978. Soc. Sci. Med. 1985, 21, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, G.; Verbrugge, L.M. Women, work, and health. Annu. Rev. Public Health. 1987, 8, 235–251. [Google Scholar] [CrossRef] [PubMed]
- Artazcoz, L.; Borrell, C.; Benach, J.; Cortès, I.; Rohlfs, I. Women, family demands and health: The importance of employment status and socio-economic position. Soc. Sci. Med. 2004, 59, 263–274. [Google Scholar] [CrossRef]
- Waldron, I.; Jacobs, J.A. Effects of labor force participation on women’s health: New evidence from a longitudinal study. J. Occup. Med. 1988, 30, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Artazcoz, L.; Artieda, L.; Borrell, C.; Cortès, I.; Benach, J.; García, V. Combining job and family demands and being healthy: What are the differences between men and women? Eur. J. Public Health 2004, 14, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Dupre, M.E.; Meadows, S.O. Disaggregating the effects of marital trajectories on health. J. Family Issues 2007, 28, 623–652. [Google Scholar] [CrossRef]
- Grundy, E.; Holt, G. Adult life experiences and health in early old age in Great Britain. Soc. Sci. Med. 2000, 51, 1061–1074. [Google Scholar] [CrossRef]
- Musick, K.; Bumpass, L. Cohabitation, Marriage, and Trajectories in Well-Being and Relationships. In California Center for Population Research On-Line Working Paper Series; 2006; Available online: https://escholarship.org/uc/item/34f1h2nt (accessed on 1 January 2022).
- Bachman, J.G.; O’Malley, P.M.; Schulenberg, J.E.; Johnston, L.D.; Bryant, A.L.; Merline, A.C. The Decline of Substance Use in Young Adulthood: Changes in Social Activities, Roles, and Beliefs; Taylor & Francis: New York, NY, USA, 2014. [Google Scholar]
- Edin, K.; Kefalas, M. Promises I Can Keep: Why Poor Women Put Motherhood Before Marriage; University of California Press: California, CA, USA, 2011. [Google Scholar]
- Bramlett, M.D.; Mosher, W.D. Cohabitation, marriage, divorce, and remarriage in the United States. Vital Health Stat. 2002, 22, 1–93. [Google Scholar]
- Moen, P.; Dempster-McClain, D.; Williams, R.M. Successful aging: A life-course perspective on women’s multiple roles and health. Am. J. Sociol. 1992, 97, 1612–1638. [Google Scholar] [CrossRef]
- Kalleberg, A.L. Good Jobs, Bad Jobs: The Rise of Polarized and Precarious Employment Systems in the United States; Russell Sage Foundation: New York, NY, USA, 2011. [Google Scholar]
- Ben-Shlomo, Y.; Kuh, D. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.M. An integrative approach to health. Demography 2010, 47, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Oxford, M.L.; Gilchrist, L.D.; Gillmore, M.R.; Lohr, M.J. Predicting variation in the life course of adolescent mothers as they enter adulthood. J. Adolesc. Health. 2006, 39, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Halfon, N.; Hochstein, M. Life course health development: An integrated framework for developing health, policy, and research. Milbank Q. 2002, 80, 433–479. [Google Scholar] [CrossRef] [Green Version]
- Uz, I. The index of cultural tightness and looseness among 68 countries. J. Cross Cult. Psychol. 2015, 46, 319–335. [Google Scholar] [CrossRef]
- Statistics Korea. Women’s Lives Through Statistics in 2020. Available online: https://kostat.go.kr/portal/korea/kor_nw/1/6/5/index.board?bmode=download&bSeq=&aSeq=384858&ord=2 (accessed on 1 October 2022).
