

Voting with Your Feet: The Impact of Urban Public Health Service Accessibility on the Permanent Migration Intentions of Rural Migrants in China

Abstract
:1. Introduction
2. Literature and Hypotheses
2.1. Literature Review
2.2. Research Hypotheses
3. Materials and Methods
3.1. Data
3.2. Variables
3.3. Empirical Strategies
3.3.1. Main Effects Model
3.3.2. Instrument Variable Method
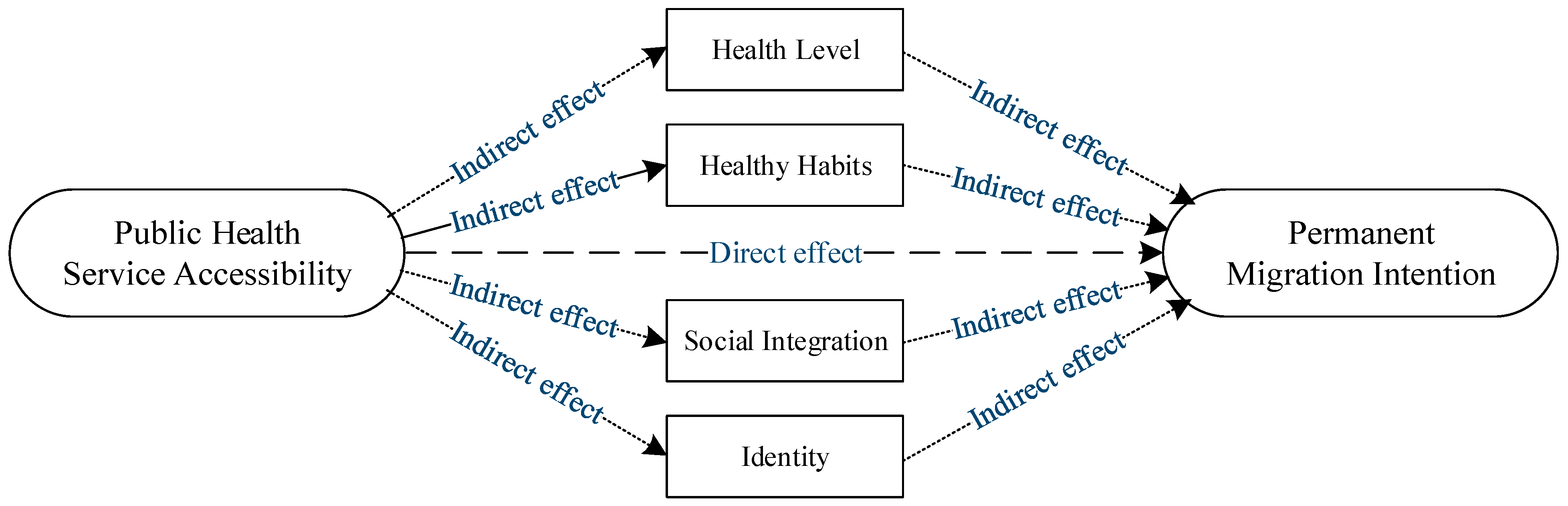
3.3.3. Mediation Effect Model
4. Empirical Analysis
4.1. Baseline Regression Results
4.2. Endogeneity
4.2.1. Instrument Variable Result
4.2.2. Omitted Variables Checks
4.3. Robustness
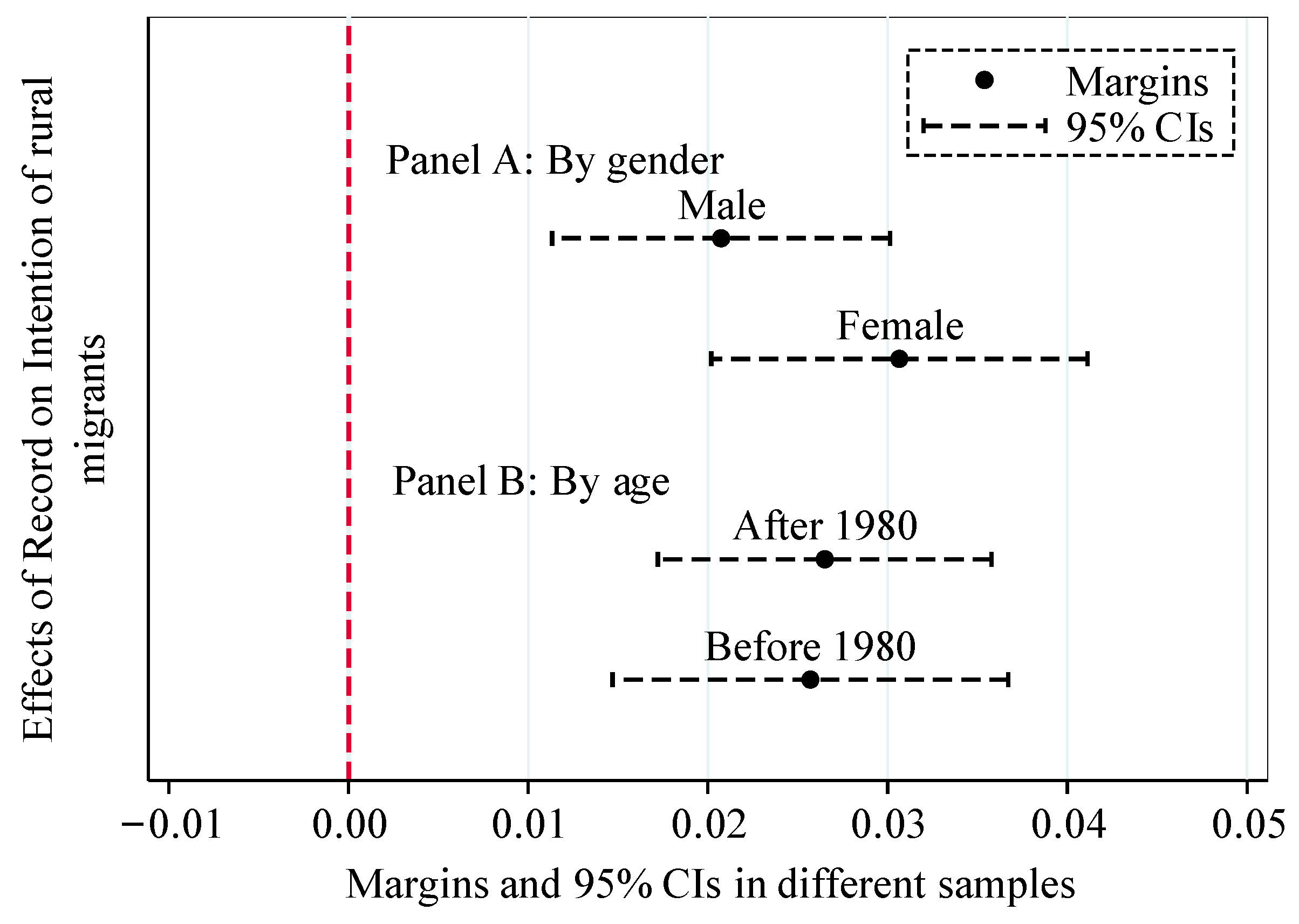
4.4. Heterogeneous Effects
4.5. Analysis of Mediating Effect
5. Discussion
6. Conclusions and Policy Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variables | Value | Mean | Std. |
|---|---|---|---|
| PMI | Registered permanent residence or permanent settlement in the current city. 1 = Yes, 0 = No | 0.447 | 0.497 |
| PHSA | Is a resident health file established? 1 = Established, 0 = Other | 0.277 | 0.447 |
| Gender | 1 = Male, 0 = Female | 0.569 | 0.495 |
| Age | Respondent’s age in 2017 (years) | 36.033 | 9.828 |
| Marriage | 1 = Married, 0 = Unmarried | 0.841 | 0.365 |
| Education | 1 = High school and above, 0 = Below high school | 0.322 | 0.467 |
| Migration range | 1 = Inter-provincial mobility, 2 = Intra-provincial inter-city, 3 = Intra-city inter-county | 1.666 | 0.752 |
| Residence time | Duration of residence in the city (years) | 6.214 | 5.924 |
| Income | Logged family per capita income (Yuan) | 7.594 | 0.693 |
| Medicare | 1 = Yes, 0 = No | 0.203 | 0.402 |
| Occupation | 1 = Self-employed, 0 = Other | 0.388 | 0.487 |
| Family size | Number of family members living together | 3.190 | 1.177 |
| GDP | Logged GDP per capita in the current city of residence in 2016 (Yuan) | 11.183 | 0.495 |
| City size | The city size of the current city of residence. 1 =< 1 million, 2 = 1–5 million, 3 = 5–10 million, 4 => 10 million | 2.016 | 0.928 |
| Key cities | Key cities for equalization of basic public services for migrant population. 1 = Yes, 0 = No | 0.437 | 0.496 |
| Healthy habits | My personal hygiene habits are not different from those of local citizens. 1 = Yes, 0 = No | 0.796 | 0.403 |
| Health level | Self-reported health. 1 = Unable to take care of himself, 2 = Unhealthy, but life can be self, 3 = Basically healthy, 4 = Healthy | 3.811 | 0.444 |
