
China’s Accession to the WTO as a Shock to Residents’ Health—A Difference-in-Difference Approach
Abstract
:1. Introduction
2. Literature Review
2.1. Studies on the Economic Effects of Trade Policy Uncertainty
2.2. Studies on the Health Effects of Trade Liberalization
3. Background and Theoretical Hypotheses
3.1. Background
3.2. Migration
3.3. Working Hours
3.4. Environmental Pollution
4. Model and Variables
4.1. Empirical Model
4.2. Variables
- Status of residents’ health (). The advantage of objective indicators over subjective indicators is that there is a uniform assessment standard across individuals. Since the beginning of the survey in 1991, CHNS has conducted three rounds of blood pressure measurement for each respondent, which provides data support for the objective evaluation of the individual health status of respondents. To avoid measurement bias resulting from the initial results being influenced by psychological fluctuations and other factors, we use only the mean values of the last two blood pressure measurements to determine whether an individual has hypertension. Respondents with systolic blood pressure greater than 120 mmHg or diastolic blood pressure greater than 80 mmHg were considered hypertensive according to the criteria recommended in the guidelines for the treatment of hypertension in China. If an individual had hypertension, it was recorded as 1, and vice versa as 0. (The regression results remain robust when we use standard errors an individual is away from the mean value of the prefecture as the dependent variable).
- Trade shock (). Trade shock can be expressed as the magnitude of an adverse change in trade policy when that change occurs. Consistent with existing studies, we measure this change using the difference between the US two-column tariff and the MFN tariff rate before China acceded to the WTO [13]. Specifically, we calculate the tariff differential based on the US’s HS-8-digit code ad valorem rates, averaged to the HS-6-digit. Next, the tariff differential at the industry level for each 4-digit of the National Economic Classification can be obtained based on the HS-CIC code conversion table provided by Brandt et al. [43]. Finally, if tariffs fall more in industries with a higher share of employment in a region, the greater the decline in tariff uncertainty in that region, and thus the initial employment structure of each region is an important determinant of its exposure to shocks. Referring to the approach of Bartik [23], we sum the industry-level tariff differentials to the prefecture level according to the following equation:where is the total employment in the region in 2001; is the employment in the industry in the same year. We identify the treatment group through the continuous variable because: (1) the greater the tariff uncertainty faced by a prefecture, the greater the impact of China’s WTO accession to permanent normal trade relations on the health status of the region’s residents; (2) the U.S. 2-column tariff was set in 1930, and the tariff differential before the implementation of the policy is highly exogenous. More specifically, China’s accession to the WTO requires the consent of all Members, and many details of the negotiated agreement remained unresolved until 2001, and the timing of WTO accession is unpredictable, i.e., China’s accession to the WTO is an exogenous event. The literature evaluating the trade and economic effects of trade policy uncertainty points out that the Smoot–Hawley tariffs imposed by the US have long been determined by history, suggesting that the tariff uncertainty is exogenous [9,13,19]. Therefore, the endogeneity problem can be avoided to a large extent. (3) The prefecture employment structure data used in this paper were established before China’s WTO accession, and the concomitant expansion of exports is a channel of influence linking trade liberalization to individual health, which will be explored in more detail below.
- Year dummy variable of WTO (). China formally joined the WTO on December 11, 2001, and its import tariffs on goods were significantly reduced, while it received the corresponding preferential import tariff treatment from the U.S. PNTR, and the tariff uncertainty it faced declined. In this paper, the year 2002 is used as the actual effective year of the policy, and the value of 1 is assigned if the sample is in the year 2002 or later, otherwise it is 0.
