
Clinicians’ Emotional Reactions toward Patients with Depressive Symptoms in Mood Disorders: A Narrative Scoping Review of Empirical Research
 , and
, and
Abstract
:1. Introduction
1.1. Mood Disorders
1.2. Working with Depressive Symptoms in Patients with Mood Disorders
1.3. Countertransference and Therapist Subjective Reactions
1.4. Aims of the Present Review
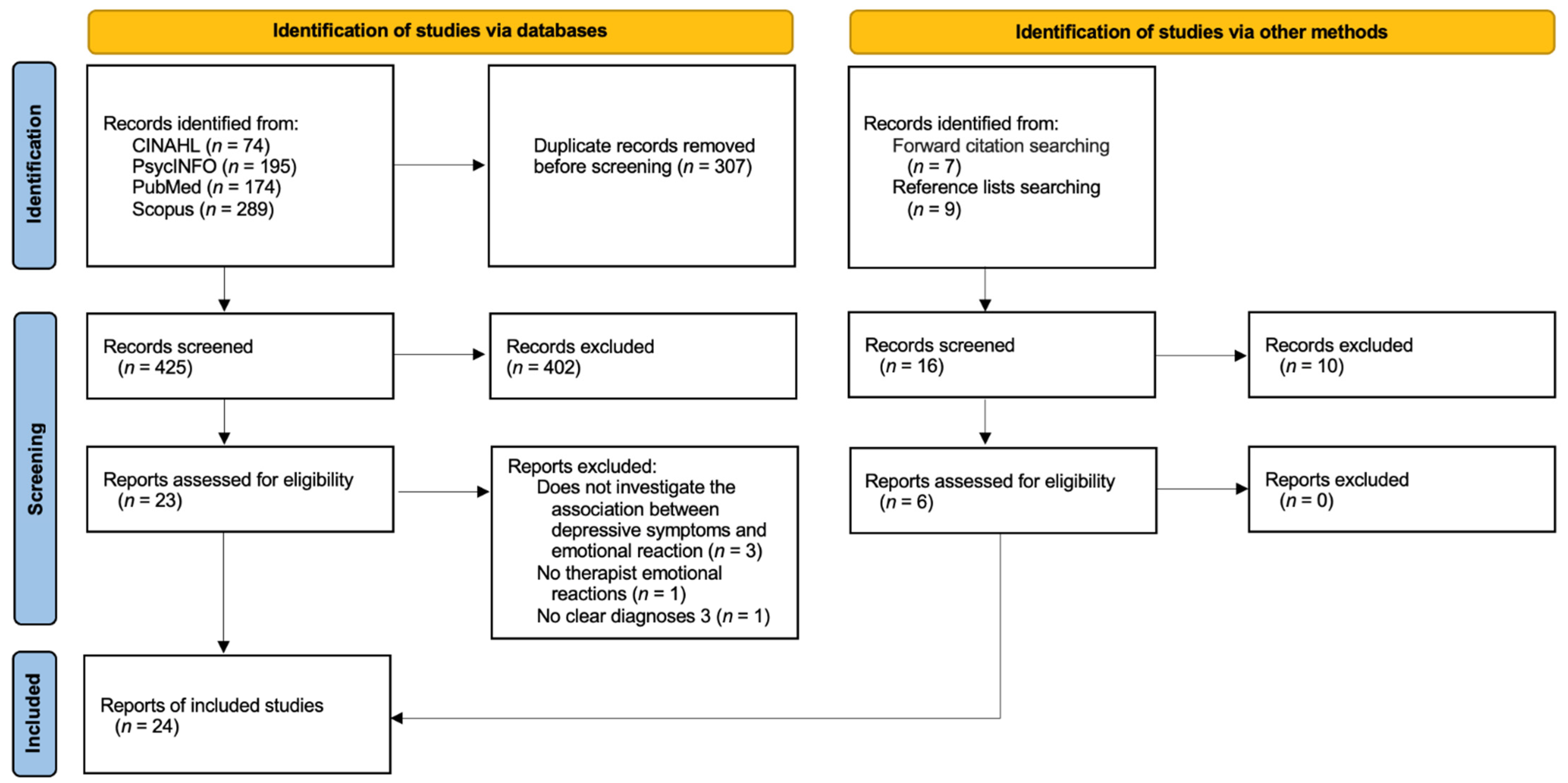
2. Methods
3. Results
3.1. Comparison between/among Different Diagnostic Groups
3.2. Clinician’s Response to Patient’s Characteristics
3.3. Countertransference and Psychotherapy Elements, Process, and Outcome
3.4. Clinicians’ Responses to Suicidal Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd ed.; American Psychiatric Publishing: Washington, DC, USA, 1980. [Google Scholar]
- Phillips, M.L.; Kupfer, D.J. Bipolar disorder diagnosis: Challenges and future directions. Lancet 2013, 381, 1663–1671. [Google Scholar] [CrossRef] [Green Version]
- Solmi, M.; Radua, J.; Olivola, M.; Croce, E.; Soardo, L.; Salazar de Pablo, G.; Il Shin, J.; Kirkbride, J.B.; Jones, P.; Kim, J.H.; et al. Age at onset of mental disorders worldwide: Large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 2022, 27, 281–295. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Datta, S.; Suryadevara, U.; Cheong, J. Mood Disorders. Continuum 2021, 27, 1712–1737. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- De Hert, M.; Correll, C.U.; Bobes, J.; Cetkovich-Bakmas, M.; Cohen, D.; Asai, I.; Detraux, J.; Gautam, S.; Möller, H.J.; Ndetei, D.M.; et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry 2011, 10, 52–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefana, A.; Youngstrom, E.A.; Chen, J.; Hinshaw, S.; Maxwell, V.; Michalak, E.; Vieta, E. The COVID-19 pandemic is a crisis and opportunity for bipolar disorder. Bipolar Disord. 2020, 22, 641–643. [Google Scholar] [CrossRef] [PubMed]
- Youngstrom, E.A.; Hinshaw, S.P.; Stefana, A.; Chen, J.; Michael, K.; Van Meter, A.; Maxwell, V.; Michalak, E.E.; Choplin, E.G.; Vieta, E. Working with bipolar disorder during the COVID-19 pandemic: Both crisis and opportunity. Wiki J. Med. 2020, 7, 1–9. [Google Scholar] [CrossRef]
- Malhi, G.S.; Bassett, D.; Boyce, P.; Bryant, R.; Fitzgerald, P.B.; Fritz, K.; Hopwood, M.; Lyndon, B.; Mulder, R.; Murray, G.; et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust. N. Z. J. Psychiatry 2015, 49, 1087–1206. [Google Scholar] [CrossRef]
- Kennedy, S.H.; Lam, R.W.; McIntyre, R.S.; Tourjman, S.V.; Bhat, V.; Blier, P.; Hasnain, M.; Jollant, F.; Levitt, A.J.; MacQueen, G.M.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: Section 3. Pharmacological treatments. Can. J. Psychiatry 2016, 61, 540–560. [Google Scholar] [CrossRef]
- Bonnín, C.M.; Jiménez, E.; Solé, B.; Torrent, C.; Radua, J.; Reinares, M.; Grande, I.; Ruíz, V.; Sánchez-Moreno, J.; Martínez-Arán, A.; et al. Lifetime psychotic symptoms, subthreshold depression and cognitive impairment as barriers to functional recovery in patients with bipolar disorder. J. Clin. Med. 2019, 8, 1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cipriani, A.; Zhou, X.; Del Giovane, C.; Hetrick, S.E.; Qin, B.; Whittington, C.; Coghill, D.; Zhang, Y.; Hazell, P.; Leucht, S.; et al. Comparative efficacy and tolerability of antidepressants for major depressive disorder in children and adolescents: A network meta-analysis. Lancet 2016, 388, 881–890. [Google Scholar] [CrossRef]
- Cuijpers, P.; Quero, S.; Noma, H.; Ciharova, M.; Miguel, C.; Karyotaki, E.; Cipriani, A.; Cristea, I.O.; Furukawa, T.A. Psychotherapies for depression: A network meta-analysis covering efficacy, acceptability and long-term outcomes of all main treatment types. World Psychiatry 2021, 20, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Guidi, J.; Fava, G.A. Sequential combination of pharmacotherapy and psychotherapy in major depressive disorder: A systematic review and meta-analysis. JAMA Psychiatry 2021, 78, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Aran, A.; Vieta, E. Precision psychotherapy. Eur. Neuropsychopharmacol. 2022, 55, 20–21. [Google Scholar] [CrossRef] [PubMed]