| Identity | I am already a local resident. 1 = Yes, 0 = No | 0.734 | 0.442 |
| Social Integration | I am willing to integrate into this city. 1 = Yes, 0 = No | 0.924 | 0.264 |
| No. | Province | City | No. | Province | City |
|---|---|---|---|---|---|
| 1 | Beijing | Chaoyang | 23 | Fujian | Xiamen |
| 2 | Fengtai | 24 | Quanzhou | ||
| 3 | Tianjin | Binhai | 25 | Jiangxi | Nanchang |
| 4 | Jinan | 26 | Shandong | Qingdao | |
| 5 | Hebei | Shijiazhuang | 27 | Henan | Zhengzhou |
| 6 | Shanxi | Taiyuan | 28 | Hubei | Wuhan |
| 7 | Inner Mongolia | Baotou | 29 | Hunan | Changsha |
| 8 | Liaoning | Dalian | 30 | Guangdong | Shenzhen |
| 9 | Jilin | Changchun | 31 | Zhongshan | |
| 10 | Heilongjiang | Harbin | 32 | Guangxi | Guilin |
| 11 | Shanghai | Minhang | 33 | Hainan | Sanya |
| 12 | Yangpu | 34 | Chongqing | Yubei | |
| 13 | Songjiang | 35 | Sichuan | Chengdu | |
| 14 | Baoshan | 36 | Guizhou | Guiyang | |
| 15 | Jiangsu | Nanjing | 37 | Yunnan | Yuxi |
| 16 | Suzhou | 38 | Tibet | Lhasa | |
| 17 | Wuxi | 39 | Shaanxi | Xi ’an | |
| 18 | Zhejiang | Hangzhou | 40 | Xianyang | |
| 19 | Ningbo | 41 | Gansu | Lanzhou | |
| 20 | Jiaxing | 42 | Qinghai | Xining | |
| 21 | Shaoxing | 43 | Ningxia | Yinchuan | |
| 22 | Anhui | Hefei | 44 | Xinjiang | Karamay |
| Variables | Male | Female | After 1980 | Before 1980 | ||||
|---|---|---|---|---|---|---|---|---|
| Coef. | Margins | Coef. | Margins | Coef. | Margins | Coef. | Margins | |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | |
| PHSA | 0.055 *** | 0.021 *** | 0.083 *** | 0.031 *** | 0.071 *** | 0.027 *** | 0.069 *** | 0.026 *** |
| (0.013) | (0.005) | (0.014) | (0.005) | (0.013) | (0.005) | (0.015) | (0.006) | |
| Constant | −2.807 *** | −3.108 *** | −3.560 *** | −2.182 *** | ||||
| (0.172) | (0.204) | (0.182) | (0.191) | |||||
| Control variables | YES | YES | YES | YES | ||||
| Pseudo R2 | 0.046 | 0.054 | 0.083 | 0.026 | ||||
| Suest test | 120.550 *** | 296.950 *** | ||||||
| Observations | 52,347 | 52,347 | 39,655 | 39,655 | 51,833 | 51,833 | 37,325 | 37,325 |
References
- Kohlenberger, J.; Buber-Ennser, I.; Rengs, B.; Leitner, S.; Landesmann, M. Barriers to health care access and service utilization of refugees in Austria: Evidence from a cross-sectional survey. Health Policy 2019, 123, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Long, C.; Tang, S.; Wang, R.; Ji, L.; Wang, Y.; Wu, T.; Li, Z.; Feng, Z. The migrating mediators and the interaction associated with the use of essential public health services: A cross-sectional study in Chinese older migrants. BMC Geriatr. 2020, 20, 475. [Google Scholar] [CrossRef] [PubMed]
