
Emergency First Responders and Professional Wellbeing: A Qualitative Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Keyword Development
2.2. Database Selection and Filters
2.3. Inclusion/Exclusion Criteria
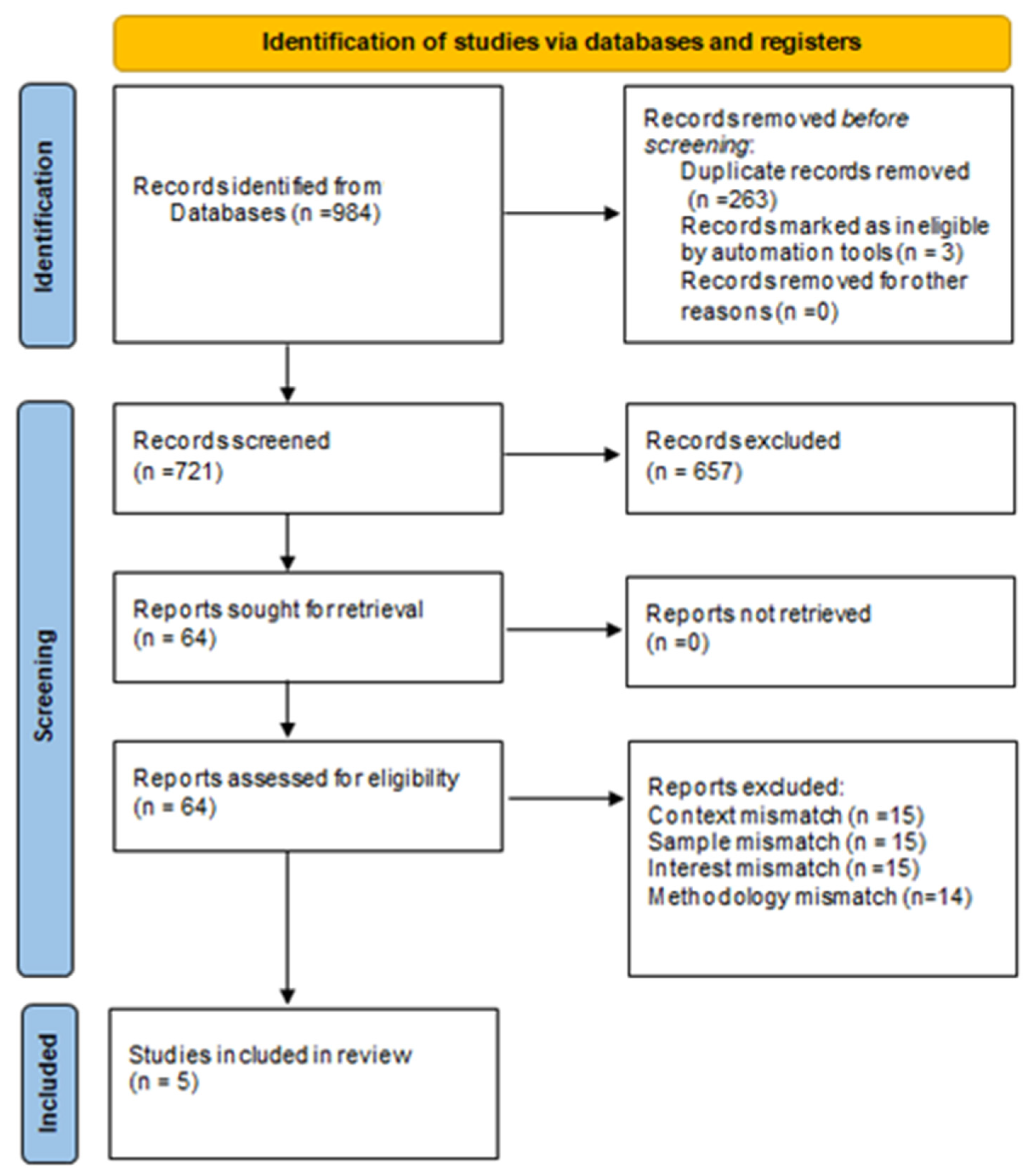
2.4. Search Results
2.5. Data Analysis
2.6. Ethical Concerns
3. Results
3.1. Quality of Evidence
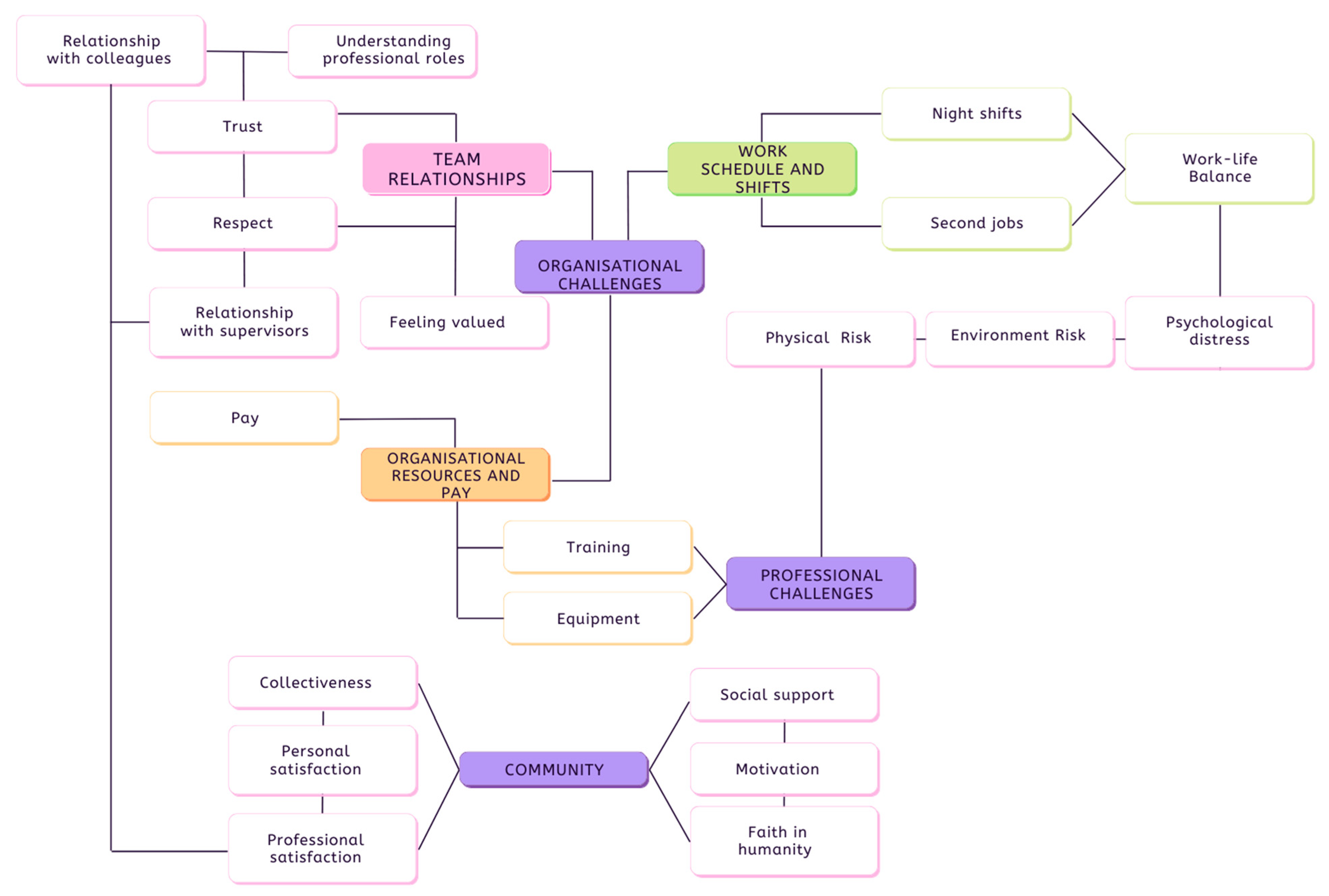
3.2. Thematic Analysis
3.2.1. Organisational Challenges
Team Relationships
“All of the participants mentioned feeling overlooked, misunderstood and marginalized. When specifically discussing the public perception, participants described feeling invisible.”[18]
Organisational Resources and Salaries
“In dispatch, the main stressors are not having the resources, in terms of ambulances for emergencies. (Jane, female, 13½ years in role).”
