
Community Health Workers’ Knowledge, Attitudes, and Practices towards Epilepsy in Sofala, Central Mozambique
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Structure of Mental Health Care Systems in Mozambique
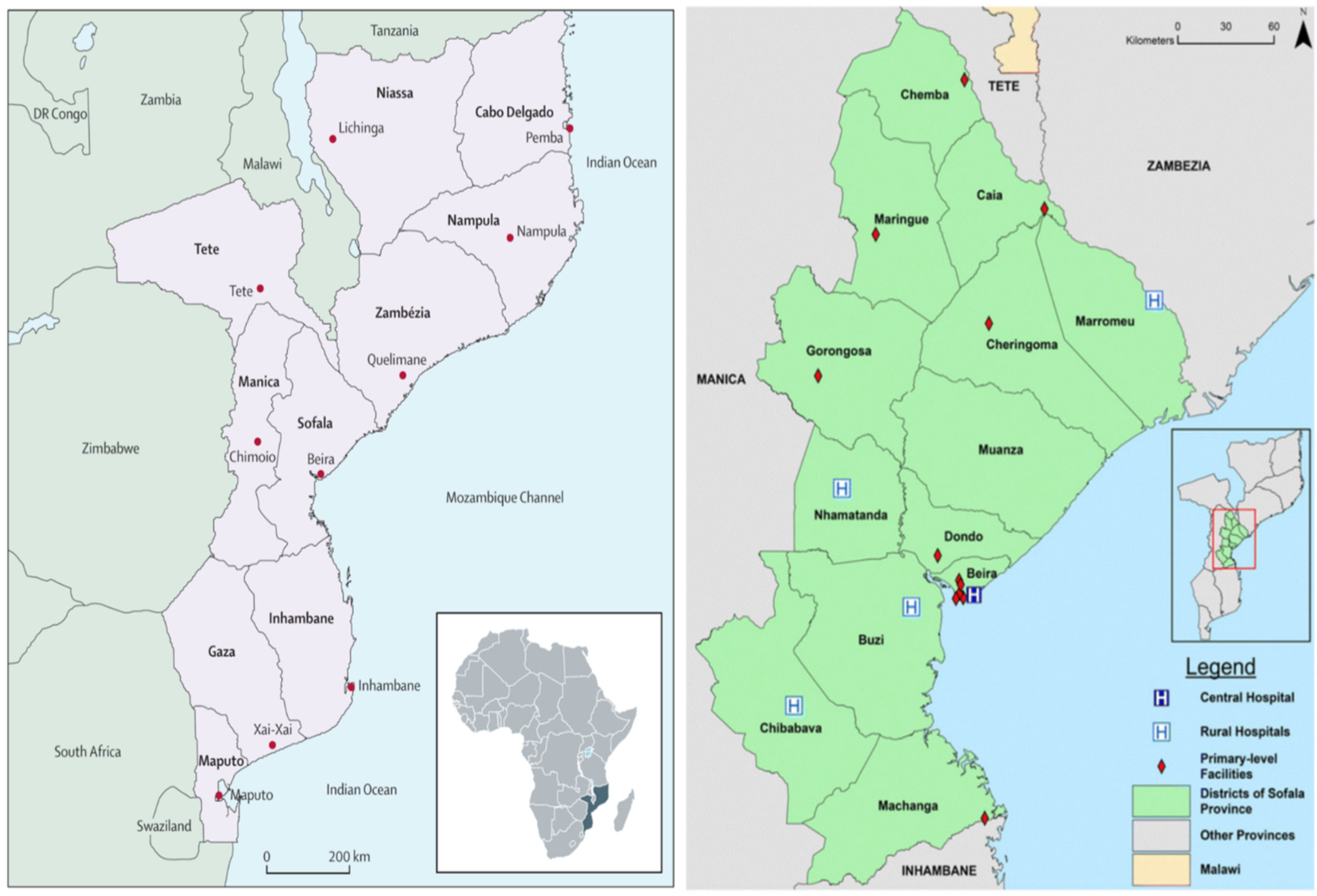
2.2. Study Design and Setting
2.3. Study Participants and Procedures
2.4. Study Instruments
2.5. Ethical Issues
2.6. Data Analysis
3. Results
3.1. Sample Description
3.2. Internal Consistency of Knowledge, Attitudes, and Practices Regarding Epilepsy Subscales and Items with Low Item Rest Correlation
3.3. CHWs Responses to the Adapted Questionnaire of Knowledge, Attitudes, and Practices towards Epilepsy
3.4. Average of Subscales of the Adapted Questionnaire of Knowledges, Attitudes, and Practices towards Epilepsy Applied to 135 CHWs in Sofala, Mozambique
4. Discussion
5. Conclusions
Key Points
- One hundred and thirty-five CHWs completed a questionnaire that included socio-demographic characteristics and 44-items divided in six subscales pertaining to KAPs towards epilepsy in nine districts of Sofala Province, Mozambique.