- Kim, J.Y.; Woo, H. A longitudinal study on marital status and depression: Variations by gender and age cohorts. Korean J. Popul. Stud. 2017, 40, 79–105. [Google Scholar]
- Lee, M.-A. Marital status and depression among Korean older adults: Gender differences. Korean J. Sociol. 2010, 44, 32–62. [Google Scholar]
- Lee, M.-S. Marital relationships and depressive symptoms among elderly population: The effects of marital status and marital satisfaction. Korean J. Sociol. 2012, 46, 176–204. [Google Scholar]
- Son, J.-Y.; Han, G.-H. The effects of marital status on health among older women: The moderating effects of age and parent-adult child relationships. Korea J. Popul. Stud. 2012, 35, 211–238. [Google Scholar]
- Cha, S.-E.; Han, K.-H. Family role status and physical/mental health of men and women: Who is more vulnerable? Korea J. Popul. Stud. 2006, 29, 167–194. [Google Scholar]
- Jeoung, J. The effects of transitions in parental status changes. J. Fam. Cult. 2016, 28, 152–183. [Google Scholar] [CrossRef]
- Moon, H.-A.; Jun, J. Scattered sleep: Analysis of postpartum mother’s sleep and its implication. J. Fam. Cult. 2017, 29, 1–26. [Google Scholar] [CrossRef]
- Vermunt, J.K. Latent class modeling with covariates: Two improved three-step approaches. Polit. Anal. 2010, 18, 450–469. [Google Scholar] [CrossRef]
- Oesterle, S.; Hawkins, J.D.; Hill, K.G.; Bailey, J.A. Men’s and women’s pathways to adulthood and their adolescent precursors. J. Marriage Fam. 2010, 72, 1436–1453. [Google Scholar] [CrossRef] [Green Version]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Struct. Equ. Model Multidiscip. J. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Masyn, K.E. Latent class analysis and Fintie mixture modeling. In The Oxford Handbook of Quantitative Methods Volume 2 Statistical Analysis; Little, T.D., Ed.; Oxford University Press: Oxford, UK, 2013; pp. 551–611. [Google Scholar]
- Collins, L.M.; Lanza, S.T. Latent Class and Latent Transition Analysis: With Applications in the Social, Behavioral, and Health Sciences; Wiley: Hoboken, NJ, USA, 2010. [Google Scholar]
- Kalleberg, A.L.; Hewison, K. Precarious work and the challenge for Asia. Am. Behav. Sci. 2013, 57, 271–288. [Google Scholar] [CrossRef]


| Work and Family Status | Wave 1 (2007) | Wave 2 (2008) | Wave 3 (2010) | Wave 4 (2012) | Wave 5 (2014) | Wave 6 (2016) |
|---|---|---|---|---|---|---|
| Unmarried women (N) | 310 | 272 | 270 | 258 | 268 | 284 |
| Married | 0 | 8.82 | 24.81 | 41.86 | 52.61 | 60.21 |
| Living with minor children | 0 | 2.26 | 10.32 | 21.29 | 33.23 | 42.26 |
| Employed | 74.52 | 66.45 | 62.26 | 50.32 | 50.65 | 53.23 |
| Married women (N) | 2066 | 1988 | 1961 | 1951 | 1960 | 1980 |
| Married | 100 | 99.4 | 98.93 | 98.46 | 97.96 | 96.72 |
| Living with minor children | 93.42 | 95.11 | 96.32 | 95.16 | 90.61 | 82.96 |
| Employed | 29.38 | 32.24 | 39.64 | 45.98 | 51.89 | 57.21 |
| Work and No Marriage/No Children | Steady Employment, Delayed Marriage and Children | Married and Children, and Interrupted Employment | Stay-at-Home Mother | Married Working Mother | Married Mother Going Back to Work | Married, No Children, and Some Work | |