“Supervisors also noted that workers needed more training on waiting for help (either from another EMS team or a supervisor) and not rushing on the last call in order to go home. However, they noted there was no scheduled time for additional training on appropriate and safe work practices.”
“Initially, when asking Darren what his routine was after finishing work, he confessed to not really having a routine. As Darren explained, he often returns to work not feeling refreshed, and he now does not experience the same enjoyment in his role as he used to.”
“Low pay, work shifts, and second jobs were related according to workers. Low wages led to second jobs, but most had no choice because of their salaries.”
Work Schedules and Shifts
3.2.2. Professional Challenges
“These responses included being located in a ‘rural area’, being exposed to ‘hot weather’ and being ‘not adequately prepared for heat waves/bushfire crises.”[21]
“Once I have an injury, just one wrong move with a patient or when carrying equipment will flare me up. I can lose three months of work.” Most supervisors reported that weight and number of pieces of equipment that EMS staff and their partners carried and handled, combined with icy, wet weather were ‘headaches’.”[19]
3.2.3. Community
“Faith driven by group-identity connects to collectively created mental, spiritual and physical spaces and practices where it is ‘safe’ to confide, reflect, debate, grow and heal through interaction with people who share a common purpose, belief or relational support.”[20]
“While several respondents stated that treating personally known patients is a source of significant stress, it was also identified that this can be rewarding. This is largely due to a ‘higher expectation to perform well’ and because ‘many (patients) are known friends or family’. However, it was also reported that ‘treating personally known patients who are not in a serious condition is easier and quite rewarding’.”[21]
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Coxon et al. (2017) [18] | GRADE | ||||||||
| Methods for data collection and analysis | Qualitative methodology based on semi-structured interviews. Data analysis followed a grounded-theory approach, or bottom-up thematic, using an inductive framework for analysis. | HIGH | |||||||
| Phenomena of interest | The focus of this study was set on the unique experiences of emergency medical service (EMS) dispatch personnel, which may produce specific stressors. | ||||||||
| Setting/Context/Culture | The study was carried out in England, UK using emergency dispatch staff. | ||||||||
| Participant characteristics/sample size | Nine participants from the Emergency Operations Centre (EOC) were recruited via purposive sampling to reflect variety in years of experience, age, and gender. As the total population of EOC dispatch workers was 36, the number of participants recruited represented a quarter of this workforce. | ||||||||
| Description of main results | Theme 1: How dispatch is perceived by others | Theme 2: Sources of stress | Theme 3: Dispatch stress reducers | ||||||
| Participants felt overlooked, misunderstood and marginalised. Friends and family minimalized the importance of their professional roles. Team relationships with field EFRs were also impeded by a poor perception of dispatch roles. This led to intrapersonal conflicts and completing tasks ouside the scope of the dispatch’s role. | Participants felt a sense of purpose in their job, that they have made a difference for people in need. Lack of resources was nonetheless noted—dispatch staff was often confronted with a lack of ambulances for emergency, which increases the response time. Intrapersonal issues impaired interaction with other EFRs. Need to constantly multitask and coordinate. Lack of training. Cumulative fatigue from one day to the next. | Good training is a coping mechanism. Induces feelings of value and appreciation for the team while improving job satisfaction. Personal motivation. Seeing the difference made to people. | |||||||
| Implications for practice | Poor intra-personal relationships between dispatch staff in emergency services and filed operatives contributes significantly to job stress. Inadvertently, this may lead dispatch staff to feel undervalued and underappreciated, decreasing job satisfaction and leading to substantial turnover rates. These data indicate that organisations that run dispatch EFR services should be mindful of developing good intrapersonal relations between their dispatch staff and other EFR teams. | ||||||||