- The internal consistency and factor structure were examined to evaluate the reliability and construct validity of the QKAP-EPI.
- We evaluated the association between sociodemographic variables and QKAP-EPI subscales using linear regression models.
- CHWs epilepsy knowledge of medical treatment, and safety/risks were adequate. However, information on the causes of epilepsy, negative attitudes, cultural treatment, and some aspects of epileptic seizures response were low.
- Heterogeneity in the level of epilepsy knowledge was observed among CHWs in the different Districts of Sofala Province and when using different local names of epilepsy (Dzumba and Nzwiti).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- World Health Organization. Epilepsy in the who african region: Bridging the Gap. In The Global Campaign Against Epilepsy “Out of the Shadows”; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- De Boer, H.M.; Moshé, S.L.; Korey, S.R.; Purpura, D.P. ILAE/IBE/WHO Global Campaign Against Epilepsy. Curr. Opin. Neurol. 2013, 26, 219–225. [Google Scholar] [CrossRef] [PubMed]
- De Boer, H.M.; Mula, M.; Sander, J.W. The global burden and stigma of epilepsy. Epilepsy Behav. 2008, 12, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation (IHME). GBD Compare Data Visualization: Mozambique; University of Washington: Seattle, WA, USA, 2013. [Google Scholar]
- Wagenaar, B.H.; Cumbe, V.; Raunig-Berhó, M.; Rao, D.; Napúa, M.; Hughes, J.P.; Sherr, K. Health facility determinants and trends of ICD-10 outpatient psychiatric consultations across Sofala, Mozambique: Time-series analyses from 2012 to 2014. BMC Psychiatry 2015, 15, 227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagenaar, B.H.; Cumbe, V.; Raunig-Berhó, M.; Rao, D.; Kohrt, B.A.; Stergachis, A.; Napua, M.; Sherr, K. Outpatient Mental Health Services in Mozambique: Use and Treatments. Psychiatr. Serv. 2016, 67, 588–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministério de Saúde: Departamento de Saúde. Relatório Anual de Saúde Mental (2014) em Moçambique; Ministério de Saúde: Maputo, Mozambique, 2014. [Google Scholar]
- World Health Organization. Epilepsy. Geneva, Switzerland. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/epilepsy (accessed on 10 September 2019).
