
Characteristics, Components, and Efficacy of Telerehabilitation Approaches for People with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Interventions
2.2.1. Telerehabilitation
2.2.2. Comparators
2.3. Information Sources for Study Selection
2.4. Selection and Data Collection Process
2.5. Study Risk of Bias Assessment
2.6. Meta-Analysis and Narrative Synthesis
3. Results
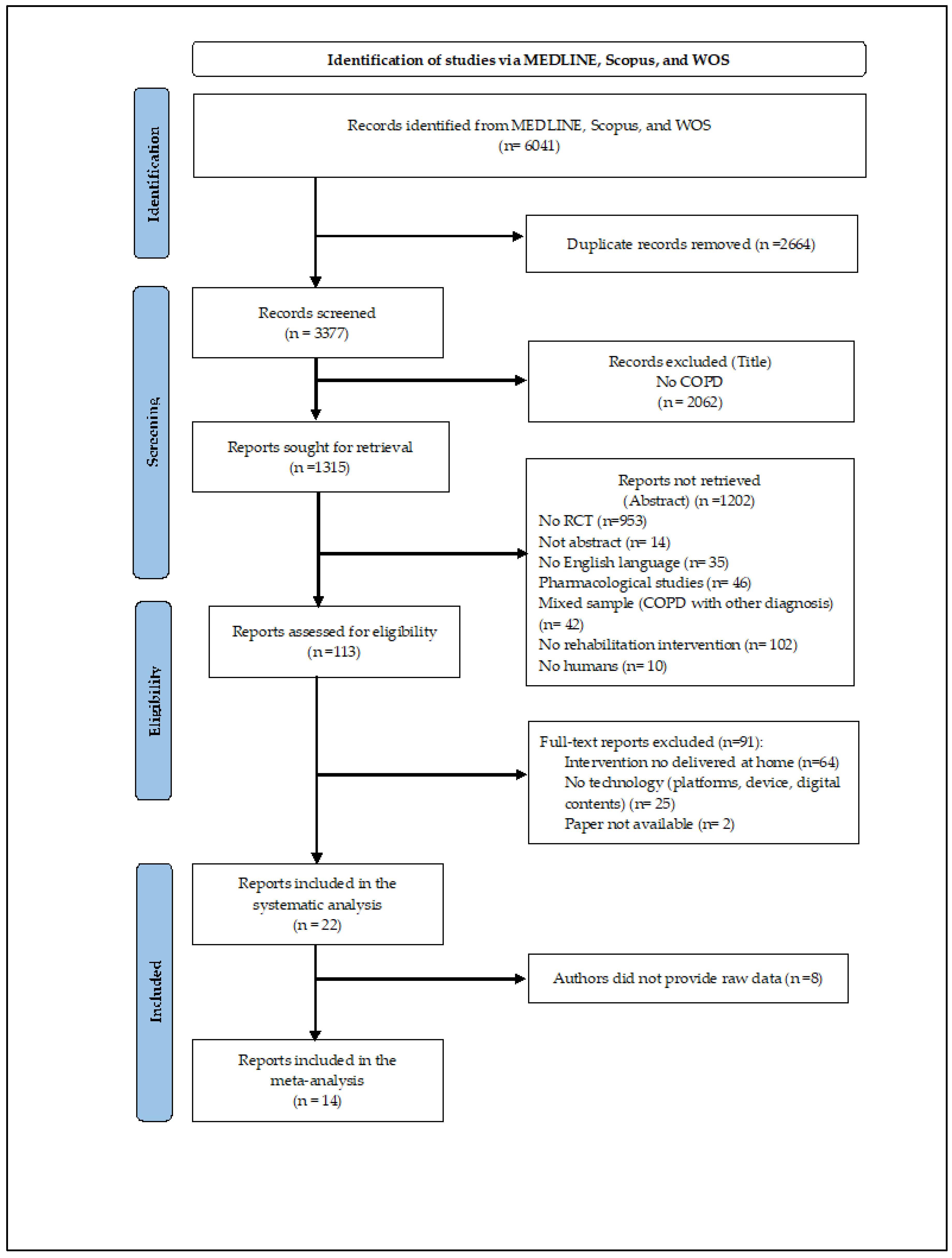
3.1. Study Selection
3.2. Participants
3.3. TR Interventions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | Testex | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Eligibility | Randomization | Allocation | Groups Similarity at Baseline | Assessor Blinding | Outcome Measures | Intention-to-Treat | Between-Group Statistical Comparison | Point Measures and Measures of Variability | Activity Monitoring in the Control Group | Exercise Intensity Remained Constant | Exercise Volume and Energy Expenditure | ||
| Ref. [36] | 1 | 1 | 0 | 1 | 0 | 2 | 0 | 2 | 1 | 0 | 1 | 0 | 9 |
| Ref. [26] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 1 | 1 | 12 |
| Ref. [37] | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 7 |
| Ref. [34] | 1 | 1 | 1 | 1 | 0 | 3 | 1 | 2 | 0 | 0 | 1 | 1 | 12 |
| Ref. [38] | 1 | 1 | 1 | 1 | 0 | 3 | 1 | 2 | 1 | 0 | 1 | 1 | 13 |
| Ref. [40] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 2 | 1 | 0 | 1 | 1 | 11 |
| Ref. [32] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 2 | 1 | 0 | 1 | 1 | 11 |
| Ref. [25] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 2 | 1 | 0 | 1 | 1 | 10 |
| Ref. [24] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 7 |
| Ref. [27] | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 1 | 1 | 11 |
| Ref. [28] | 1 | 1 | 1 | 1 | 1 | 2 | 0 | 2 | 1 | 0 | 1 | 1 | 12 |
| Ref. [39] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 6 |
| Ref. [31] | 1 | 1 | 1 | 1 | 1 | 3 | 0 | 0 | 1 | 0 | 0 | 1 | 10 |
| Ref. [22] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 2 | 0 | 0 | 1 | 0 | 7 |
| Ref. [41] | 1 | 1 | 1 | 1 | 0 | 3 | 1 | 2 | 1 | 0 | 1 | 1 | 13 |
| Ref. [29] | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 1 | 1 | 0 | 1 | 1 | 6 |
| Ref. [23] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 2 | 0 | 0 | 1 | 1 | 6 |
| Ref. [33] | 0 | 1 | 1 | 1 | 1 | 3 | 1 | 2 | 1 | 0 | 1 | 1 | 13 |
| Ref. [8] | 1 | 1 | 1 | 1 | 0 | 3 | 0 | 1 | 0 | 0 | 1 | 0 | 9 |
| Ref. [21] | 1 | 1 | 0 | 0 | 1 | 2 | 0 | 2 | 1 | 0 | 1 | 1 | 10 |
| Ref. [35] | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 5 |
| Ref. [30] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 2 | 1 | 0 | 1 | 1 | 11 |
| Study | Group | Subjects [N] | Sex [N Male; Female] | Age(y) [M; SD] | FEV1 L/%pred [M; SD] | FVC1 L/%pred [M; SD] |
|---|---|---|---|---|---|---|
| Ref. [36] | TR | 100 | 35; 65 | 69.43; 7.38 | -/39.55; 15.13 | - |
| CI | 100 | 32; 68 | 68.87; 5.33 | -/38.65; 13.68 | - | |
| Ref. [26] | TR | 64 | 41; 23 | 69.10; 7.90 | -/58.00; 23.60 | -/88.40; 22.00 |
| CI | 26 | 18; 8 | 71.40; 8.60 | -/60.50; 20.10 | -/83.20; 21.20 | |
| Ref. [37] | TR | 27 | 16; 11 | 67.40; 10.20 | -/36.10; 14.10 | -/67.40; 19.90 |
| CI | 27 | 15; 12 | 72.50; 7.40 | -/32.80; 8.50 | -/70.20; 17.00 | |
| Ref. [34] | TR | 171 | 111; 60 | 66.00; 8.00 | -/55.00; 20.00 | - |
| NI | 172 | 108; 64 | 67.00; 8.00 | -/57.00; 21.00 | - | |
| Ref. [38] | TR | 46 | 30; 16 | 62.30; 8.20 | -/42.39; 13.49 | -/73.38; 15.88 |