| Dropkin et al. (2015) [19] | GRADE | ||||||||
| Methods for data collection and analysis | Qualitative methodology with semi-structured interviews and focus-groups. Grounded theory thematic analysis approach. A preliminary pilot interview to guide the development for the interviews and focus-groups questions was carried. | HIGH | |||||||
| Phenomena of interest | Study explores work-related health problems for emergency medical service (EMS) workers, to identify potential risk factors at the organisational level, task-related risks, exposure risks and potential preventive strategies. | ||||||||
| Setting/Context/Culture | Study carried out in the US, in the context of role development and expansion of job attributes for EMS. | ||||||||
| Participant characteristics/sample size | EMS and supervisors recruited from the largest hospital-based ambulance service in North-East US. Ten teams were interviewed Focus-groups were carried out with 68 supervisors and 22 EMSs. Most participants were over the age of 35 years old, white, and all were men. 85% of them had back problems, and 55% rated their health as good or excellent. Musculoskeletal problems were reported by all participants. | ||||||||
| Description of main results | Theme 1: Most common physical health problems | Theme 2: Risk factors | Theme 3: Challenges for tackling these risks | ||||||
| Back pain and shoulder injuries. Other fitness issues reported. Impact on staffing and job rotation, as well as medical care. | Supervisors and EMS alike identified the work organisation as a risk factor due to work characteristics, patient characteristics and partner pair-up. These risk factors impacted training, equipment, shift hours and sometimes required having a second job. | Trust and social support at work was low. Rest and meal breaks were sparse or substandard. Financial issues. Training shortage. Additional issues reported were financial issues, hourly shifts, equipment availablility, and lack of job rewards and respect. | |||||||
| Implications for practice | Risks to physical wellbeing seem to derive from work specificities for EFRs. The way in which organisations can mitigate these risks is by screening employees for fitness before hire, providing adequate training and equipment. To mitigate psychosocial risks, organisations could enable partnerships in shift working between people who can work together well, schedule shifts to allow sufficient rest days, and allow for rest breaks and meals. | ||||||||
| Eriksen (2019) [20] | GRADE | ||||||||
| Methods for data collection and analysis | Qualitative methodology based on semi-structured interviews and focus groups, and analysed via the thematic coding software NVivo. | HIGH | |||||||
| Phenomena of interest | The experiences of emergency workers in coping, caring and believing during disaster recovery. Investigation is centred around three concepts: faith as performativity, embodiment and the holding environment, as components of a system that regulates coping capacity. Faith in this context does not reflect religious belief, but rather inter-group relations in crisis situations. | ||||||||
| Setting/Context/Culture | Disaster recovery workers from Australia. Participants had work experience in New South Wales or Victoria, and were faith leaders, group supervisors, recovery coordinators, volunteers and community care workers | ||||||||
| Participant characteristics/sample size | 18 people working in disaster recovery for the interviews, plus another sample of 33 participants for focus-groups. | ||||||||
| Description of main results | Theme 1: Risk management of formative tensions | Theme 2: Embodying work and modalities of faith | |||||||
| Self-care and coping strategies | Points of exposure to harm | Spiritual Response | Psychological and physiological response | ||||||
| Having a sense of prioritising and experiential knowledge. Training, debriefing, safe-space and ability to ask for help. Leadership and group communication. Adaptability under pressure. Disasters elicit a sense of community. | Prolonged exposure to risks and organisational pressures. Conflicting views. Limited listening from leaders and co-workers. Control-based power dynamics. Negative sensory experiences. Trigger points. Isolation. Personal impacts. A small group of participants mentioned media and news reading as sources of harm, due to dramatic approach of disaster coverage. | Feeling a sense of connectedness coming from a love for humanity. Religious beliefs. Religion as a way to cope with stress. Innate resilience, and spirituality. | In the context of disasters, the feelings of connectedness and spirituality seemed to promote actions of providing support to others but also feelings of being overwhelmed, overloaded and fragile. Inadequacies in the intervention, limited resources as well as frustrations were also reported. For some participants, disaster work also produced changes in their weight, increases in adrenalin and burnout. | ||||||