- World Health Organization. Epilepsy Management at Primary Health Level in Rural China: WHO/ILAE/IBE a Global Campaign against Epilepsy. Demostration Project; WHO China Rep.; World Health Organization: Geneva, Switzerland, 2009; pp. 1–32. [Google Scholar]
- Baskind, R.; Birbeck, G. Epilepsy Care in Zambia: A Study of Traditional Healers. Epilepsia 2005, 46, 1121–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Organización Mundial de la Salud. Trastornos Neurológicos: Desafíos para la Salud Pública; Organización Mundial de la Salud: Washington, DC, USA, 2006. [Google Scholar]
- Patterson, V.; Samant, S.; Singh, M.B.; Jain, P.; Agavane, V.; Jain, Y. Diagnosis of epileptic seizures by community health workers using a mobile app: A comparison with physicians and a neurologist. Seizure 2018, 55, 4–8. [Google Scholar] [CrossRef] [Green Version]
- Santos, P.F.; Wainberg, M.L.; Caldas-de-Almeida, J.M.; Saraceno, B.; Mari, J.D.J. Overview of the mental health system in Mozambique: Addressing the treatment gap with a task-shifting strategy in primary care. Int. J. Ment. Health Syst. 2016, 10, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Patel, V.; Weiss, H.; Chowdhary, N.; Naik, S.; Pednekar, S.; Chatterjee, S.; De Silva, M.; Bhat, B.; Araya, R.; King, M.; et al. The effectiveness of a lay health worker led intervention for depressive and anxiety disorders in primary care: The MANAS cluster randomized trial in Goa, India. Lancet 2010, 376, 2086–2095. [Google Scholar] [CrossRef] [Green Version]
- Chomba, E.N.; Haworth, A.; Atadzhanov, M.; Mbewe, E.; Birbeck, G.L. Zambian health care workers’ knowledge, attitudes, beliefs, and practices regarding epilepsy. Epilepsy Behav. 2007, 10, 111–119. [Google Scholar] [CrossRef] [Green Version]
- Ezeala-Adikaibe, B.A.; Achor, J.U.; Nwabueze, A.C.; Agomoh, A.O.; Chikani, M.; Ekenze, O.S.; Onwuekwe, I.O.; Orakwue, M. Knowledge, attitude, and practice of epilepsy among community residents in Enugu, South East Nigeria. Seizure 2014, 23, 882–888. [Google Scholar] [CrossRef] [PubMed]
- Dolo, H.; Mandro, M.; Wonya’Rossi, D.; Ngave, F.; Fraeyman, J.; Siewe, J.N.; Suykerbuyk, P.; Colebunders, R. Community perceptions of epilepsy and its treatment in an onchocerciasis endemic region in Ituri, Democratic Republic of Congo. Infect. Dis. Poverty 2018, 7, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuliano, L.; Cicero, C.E.; Padilla, S.; Camargo, M.; Sofia, V.; Zappia, M.; Bartoloni, A.; Gómez, E.B.C.; Nicoletti, A. Knowledge and attitudes towards epilepsy among nonmedical health workers in rural Bolivia: Results after a long-term activity in the Chaco region. Epilepsy Behav. 2018, 85, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Musyimi, C.W.; Mutiso, V.N.; Ndetei, D.M.; Unanue, I.; Desai, D.; Patel, S.G.; Musau, A.; Henderson, D.C.; Nandoya, E.S.; Bunders, J. Mental health treatment in Kenya: Task-sharing challenges and opportunities among informal health providers. Int. J. Ment. Health Syst. 2017, 11, 45. [Google Scholar] [CrossRef] [Green Version]
- Ministério de Saúde: Direcção Nacional de Saúde Pública. Programa de Revitalização dos Agentes Polivalentes Elementares de Saúde—APEs; Ministério de Saúde: Maputo, Mozambique, 2010. [Google Scholar]