| CI | 48 | 33; 15 | 63.00; 6.60 | -/42.93; 13.78 | -/74.50; 15.47 | |
| Ref. [40] | TR | 67 | 32; 35 | 68.40; 8.70 | -/32.60; 10.30 | - |
| CI | 67 | 28; 39 | 68.20; 9.40 | -/33.70; 8.40 | - | |
| Ref. [32] | TR | 80 | 48; 32 | 69.00; 13.00 | -/52.00; 19.00 | -/78.00; 17.00 |
| CI | 86 | 51; 35 | 69.00; 10.00 | -/49.00; 19.00 | -/79.00; 22.00 | |
| Ref. [25] | TR | 53 | 44; 9 | 70.92; 6.38 | - | - |
| CI | 53 | 43; 10 | 71.83; 7.60 | - | - | |
| Ref. [24] | TR | 12 | 10; 2 | 74.00; 8.00 | -/58.00; 23.20 | 2.80; 0.70/- |
| CI | 15 | 14; 1 | 75.00; 9.00 | -/60.60; 20.80 | 3.20; 0.70/- | |
| Ref. [27] | TR | 29 | 17; 12 | 68.00; 9.00 | -/90.00; 8.00 | -/104.00; 8.00 |
| NI | 29 | 17; 12 | 67.00; 10.00 | -/92.00; 7.00 | -/104.00; 24.00 | |
| Ref. [28] | TR | 10 | 4; 6 | 73.00; 4.00 | 1.00; 0.30/- | - |
| NI | 10 | 3; 7 | 67.00; 8.00 | 0.90; 0.20/- | - | |
| Ref. [39] | TR | 50 | 41; 9 | 65.90; 8.90 | -/48.70; 11.20 | 0.00; 11.20/- |
| CI1 | 50 | 38; 12 | 65.60; 8.80 | -/50.40; 11.40 | -/50.30; 11.40 | |
| CI2 | 50 | 37; 13 | 64.80; 9.30 | -/47.40; 11.50 | -/48.40; 10.30 | |
| Ref. [31] | TR | 29 | 21; 8 | 69.40; 3.30 | -/49.20; 0.50 | 1.70; 0.00/- |
| NI | 28 | 23; 5 | 68.80; 1.40 | -/49.80; 0.70 | 1.80; 0.00/- | |
| Ref. [22] | TR | 33 | 27; 6 | 66.40; 9.50 | -/47.50; 23.30 | -/68.70; 30.20 |
| CI | 23 | 19; 4 | 71.30; 6.70 | -/51.50; 23.90 | -/79.10; 30.00 | |
| NI | 29 | 19; 10 | 70.80; 8.70 | -/41.40; 18.40 | -/69.90; 28.00 | |
| Ref. [41] | TR | 22 | 19; 3 | 70.40; 9.40 | -/61.00; 18.70 | - |
| NI | 20 | 14; 6 | 65.06; 11.10 | -/69.40; 24.00 | - | |
| Ref. [29] | TR | 10 | 9; 1 | 69.20; 5.41 | -/64.60; 11.97 | - |
| NI | 10 | 10; 0 | 67.40; 6.60 | -/60.40; 20.14 | - | |
| Ref. [23] | TR | 17 | 7; 10 | 65.00; - | -/61.40 | - |
| CI | 19 | 3; 16 | 64.00; - | -/58.00 | - | |
| Ref. [33] | TR | 19 | 12; 7 | 73.00; 8.00 | -/60.00; 23.00 | -/89.00; 25.00 |
| NI | 17 | 6; 11 | 75.00; 9.00 | -/68.00; 19.00 | -/98.00; 17.00 | |
| Ref. [8] | TR | 47 | 44; 3 | 66.90; 9.60 | -/49.60; 21.90 | -/80.70; 20.20 |
| CI | 50 | 38; 12 | 66.70; 7.30 | -/51.80; 17.30 | -/78.40; 18.40 | |
| NI | 50 | 37; 13 | 64.00; 8.00 | -/51.70; 21.00 | -/80.00; 20.30 | |
| Ref. [21] | TR | 84 | 42; 42 | 62.00; 9.00 | -/59.00; 20.00 | -/101.00; 20.00 |
| NI | 73 | 37; 36 | 63.00; 8.00 | -/53.00; 15.00 | -/99.00; 19.00 | |
| Ref. [35] | TR | 55 | 21; 34 | 69.30; 7.80 | 0.40; 1.20/- | 0.50; 0.20/- |
| NI | 65 | 36; 29 | 71.80; 8.10 | 0.30; 0.10/- | 0.50; 0.20/- | |
| Ref. [30] | TR | 23 | - | 67.50; 6.20 | -/46.70; 13.50 | 2.20; 0.70/- |
| CI1 | 23 | - | 68.30; 7.00 | -/42.60; 12.00 | 2.10; 0.80/- | |
| CI2 | 23 | - | 67.20; 7.30 | -/47.20; 12.40 | 2.30; 0.60/- | |
| CI3 | 23 | - | 69.40; 6.40 | -/48.20; 15.00 | 2.30; 0.80/- |
| Study | FITT Descriptors | TR Approach | Technology | |||
|---|---|---|---|---|---|---|
| Model * | Monitoring/Assessment | Decision | Feedback | |||
| Ref. [36] | Frequency: 10–20 sessions/W × 12 W Intensity: - Time: 25–30 min Type: I, M (educational + Banduanjin exercise training) | A | Y | Y | Online | Platform: WeChat Device: mobile phone + PC Digital content |
| Ref. [26] | Frequency: 2–5 sessions/W × 6 W Intensity: increment of session length every W Time: - Type: I, M (educational + aerobic exercise training) | A | Y | Y | Online | Platform: My COPD Digital content |