| Implications for practice | The holding environment, described as the cultural and physical space in which the disaster occurs, seems to influence the ability of disaster recovery workers to cope with the effects of being exposed to these events. Disasters seem to naturally cause a greater sense of community among people and by this, elicit interventional responses, albeit with some psychological and physiological costs to the disaster worker. Organisations can therefore foster this sense of community, spirituality and social support to increase coping skills in their work force. Study recommends a coping model based around individual grounded faith and faith that is collectively created. | ||||||||
| Paterson et al. (2014) [21] | GRADE | ||||||||
| Methods for data collection and analysis | Mixed-methods approach following a survey design combined with three additional open-ended questions. Quantitative data was analysed via descriptive means. Qualitative data analysed via systematic coding and theme extraction. | HIGH | |||||||
| Phenomena of interest | How fatigue is perceived by paramedics and what factors are thought to contribute to fatigue. | ||||||||
| Setting/Context/Culture | Study was carried out in Australia, using a sample of paramedics. | ||||||||
| Participant characteristics/sample size | 49 paramedics were included in the study. 20 worked in ambulance services for 5 to 10 years. 12 worked in the ambulance service for 10 to 15 years. 7 participants had been employed in the service for less than 5 years. 7 had been employed for more than 20 years. | ||||||||
| Description of main results | Theme 1: Working Time | Theme 2: Sleep | Theme 3: Workload | Theme 4: Health and Wellbeing | Theme 5: Work–life Environment | ||||
| Night shifts are the main cause of fatigue. Associated with performance impairments in the absence of breaks. | Difficulty sleeping outside night shifts, particularly before the night shift. Imbalanced circadian rhythm. Poor home environment. Sleep interruptions. | Increased work load was also reported as a contributor to fatigue, yet this was more pronounced doing night shifts where activity seemed to be more intense. | Exhaustion and mood swings exacerbated by poor diets and limited exercise time leading to weight gain. | Living in a rural area associated with being fatigued due to commute. Increased heath waves and bushfire incidents contribute to fatigue. Poor work–life balance: participants had to work their way around family responsibility, work and learning. | |||||
| Implications for practice | By acknowledging fatigue factors among their staff, organisations can develop interventional models to mitigate or eliminate these factors. The implementation of such as system would potentially be complex, as initially organisational research would have to be conducted to identify sources of fatigue, and interventions developed based on the attained results. | ||||||||
| Pyper and Paterson (2016) [22] | GRADE | ||||||||
| Methods for data collection and analysis | Mixed-methods approach to assess levels of fatigue, stress and emotional trauma in rural and regional ambulance personnel. Fatigue was assessed via the Chalder’s Fatigue Questionnaire (CFQ). Depression was assessed by using the Depression Anxiety Stress Scale (DASS-21), and emotional trauma was assessed via the Impact of Event Scale (IES). Data analysed via descriptive statistics as well as qualitative coding of open-end questions. | HIGH | |||||||
| Phenomena of interest | The study sought to determine if similar levels of fatigue and stress are present within rural and regional ambulance staff. | ||||||||
| Setting/Context/Culture | The investigation was carried out in Australia. | ||||||||
| Participant characteristics/sample size | The sample consisted of 134 ambulance workers from regional and rural areas. | ||||||||