- Grande, I.; Berk, M.; Birmaher, B.; Vieta, E. Bipolar disorder. Lancet 2016, 387, 1561–1572. [Google Scholar] [CrossRef]
- Kalin, N.H. Advances in understanding and treating mood disorders. Am. J. Psychiatry 2020, 177, 647–650. [Google Scholar] [CrossRef]
- Carvalho, A.F.; Firth, J.; Vieta, E. Bipolar Disorder. NEJM 2020, 383, 58–66. [Google Scholar] [CrossRef]
- Jenkins, M.M.; Youngstrom, E.A.; Youngstrom, J.K.; Feeny, N.C.; Findling, R.L. Generalizability of evidence-based assessment recommendations for pediatric bipolar disorder. Psychol. Assess. 2012, 24, 269–281. [Google Scholar] [CrossRef] [Green Version]
- Youngstrom, E.A.; Halverson, T.F.; Youngstrom, J.K.; Lindhiem, O.; Findling, R.L. Evidence-Based Assessment from Simple Clinical Judgments to Statistical Learning: Evaluating a Range of Options Using Pediatric Bipolar Disorder as a Diagnostic Challenge. Clin. Psychol. Sci. Pract. 2018, 6, 243–265. [Google Scholar] [CrossRef]
- Hunsley, J.; Mash, E.J. A Guide to Assessments That Work, 2nd ed.; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Youngstrom, E.A.; Van Meter, A.; Frazier, T.W.; Hunsley, J.; Prinstein, M.J.; Ong, M.L.; Youngstrom, J.K. Evidence-based assessment as an integrative model for applying psychological science to guide the voyage of treatment. Clin. Psychol. Sci. Pract. 2017, 24, 331–363. [Google Scholar] [CrossRef]
- Durosini, I.; Aschieri, F. Therapeutic assessment efficacy: A meta-analysis. Psychol. Assess. 2021, 33, 962–972. [Google Scholar] [CrossRef] [PubMed]
- Kealy, D.; Rice, S.M.; Ferlatte, O.; Ogrodniczuk, J.S.; Oliffe, J.L. Better doctor-patient relationships are associated with men choosing more active depression treatment. JABFM 2019, 32, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambert, W.; Salzer, M.S.; Bickman, L. Clinical outcome, consumer satisfaction, and ad hoc ratings of improvement in children’s mental health. J. Consult. Clin. Psychol. 1998, 66, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Youngstrom, E.A.; Van Meter, A. Empirically supported assessment of children and adolescents. Clin. Psychol. Sci. Pract. 2016, 23, 327–347. [Google Scholar] [CrossRef]
- Wright, A.J.; Pade, H.; Gottfried, E.D.; Arbisi, P.A.; McCord, D.M.; Wygant, D.B. Evidence-based clinical psychological assessment (EBCPA): Review of current state of the literature and best practices. Prof. Psychol. Res. Pract. 2022, 53, 372–386. [Google Scholar] [CrossRef]
- Stricker, G. Reflections on psychotherapy integration. Clin. Psychol. Sci. Pract. 1994, 1, 3–12. [Google Scholar] [CrossRef]
- Finn, S.E. Our Clients’ Shoes; Routledge: New York, NY, USA, 2007. [Google Scholar]
- Stricker, G. A second look at psychotherapy integration. J. Psychother. Integr. 2010, 20, 397–405. [Google Scholar] [CrossRef]
- Gelso, C.J. The Therapeutic Relationship in Psychotherapy Practice: An Integrative Perspective; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Stefana, A.; Gamba, A. Semeiotica e diagnosi psico (pato) logica. J. Psychopathol. 2013, 19, 351–358. [Google Scholar]
- Psychodynamic Diagnostic Manual, (PDM-2), 2nd ed.; Lingiardi, V.; McWilliams, N. (Eds.) Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Norcross, J.C.; Lambert, M.J. Psychotherapy relationships that work III. Psychotherapy 2018, 55, 303–315. [Google Scholar] [CrossRef]
- Bhatia, A.; Gelso, C.J. Therapists’ perspective on the therapeutic relationship: Examining a tripartite model. Couns. Psychol. Q. 2018, 31, 271–293. [Google Scholar] [CrossRef]
- Norcross, J.C.; Lambert, M.J. Psychotherapy relationships that work, 3rd ed. In Volume 1: Evidence-Based Therapist Contributions; Oxford University Press: New York, NY, USA, 2019. [Google Scholar]
- Horesh, D.; Hasson-Ohayon, I.; Harwood-Gross, A. The contagion of psychopathology across different psychiatric disorders: A comparative theoretical analysis. Brain Sci. 2021, 12, 67. [Google Scholar] [CrossRef] [PubMed]