| Ref. [37] | Frequency: 3–5 sessions/W × 8 W Intensity: - Time: - Type: I, U (aerobic/anaerobic exercise training) | A | Y | Y | Online | Platform: Virtual Autonomous Physiotherapist Agent platform Device: tablet/pc + pulsometer + biometric sensor Digital content |
| Ref. [34] | Frequency: 12 W Intensity: - Time: - Type: I, U (aerobic exercise training) | S | Y | Y | Offline | Platform: Fitbug Air coaching platform Device: step counter Digital content |
| Ref. [38] | Frequency: 3 sessions/W × 8 W Intensity: - Time: 120 min Type: I, M (educational + aerobic/breathing/weightlifting exercise training) | A | Y | Y | Online | Platform: TelePR platform Device: mobile phone + pulsometer Digital content |
| Ref. [40] | Frequency: 3 sessions/W × 10 W Intensity: Borg (score 4–7) + 40–80% of one repetition maximum (8–25 repetitions) Time: 35 min Type: G, M (educational + endurance exercise training) | S | Y | Y | Online | Device: videoconference system + touchscreen |
| Ref. [32] | Frequency: 2 sessions/W × 8 W Intensity: - Time: 30 min Type: I, M (Motivational + aerobic/strength/endurance exercise training) | A | Y | Y | Online | Device: pedometer + telephone |
| Ref. [25] | Frequency: 12 W Intensity: heart rate + conscious exertion score Time: 25–30 min Type: I, M (educational+ inspiratory muscles exercise training) | A | Y | Y | Online | Platform: Pulmonary Internet Explorer Rehabilitation platform + WeChat account Device: mobile phones + PC Digital content |
| Ref. [24] | Frequency: 7 sessions/W × 52 W Intensity: 30–40% maximal inspiratory muscle forces Time: - Type: I, M (educational+ aerobic/inspiratory muscles exercise training) | A | N | N | Offline | Device: pedometer fitted with actigraph |
| Ref. [27] | Frequency: 5 sessions/W × 8 W Intensity: Borg Time: 30 min Type: I, M (self-management + endurance exercise training) | A | Y | Y | Online | Device: pedometer + mobile phones |
| Ref. [28] | Frequency: 21 sessions/W × 8 W Intensity: 40–50% Pi max Time: - Type: I, U (inspiratory muscles exercise training) | A | Y | Y | No | Device: POWERbreathe KH2 |
| Ref. [39] | Frequency: 2 sessions/W × 8 W Intensity: - Time: - Type: I, U (exercise training) | A | Y | Y | Offline | Platform: WeChat platform Device: mobile phones Digital content |
| Ref. [31] | Frequency: 16 W Intensity: - Time: - Type: I, U (inspiratory muscles exercise training) | A | Y | N | Offline | Platform: Dyspnea breathing program website Digital content |
| Ref. [22] | Frequency: 3 sessions/W × 12 W Intensity: 60–80% of maximal heart rate on 6 MWT Time: - Type: I, U (aerobic/strength exercise training) | A | Y | Y | Offline | Device: Heart monitor |
| Ref. [41] | Frequency: 1 session/W × 24 W Intensity: - Time: 60 min Type: G, M (educational + aerobic/stretching exercise training) | A | Y | Y | Online | Platform: self-management program Device: pedometer + smartphone Digital content |
| Ref. [29] | Frequency: 3 sessions/W × 8 W Intensity: Borg + no more than 10 repetitions for endurance exercises Time: 65 min Type: I, M (self-management + aerobic/endurance exercise training) | A | Y | Y | Online | Digital content |
| Ref. [23] | Frequency: 14 sessions/W × 12 W Intensity: Borg Time: - Type: I, U (inspiratory muscles exercise training) | A | Y | Y | Online | Device: mechanical threshold leadings breathing trainer + web-based SurveyXactn software |
| Ref. [33] | Frequency: 3 sessions/W × 8 W Intensity: Borg Time: 60 min Type: I, U (aerobic/strength exercise training) | S | Y | Y | Online | Device: PC with in-built camera + lower limb cycle ergometer + finger-tip pulse oximeter + real-time videoconferencing system |