|---|---|---|---|---|---|---|---|
| Education (ref. high school or below) | |||||||
| Two-year college | 0.525 | 0.831 | 1.299 * | 0.366 | 0.286 | −0.074 | −0.055 |
| (0.59) | (0.58) | (0.65) | (0.48) | (0.58) | (0.51) | (0.65) | |
| Four-year college or above | 1.011 * | 1.129 * | 0.886 | −0.417 | 0.473 | −0.942 + | 0.127 |
| (0.50) | (0.52) | (0.65) | (0.44) | (0.52) | (0.48) | (0.59) | |
| Age (W1) | 0.110 * | −0.071 | 0.020 | 0.383 *** | 0.531 *** | 0.377 *** | 0.351 *** |
| (0.05) | (0.06) | (0.08) | (0.05) | (0.07) | (0.05) | (0.06) | |
| Self-rated health (W1) | 0.016 | 0.219 | 0.199 | 0.348 + | 0.526 * | 0.257 | 0.124 |
| (0.22) | (0.22) | (0.26) | (0.20) | (0.26) | (0.21) | (0.23) | |
| Structural resources | |||||||
| Living standard at age 15 years | 0.212 | 0.603 | 0.126 | 0.120 | 0.312 | 0.594 + | −0.029 |
| (0.34) | (0.38) | (0.43) | (0.29) | (0.33) | (0.31) | (0.41) | |
| Parents’ education (ref. middle school or below) | |||||||
| High school | 0.160 | −0.309 | 0.152 | 0.266 | −0.084 | −0.205 | 0.599 |
| (0.48) | (0.48) | (0.52) | (0.42) | (0.48) | (0.45) | (0.55) | |
| College or above | −0.106 | −1.003 | −0.696 | −0.851 | −1.395 * | −2.050 *** | 0.035 |
| (0.59) | (0.64) | (0.77) | (0.54) | (0.62) | (0.61) | (0.75) | |
| Living arrangement at age 15 years | 0.199 | −0.191 | 0.693 | 0.700 | 0.970 + | 0.372 | 1.409 + |
| (0.62) | (0.67) | (0.89) | (0.49) | (0.58) | (0.53) | (0.75) | |
| Value orientations | |||||||
| Conservative marriage norm (W1, range 1~4) | |||||||
| Everyone must get married | 0.591 + | 0.270 | 0.592 + | 0.647 ** | 1.105 ** | 0.462 + | 0.525 |
| (0.34) | (0.30) | (0.33) | (0.24) | (0.34) | (0.26) | (0.36) | |
| Marriage should be with someone from a similar family background | −0.311 | −0.338 | 0.043 | 0.144 | −0.320 | −0.148 | −0.311 |
| (0.30) | (0.31) | (0.35) | (0.24) | (0.28) | (0.25) | (0.34) | |
| It is better to get married early | 0.021 | 0.020 | 0.189 | 0.367 | −0.585 | 0.191 | 0.194 |
| (0.38) | (0.39) | (0.42) | (0.28) | (0.38) | (0.28) | (0.41) | |
| It is good to have children early if you are married | 0.160 | 0.178 | −0.263 | 0.526 * | 0.617 * | 0.641 * | 0.209 |
| (0.33) | (0.32) | (0.36) | (0.23) | (0.31) | (0.26) | (0.31) | |
| Conservative gender-role attitude (W1, range 1~4) | |||||||
| Ideally, men should have a job and women should take care of the household | −0.018 | −0.067 | 0.214 | 0.112 | 0.095 | −0.321 | −0.002 |
| (0.31) | (0.30) | (0.31) | (0.23) | (0.27) | (0.26) | (0.34) | |
| Housewives also have to go to work so that marital relations are equal | 0.272 | −0.580+ | −0.851 * | 0.084 | −0.674 * | 0.053 | −0.456 |
| (0.29) | (0.32) | (0.39) | (0.24) | (0.29) | (0.24) | (0.35) | |
| If housewives with preschool children work, it will have a negative impact on their children’s education | −0.267 | −0.196 | −0.992 ** | 0.365 | −0.124 | 0.637 * | 0.213 |
| (0.34) | (0.31) | (0.37) | (0.24) | (0.30) | (0.26) | (0.39) | |