- Individual-level characteristic variables (). Residents’ health will inevitably be influenced by individual-level factors; concerning the relevant literature, the following control variables are introduced: (1) Gender (). The value is 1 when the respondent is male, otherwise, it is 0. (2) Age (). It is expressed as the logarithm of the difference between the year the respondent was interviewed and his or her calendar year of birth. (In semi-logarithmic form, the effect of age on health is . The results are unaffected when we do not take the logarithm of the age). (3) Educational background (): The CHNS database records the highest educational level obtained by each respondent, and the questionnaire results include seven types of results: never educated, graduated from elementary school, graduated from junior high school, graduated from high school, graduated from secondary school, graduated from college or university, and graduated from master’s degree or above. We assign values 0~6 to in order. (The results remain robust when we replace the categorical variable with a series of dummy variables and their interaction terms with ). (4) Whether the respondent has medical insurance (). The variable takes the value of 1 when the respondent has health insurance and 0 otherwise. (5) Marital status (). CHNS gives the marital status of each respondent in that year, and distinguishes five types of states: unmarried, married, divorced, widowed, and separated, and assigns values from 1 to 5 in that order. (Similar to the variable of educational background, the results remain robust when we replace the categorical variable with a series of dummy variables and their interaction terms with ).
4.3. Data
5. Empirical Results
5.1. Baseline Specification