| Ref. [8] | Frequency: 5 sessions/W × 52 W Intensity: - Time: 60 min Type: I, M (psychological support + self-management + breathing exercise training) | A | Y | Y | Online | Platform: TELECARE platform Device: multimodal apparatus wireless fitted with Bluetooth technology + tablet |
| Ref. [21] | Frequency: 7 sessions/W × 26 W Intensity: set by the website Time: - Type: I, U (aerobic exercise training) | A | Y | Y | Offline | Platform: website Device: embedded accelerometer in the smartphone |
| Ref. [35] | Frequency: - Intensity: - Time: - Type: I, M (educational + self-management + inspiratory muscles exercise training) | A | Y | N | Online | Platform: web platform Digital content |
| Ref. [30] | Frequency: 7 sessions/W × 8 W Intensity: set by the website Time: 50 min Type: I, U (aerobic exercise training) | A | Y | Y | Offline | Device: threshold inspiratory trainer + threshold expiratory trainer with monitoring device |
3.4. TR Approach
3.5. TR Technology
3.6. TR Adherence and Safety
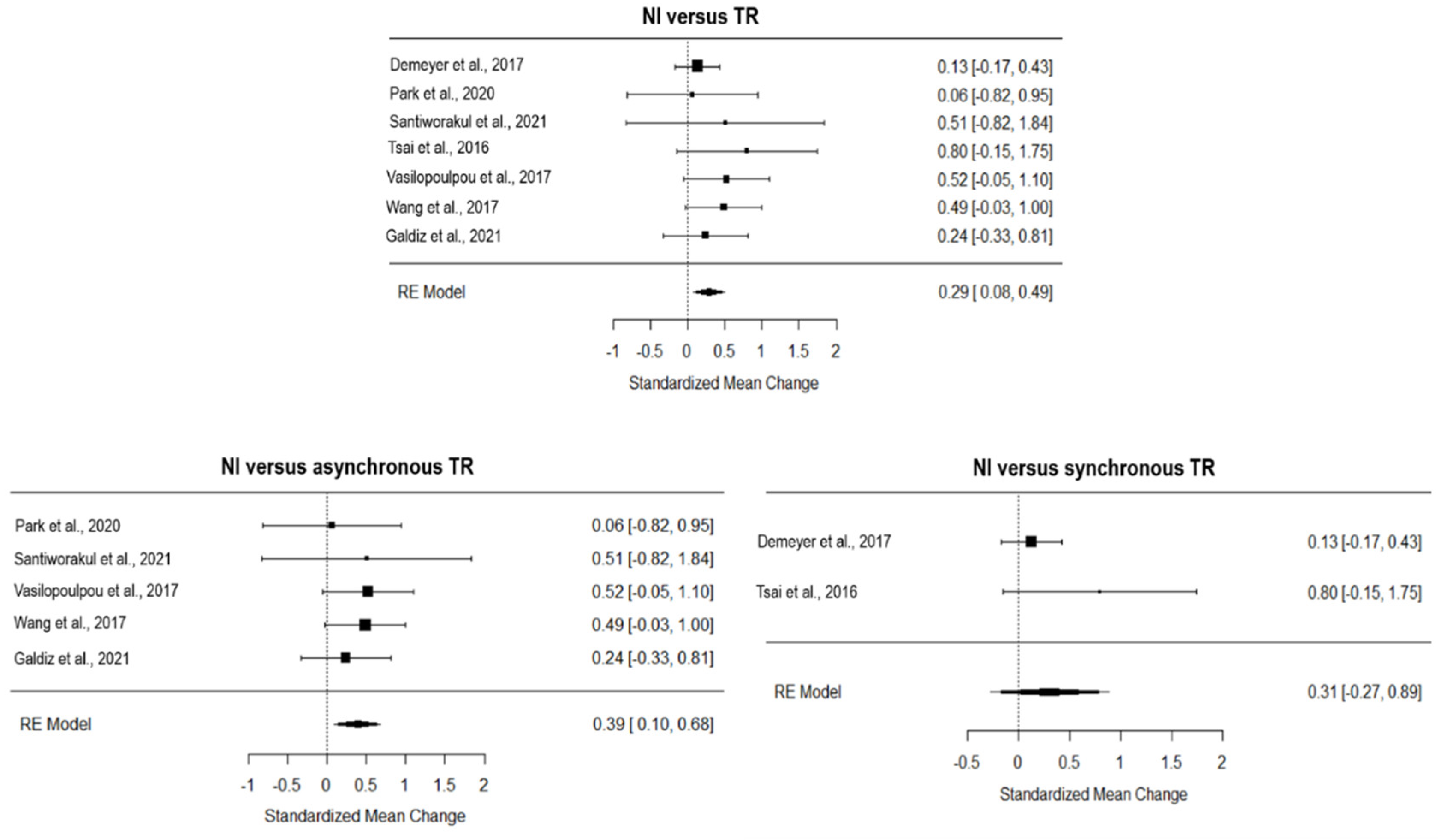
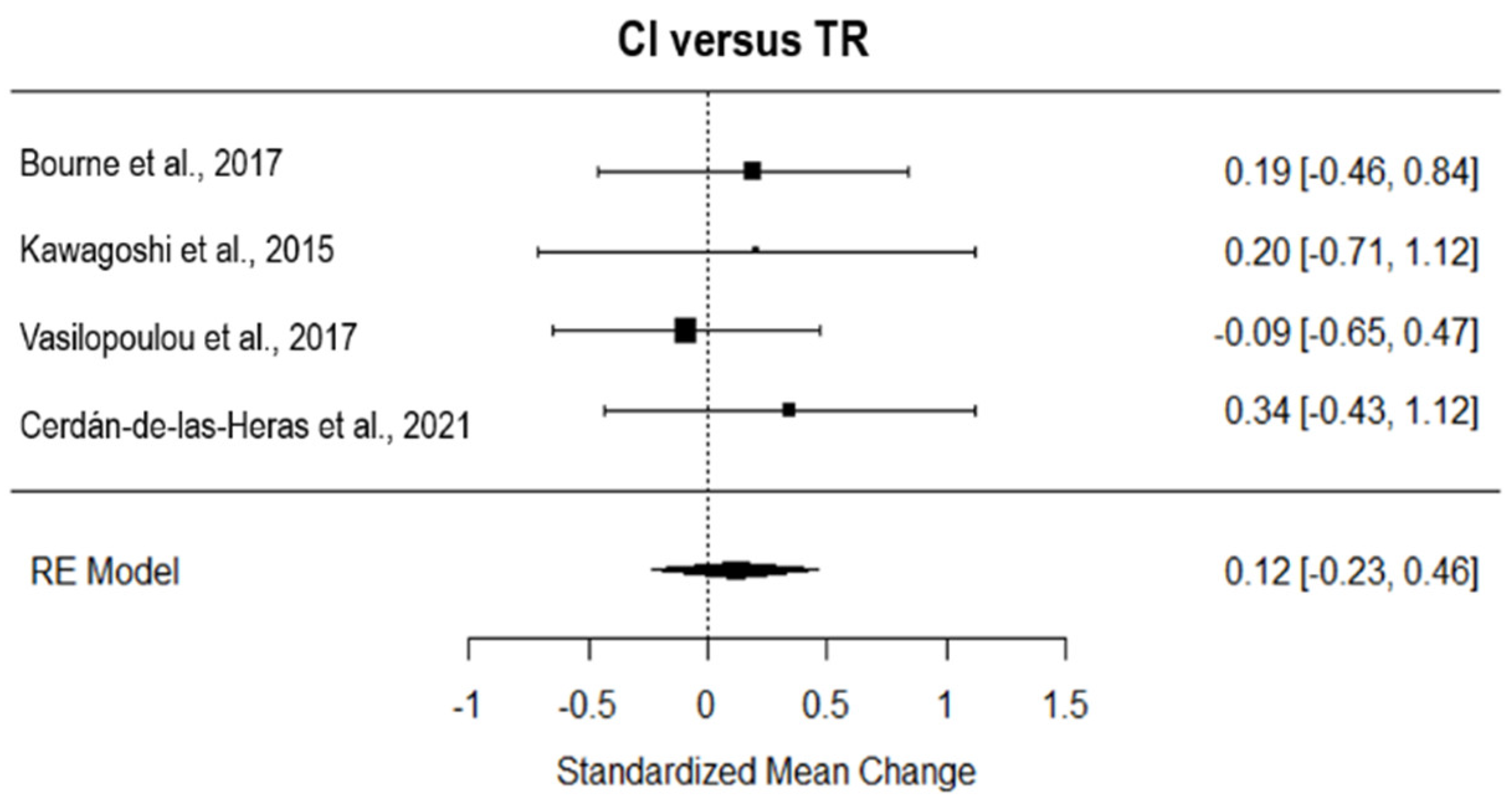
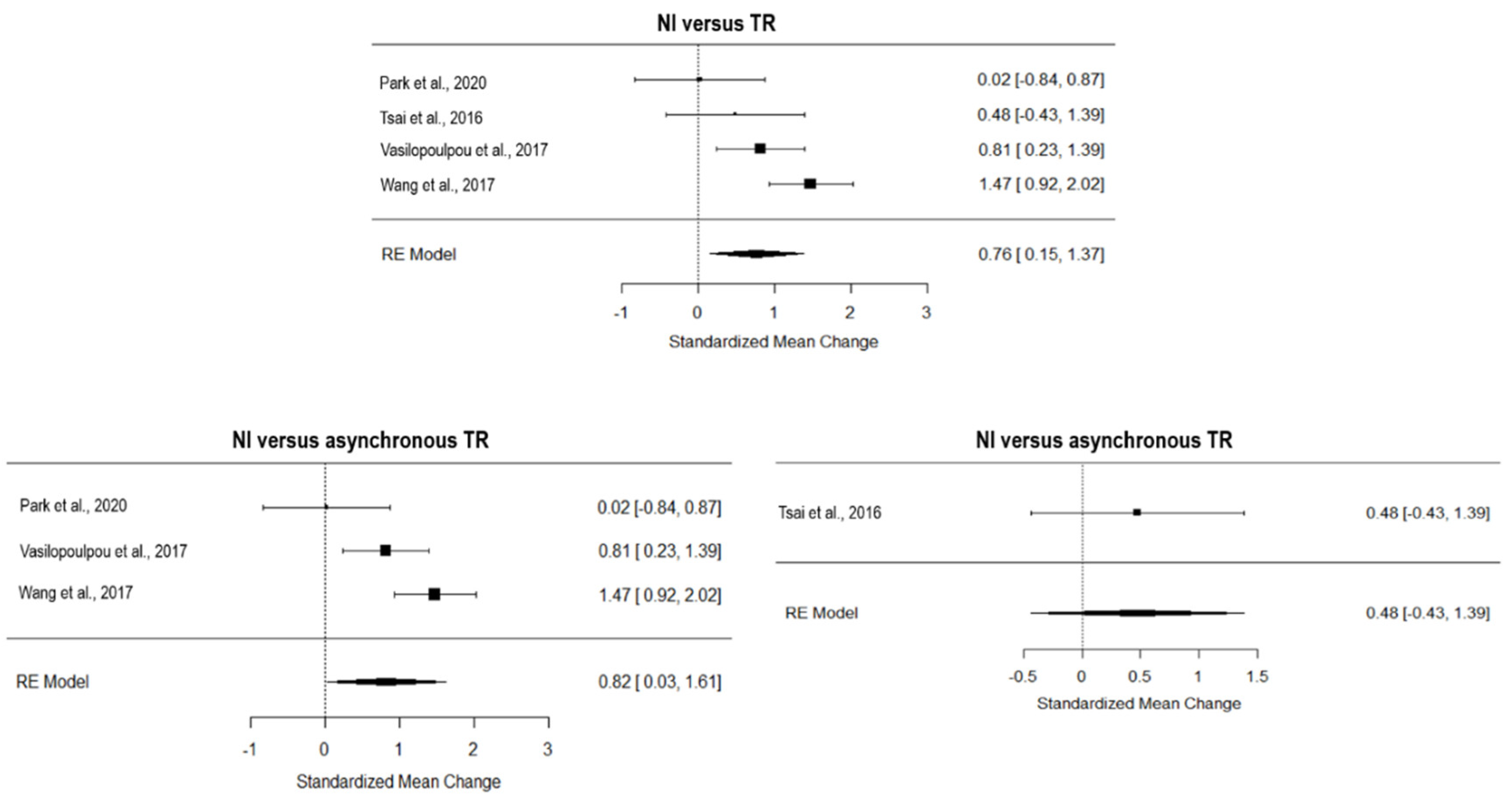
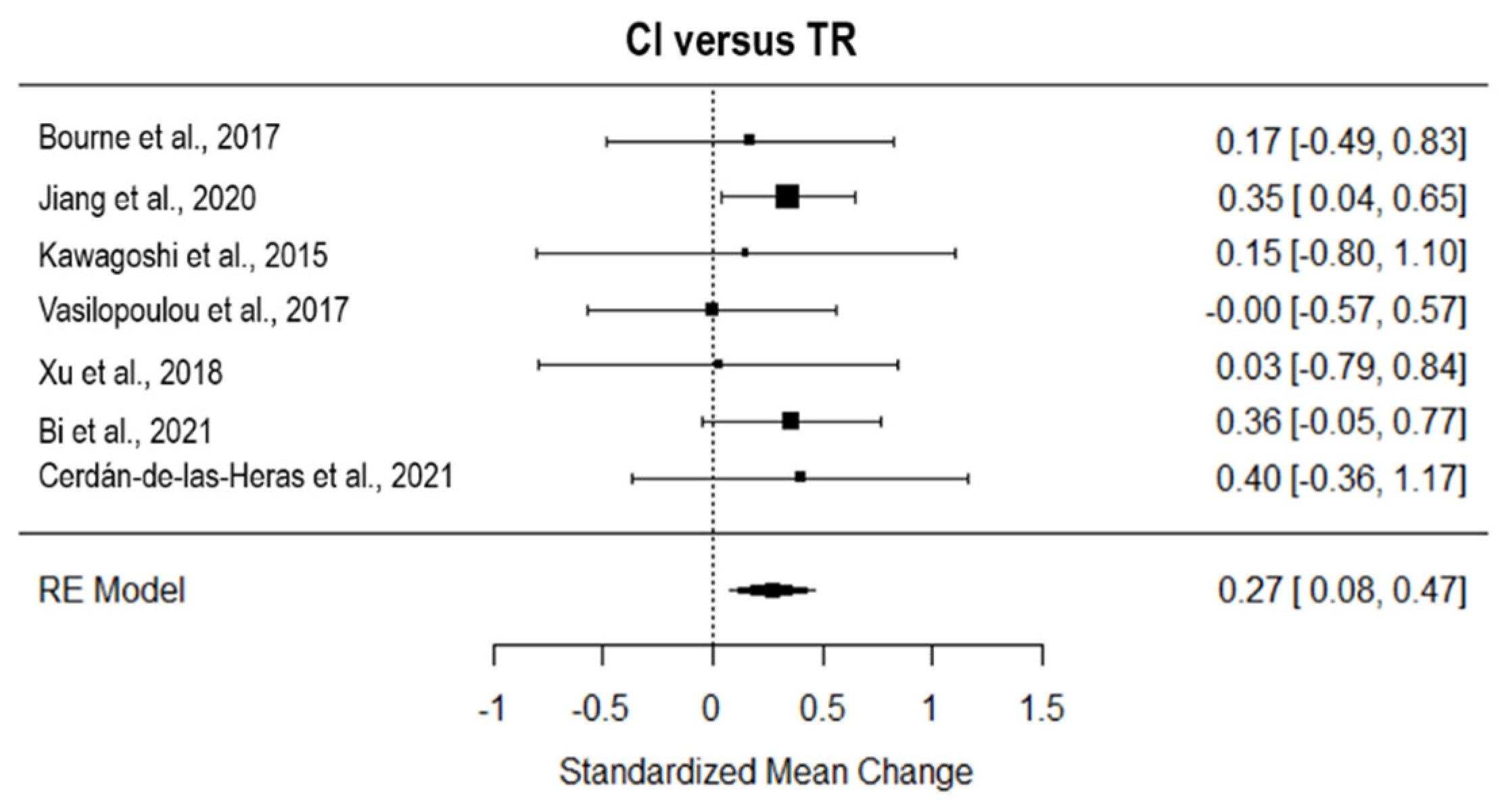
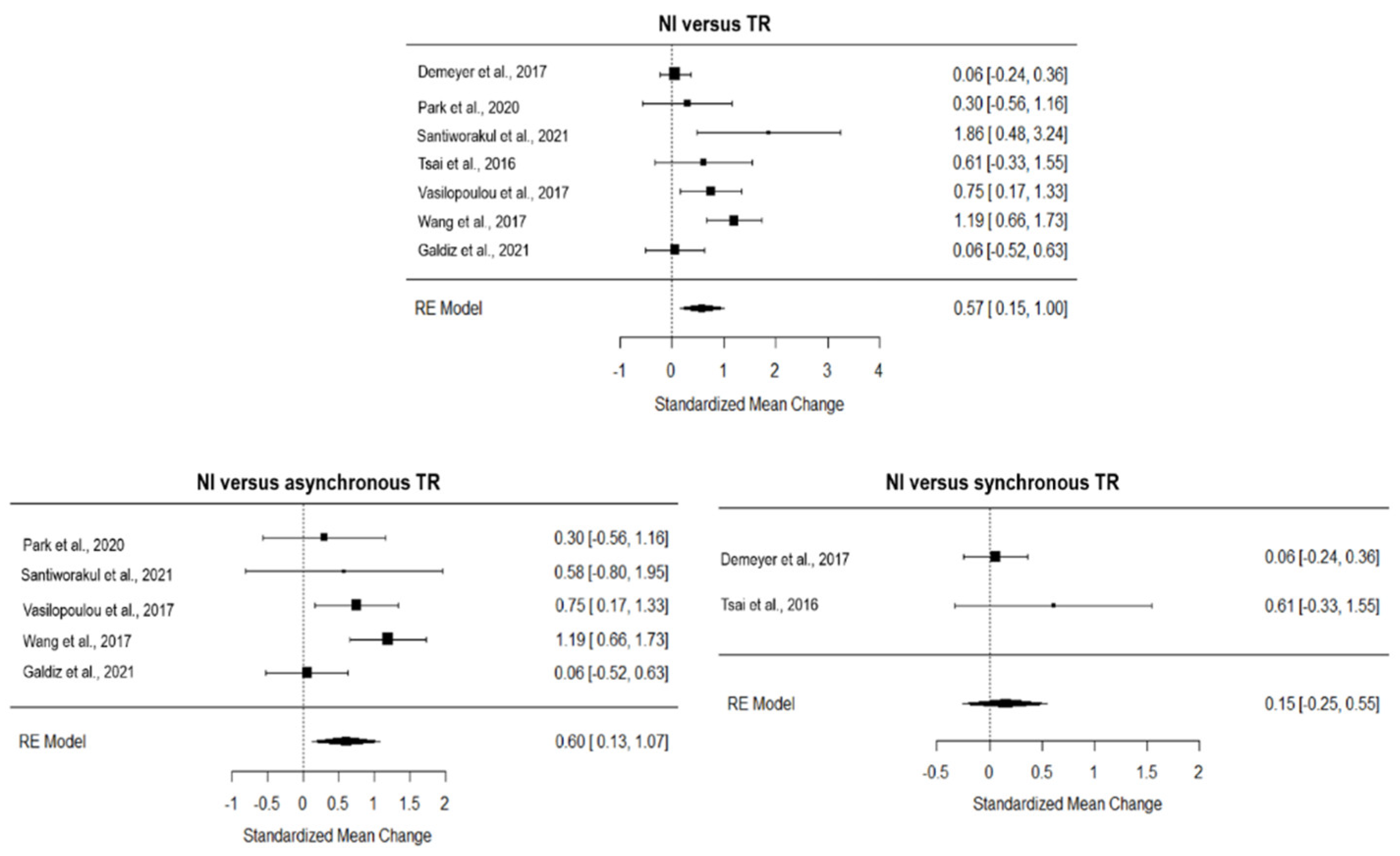
3.7. Efficacy at the End of Rehabilitation
3.8. Dyspnoea
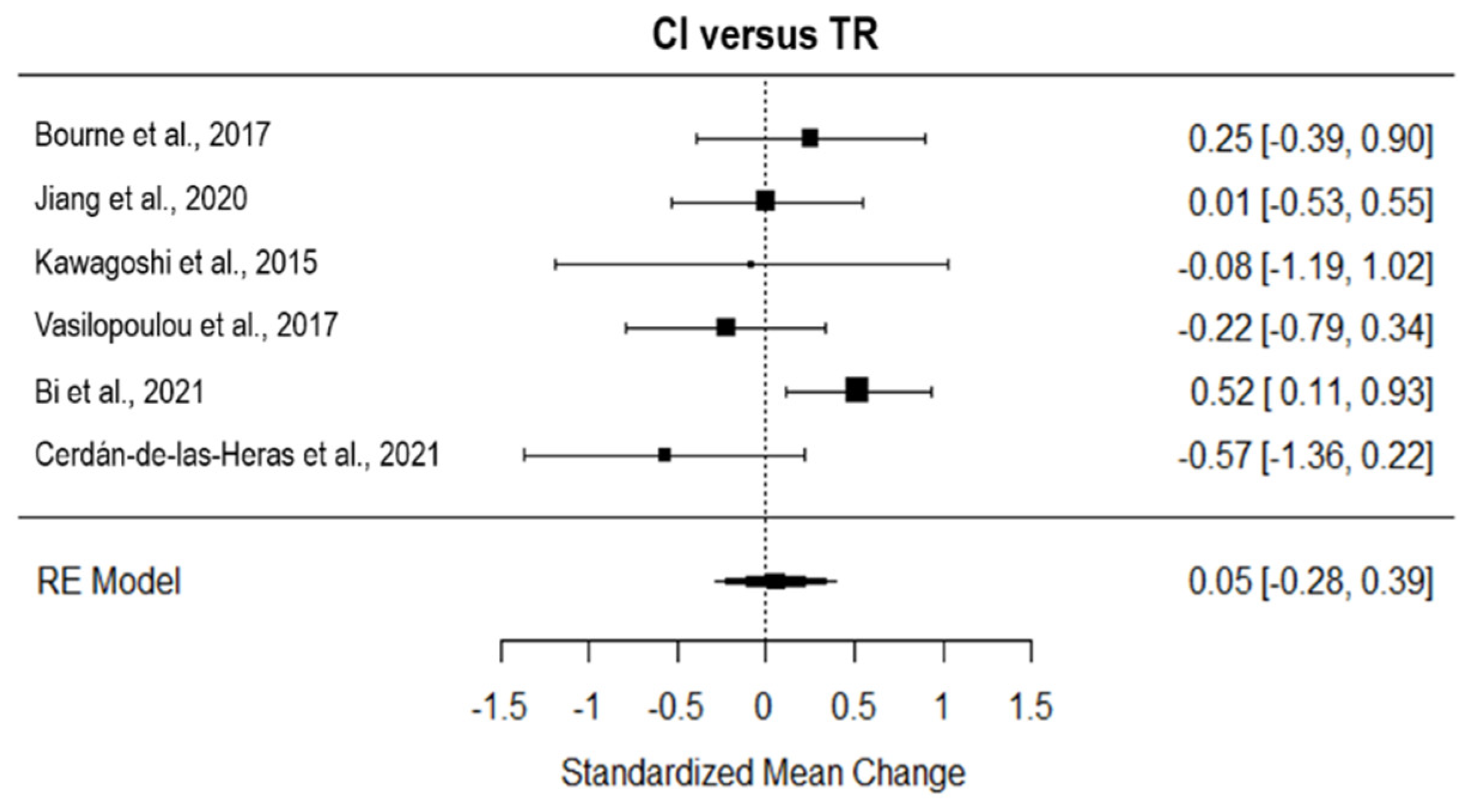
3.9. Quality of Life
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Burden Disease. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- Nugent, R.; Bertram, M.Y.; Jan, S.; Niessen, L.W.; Sassi, F.; Jamison, D.T.; Pier, E.G.; Beaglehole, R. Investing in non-communicable disease prevention and management to advance the Sustainable Development Goals. Lancet 2018, 391, 2029–2035. [Google Scholar] [CrossRef]
- Lainscak, M.; Anker, S.D. Heart failure, chronic obstructive pulmonary disease, and asthma: Numbers, facts, and challenges. ESC Heart Fail 2015, 2, 103–107. [Google Scholar] [CrossRef]
- Ryrsø, C.K.; Godtfredsen, N.S.; Kofod, L.M.; Lavesen, M.; Mogensen, L.; Tobberup, R.; Farver-Vestergaard, I.; Callesen, H.E.; Tendal, B.; Lange, P.; et al. Lower mortality after early supervised pulmonary rehabilitation following COPD-exacerbations: A systematic review and meta-analysis. BMC Pulm. Med. 2018, 18, 154. [Google Scholar] [CrossRef] [Green Version]
- Gee, P.M.; Greenwood, D.A.; Paterniti, D.A.; Ward, D.; Miller, L.M. The eHealth Enhanced Chronic Care Model: A theory derivation approach. J. Med. Internet Res. 2015, 17, e86. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.; et al. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [Green Version]
- Tabak, M.; Brusse-Keizer, M.; van der Valk, P.; Hermens, H.; Vollenbroek-Hutten, M. A telehealth program for self-management of COPD exacerbations and promotion of an active lifestyle: A pilot randomized controlled trial. Int. J. Chron. Obs. Pulmon. Dis 2014, 9, 935–944. [Google Scholar] [CrossRef] [Green Version]
- Vasilopoulou, M.; Papaioannou, A.I.; Kaltsakas, G.; Louvaris, Z.; Chynkiamis, N.; Spetsioti, S.; Kortianou, E.; Genimata, S.A.; Palamidas, A.; Kostikas, K.; et al. Home-based maintenance tele-rehabilitation reduces the risk for acute exacerbations of COPD, hospitalisations and emergency department visits. Eur. Respir. J. 2017, 49, 1602129. [Google Scholar] [CrossRef] [Green Version]