- Joiner, T.E.; Katz, J. Contagion of depressive symptoms and mood: Meta-analytic review and explanations from cognitive, behavioral, and interpersonal viewpoints. Clin. Psychol. Sci. Pract. 1999, 6, 149–164. [Google Scholar] [CrossRef]
- Rahn, E.; Mahnkopf, A. Lehrbuch Psychiatrie für Studium und Beruf; Psychiatrie Verlag: Cologne, Germany, 2009. [Google Scholar]
- Roubal, J.; Rihacek, T. Therapists’ in-session experiences with depressive clients: A grounded theory. Psychother. Res. 2016, 26, 206–219. [Google Scholar] [CrossRef]
- Deutsch, C.J. Self-reported sources of stress among psychotherapists. Prof. Psychol. Res. Pract. 1984, 15, 833–845. [Google Scholar] [CrossRef]
- Jenaro, C.; Flores, N.; Arias, B. Burnout and coping in human service practitioners. Prof. Psychol. Res. Pract. 2007, 38, 80–87. [Google Scholar] [CrossRef]
- Cain, N.R. Psychotherapists with personal histories of psychiatric hospitalization: Countertransference in wounded healers. Psychiatr. Rehabil. J. 2000, 24, 22–28. [Google Scholar] [CrossRef]
- Brody, E.M.; Farber, B.A. The effects of therapist experience and patient diagnosis on countertransference. Psychotherapy 1996, 33, 372–380. [Google Scholar] [CrossRef]
- Koekkoek, B.; van Meijel, B.; Hutschemaekers, G. “Difficult patients” in mental health care: A review. Psychiatr. Serv. 2006, 57, 795–802. [Google Scholar] [CrossRef]
- McWilliams, N. Psychoanalytic Diagnosis: Understanding Personality Structure in the Clinical Process, 2nd ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Wolf, A.W.; Goldfried, M.R.; Muran, J.C. Introduction. In Transforming Negative Reactions to Clients: From Frustration to Compassion; Wolf, A.W., Goldfried, M.R., Muran, J.C., Eds.; American Psychological Association: Washington, DC, USA, 2013; pp. 3–18. [Google Scholar]
- Wolf, A.W.; Goldfried, M.R.; Muran, J.C. Conclusion and clinical guidelines. In Transforming Negative Reactions to Clients: From Frustration to Compassion; Wolf, A.W., Goldfried, M.R., Muran, J.C., Eds.; American Psychological Association: Washington, DC, USA, 2013; pp. 269–282. [Google Scholar]
- Wolf, A.W.; Goldfried, M.R.; Muran, J.C. Therapist negative reactions: How to transform toxic experiences. In How and Why Are Some Therapists Better than Others?: Understanding Therapist Effects; Castonguay, L.G., Hill, C.E., Eds.; American Psychological Association: Washington, DC, USA, 2017; pp. 175–192. [Google Scholar]
- Stefana, A. The origins of the notion of countertransference. Psychoanal. Rev. 2015, 102, 437–460. [Google Scholar] [CrossRef]
- Stefana, A. History of Countertransference. From Freud to the British Object Relations School; Routledge: London, UK; New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Stefana, A.; Hinshelwood, R.D.; Borensztejn, C.L. Racker and Heimann on countertransference: Similarities and differences. Psychoanal. Quart. 2021, 90, 105–137. [Google Scholar] [CrossRef] [PubMed]
- Fiedler, F.E. On different types of countertransference. J. Clin. Psychol. 1951, 7, 101–107. [Google Scholar] [CrossRef]
- Cutler, R.L. Countertransference effects in psychotherapy. J. Consult. Psychol. 1958, 22, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A.; Lipsher, D.H.; Miller, P.E. Psychotherapists approach-avoidance reactions to patients’ expressions of hostility. J. Consult. Psychol. 1960, 24, 1–8. [Google Scholar] [CrossRef]
- Yulis, S.; Kiesler, D.J. Countertransference response as a function of therapist anxiety and content of patient talk. J. Consult. Clin. Psychol. 1968, 32, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Gelso, C.J.; Hayes, J.A. Countertransference and the Therapist’s Inner Experience: Perils and Possibilities; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2007. [Google Scholar]
- Colson, D.B.; Allen, J.G.; Coyne, L.; Dexter, N.; Jehl, N.; Mayer, C.A.; Spohn, H. An anatomy of countertransference: Staff reactions to difficult psychiatric hospital patients. Hosp. Community Psych. 1986, 37, 923–928. [Google Scholar] [CrossRef]