5.2. DID Validity Test
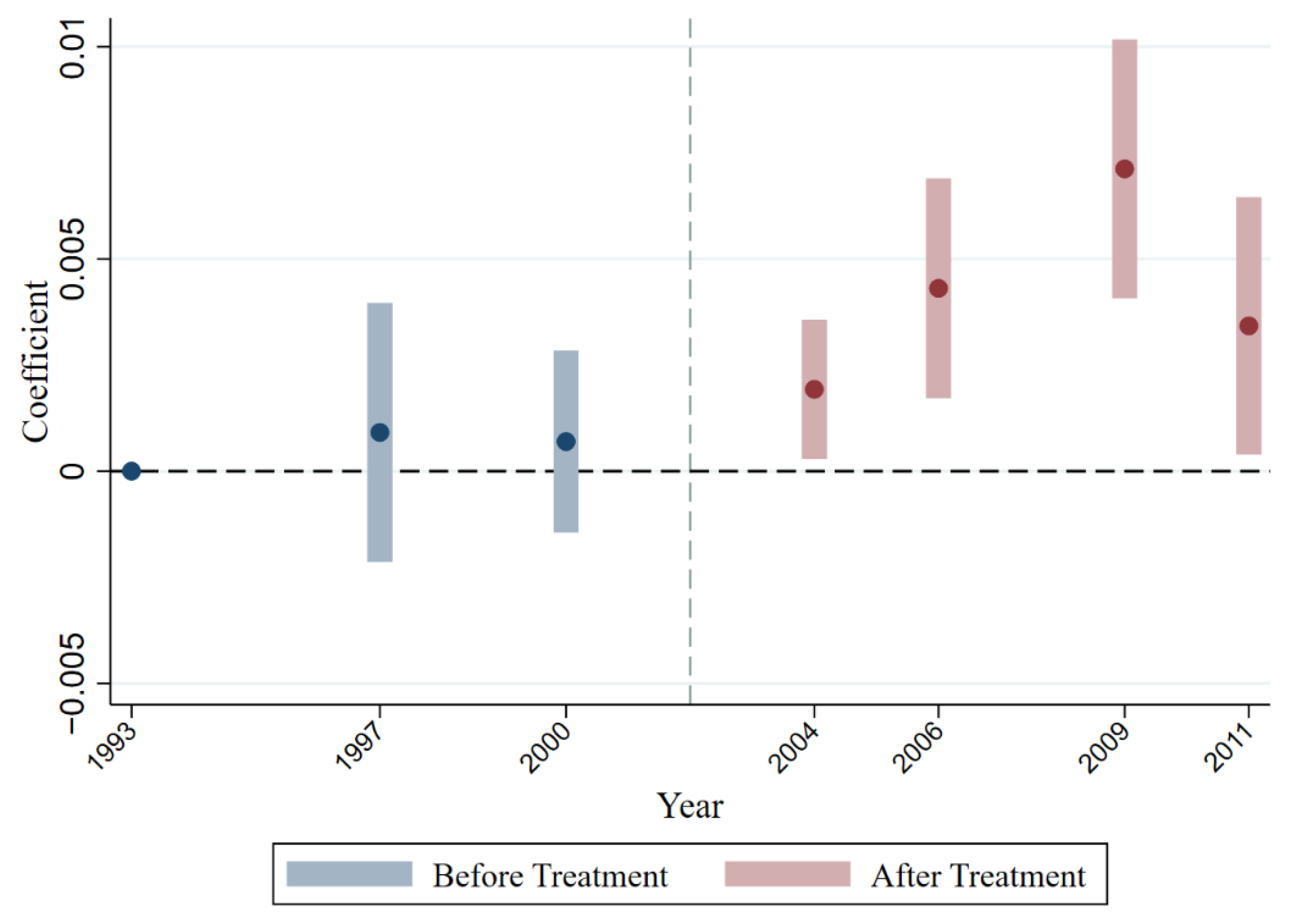
5.2.1. Dynamic Effect
5.2.2. Expectation Effect
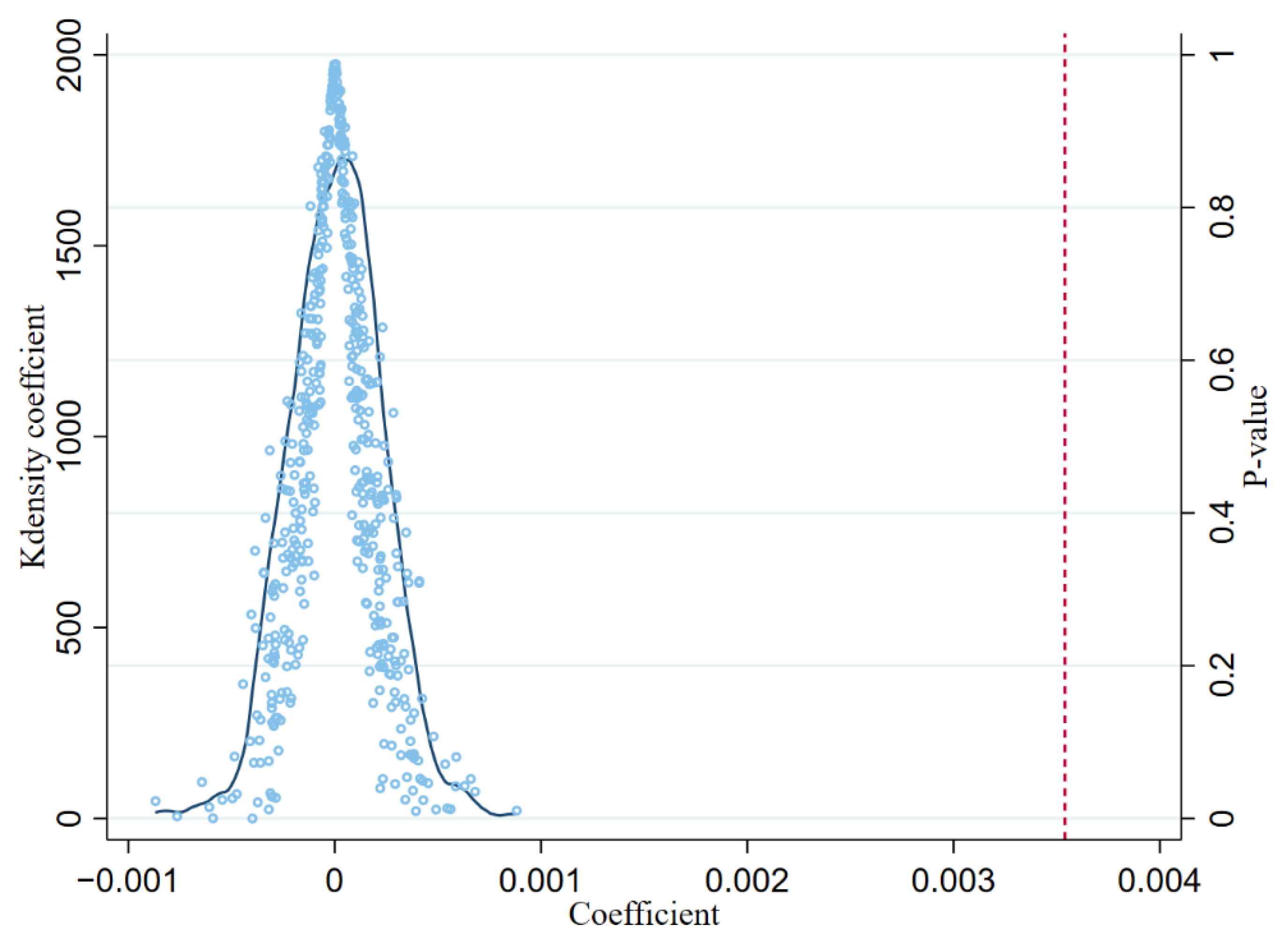
5.2.3. Placebo Test
5.3. Robustness Tests
5.3.1. Indicator Change
5.3.2. Two-Period DID
5.3.3. Controlling for Interferences from Other Sources
5.3.4. Prefecture-Specific Trends
5.3.5. Weighted Regression
6. Heterogeneity Impact Analysis
6.1. Type of Residence
6.2. Gender
6.3. Geography
6.4. Testing for Nonlinearity
7. Mechanism
7.1. Migration
7.2. Working Hours
7.3. Environmental Pollution
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Deaton, A.; Paxson, C. Mortality, education, income, and inequality among American cohorts. In Themes in the Economics of Aging; University of Chicago Press: Chicago, IL, USA, 2001; pp. 129–170. [Google Scholar]
- Rodriguez-Martinez, A.; Zhou, B.; Sophiea, M.K.; Bentham, J.; Paciorek, C.J.; Iurilli, M.L.; Carrillo-Larco, R.M.; Bennett, J.E.; Di Cesare, M.; Taddei, C. Height and body-mass index trajectories of school-aged children and adolescents from 1985 to 2019 in 200 countries and territories: A pooled analysis of 2181 population-based studies with 65 million participants. Lancet 2020, 396, 1511–1524. [Google Scholar] [CrossRef]
- Levine, D.I.; Rothman, D. Does trade affect child health? J. Health Econ. 2006, 25, 538–554. [Google Scholar] [CrossRef] [PubMed]
- Bombardini, M.; Li, B. Trade, pollution and mortality in China. J. Int. Econ. 2020, 125, 103321. [Google Scholar] [CrossRef] [Green Version]
- Stevens, P.; Urbach, J.; Wills, G. Healthy trade: The relationship between open trade and health. Foreign Trade Rev. 2013, 48, 125–135. [Google Scholar] [CrossRef]