- Volpato, E.; Toniolo, S.; Pagnini, F.; Banfi, P. The Relationship between Anxiety, Depression and Treatment Adherence in Chronic Obstructive Pulmonary Disease: A Systematic Review. Int. J. Chron. Obs. Pulmon. Dis. 2021, 16, 2001–2021. [Google Scholar] [CrossRef]
- Oates, G.R.; Niranjan, S.J.; Ott, C.; Scarinci, I.C.; Schumann, C.; Parekh, T.; Dransfield, M.T. Adherence to Pulmonary Rehabilitation in COPD: A qualitative exploration of patient perspectives on barriers and facilitators. J. Cardiopulm. Rehabil. Prev. 2019, 39, 344–349. [Google Scholar] [CrossRef]
- Bashi, N.; Fatehi, F.; Mosadeghi-Nik, M.; Askari, M.S.; Karunanithi, M. Digital health interventions for chronic diseases: A scoping review of evaluation frameworks. BMJ Health Care Inform. 2020, 27, e100066. [Google Scholar] [CrossRef] [Green Version]
- Di Tella, S.; Pagliari, C.; Blasi, V.; Mendozzi, L.; Rovaris, M.; Baglio, F. Integrated telerehabilitation approach in multiple sclerosis: A systematic review and meta-analysis. J. Telemed. Telecare 2020, 26, 385–399. [Google Scholar] [CrossRef]
- Maisto, M.; Diana, B.; Di Tella, S.; Matamala-Gomez, M.; Montana, J.I.; Rossetto, F.; Mavrodiev, P.A.; Cavalera, C.; Blasi, V.; Mantovani, F.; et al. Digital Interventions for Psychological Comorbidities in Chronic Diseases-A Systematic Review. J. Pers. Med. 2021, 11, 30. [Google Scholar] [CrossRef]
- Cox, N.S.; Dal Corso, S.; Hansen, H.; McDonald, C.F.; Hill, C.J.; Zanaboni, P.; Alison, J.A.; O’Halloran, P.; Macdonald, H.; Holland, A.E. Telerehabilitation for chronic respiratory disease. Cochrane Database Syst. Rev. 2021, 1, Cd013040. [Google Scholar] [CrossRef]
- Theodoros, D.; Russell, T. Telerehabilitation: Current perspectives. Stud. Health Technol. Inf. 2008, 131, 191–209. [Google Scholar]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Isernia, S.; Pagliari, C.; Jonsdottir, J.; Castiglioni, C.; Gindri, P.; Gramigna, C.; Palumbo, G.; Salza, M.; Molteni, F.; Baglio, F. Efficiency and Patient-Reported Outcome Measures From Clinic to Home: The Human Empowerment Aging and Disability Program for Digital-Health Rehabilitation. Front. Neurol. 2019, 10, 1206. [Google Scholar] [CrossRef] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Smart, N.A.; Waldron, M.; Ismail, H.; Giallauria, F.; Vigorito, C.; Cornelissen, V.; Dieberg, G. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. Int. J. Evid. Based Health 2015, 13, 9–18. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Vorrink, S.N.; Kort, H.S.; Troosters, T.; Zanen, P.; Lammers, J.J. Efficacy of an mHealth intervention to stimulate physical activity in COPD patients after pulmonary rehabilitation. Eur. Respir. J. 2016, 48, 1019–1029. [Google Scholar] [CrossRef] [PubMed]
- Mendes de Oliveira, J.C.; Studart Leitão Filho, F.S.; Malosa Sampaio, L.M.; Negrinho de Oliveira, A.C.; Hirata, R.P.; Costa, D.; Donner, C.F.; de Oliveira, L.V. Outpatient vs. home-based pulmonary rehabilitation in COPD: A randomized controlled trial. Multidiscip. Respir. Med. 2010, 5, 401–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, D.; Svenningsen, H. Adherence to home-based inspiratory muscle training in individuals with chronic obstructive pulmonary disease. Appl. Nurs. Res. 2018, 43, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Kawagoshi, A.; Kiyokawa, N.; Sugawara, K.; Takahashi, H.; Sakata, S.; Satake, M.; Shioya, T. Effects of low-intensity exercise and home-based