- Lewis, G.; Appleby, L. Personality disorder: The patients psychiatrists dislike. BJP 1988, 153, 44–49. [Google Scholar] [CrossRef]
- Newman, C.F. Cognitive Therapy, Countertransference, and the Borderline Patient; Unpublished manuscript; Center for Cognitive Therapy: Philadelphia, PA, USA, 1989. [Google Scholar]
- Beck, A.T.; Freeman, E. Associates Cognitive Therapy of Personality Disorders; The Guilford Press: London, UK, 1990. [Google Scholar]
- Hayes, J.A.; Gelso, C.J.; Goldberg, S.; Kivlighan, D.M. Countertransference management and effective psychotherapy: Meta-analytic findings. Psychotherapy 2018, 55, 496–507. [Google Scholar] [CrossRef]
- Fonzi, L.; Pallagrosi, J.; Picardi, A.; Biondi, M.; Pallagrosi, M. Exploring how the psychiatrist experiences the patient during the diagnostic evaluation: The Assessment of Clinician’s Subjective Experience (ACSE). Phenomenol. Cogn. Sci. 2022, 21, 107–119. [Google Scholar] [CrossRef]
- Gelso, C.J.; Kline, K.V. Some directions for research and theory on countertransference. Psychother. Res. 2022, 32, 46–51. [Google Scholar] [CrossRef]
- Gabbard, G.O. Psychodynamic Psychiatry in Clinical Practice, 5th ed.; American Psychiatric Pub: Washington, DC, USA, 2014. [Google Scholar]
- Tanzilli, A.; Lingiardi, V. The Diagnostic Use of Countertransference in Psychodynamic Practice. In The Clinician in the Psychiatric Diagnostic Process; Biondi, M., Picardi, A., Pallagrosi, M., Fonzi, L., Eds.; Springer: Cham, Switzerland, 2022. [Google Scholar] [CrossRef]
- Stefana, A.; Bulgari, V.; Youngstrom, E.; Bordin, C.; Dakanalis, A.; Hopwood, C. Patient personality and psychotherapist reactions in individual psychotherapy setting: A systematic review. Clin. Psychol. Psychot. 2020, 27, 697–713. [Google Scholar] [CrossRef] [PubMed]
- Gabbard, G.O. Long-Term Psychodynamic Psychotherapy: A Basic Text; American Psychiatric Association Publishing: Arlington, VA, USA, 2017. [Google Scholar]
- Robinson, O.C. The idiographic/nomothetic dichotomy: Tracing historical origins of contemporary confusions. Hist. Philos. Psychol. 2011, 13, 32–39. [Google Scholar]
- Lingiardi, V.; McWilliams, N. Introduction to the special issue on the Psychodynamic Diagnostic Manual, 2nd Edition (PDM-2): The PDM: Yesterday, today, tomorrow. Psychoanal. Psychol. 2018, 35, 289–293. [Google Scholar] [CrossRef] [Green Version]
- McIntyre, S.M.; Schwartz, R.C. Therapists’ differential countertransference reactions toward clients with major depression or borderline personality disorder. J. Clin. Psychol. 1998, 54, 923–931. [Google Scholar] [CrossRef]
- Kiesler, D.J. IMI: Manual for the Impact Message Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1987. [Google Scholar]
- Carpenter, B.N.; Suhr, P. Stress Appraisal: Measurement and Correlates; American Psychological Association: Washington, DC, USA, 1988. [Google Scholar]
- Pallagrosi, M.; Fonzi, L.; Picardi, A.; Biondi, M. Association between clinician’s subjective experience during patient evaluation and psychiatric diagnosis. Psychopathology 2016, 49, 83–94. [Google Scholar] [CrossRef]
- Pallagrosi, M.; Fonzi, L.; Picardi, A.; Biondi, M. Assessing clinician’s subjective experience during interaction with patients. Psychopathology 2014, 2014. 47, 111–118. [Google Scholar] [CrossRef]
- Putrino, N.; Casari, L.; Mesurado, B.; Etchevers, M. Psychotherapists’ emotional and physiological reactions toward patients with either borderline personality disorder or depression. Psychother. Res. 2020, 30, 912–919. [Google Scholar] [CrossRef]
- Rossberg, J.I.; Karterud, S.; Pedersen, G.; Friis, S. Psychiatric symptoms and countertransference feelings: An empirical investigation. Psychiat. Res. 2010, 178, 191–195. [Google Scholar] [CrossRef]
- Røssberg, J.I.; Hoffart, A.; Friis, S. Psychiatric staff members’ emotional reactions toward patients. A psychometric evaluation of an extended version of the Feeling Word Checklist (FWC-58). Nord. J. Psychiat. 2003, 57, 45–53. [Google Scholar] [CrossRef]