- Handley, K. Exporting under trade policy uncertainty: Theory and evidence. J. Int. Econ. 2014, 94, 50–66. [Google Scholar] [CrossRef] [Green Version]
- Handley, K.; Limao, N. Trade and investment under policy uncertainty: Theory and firm evidence. Am. Econ. J. Econ. Policy 2015, 7, 189–222. [Google Scholar] [CrossRef] [Green Version]
- Handley, K.; Limao, N. Policy uncertainty, trade, and welfare: Theory and evidence for China and the United States. Am. Econ. Rev. 2017, 107, 2731–2783. [Google Scholar] [CrossRef] [Green Version]
- Feng, L.; Li, Z.; Swenson, D.L. Trade policy uncertainty and exports: Evidence from China’s WTO accession. J. Int. Econ. 2017, 106, 20–36. [Google Scholar] [CrossRef] [Green Version]
- Hu, G.; Liu, S. Economic Policy Uncertainty (EPU) and China’s export fluctuation in the post-pandemic era: An empirical analysis based on the TVP-SV-VAR model. Front. Public Health 2021, 9, 788171. [Google Scholar] [CrossRef]
- Imbruno, M. Importing under trade policy uncertainty: Evidence from China. J. Comp. Econ. 2019, 47, 806–826. [Google Scholar] [CrossRef]
- Zhao, T. Economic policy uncertainty and manufacturing value-added exports. Eng. Econ. 2022, 33, 103–114. [Google Scholar] [CrossRef]
- Pierce, J.R.; Schott, P.K. The surprisingly swift decline of US manufacturing employment. Am. Econ. Rev. 2016, 106, 1632–1662. [Google Scholar] [CrossRef] [Green Version]
- Gilchrist, S.; Sim, J.W.; Zakrajšek, E. Uncertainty, Financial Frictions, and Investment Dynamics; NBER Working Paper; No. 20038; National Bureau of Economic Research: Cambridge, MA, USA, 2014. [Google Scholar]
- Ouyang, D.; Yuan, W. Industrial Development and Trade Policy Uncertainty: Evidence from China’s WTO Accession. 2022. No. 4188516. Available online: https://ssrn.com/abstract=4188516 (accessed on 12 August 2022).