| Description of main results | Theme 1: Fatigue | Theme 2: Stressors | |||||||
| High levels of fatigue and emotional trauma reported by ambulance staff working in rural and regional areas, despite serving a lower population when compared to urban ambulance staff. | Unique stressors include having to provide emergency medical services to people that are personally known by ambulance staff. However, personal involvement may also increase professionalism and care. | ||||||||
| Implications for practice | Organisations managing emergency first responses in rural and regional areas should be aware of the fact that workload is not the only factor affecting fatigue, stress and emotional trauma in their staff. | ||||||||
Appendix B
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Coxon et al., 2017 [18] | Y | Y | Y | Y | Y | U | U | Y | Y | Y |
| Dropkin et al., 2015 [19] | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| Eriksen (2019) [20] | Y | Y | Y | Y | Y | U | U | Y | Y | Y |
| Study Title | Synthesised Findings | Type of Research | Dependability (2, 3, 4, 6, 7) | Credibility | ConQual Score |
|---|---|---|---|---|---|
| Coxon et al., 2017 [18] | Underlines the importance of dispatch staff and their wellbeing for EFR. Dispatch staff feel underappreciated which may cause tensions between teams. | Qualitative (high) | Unchanged | Unequivocal | HIGH |
| Dropkin et al., 2015 [19] | Working in medical EFR professions is often associated with musculoskeletal problems and poor mental wellbeing. The ability to choose a work partner and physical training and testing may moderate these effects. | Qualitative (high) | Unchanged | Unequivocal | HIGH |
| Eriksen, 2019 [20] | Lack of knowledge or understanding of BSE. The holding environment in these circumstances seems to be formed by risk exposures (stakeholders, resources, cultural norms, politics and demographic), and care and coping strategies (care framework, belief framework, job appeal and modifies). Faith divided between individual grounded faith and faith that is collectively created. Response to disasters within the holding environment seems to be characterised by physical, psychological and spiritual effects. | Qualitative (high) | Unchanged | Unequivocal | HIGH |
| Study | Questions | Yes | No | Can’t Tell | Comments |
| Paterson et al., 2014 [21] | Is there an adequate rationale for using a mixed methods design to address the research question? | ✓ | |||
| Are the different components of the study effectively integrated to answer the research question? | ✓ | ||||
| Are the outputs of the integration of qualitative and quantitative components adequately interpreted? | ✓ | ||||
| Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? | N/A | ||||
| Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? | ✓ | ||||
| Study | Questions | Yes | No | Can’t Tell | Comments |
| Pyper and Paterson 2016 [22] | Is there an adequate rationale for using a mixed methods design to address the research question? | ✓ | |||
| Are the different components of the study effectively integrated to answer the research question? | ✓ | ||||
| Are the outputs of the integration of qualitative and quantitative components adequately interpreted? | ✓ | ||||
| Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? | N/A | ||||
| Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? | ✓ |
| Study | Summary of Findings | Category Definition | Grade Score |
|---|---|---|---|
| Paterson et al. (2014) [21] | Paramedics have a good understanding of fatigue and its sources. Organisational research into these causes can form the basis of interventions meant to reduce fatigue | True effect lies close to estimate effect. Further research is unlikely to change confidence in estimate effect. | HIGH |
| Pyper and Paterson (2016) [22] | There are unique and complex challenges faced by rural ambulance staff. These include social pressures for caring for people whom they know, as well as limited resources. | True effect lies close to estimate effect. Further research is unlikely to change confidence in estimate effect. | HIGH |
References
- Sharp, M.-L.; Harrison, G.; Solomon, N.; Fear, N.; King, H.; Pike, G. Assessing the Mental Health and Wellbeing of the Emergency Responder Community in the UK; Open University and Kings College London: London, UK, 2020. [Google Scholar]
- Queirós, C.; Passos, F.; Bártolo, A.; Marques, A.J.; da Silva, C.F.; Pereira, A. Burnout and Stress Measurement in Police Officers: Literature Review and a Study With the Operational Police Stress Questionnaire. Front. Psychol. 2020, 11, 587. [Google Scholar] [CrossRef] [PubMed]