- Dahl, H.-S.J.; Røssberg, J.I.; Bøgwald, K.-P.; Gabbard, G.O.; Høglend, P. Countertransference feelings in one year of individual therapy: An evaluation of the factor structure in the Feeling Word Checklist-58. Psychother. Res. 2012, 22, 12–25. [Google Scholar] [CrossRef]
- Datz, F.; Parth, K.; Rohm, C.; Madanoglu, S.; Seidman, C.; Löffler-Stastka, H. Dimensions of activity in countertransference and therapist reactions: Therapist reactions during sessions with depressed patients. Z. Für Psychosom. Med. Psychother. 2016, 62, 322–335. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.E. Therapeutic Action: A Guide to Psychoanalytic Therapy; Aronson: Rockville, MD, USA, 2000. [Google Scholar]
- Zittel, C.; Westen, D. The Countertransference Questionnaire; Departments of Psychology and Psychiatry and Behavioral Sciences, Emory University: Atlanta, GA, USA, 2003. [Google Scholar]
- Friedman, S.M.; Gelso, C.J. The development of the inventory of countertransference behavior. J. Clin. Psychol. 2000, 56, 1221–1235. [Google Scholar] [CrossRef]
- Brøsholen, P.; Ulberg, R.; Dahl, H.S.J.; Thorén, A. Therapists’ emotional responses in individual therapy with depressed adolescents: An evaluation of the data structure of the Feeling-Word Checklist—28. Int. J. Environ. Res. Public Health 2022, 19, 9496. [Google Scholar] [CrossRef] [PubMed]
- Ulberg, R.; Falkenberg, A.A.; Nærdal, T.B.; Johannessen, H.; Olsen, J.E.; Eide, T.K.; Hersoug, A.G.; Dahl, H.S.J. Countertransference feelings when treating teenagers. A psychometric evaluation of the Feeling Word Checklist—24. Am. J. Psychot. 2013, 67, 347–358. [Google Scholar] [CrossRef] [Green Version]
- Stiles, W.B. Measurement of the impact of psychotherapy sessions. J. Consult. Clin. Psychol. 1980, 48, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Betan, E.; Heim, A.K.; Conklin, C.Z.; Westen, D. Countertransference phenomena and personality pathology in clinical practice: An empirical investigation. Am. J. Psychiat. 2005, 162, 890–898. [Google Scholar] [CrossRef]
- Tanzilli, A.; Colli, A.; Del Corno, F.; Lingiardi, V. Factor structure, reliability, and validity of the Therapist Response Questionnaire. Personal. Disord. Theory Res. Treat. 2016, 7, 147–158. [Google Scholar] [CrossRef]
- Yaseen, Z.; Galynker, I.I.; Cohen, L.J.; Briggs, J. Clinicians’ conflicting emotional responses to high suicide-risk patients—Association with short-term suicide behaviors: A prospective pilot study. Compr. Psychiatry 2017, 76, 69–78. [Google Scholar] [CrossRef]
- Horvath, A.O.; Greenberg, L.S. Development and validation of the Working Alliance Inventory. J. Couns. Psycho. 1989, 36, 223–233. [Google Scholar] [CrossRef]
- Barzilay, S.; Yaseen, Z.S.; Hawes, M.; Gorman, B.; Altman, R.; Foster, A.; Apter, A.; Rosenfield, P.; Galynker, I. Emotional responses to suicidal patients: Factor structure, construct, and predictive validity of the Therapist Response Questionnaire-Suicide Form. Front. Psychiatry 2018, 9, 104. [Google Scholar] [CrossRef]
- Michaud, L.; Ligier, F.; Bourquin, C.; Corbeil, S.; Saraga, M.; Stiefel, F.; Séguin, M.; Turecki, G.; Richard-Devantoy, S. Differences and similarities in instant countertransference towards patients with suicidal ideation and personality disorders. J. Affect. Disord. 2020, 265, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Löffler-Stastka, H.; Sell, C.; Zimmermann, J.; Huber, D.; Klug, G. Is countertransference a valid source of clinical information? Investigating emotional responses to audiotaped psychotherapy sessions. B. Menninger. Clin. 2019, 83, 353–375. [Google Scholar] [CrossRef]
- Picardi, A.; Pallagrosi, M.; Fonzi, L.; Biondi, M. Psychopathological dimensions and the clinician’s subjective experience. Psychiat. Res. 2017, 258, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Moukaddam, N.; Andry, T.; Cao, J.; Moon, Y.M.; Tucci, V.; Shah, A.; Lomax, J.W. Instant countertransference affects assessment and treatment recommendations for depression in patients openly professing religious faith. Spiritual. Clin. Pract. 2019, 6, 100. [Google Scholar] [CrossRef]