- Carballo, J.; Handley, K.; Limão, N. Economic and Policy Uncertainty: Export Dynamics and the Value of Agreements; NBER Working Paper; No. 24368; National Bureau of Economic Research: Cambridge, MA, USA, 2018. [Google Scholar]
- Yu, M. Processing trade, tariff reductions and firm productivity: Evidence from Chinese firms. Econ. J. 2015, 125, 943–988. [Google Scholar] [CrossRef]
- Amiti, M.; Konings, J. Trade liberalization, intermediate inputs, and productivity: Evidence from Indonesia. Am. Econ. Rev. 2007, 97, 1611–1638. [Google Scholar] [CrossRef]
- Liu, Q.; Ma, H. Trade policy uncertainty and innovation: Firm level evidence from China’s WTO accession. J. Int. Econ. 2020, 127, 103387. [Google Scholar] [CrossRef]
- Schott, P.; Pierce, J.; Schaur, G.; Heise, S. Trade policy uncertainty and the structure of supply chains. In Proceedings of the 2017 Meeting Papers; Society for Economic Dynamics: Stonybrook, NY, USA, 2017. [Google Scholar]
- Shepotylo, O.; Stuckatz, J. Quantitative Text Analysis of Policy Uncertainty: FDI and Trade of Ukrainian Manufacturing Firms; Social Science Electronic Publishing: Rochester, NY, USA, 2017. [Google Scholar]
- Greenland, A.; Ion, M.; Lopresti, J. Exports, investment and policy uncertainty. Can. J. Econ./Rev. Can. D’économique 2019, 52, 1248–1288. [Google Scholar] [CrossRef]
- Bartik, T.J. Who Benefits From State and Local Economic Development Policies; WE Upjohn Institute for Employment Research: Kalamazoo, MI, USA, 1991. [Google Scholar]
- Owen, A.L.; Wu, S. Is trade good for your health? Rev. Int. Econ. 2007, 15, 660–682. [Google Scholar] [CrossRef]
- Herzer, D. The long-run relationship between trade and population health: Evidence from five decades. World Econ. 2017, 40, 462–487. [Google Scholar] [CrossRef] [Green Version]
- Adda, J.; Fawaz, Y. The health toll of import competition. Econ. J. 2020, 130, 1501–1540. [Google Scholar] [CrossRef]
- McManus, T.C.; Schaur, G. The effects of import competition on worker health. J. Int. Econ. 2016, 102, 160–172. [Google Scholar] [CrossRef]
- Guerrico, S.F. The effects of trade-induced worker displacement on health and mortality in Mexico. J. Health Econ. 2021, 80, 102538. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M. Exporting sweatshops? Evidence from Myanmar. Rev. Econ. Stat. 2020, 102, 442–456. [Google Scholar] [CrossRef]
- Lang, M.; McManus, T.C.; Schaur, G. The effects of import competition on health in the local economy. Health Econ. 2019, 28, 44–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dix-Carneiro, R.; Kovak, B.K. Trade liberalization and regional dynamics. Am. Econ. Rev. 2017, 107, 2908–2946. [Google Scholar] [CrossRef] [Green Version]
- Fan, H.; Lin, F.; Lin, S. The hidden cost of trade liberalization: Input tariff shocks and worker health in China. J. Int. Econ. 2020, 126, 103349. [Google Scholar] [CrossRef]