| The house couple live in must be under the joint-ownership. | −0.424 | 0.204 | -0.043 | 0.216 | 0.239 | 0.098 | 0.153 |
| (0.28) | (0.30) | (0.32) | (0.21) | (0.23) | (0.23) | (0.29) | |
| Constant | −3.794 | 1.756 | 0.032 | −16.963 *** | −18.702 *** | −15.136 *** | −12.992 *** |
| (2.40) | (2.90) | (3.15) | (2.53) | (2.99) | (2.45) | (3.08) | |
| Observations | 149 | 143 | 114 | 910 | 617 | 578 | 153 |
| Variables | M1 | M2 | M3 |
|---|---|---|---|
| Family formation pathways (ref. no family formation with limited employment) | |||
| Work and no marriage/no children | 0.368 ** | 0.378 ** | 0.359 ** |
| (0.12) | (0.12) | (0.12) | |
| Steady employment, delayed marriage and children | 0.520 *** | 0.484 *** | 0.451 *** |
| (0.12) | (0.12) | (0.12) | |
| Married, children, and interrupted employment | 0.398 ** | 0.365 ** | 0.333 ** |
| (0.13) | (0.13) | (0.13) | |
| Stay-at-home mother | 0.342 *** | 0.430 *** | 0.410 *** |
| (0.10) | (0.10) | (0.10) | |
| Married working mother | 0.319 ** | 0.435 *** | 0.409 *** |
| (0.10) | (0.11) | (0.10) | |
| Married mother going back to work | 0.327 ** | 0.425 *** | 0.404 *** |
| (0.10) | (0.10) | (0.10) | |
| Married, no children, and some work | 0.235 * | 0.340 ** | 0.317 ** |
| (0.12) | (0.12) | (0.12) | |
| Age (W1) | −0.017 *** | −0.014 *** | |
| (0.00) | (0.00) | ||
| Education (ref. high school or below) | |||
| Two-year college | 0.060 | 0.052 | |
| (0.04) | (0.04) | ||
| Four-year college or above | 0.060 + | 0.057 | |
| (0.04) | (0.04) | ||
| Living standard at age 15 years | 0.000 | −0.006 | |
| (0.02) | (0.02) | ||
| Parents’ education (ref. middle school or below) | |||
| High school | 0.007 | 0.004 | |
| (0.03) | (0.03) | ||
| College or above | 0.022 | 0.024 | |
| (0.05) | (0.05) | ||
| Living arrangement at age 15 years (ref. living with both parents) | −0.029 | −0.051 | |
| (0.05) | (0.05) | ||
| Self-rated health (W1) | 0.126 *** | ||
| (0.02) | |||
| Regular exercise (no exercise) | |||
| 1–2 days | 0.014 | ||
| (0.05) | |||
| 3–4 days | 0.077 + | ||
| (0.04) | |||
| ≥ 5 days | −0.014 | ||
| (0.05) | |||
| Constant | 3.375 *** | 3.859 *** | 3.293 *** |
| (0.10) | (0.16) | (0.18) | |
| Observations | 2376 | 2376 | 2376 |
| R-squared | 0.009 | 0.021 | 0.043 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Woo, H.; Han, S.W. Work and Family Pathways and Their Associations with Health for Young Women in Korea. Int. J. Environ. Res. Public Health 2022, 19, 15704. https://doi.org/10.3390/ijerph192315704
Kim Y, Woo H, Han SW. Work and Family Pathways and Their Associations with Health for Young Women in Korea. International Journal of Environmental Research and Public Health. 2022; 19(23):15704. https://doi.org/10.3390/ijerph192315704
Chicago/Turabian StyleKim, Yujin, Hyeyoung Woo, and Sinn Won Han. 2022. "Work and Family Pathways and Their Associations with Health for Young Women in Korea" International Journal of Environmental Research and Public Health 19, no. 23: 15704. https://doi.org/10.3390/ijerph192315704