- Cumbe, V.F.J.; Muanido, A.G.; Manaca, M.N.; Fumo, H.; Chiruca, P.; Hicks, L.; de Jesus Mari, J.; Wagenaar, B.H. Validity and Item Response Theory Properties of the Patient Health Questionnaire-9 for Primary Care Depression Screening in Mozambique (PHQ-9- MZ). BMC Psychiatry 2019, 20, 382. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, P.F. 25 Anos de Saúde Mental em Moçambique (1984–2009). Rev. Psique. 2011, 1. [Google Scholar]
- Instituto Nacional de Estatística (INE). Anuário da Província de Sofala, 2017; Instituto Nacional de Estatística (INE): Maputo, Moçambique, 2017. [Google Scholar]
- Direcção Provincial de Saúde de Sofala; Departamento de Saúde Pública. Relatório Anual de Saúde Mental, 2017; Direcção Provincial de Saúde de Sofala: Beira, Moçambique, 2018. [Google Scholar]
- Direcção Provincial de Saúde de Sofala. Departamento Provincial de Planificação e Cooperação: Projecção da População 2017; Direcção Provincial de Saúde de Sofala: Beira, Mozambique, 2018. [Google Scholar]
- Mbuba, C.K.; Abubakar, A.; Hartley, S.; Odermatt, P.; Newton, C.R.; Carter, J.A. Development and validation of the Kilifi Epilepsy Beliefs and Attitude Scale. Epilepsy Behav. 2012, 24, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.H.; Han, H.-R.; Kim, M.T.; Chan, K.S. An Introduction to Item Response Theory for Patient-Reported Outcome Measurement. Patient Patient Cent. Outcomes Res. 2014, 7, 23–35. [Google Scholar] [CrossRef] [Green Version]
- Nhancale, P.S. Convulsões, Medo e Estigma: Epilepsia, Ejile-Jile, Nhoka yi Kulo no Bairro Central “C”, Maputo. Bachelor’s Thesis, Universidade Eduardo Mondlane, Faculdade de Letras e Ciências Sociais, Maputo, Mozambique, 2015. [Google Scholar]
- El Sharkawy, G.; Newton, C.; Hartley, S. Attitudes and practices of families and health care personnel toward children with epilepsy in Kilifi, Kenya. Epilepsy Behav. 2006, 8, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Langa, A.P.; Gouveia, M.L.; Nhantumbo, B.; Andrassone, P.; Nhabinde, A.; Wate, J. Relatório do Estudo Sobre Comportamentos, Atitudes e Práticas Sobre a Epilepsia, Nos Distritos de Chibuto e Chókwè, Província de Gaza; Departamento de Saúde Mental: Maputo, Mozambique, 2012. [Google Scholar]
- Andermann, L.F. Epilepsy in Our World: An Ethnographic View. Epilepsy Behav. 2000, 1, 169–175. [Google Scholar] [CrossRef]
- Desai, P.; Padma, M.V.; Jain, S.; Maheshwari, M.C. Knowledge, attitudes, and practice of epilepsy: Experience at a comprehensive rural health services project. Seizure 1998, 7, 133–138. [Google Scholar] [CrossRef]
- Martin, A.R. Exploring Patient Beliefs: Steps to Enhancing Physician-Patient Interaction. Arch. Intern. Med. 1983, 143, 1773–1775. [Google Scholar] [CrossRef]
- Giel, R. The Epileptic Outcast. East Afr. Med. J. 1968, 45, 27–31. [Google Scholar]
- Kabir, M.; Iliyasu, Z.; Abubakar, I.S.; Kabir, Z.S.; Farinyaro, A.U. Knowledge, attitude, and beliefs about epilepsy among adults in a northern Nigerian urban. Ann. Afr. Med. 2005, 4, 107–112. [Google Scholar]


{kind=link}
| Variables | Categories | n (%) |
|---|---|---|
| Age | 20–30 | 45 (33, 33) |
| 31–40 | 41 (30, 37) | |
| 41–50 | 15 (11, 11) | |
| >50 | 33 (24, 44) | |
| Missing | 1 (0, 74) | |
| Sex | Male | 94 (69, 63) |
| Female | 40 (29, 63) | |
| Missing | 1 (0, 74) | |
| Civil Status | Single | 47 (34, 81) |
| Married | 18 (13, 33) | |
| Common Law Marriage | 58 (42, 96) | |
| Divorced | 3 (2, 22) | |
| Separated | 7 (5, 19) | |