- Facchini, G.; Liu, M.Y.; Mayda, A.M.; Zhou, M. China’s “Great Migration”: The impact of the reduction in trade policy uncertainty. J. Int. Econ. 2019, 120, 126–144. [Google Scholar] [CrossRef]
- Wang, F.; Milner, C.; Scheffel, J. Labour market reform and firm-level employment adjustment: Evidence from the hukou reform in China. J. Dev. Econ. 2021, 149, 102584. [Google Scholar] [CrossRef]
- Johansson, M.; Partanen, T. Role of trade unions in workplace health promotion. Int. J. Health Serv. 2002, 32, 179–193. [Google Scholar] [CrossRef]
- Gardner, J.; Oswald, A.J. Money and mental wellbeing: A longitudinal study of medium-sized lottery wins. J. Health Econ. 2007, 26, 49–60. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, D.; Von Wachter, T. Job displacement and mortality: An analysis using administrative data. Q. J. Econ. 2009, 124, 1265–1306. [Google Scholar] [CrossRef]
- Burgoon, B.; Raess, D. Globalization and working time: Working hours and flexibility in Germany. Politics Soc. 2009, 37, 554–575. [Google Scholar] [CrossRef]
- Steinmetz, H.; Schmidt, P. Subjective health and its relationship with working time variables and job stressors: Sequence or general factor model? Work Stress 2010, 24, 159–178. [Google Scholar] [CrossRef]
- Lovely, M.; Popp, D. Trade, Technology, and the Environment: Why Have Poor Countries Regulated Sooner? NBER Working Paper; No. 14286; National Bureau of Economic Research: Cambridge, MA, USA, 2008. [Google Scholar]
- Managi, S.; Hibiki, A.; Tsurumi, T. Does trade openness improve environmental quality? J. Environ. Econ. Manag. 2009, 58, 346–363. [Google Scholar] [CrossRef]
- Bertrand, M.; Duflo, E.; Mullainathan, S. How much should we trust differences-in-differences estimates? Q. J. Econ. 2004, 119, 249–275. [Google Scholar] [CrossRef] [Green Version]
- Brandt, L.; Van Biesebroeck, J.; Wang, L.; Zhang, Y. WTO accession and performance of Chinese manufacturing firms. Am. Econ. Rev. 2017, 107, 2784–2820. [Google Scholar] [CrossRef] [Green Version]
- Kemptner, D.; Jürges, H.; Reinhold, S. Changes in compulsory schooling and the causal effect of education on health: Evidence from Germany. J. Health Econ. 2011, 30, 340–354. [Google Scholar] [CrossRef] [Green Version]
- Angrist, J.D.; Pischke, J.-S. Mostly Harmless Econometrics; Princeton University Press: Princeton, NJ, USA, 2008. [Google Scholar]
- La Ferrara, E.; Chong, A.; Duryea, S. Soap operas and fertility: Evidence from Brazil. Am. Econ. J. Appl. Econ. 2012, 4, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Qiu, L.D. Intermediate input imports and innovations: Evidence from Chinese firms’ patent filings. J. Int. Econ. 2016, 103, 166–183. [Google Scholar] [CrossRef]
- Robertson, R. Trade liberalisation and wage inequality: Lessons from the Mexican experience. World Econ. 2000, 23, 827–849. [Google Scholar] [CrossRef]
- Chen, Y.; Ebenstein, A.; Greenstone, M.; Li, H. Evidence on the impact of sustained exposure to air pollution on life expectancy from China’s Huai River policy. Proc. Natl. Acad. Sci. USA 2013, 110, 12936–12941. [Google Scholar] [CrossRef]