- Hamdan, M.; Hamra, A.A. Burnout among Workers in Emergency Departments in Palestinian Hospitals: Prevalence and Associated Factors. BMC Health Serv. Res. 2017, 17, 407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guise, J.-M.; Hansen, M.; O’brien, K.; Dickinson, C.; Meckler, G.; Engle, P.; Lambert, W.; Jui, J. Emergency Medical Services Responders’ Perceptions of the Effect of Stress and Anxiety on Patient Safety in the out-of-Hospital Emergency Care of Children: A Qualitative Study. BMJ Open 2017, 7, 14057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilal, S.; Litsey, B. Reducing Police Turnover: Recommendations for the Law Enforcement Agency. Int. J. Police Sci. Manag. 2020, 22, 73–83. [Google Scholar] [CrossRef]
- Rice, V.; Glass, N.; Ogle, K.R.; Parsian, N. Exploring Physical Health Perceptions, Fatigue and Stress among Health Care Professionals. J. Multidiscip. Healthc. 2014, 7, 155–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumberg, D.M.; Giromini, L.; Papazoglou, K.; Thornton, A.R. Impact of The HEROES Project on First Responders’ Well-Being. J. Community Saf. Well-Being 2020, 5, 8. [Google Scholar] [CrossRef]
- Dodge, R.; Daly, A.; Huyton, J.; Sanders, L. The Challenge of Defining Wellbeing. Int. J. Wellbeing 2012, 2, 222–235. [Google Scholar] [CrossRef] [Green Version]
- Mansfield, L.; Daykin, N.; Kay, T. Leisure and Wellbeing. Leis. Stud. 2020, 39, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Bodeker, G.; Pecorelli, S.; Choy, L.; Guerra, R.; Kariippanon, K. Well-Being and Mental Wellness. In Oxford Research Encyclopedia of Global Public Health; Oxford University Press: Oxford, UK, 2020. [Google Scholar] [CrossRef]
- Joyce, S.; Shand, F.; Lal, T.J.; Mott, B.; Bryant, R.A.; Harvey, S.B. Resilience@Work Mindfulness Program: Results from a Cluster Randomized Controlled Trial with First Responders. J. Med. Internet Res. 2019, 21, e12894. [Google Scholar] [CrossRef] [PubMed]
- Wild, J.; El-Salahi, S.; Esposti, M.D.; Thew, G.R. Evaluating the Effectiveness of a Group-Based Resilience Intervention versus Psychoeducation for Emergency Responders in England: A Randomised Controlled Trial. PLoS ONE 2020, 15, e0241704. [Google Scholar] [CrossRef] [PubMed]
- Bettany-Saltikov, J. How to Do a Systematic Literature Review in Nursing: A Step-by-Step Guide, 2nd ed.; McSherry, R., Ed.; Open University Press: London, UK, 2016. [Google Scholar]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 1st ed.; John Wiley & Sons: Chichester, UK, 2008. [Google Scholar] [CrossRef]
- Booth, A.; Sutton, A.; Papaioannou, D. Systematic Approaches to a Successful Review, 2nd ed.; Sage: London, UK, 2016. [Google Scholar]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar] [CrossRef]
- Gough, D.; Oliver, S.; Thomas, J. (Eds.) An Introduction to Systematic Reviews, 2nd ed.; SAGE: London, UK, 2017. [Google Scholar]
- Coxon, A.; Cropley, M.; Schofield, P.; Start, K.; Horsfield, C.; Quinn, T. “You’re Never Making Just One Decision”: Exploring the Lived Experiences of Ambulance Emergency Operations Centre Personnel. Emerg. Med. J. 2017, 33, 645–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dropkin, J.; Moline, J.; Power, P.M.; Kim, H. A Qualitative Study of Health Problems, Risk Factors, and Prevention among Emergency Medical Service Workers. Work 2015, 52, 935–951. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, C. Coping, Caring and Believing: The Embodied Work of Disaster Recovery Workers. Emot. Space Soc. 2019, 32, 100592. [Google Scholar] [CrossRef]
- Paterson, J.L.; Sofianopoulos, S.; Williams, B. What Paramedics Think about When They Think about Fatigue: Contributing Factors. EMA-Emerg. Med. Australas. 2014, 26, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Pyper, Z.; Paterson, J.L. Fatigue and Mental Health in Australian Rural and Regional Ambulance Personnel. EMA-Emerg. Med. Australas. 2016, 28, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.; Grove, S.K.; Sutherland, S. Burns and Grove’s the Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence, 8th ed.; Elsevier: St. Louis, MO, USA, 2017. [Google Scholar]
- LoBiondo-Wood, G.; Haber, J. Nursing Research: Methods and Critical Appraisal for Evidence-Based Practice, 8th ed.; Mosby Elsevier: St. Louis, MO, USA, 2014. [Google Scholar]
- Joanna Briggs Institute. Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 19 April 2022).