pulmonary rehabilitation with pedometer feedback on physical activity in elderly patients with chronic obstructive pulmonary disease. Respir. Med. 2015, 109, 364–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; Liu, F.; Guo, J.; Sun, P.; Chen, Z.; Li, J.; Cai, L.; Zhao, H.; Gao, P.; Ding, Z.; et al. Evaluating an Intervention Program Using WeChat for Patients with Chronic Obstructive Pulmonary Disease: Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e17089. [Google Scholar] [CrossRef] [Green Version]
- Bourne, S.; DeVos, R.; North, M.; Chauhan, A.; Green, B.; Brown, T.; Cornelius, V.; Wilkinson, T. Online versus face-to-face pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: Randomised controlled trial. BMJ Open 2017, 7, e014580. [Google Scholar] [CrossRef] [Green Version]
- Lahham, A.; McDonald, C.F.; Moore, R.; Cox, N.S.; Rawlings, S.; Nichols, A.; Liacos, A.; Holland, A.E. The impact of home-based pulmonary rehabilitation on people with mild chronic obstructive pulmonary disease: A randomised controlled trial. Clin. Respir. J. 2020, 14, 335–344. [Google Scholar] [CrossRef]
- Langer, D.; Ciavaglia, C.; Faisal, A.; Webb, K.A.; Neder, J.A.; Gosselink, R.; Dacha, S.; Topalovic, M.; Ivanova, A.; O’Donnell, D.E. Inspiratory muscle training reduces diaphragm activation and dyspnea during exercise in COPD. J. Appl. Physiol. (1985) 2018, 125, 381–392. [Google Scholar] [CrossRef] [Green Version]
- Santiworakul, A.; Piya-Amornphan, N.; Jianramas, N. A Home-Based Multimedia Pulmonary Rehabilitation Program Improves Clinical Symptoms and Physical Performance of Patients with Chronic Obstructive Pulmonary Disease. Int. J. Environ. Res. Public Health 2021, 18, 11479. [Google Scholar] [CrossRef]
- Xu, W.; Li, R.; Guan, L.; Wang, K.; Hu, Y.; Xu, L.; Zhou, L.; Chen, R.; Chen, X. Combination of inspiratory and expiratory muscle training in same respiratory cycle versus different cycles in COPD patients: A randomized trial. Respir. Res. 2018, 19, 225. [Google Scholar] [CrossRef]
- Liu, F.; Cai, H.; Tang, Q.; Zou, Y.; Wang, H.; Xu, Z.; Wei, Z.; Wang, W.; Cui, J. Effects of an animated diagram and video-based online breathing program for dyspnea in patients with stable COPD. Patient Prefer. Adherence 2013, 7, 905–913. [Google Scholar] [CrossRef]
- Holland, A.E.; Mahal, A.; Hill, C.J.; Lee, A.L.; Burge, A.T.; Cox, N.S.; Moore, R.; Nicolson, C.; O’Halloran, P.; Lahham, A.; et al. Home-based rehabilitation for COPD using minimal resources: A randomised, controlled equivalence trial. Thorax 2017, 72, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Tsai, L.L.; McNamara, R.J.; Moddel, C.; Alison, J.A.; McKenzie, D.K.; McKeough, Z.J. Home-based telerehabilitation via real-time videoconferencing improves endurance exercise capacity in patients with COPD: The randomized controlled TeleR Study. Respirology 2017, 22, 699–707. [Google Scholar] [CrossRef] [Green Version]
- Demeyer, H.; Louvaris, Z.; Frei, A.; Rabinovich, R.A.; de Jong, C.; Gimeno-Santos, E.; Loeckx, M.; Buttery, S.C.; Rubio, N.; Van der Molen, T.; et al. Physical activity is increased by a 12-week semiautomated telecoaching programme in patients with COPD: A multicentre randomised controlled trial. Thorax 2017, 72, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; He, L.; Tao, Y.; Sun, L.; Zheng, H.; Zheng, Y.; Shen, Y.; Liu, S.; Zhao, Y.; Wang, Y. Evaluating a Web-Based Coaching Program Using Electronic Health Records for Patients With Chronic Obstructive Pulmonary Disease in China: Randomized Controlled Trial. J. Med. Internet Res. 2017, 19, e264. [Google Scholar] [CrossRef]