- Tanaka, S. Environmental regulations on air pollution in China and their impact on infant mortality. J. Health Econ. 2015, 42, 90–103. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Observations | Average | SD | Min | Max |
|---|---|---|---|---|---|
| 61,106 | 0.136 | 0.343 | 0 | 1 | |
| 61,106 | 5.002 | 8.509 | 0.148 | 51.506 | |
| 61,106 | 0.488 | 0.5 | 0 | 1 | |
| 61,106 | 3.536 | 0.668 | 0 | 4.615 | |
| 61,106 | 1.647 | 1.388 | 0 | 6 | |
| 61,106 | 0.48 | 0.5 | 0 | 1 | |
| 61,106 | 1.949 | 0.705 | 1 | 5 |
| (1) | (2) | (3) | |
|---|---|---|---|
| health | health | health | |
| 0.00278 *** | 0.00402 *** | 0.00354 *** | |
| (0.00057) | (0.00067) | (0.00083) | |
| 0.03810 *** | 0.03814 *** | ||
| (0.00555) | (0.00555) | ||
| 0.17831 *** | 0.17831 *** | ||
| (0.00987) | (0.00989) | ||
| –0.02716 *** | −0.02717 *** | ||
| (0.00264) | (0.00263) | ||
| 0.02064 ** | 0.02058 ** | ||
| (0.00742) | (0.00734) | ||
| 0.00407 | 0.00412 | ||
| (0.00487) | (0.00485) | ||
| 0.00753 | |||
| (0.00526) | |||
| Prefecture FE | YES | YES | YES |
| Year FE | YES | YES | YES |
| N | 61,106 | 55,320 | 55,320 |
| Adjusted R2 | 0.024 | 0.107 | 0.107 |
| (1) | (2) | (3) | |
|---|---|---|---|
| Dynamic Effect | Expectation Effect | ||
| 0.00091 | |||
| (0.00156) | |||
| 0.00070 | |||
| (0.00109) | |||
| 0.00193 ** | |||
| (0.00084) | |||
| 0.00431 *** | |||
| (0.00132) | |||
| 0.00712 *** | |||
| (0.00156) | |||
| 0.00342 ** | |||
| (0.00155) | |||
| 0.00254 *** | 0.00370 *** | ||
| (0.00070) | (0.00091) | ||
| −0.00056 | 0.00034 | ||
| (0.00092) | (0.00118) | ||
| Controls | YES | NO | YES |
| Prefecture FE | YES | YES | YES |
| Year FE | YES | YES | YES |
| N | 51,098 | 61,106 | 55,320 |
| Adjusted R2 | 0.107 | 0.024 | 0.107 |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | |
|---|---|---|---|---|---|---|---|---|---|
| Subjective Health | Weighted Health | Two-Period DID | Financial Crisis | FDI Liberalization | Environmental Policy | Employment | Prefecture-Specific Trends | Weighted Regression | |
| 0.00353 *** | 0.00287 *** | 0.00215 ** | 0.00310 *** | 0.00264 ** | 0.00271 *** | 0.00269 *** | |||
| (0.00067) | (0.00075) | (0.00085) | (0.00095) | (0.00093) | (0.00079) | (0.00077) | |||
| 0.00103 *** | 0.00211 ** | ||||||||
| (0.00017) | (0.00066) | ||||||||
| 0.02317 | 0.02461 * | 0.02464 * | 0.02488 ** | ||||||
| (0.01336) | (0.01298) | (0.01292) | (0.01071) | ||||||
| 0.00001 | 0.00007 | 0.00042 | |||||||
| (0.00187) | (0.00184) | (0.00180) | |||||||
| −0.00204 ** | −0.00209 *** | −0.00118 | |||||||
| (0.00067) | (0.00066) | (0.00078) | |||||||
| −0.02487 | −0.02353 | 0.00520 | |||||||
| (0.03111) | (0.03571) | (0.04334) | |||||||
| −0.00001 | −0.00001 | 0.00002 | |||||||
| (0.00010) | (0.00010) | (0.00011) | |||||||
| −0.00001 | −0.00004 | ||||||||
| (0.00003) | (0.00003) | ||||||||