| Widow | 2 (1, 48) | |
| Schooling Level Achieved | Primary | 44 (32, 59) |
| Secondary or High | 75 (55, 56) | |
| Missing | 16 (11, 85) | |
| Primary Occupation | Unemployed | 63 (46, 67) |
| Farmer | 31 (22, 96) | |
| Other (e.g., Students, Teacher, and Trader) | 40 (29, 63) | |
| Missing | 1 (0, 74) | |
| Religion | Christian | 95 (70, 37) |
| Other Religion | 36 (26, 67) | |
| Missing | 4 (2, 96) |
| Subscale | Ordinal Alpha | Items with Low Item-Rest Correlation 2 |
|---|---|---|
| Causes of epilepsy | 0.650 | 1 |
| Medical treatment 1 | 0.694 | 13, 14 |
| Cultural treatment | 0.797 | 15, 22 |
| Safety and risks | 0.926 | — |
| Negative attitudes | 0.904 | — |
| Practices during seizures | 0.238 | 41, 42 |
| Item of Each Scale | I Don’t Believe n (%) | Believe a Little n (%) | Totally Believe n (%) |
|---|---|---|---|
| Causes of Epilepsy | |||
| 1.Epilepsy is Inherited | 71(52.59) | 20 (14.81) | 44 (32.59) |
| 2. Head Injury | 36 (26.67) | 19 (14.07) | 80 (59.26) |
| 3. Childbirth Injury | 58 (42.96) | 26 (19.26) | 51 (37.78) |
| 4. Malaria/Meningitis/Fever | 50 (37.04) | 23 (17.04) | 62 (45.93) |
| 5. Brain Injury | 28 (20.74) | 33 (24.44) | 74 (54.81) |
| Medical Treatment | |||
| 6. Possible to Treat Epilepsy | 12 (8.89) | 19 (14.07) | 104 (77.04) |
| 7. Antiepileptic Medicines Should Be Taken Continuously to Function Properly | 12 (8.89) | 18 (13.33) | 105 (77.78) |
| 8. Antiepileptic Medicines Are Available at the Health Facilities | 7 (5.19) | 9 (6.67) | 119 (88.15) |
| 9. Njiri Njiri * is Best Treated by a Doctor | 18 (13.33) | 20 (14.81) | 97 (71.85) |
| 10. PWE Should Be Placed in a Safe Place During the Seizures | 3 (2.22) | 0 (0.0) | 132 (97.78) |
| 11. Antiepileptic Medicines Control Seizures | 16 (11.85) | 22 (16.30) | 97 (71.85) |
| 12. Lack of Antiepileptic Medicines May Precipitate Seizures on PWE | 17 (12.59) | 20 (14.81) | 98 (72.59) |
| 13. Nzwite * is Best treated By a Doctor | 17 (12.59) | 16 (11.85) | 102 (75.56) |
| 14. Antiepileptic Medicines May Cause Side Effects | 42 (31.11) | 38 (28.15) | 55 (40.74) |
| Cultural Treatment | |||
| 15. PWE that Burn Will Never Be Cured | 69 (51.11) | 21 (15.56) | 45 (33.33) |
| 16. Dzumba * Can Be Treated Unlike Nzwite | 64 (47.41) | 32 (23.70) | 39 (28.89) |
| 17. Guru * is Best Treated by a Nhanga | 94 (69.63) | 25 (18.52) | 16 (11.85) |
| 18. Spreading Water in PWE During Seizures Treats Epilepsy | 107 (79.26) | 16 (11.85) | 12 (8.89) |
| 19. Make Smell Shoes to PWE, During Seizures Treats Epilepsy | 107 (79.26) | 16 (11.85) | 12 (8.89) |
| 20. Fumigation Treats Epilepsy | 109 (80.74) | 12 (8.89) | 14 (10.37) |
| 21. It is Good to Put a Stick in the Mouth of the PWE During Seizures | 104 (77.04) | 12 (8.89) | 19 (14.07) |
| 22. Legs of a PWE Should Be Stretched During Seizures | 64 (47.41) | 28 (20.74) | 43 (31.85) |
| 23. Dwiti * is Best Treated by a Nhanga ** | 84 (62.22) | 33 (24.44) | 18 (13.33) |
| Safety and Risks | |||
| 24. PWE Should Not Climb the Trees | 26 (19.26) | 9 (6.67) | 100 (74.04) |
| 25. PWE Should Not Drive | 25 (18.52) | 15 (11.11) | 95 (70.37) |
| 26. PWE Should Avoid Being Near the Fire | 15 (11.11) | 5 (3.70) | 115 (85.19) |
| 27.PWE Should Avoid Staying in Places Near Water | 17 (12.59) | 11 (8.15) | 107 (79.26) |
| Negative Attitudes | |||
| 28. PWE Should Not or Can Not Get Married | 89 (65.93) | 14 (10.37) | 32 (23.70) |