- Bi, J.; Yang, W.; Hao, P.; Zhao, Y.; Wei, D.; Sun, Y.; Lin, Y.; Sun, M.; Chen, X.; Luo, X.; et al. WeChat as a Platform for Baduanjin Intervention in Patients With Stable Chronic Obstructive Pulmonary Disease in China: Retrospective Randomized Controlled Trial. JMIR Mhealth Uhealth 2021, 9, e23548. [Google Scholar] [CrossRef]
- Cerdán-de-Las-Heras, J.; Balbino, F.; Løkke, A.; Catalán-Matamoros, D.; Hilberg, O.; Bendstrup, E. Effect of a New Tele-Rehabilitation Program versus Standard Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2021, 11, 11. [Google Scholar] [CrossRef]
- Galdiz, J.B.; Gómez, A.; Rodriguez, D.; Guell, R.; Cebollero, P.; Hueto, J.; Cejudo, P.; Ortega, F.; Sayago, I.; Chic, S.; et al. Telerehabilitation Programme as a Maintenance Strategy for COPD Patients: A 12-Month Randomized Clinical Trial. Arch. Bronconeumol. 2021, 57, 195–204. [Google Scholar] [CrossRef]
- Li, Y.; Qian, H.; Yu, K.; Huang, Y. The Long-Term Maintenance Effect of Remote Pulmonary Rehabilitation via Social Media in COPD: A Randomized Controlled Trial. Int. J. Chron. Obs. Pulmon. Dis. 2022, 17, 1131–1142. [Google Scholar] [CrossRef]
- Hansen, H.; Bieler, T.; Beyer, N.; Kallemose, T.; Wilcke, J.T.; Østergaard, L.M.; Frost Andeassen, H.; Martinez, G.; Lavesen, M.; Frølich, A.; et al. Supervised pulmonary tele-rehabilitation versus pulmonary rehabilitation in severe COPD: A randomised multicentre trial. Thorax 2020, 75, 413–421. [Google Scholar] [CrossRef] [Green Version]
- Park, S.K.; Bang, C.H.; Lee, S.H. Evaluating the effect of a smartphone app-based self-management program for people with COPD: A randomized controlled trial. Appl. Nurs. Res. 2020, 52, 151231. [Google Scholar] [CrossRef] [PubMed]
- Richardson, C.R.; Franklin, B.; Moy, M.L.; Jackson, E.A. Advances in rehabilitation for chronic diseases: Improving health outcomes and function. BMJ 2019, 365, l2191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloem, B.R.; Munneke, M. Revolutionising management of chronic disease: The ParkinsonNet approach. BMJ 2014, 348, g1838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossetto, F.; Borgnis, F.; Blasi, V.; Banfi, P.I.; Tavanelli, M.; Realdon, O.; Mantovani, F.; Foglia, E.; Garagiola, E.; Croce, D.; et al. System Integrated Digital Empowerment and Rehabilitation to promote patient Activation and well-Being (SIDERA^ B): Protocol for a Randomized Crossover Trial on Effectiveness and Implementation. medRxiv 2022. [Google Scholar] [CrossRef]
- Khakban, A.; Sin, D.D.; FitzGerald, J.M.; McManus, B.M.; Ng, R.; Hollander, Z.; Sadatsafavi, M. The Projected Epidemic of Chronic Obstructive Pulmonary Disease Hospitalizations over the Next 15 Years. A Population-based Perspective. Am. J. Respir. Crit. Care Med. 2017, 195, 287–291. [Google Scholar] [CrossRef]







| Outcome | Domain | Subdomain | Tool | Pre-Based | Prom-Based | References |
|---|---|---|---|---|---|---|
| Medical Benefit | Functional Capacity | Endurance | 6 min Walk Distance | x | [8,21,22,23,24,26,27,29,30,31,32,33,34,35,37,38,39,40,41] | |
| Endurance shuttle walk test | x | [33] | ||||
| Physical Activity | Actigraph | x | [8,21,24,27,33,34,37,40,41] | |||
| Physical Activity Level | x | [40] | ||||