- Bonelli, R.; Dew, R.E.; Koenig, H.G.; Rosmarin, D.H.; Vasegh, S. Religious and Spiritual Factors in Depression: Review and Integration of the Research. Depress. Res. Treat. 2012, 2012, 962860. [Google Scholar] [CrossRef] [PubMed]
- Pengpid, S.; Peltzer, K. Religiosity and Depression Among Community-Dwelling Older Adults in India: Results of a National Survey in 2017–2018. J. Relig. Health, online ahead of print. 2022. [Google Scholar] [CrossRef]
- Genova, F.; Gazzillo, F. Personality organization, personality styles, and the emotional reactions of treating clinicians. Psychodyn. Psychiatry 2018, 46, 357–392. [Google Scholar] [CrossRef] [PubMed]
- Hennissen, V.C.; Meganck, R.; Van Nieuwenhove, K.; Norman, U.A.; Loeys, T.; Desmet, M. Therapists’ responses toward dependent (anaclitic) and self-critical (introjective) depressed outpatients: A multilevel approach. Psychotherapy 2019, 56, 193–204. [Google Scholar] [CrossRef]
- Dahl, H.S.J.; Høglend, P.; Ulberg, R.; Amlo, S.; Gabbard, G.O.; Perry, J.C.; Christoph, P.C. Does therapists’ disengaged feelings influence the effect of transference work? A study on countertransference. Clin. Psychol. Psychot. 2017, 24, 462–474. [Google Scholar] [CrossRef]
- Tanzilli, A.; Majorana, M.; Fonzi, L.; Pallagrosi, M.; Picardi, A.; Coccanari de’ Fornari, M.A.; Biondi, M.; Lingiardi, V. Relational variables in short-term psychodynamic psychotherapy: An effectiveness study. RIPPO 2018, 21, 190–200. [Google Scholar] [CrossRef]
- Falkenström, F.; Holmqvist, R. Therapist in-session feelings predict change in depressive symptoms in interpersonal and brief relational psychotherapy. Psychother. Res. 2022, 32, 571–584. [Google Scholar] [CrossRef]
- Safran, J.D.; Muran, J.C. Negotiating the Therapeutic Alliance: A Relational Treatment Guide; Guilford Press: New York, NY, USA, 2000. [Google Scholar]
- Klerman, G.; Weissman, M.M.; Rounsaville, B.; Chevron, E. Interpersonal Psychotherapy of Depression; Basic Books: New York, NY, USA, 1984. [Google Scholar]
- Hatcher, R.L.; Gillaspy, J.A. Development and validation of a revised short version of the Working Alliance Inventory. Psychother. Res. 2006, 16, 12–25. [Google Scholar] [CrossRef]
- Hennissen, V.; Meganck, R.; Van Nieuwenhove, K.; Krivzov, J.; Dulsster, D.; Desmet, M. Countertransference processes in psychodynamic therapy with dependent (anaclitic) depressed patients: A qualitative study using supervision data. Psychodyn. Psychiatry 2020, 48, 163–193. [Google Scholar] [CrossRef]
- Michaud, L.; Greenway, K.T.; Corbeil, S.; Bourquin, C.; Richard-Devantoy, S. Countertransference towards suicidal patients: A systematic review. Curr. Psychol. 2021, 1–15. [Google Scholar] [CrossRef]
- Markin, R.D.; McCarthy, K.S.; Barber, J.P. Transference, countertransference, emotional expression, and session quality over the course of supportive expressive therapy: The raters’ perspective. Psychother. Res. 2013, 23, 152–168. [Google Scholar] [CrossRef]
- Whyte, C.R.; Constantopoulos, C.; Bevans, H.G. Types of countertransference identified by Q-analysis. Brit. J. Med. Psychol. 1982, 2, 187–201. [Google Scholar] [CrossRef]
- Kernberg, O.F. The four basic components of psychoanalytic technique and derived psychoanalytic psychotherapies. World Psychiatry 2016, 15, 287–288. [Google Scholar] [CrossRef] [Green Version]
- Laverdière, O.; Beaulieu-Tremblay, T.; Descôteaux, J.; Simard, V. Countertransference and Psychological Assessment: Direct and Indirect Exposure. J. Nerv. Ment. Dis. 2018, 206, 455–460. [Google Scholar] [CrossRef]
- Prasko, J.; Ociskova, M.; Vanek, J.; Burkauskas, J.; Slepecky, M.; Bite, I.; Krone, I.; Sollar, T.; Juskiene, A. Managing Transference and Countertransference in Cognitive Behavioral Supervision: Theoretical Framework and Clinical Application. Psychol. Res. Behav. Manag. 2022, 15, 2129. [Google Scholar] [CrossRef]