- Fauk, N.K.; Ziersch, A.; Gesesew, H.; Ward, P.; Green, E.; Oudih, E.; Tahir, R.; Mwanri, L. Migrants and Service Providers’ Perspectives of Barriers to Accessing Mental Health Services in South Australia: A Case of African Migrants with a Refugee Background in South Australia. Int. J. Environ. Res. Public Health 2021, 18, 8906. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Yu, Q.; Wang, X.; Shi, P.; Shen, Q.; Zhang, Z.; Chen, Z.; Pu, C.; Xu, L.; Hu, Z.; et al. Are Essential Women’s Healthcare Services Fully Covered? A Comparative Analysis of Policy Documents in Shanghai and New York City from 1978–2017. Int. J. Environ. Res. Public Health 2021, 18, 4261. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Xie, Y.; Zhou, D. Air pollution’s impact on the settlement intention of domestic migrants: Evidence from China. Environ. Impact Assess. Rev. 2022, 95, 106761. [Google Scholar] [CrossRef]
- Meng, X. Does a Different Household Registration Affect Migrants’ Access to Basic Public Health Services in China? Int. J. Environ. Res. Public Health 2019, 16, 4615. [Google Scholar] [CrossRef] [Green Version]
- Ren, Y.; Zhou, Z.; Cao, D.; Ma, B.H.; Shen, C.; Lai, S.; Chen, G. Did the Integrated Urban and Rural Resident Basic Medical Insurance Improve Benefit Equity in China? Value Health 2022, 25, 1548–1558. [Google Scholar] [CrossRef]
- Chen, Y.; Parker, M.; Zheng, X.; Fang, X. Health Insurance Coverage of Migrant Workers in China. Chin. Econ. 2022, 55, 332–342. [Google Scholar] [CrossRef]
- Liu, W.-M.; Ngo, P. Voting with your feet: Political competition and internal migration in the United States. Eur. J. Political Econ. 2020, 65, 101931. [Google Scholar] [CrossRef]
- Cheng, M.; Duan, C. The changing trends of internal migration and urbanization in China: New evidence from the seventh National Population Census. China Popul. Dev. Stud. 2021, 5, 275–295. [Google Scholar] [CrossRef]
- Yang, K.; Peng, H.; Chen, J. Social Citizenship Rights and Responsibilities: A Survey of Rural Migrant Workers’ Attitudes in China. China Rev. 2022, 22, 171–199. [Google Scholar]
- Tiebout, C.M. A Pure Theory of Local Expenditures. J. Political Econ. 1956, 64, 416–424. [Google Scholar] [CrossRef]