| Incremental Shuttle Walking Test | x | [33] | ||||
| Functional Performance Inventory—Short Form | x | [33] | ||||
| BMI | Weight × height2 | x | [21,22,30] | |||
| Strength | Quadricep force | x | [29,34] | |||
| Triceps force | x | [29] | ||||
| Breath | Modified Medical Research Council dyspnea scale | x | [8,22,24,25,27,28,30,32,33,34,35,39] | |||
| San Diego Shortness of Breath Questionnaire | x | [41] | ||||
| Spirometry values (i.e., FEV1, FVC) | x | [21,22,23,24,28,30,31,33,35,36,37,39] | ||||
| Participation | Quality of Life | St George’s Hospital Respiratory Questionnaire | x | [8,25,30,31,35,37] | ||
| COPD-CAT | x | [8,24,26,30,33,34,36,39,40] | ||||
| Chronic Respiratory Questionnaire | x | [21,24,27,32,33,38] | ||||
| EuroQol 5-Dimension Questionnaire | x | [40] | ||||
| 36-Item Short-Form Health Survey | x | [38,41] | ||||
| Clinical COPD Questionnaire | x | [29,40] | ||||
| IADL | x | [37,39] | ||||
| Mood | Hospital Anxiety and Depression Scale | x | [26,30,32,33,40] | |||
| Profile of Mood States-Short Form | x | [41] | ||||
| General Anxiety Disorder Score | x | [37] | ||||
| Beck Depression Inventory | x | [39] | ||||
| State-trait Anxiety Inventory | x | [39] | ||||
| Self-Efficacy | Exercise Self-Regulatory Efficacy Scale | x | [25] | |||
| Self-Efficacy for Managing Chronic Disease 6-Item Scale | x | [41] | ||||
| Alberto Chronic Obstructive Pulmonary Disease Self-Care Behavior Inventory | x | [41] | ||||
| Pulmonary Rehabilitation Adapted Index of Self-Efficacy | x | [32,33] | ||||
| Social Support | MOS Social Support Survey | x | [41] | |||
| Mortality | - | N Deaths | [40] | |||
| Morbidity | - | COPD-specific COmorbidity TEst | x | [32] | ||
| Exacerbation history and comorbidity | x | [34] | ||||
| Patient-Relevant | Adherence | - | N sessions/expected N sessions × 100 | x | [8] | |
| N sessions performed | x | [23,26,33,37,41] | ||||
| Time dedicated to tasks | x | [41] | ||||
| Work rate/exercise time (s) | x | [33] | ||||
| N participants who complied with treatment (at least 8 consecutive weeks) | x | [38] | ||||
| Safety | - | Adverse events and hospitalizations | x | [26,34,35,37,38,39,41] | ||
| Frequency of ED visits, outpatient clinic visits | x | [39,41] | ||||
| Open-ended questions | x | [41] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isernia, S.; Pagliari, C.; Bianchi, L.N.C.; Banfi, P.I.; Rossetto, F.; Borgnis, F.; Tavanelli, M.; Brambilla, L.; Baglio, F., on behalf of the CPTM Group. Characteristics, Components, and Efficacy of Telerehabilitation Approaches for People with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15165. https://doi.org/10.3390/ijerph192215165
Isernia S, Pagliari C, Bianchi LNC, Banfi PI, Rossetto F, Borgnis F, Tavanelli M, Brambilla L, Baglio F on behalf of the CPTM Group. Characteristics, Components, and Efficacy of Telerehabilitation Approaches for People with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(22):15165. https://doi.org/10.3390/ijerph192215165
Chicago/Turabian StyleIsernia, Sara, Chiara Pagliari, Luca Nicola Cesare Bianchi, Paolo Innocente Banfi, Federica Rossetto, Francesca Borgnis, Monica Tavanelli, Lorenzo Brambilla, and Francesca Baglio on behalf of the CPTM Group. 2022. "Characteristics, Components, and Efficacy of Telerehabilitation Approaches for People with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 22: 15165. https://doi.org/10.3390/ijerph192215165