| 29. PWE Should Not Go to School | 97 (71.85) | 8 (5.93) | 30 (22.22) |
| 30. PWE Should Not or Can Not Have a Job | 100 (74.04) | 13 (9.63) | 22 (16.3) |
| 31. PWE Should Not or Can Not Have a Normal Life | 83 (61.48) | 17 (12.59) | 35 (25.93) |
| 32. PWE Should Be Isolated | 109 (80.74) | 8 (5.93) | 18 (13.33) |
| 33. PWE Should Be Rejected | 109 (80.74) | 12 (8.89) | 14 (10.37) |
| 34. PWE Should Be Offended | 112 (82.96) | 9 (6.67) | 14 (10.37) |
| 35. PWE are Burden for Society and Family | 74 (54.81) | 22 (16.30) | 39 (28.89) |
| 36. PWE Performs Poorly at School | 68 (50.37) | 34 (25.19) | 33 (24.44) |
| 37. PWE Gives a Lot of Work | 70 (51.85) | 27 (20.00) | 38 (28.15) |
| 38. PWE Are Crazy | 84 (62.22) | 23 (17.04) | 28 (20.74) |
| Practices During Seizures | |||
| 39. We Should Put a Stick in the Mouth of the PWE During Seizures | 99 (73.33) | 14 (10.37) | 22 (16.30) |
| 40. We Should Give a Drink to the PWE During Seizures | 106 (78.52) | 17 (12.59) | 12 (8.89) |
| 41. We Should Stay Away from PWE During Seizures | 96 (71.11) | 14 (10.37) | 25 (18.52) |
| 42. We Should Hold PWE During Seizures to Stop Seizures | 44 (32.59) | 21 (15.85) | 70 (51.85) |
| 43. We Must Help PWE During the Seizures Not to Hit the Head on the Ground | 14 (10.37) | 6 (4.44) | 115 (85.19) |
| 44. We Must Place the PWE in the Right Lateral Safety Position to Avoid Aspiration | 12 (8.89) | 13 (9.63) | 110 (81.48) |
| Mean (SD) | (1) | (2) | (3) | (4) | (5) | (6) | (7) | |
|---|---|---|---|---|---|---|---|---|
| (1) Causes of epilepsy | 1.10 (0.53) | -- | ||||||
| (2) Medical treatment | 1.63 (0.28) | 0.170 | -- | |||||
| (3) Cultural treatment | 1.48 (0.39) | −0.213 | 0.007 | -- | ||||
| (4) Safety and risks | 1.62 (0.59) | −0.078 | 0.159 | 0.108 | -- | |||
| (5) Negative Attitudes | 1.47 (0.48) | −0.118 | −0.071 | 0.392 | 0.319 | -- | ||
| (6) Practices of sticking into a mouth, give a drink, stay away | 1.43 (0.42) | −0.007 | 0.132 | 0.174 | 0.141 | 0.151 | -- | |
| (7) Practices of holding, helping, placing in safety position | 1.60 (0.48) | −0.109 | 0.054 | 0.575 | 0.204 | 0.254 | 0.086 | -- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cumbe, V.F.J.; Greene, C.; Fumo, A.M.T.; Fumo, H.; Mabunda, D.; Gouveia, L.C.; Oquendo, M.A.; Duarte, C.S.; Sidat, M.; Mari, J.d.J. Community Health Workers’ Knowledge, Attitudes, and Practices towards Epilepsy in Sofala, Central Mozambique. Int. J. Environ. Res. Public Health 2022, 19, 15420. https://doi.org/10.3390/ijerph192215420
Cumbe VFJ, Greene C, Fumo AMT, Fumo H, Mabunda D, Gouveia LC, Oquendo MA, Duarte CS, Sidat M, Mari JdJ. Community Health Workers’ Knowledge, Attitudes, and Practices towards Epilepsy in Sofala, Central Mozambique. International Journal of Environmental Research and Public Health. 2022; 19(22):15420. https://doi.org/10.3390/ijerph192215420
Chicago/Turabian StyleCumbe, Vasco Francisco Japissane, Claire Greene, Afonso Mazine Tiago Fumo, Hélder Fumo, Dirceu Mabunda, Lídia Chaúque Gouveia, Maria A. Oquendo, Cristiane S. Duarte, Mohsin Sidat, and Jair de Jesus Mari. 2022. "Community Health Workers’ Knowledge, Attitudes, and Practices towards Epilepsy in Sofala, Central Mozambique" International Journal of Environmental Research and Public Health 19, no. 22: 15420. https://doi.org/10.3390/ijerph192215420