- Hong, Q.N.; Gonzalez-Reyes, A.; Pluye, P. Improving the Usefulness of a Tool for Appraising the Quality of Qualitative, Quantitative and Mixed Methods Studies, the Mixed Methods Appraisal Tool (MMAT). J. Eval. Clin. Pract. 2018, 24, 459–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guest, G.; MacQueen, K.M.; Namey, E.E. Applied Thematic Analysis; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2012. [Google Scholar] [CrossRef]
- Onwuegbuzie, A.J.; Frels, R. 7 Steps to a Comprehensive Literature Review: A Multimodal and Cultural Approach; SAGE: London, UK, 2016. [Google Scholar]
- Arble, E.; Daugherty, A.M.; Arnetz, B.B. Models of First Responder Coping: Police Officers as a Unique Population. Stress Health 2018, 34, 612–621. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.D.; Mullins-Jaime, C.; Dyal, M.A.; DeJoy, D.M. Stress, Burnout and Diminished Safety Behaviors: An Argument for Total Worker Health® Approaches in the Fire Service. J. Saf. Res. 2020, 75, 189–195. [Google Scholar] [CrossRef] [PubMed]


| Population | Emergency responders across all domains (fire, police, emergency first responders) |
| Interest | Emergency and crisis situations, flooding, psychological, wellbeing |
| Context | Primary context: UK, United Kingdom, England, Wales, Scotland, Northern, and Ireland. Secondary Context: Europe, USA, Australia, and Canada. |
| Inclusion | Exclusion |
|---|---|
| Study sample includes all categories of emergency response personnel: fire-fighters, ambulance staff, police staff, medical staff responding to crisis, and dispatcher for emergency situation calls. | Study sample is not specific to EFR. This may include students in training for becoming EFR, medical staff in local hospitals unrelated to community crisis situations, or dispatch for suicide help lines. |
| If other staff is included in the research, then data for EFR is separately reported and analysed. | Studies including volunteers as emergency first responders, or studies for which professional EFR samples have not been separately analysed. |
| Studies assessing contribution factors to wellbeing deterioration among EFR. | Studies assessing the prevalence of cautions caused by exposure to crisis situations in EFR. |
| Studies assessing, wellbeing as related to professional/organisational, emotional, physical and psychological wellbeing. | Studies focusing on wellbeing domains outside the context of emergency situations. |
| Studies assessing interventions to improve all or one aspect of wellbeing for EFR attending crisis situations. | Studies focusing on interventions to improve response times in EFR or procedural interventions. |
| Studies assessing the impact of crisis situations on EFRs wellbeing. | Studies assessing the impact of crisis situations on local populations. |
| Published within the past 20 years. | Published before 2002. |
| Published in English. | Published in a language other than English. |
| Empirical study/primary research. | Secondary research studies/commentary articles. |
| Qualitative and mixed-methods studies | Quantitative articles |
| Databases | |||
|---|---|---|---|
| Keywords | Science Direct | PubMed | ProQuest |
| Emergency responders’ wellbeing/welfare | 205 | 4 | 7 |
| Ambulance first responders’ wellbeing/welfare | 249 | 1 | 5 |
| Police first responders’ wellbeing/welfare | 259 | 2 | 2 |
| Fire-fighters first responders’ wellbeing/welfare | 245 | 2 | 3 |
| Total: 984 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bevan, M.P.; Priest, S.J.; Plume, R.C.; Wilson, E.E. Emergency First Responders and Professional Wellbeing: A Qualitative Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 14649. https://doi.org/10.3390/ijerph192214649
Bevan MP, Priest SJ, Plume RC, Wilson EE. Emergency First Responders and Professional Wellbeing: A Qualitative Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(22):14649. https://doi.org/10.3390/ijerph192214649
Chicago/Turabian StyleBevan, Malcolm P., Sally J. Priest, Ruth C. Plume, and Emma E. Wilson. 2022. "Emergency First Responders and Professional Wellbeing: A Qualitative Systematic Review" International Journal of Environmental Research and Public Health 19, no. 22: 14649. https://doi.org/10.3390/ijerph192214649