- Heinonen, E.; Nissen-Lie, H.A. The professional and personal characteristics of effective psychotherapists: A systematic review. Psychot. Res. 2020, 30, 417–432. [Google Scholar] [CrossRef]
- Clements-Hickman, A.L.; Reese, R.J. The person of the therapist: Therapists’ personal characteristics as predictors of alliance and treatment outcomes. Psychot. Res. online ahead of print. 2022. [Google Scholar] [CrossRef]
- Castonguay, L.G.; Hill, C.E. (Eds.) How and Why Are Some Therapists Better than Others?: Understanding Therapist Effects; American Psychological Association: Washington, DC, USA, 2017. [Google Scholar] [CrossRef]
- Hayes, J.A.; Riker, J.R.; Ingram, K.M. Countertransference behavior and management in brief counseling: A field study. Psychot. Res. 1997, 7, 145–153. [Google Scholar] [CrossRef]
- Colli, A.; Ferri, M. Patient personality and therapist countertransference. Curr. Opin. Psychiatry 2015, 28, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Stefana, A.; Langfus, J.A.; Vieta, E.; Fusar-Poli, P.; Youngstrom, E.A. Development and initial validation of the Relation In-Session Questionnaire (RISQ) and the Assessing Risk of Relationship Rupture (AR3) scales. PsyArXiv 2022, preprint. [Google Scholar] [CrossRef]
- Gelso, C. A tripartite model of the therapeutic relationship: Theory, research, and practice. Psychot. Res. 2014, 24, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Stefana, A.; Fusar-Poli, P.; D’Imperio, D.; Choplin, E.; Dakanalis, A.; Vieta, E. Mapping the psychoanalytic literature on bipolar disorder: A scoping review of journal articles. Braz. J. Psychiatry, online ahead of print. 2022. [Google Scholar] [CrossRef]
- Stefana, A.; Youngstrom, E.A.; Vieta, E. Empirical support for the use and further study of the countertransference construct in the clinical care of patients with bipolar disorder. Bipolar. Disord. 2022, 24, 84–85. [Google Scholar] [CrossRef] [PubMed]
- Stefana, A.; D’Imperio, D.; Dakanalis, A.; Vieta, E.; Fusar-Poli, P.; Youngstrom, E.A. Probing the impact of psychoanalytic therapy for bipolar disorders: A scoping review. Int. Forum. Psychoanal. online ahead of print. 2022. [Google Scholar] [CrossRef]
- De Page, L.; Boulanger, M.; De Villers, B.; Di Virgilio, P.; Pham, T.; Saloppé, X.; Thiry, B. Countertransference in forensic inpatient settings: An empirical examination of therapist responses to patients with psychotic disorders. J. Forensic. Nurs. 2021, 17, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.; Beazley, P.I. Judging personality disorder: A systematic review of clinician attitudes and responses to borderline personality disorder. J. Psychiatr. Pract. 2022, 28, 275–293. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Measure Name | Description | Items/Factors/Subscales |
|---|---|---|
| Psychotherapy Process Q-set (PQS) Jones [82] | Q sort 100 items It is applied to recorded single session. Clinical judges sort items into nine categories from 1 (least characteristic) to 9 (most characteristic). | The items are divided into three categories that describe or attempt to capture the following areas:
|
| Countertransference Behavior Inventory (CBI) Friedman & Gelso [84] | Observational rating 21-items Designed for supervisors to assess perceived countertransference behavior during therapy sessions, rating reactions to a particular patient in a given therapy session. 5-point Likert scale ranging from 1 (to little or no extent) to 5 (to a great extent). | Exploratory factor analysis identified two factors:
|
| Assessment of Clinician’s Subjective Experience (ACSE) Pallagrosi et al. [76] | Clinician self-report 46 items measuring subjective experience during clinical interaction with patients. Each item refers to a specific phase of the visit: “at the beginning”, “in the course of” or “at the end”. 5-point Likert scale ranging from 0 (not at all/never) to 4 (extremely/always). | Principal component analysis identified five subscales.