| Controls | YES | YES | YES | YES | YES | YES | YES | YES | YES |
| Prefecture FE | YES | YES | YES | YES | YES | YES | YES | YES | YES |
| Year FE | YES | YES | YES | YES | YES | YES | YES | YES | YES |
| N | 52,422 | 29,919 | 16,604 | 30,185 | 55,320 | 55,320 | 55,320 | 55,320 | 51,098 |
| Adjusted R2 | 0.107 | 0.136 | 0.162 | 0.108 | 0.107 | 0.107 | 0.107 | 0.107 | 0.104 |
| (1) | (2) | (3) | (4) | (5) | (6) | |
|---|---|---|---|---|---|---|
| Urban | Rural | Female | Male | Coastal Areas | Other Areas | |
| 0.00535 *** | 0.00285 | 0.00132 | 0.00423 *** | 0.00341 ** | 0.00358 | |
| (0.00169) | (0.00267) | (0.00087) | (0.00100) | (0.00119) | (0.00296) | |
| Controls | YES | YES | YES | YES | YES | YES |
| Prefecture FE | YES | YES | YES | YES | YES | YES |
| Year FE | YES | YES | YES | YES | YES | YES |
| N | 20,592 | 34,728 | 28,842 | 26,478 | 25,889 | 29,431 |
| Adjusted R2 | 0.114 | 0.105 | 0.121 | 0.097 | 0.108 | 0.108 |
| Variables | health |
|---|---|
| Group1: | 0.05524 |
| (0.03661) | |
| Group2: | 0.05086 ** |
| (0.02192) | |
| Group3: | 0.03318 ** |
| (0.01294) | |
| Group4: | 0.01126 |
| (0.00827) | |
| Group5: | 0.00552 *** |
| (0.00141) | |
| Controls | YES |
| Prefecture FE | YES |
| Year FE | YES |
| N | 55,320 |
| Adjusted R2 | 0.107 |
| (1) | (2) | (3) | (4) | |
|---|---|---|---|---|
| health | hours | pollutant | ||
| non-hukou | hukou | |||
| 0.00523 ** | 0.00281 * | 0.57991 ** | 0.06459 ** | |
| (0.00177) | (0.00145) | (0.24857) | (0.02802) | |
| −0.20980 *** | 0.09785 ** | 3.75144 | 2.92683 *** | |
| (0.03371) | (0.03597) | (5.22026) | (0.38732) | |
| 0.00487 | −0.17561 * | −6.57101 | −2.78619 *** | |
| (0.01953) | (0.07166) | (5.28266) | (0.44092) | |
| 0.00044 *** | 0.00027 ** | 0.00854 | 0.01412 *** | |
| (0.00002) | (0.00009) | (0.00605) | (0.00123) | |
| −0.00007 | 0.00001 | −0.00299 | 0.00017 | |
| (0.00014) | (0.00005) | (0.00550) | (0.00012) | |
| Controls | YES | YES | YES | YES |
| Prefecture FE | YES | YES | YES | YES |
| Year FE | YES | YES | YES | YES |
| N | 24,052 | 28,987 | 26,247 | 5472 |
| Adjusted R2 | 0.040 | 0.044 | 0.095 | 0.939 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Y.; Wu, C.; Zhu, X.; Bian, P. China’s Accession to the WTO as a Shock to Residents’ Health—A Difference-in-Difference Approach. Int. J. Environ. Res. Public Health 2022, 19, 14728. https://doi.org/10.3390/ijerph192214728
Sun Y, Wu C, Zhu X, Bian P. China’s Accession to the WTO as a Shock to Residents’ Health—A Difference-in-Difference Approach. International Journal of Environmental Research and Public Health. 2022; 19(22):14728. https://doi.org/10.3390/ijerph192214728
Chicago/Turabian StyleSun, Yiping, Chengjun Wu, Xiaoming Zhu, and Pingguan Bian. 2022. "China’s Accession to the WTO as a Shock to Residents’ Health—A Difference-in-Difference Approach" International Journal of Environmental Research and Public Health 19, no. 22: 14728. https://doi.org/10.3390/ijerph192214728