|
| Experience and Attitude Scale (EAS) Brody & Faber [45] | Clinician self-report 25 items Assesses the overall experience in psychotherapy (15 items) and attitudes towards their own emotional reactions in therapy (10 items). Clinicians rate the intensity or frequency of their reactions. 5-point Likert scale ranging from 1 (not at all/hardly ever) to 5 (very much so/very often). | The authors used only the subscale on the therapist’s attitudes toward their emotional reactions. Items were not summed, analyzing all 10 items separately. The aspects assessed by the items are as follows:
|
| Feeling Word Checklist (FWC) Røssberg et al. [79] | Clinician self-report 58 items Therapists rate degree they have experienced different feelings toward the patient. 5-point Likert scale ranging from 0 (nothing) to 4 (very much). Note that some shorter versions (28- and 24-item versions) use a 4-point Likert scale ranging from 0 (nothing/not at all) to 3 (very much). | Principal component analysis identified four subscales:
|
| Impact Message Inventory (IMI) Kiesler [73] | Clinician self-report 90 items Measures distinctive internal reactions (referred to as impact messages) that the therapist experiences to the full range of interpersonal behaviors indexed along the circumference of the interpersonal circle. 4-point Likert scale ranging from 1 (not at all) to 4 (very similar). | Items are clustered into four subscales:
|
| Stress Appraisal Scale (SAS) Carpenter & Suhr [74] | Clinician self-report 36 items Investigates the therapist’s feelings about entering a therapeutic relationship with a patient listened to in an audiotaped interview. 4-point Likert scale ranging from 1 (very untrue of me) to 4 (very true of me) by rating how accurate each statement is of the therapist’s reactions. | Items are grouped into four subscales, which in turn are clustered into three primary categories.
|
| Therapist Positive Feeling Index (TPFI) Stiles [87] | Clinician self-report 6 items The TPFI is part of the Session Evaluation Questionnaire. It assesses the emotional expression of the therapist. The original version of this subscale begins with the stem ‘‘Right now I feel,’’ but was changed in the included study to, ‘‘To what extent did the therapist express feelings of __ during the session.’’ This stem is followed by the five bipolar adjectives that are rated on a continuum from 1 to 7 by a coder. | A total score is calculated using the mean rating on the following bipolar adjectives.
|
| Therapist Response Questionnaire (TRQ) Zittel Conklin & Westen [83] | Clinician self-report 79 items Assesses CT patterns in a psychotherapeutic setting on a wide range of cognitive, affective and behavioral responses therapists have to their patients. 5-point Likert scale ranging from 1 (not true) to 5 (very true). | The English version revealed an eight-factor structure [88]:
|
| Therapist Response Questionnaire—Suicide Form (TRQ-SF) Yaseen et al. [90] | Clinician self-report 10 items Assesses clinicians’ responses to suicidal patients after a single encounter. It includes five items derived from the TRQ [83], two items from the WAI [91] and three items developed de novo. 5-point Likert scale ranging from 0 (not at all) to 4 (extremely). | Three subscales have been identified and validated by Barzilay et al. [92] and adopted by Michaud et al. [93]:
|
| Vignettes Rating Scale (VRS) Brody & Faber [45] | Clinician self-report 20 items Assesses the extent to which the clinician imagined that actually working with the patient described in a clinical vignette would generate a variety of feelings and reactions. 5-point Likert scale, with response options ranging from 1 (much less than usual) to 5 (much more than usual). |
Three different aspects of countertransference:
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefana, A.; Fusar-Poli, P.; Gnisci, C.; Vieta, E.; Youngstrom, E.A. Clinicians’ Emotional Reactions toward Patients with Depressive Symptoms in Mood Disorders: A Narrative Scoping Review of Empirical Research. Int. J. Environ. Res. Public Health 2022, 19, 15403. https://doi.org/10.3390/ijerph192215403
Stefana A, Fusar-Poli P, Gnisci C, Vieta E, Youngstrom EA. Clinicians’ Emotional Reactions toward Patients with Depressive Symptoms in Mood Disorders: A Narrative Scoping Review of Empirical Research. International Journal of Environmental Research and Public Health. 2022; 19(22):15403. https://doi.org/10.3390/ijerph192215403
Chicago/Turabian StyleStefana, Alberto, Paolo Fusar-Poli, Cristina Gnisci, Eduard Vieta, and Eric A. Youngstrom. 2022. "Clinicians’ Emotional Reactions toward Patients with Depressive Symptoms in Mood Disorders: A Narrative Scoping Review of Empirical Research" International Journal of Environmental Research and Public Health 19, no. 22: 15403. https://doi.org/10.3390/ijerph192215403