- Hu, X.; Sun, M.; Tang, S.; Lommel, L.L. Frequency of basic public health services utilization by married female migrants in China: Associations of social support, discrimination and sociodemographic factors. BMC Womens Health 2021, 21, 344. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Huang, T.; Li, A.; Wang, Z. Does universal health insurance coverage reduce unmet healthcare needs in China? Evidence from the National Health Service Survey. Int. J. Equity Health 2021, 20, 43. [Google Scholar] [CrossRef] [PubMed]
- Bollini, P.; Siem, H. No real progress towards equity: Health of migrants and ethnic minorities on the eve of the year 2000. Soc. Sci. Med. 1995, 41, 819–828. [Google Scholar] [CrossRef]
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and health in an increasingly diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Qin, J.M. Progress in basic public health service projects in China. Chin. J. Public Health 2017, 33, 1289–1297. [Google Scholar] [CrossRef]
- Liu, Z.; Xiao, Y.; Zhao, K. Implementation progress and effect of National Essential Public Health Services Program in China. Chin. J. Public Health 2019, 35, 657–664. [Google Scholar] [CrossRef]
- Zhang, J.; Lin, S.; Liang, D.; Qian, Y.; Zhang, D.; Hou, Z. Public Health Services Utilization and Its Determinants among Internal Migrants in China: Evidence from a Nationally Representative Survey. Int. J. Environ. Res. Public Health 2017, 14, 1002. [Google Scholar] [CrossRef] [Green Version]
- Jing, Z.; Wang, Y.; Ding, L.; Tang, X.; Feng, Y.; Zhou, C. Effect of social integration on the establishment of health records among elderly migrants in China: A nationwide cross-sectional study. BMJ Open 2019, 9, e034255. [Google Scholar] [CrossRef] [Green Version]
- Tang, S.; Long, C.; Wang, R.; Liu, Q.; Feng, D.; Feng, Z. Improving the utilization of essential public health services by Chinese elderly migrants: Strategies and policy implication. J. Glob. Health 2020, 10, 010807. [Google Scholar] [CrossRef] [PubMed]
- Piore, M.J. Labor Market Segmentation: To What Paradigm Does It Belong? Am. Econ. Rev. 1983, 73, 249–253. [Google Scholar]
- Lewis, W.A. Economic Development with Unlimited Supplies of Labour. Manch. Sch. 1954, 22, 139–191. [Google Scholar] [CrossRef]
- Lee, E.S. A theory of migration. Demography 1966, 3, 47–57. [Google Scholar] [CrossRef]
- Todaro, M.P. A Model of Labor Migration and Urban Unemployment in Less Developed Countries. Am. Econ. Rev. 1969, 59, 138–148. [Google Scholar]
- Stark, O.; Levhari, D. On Migration and Risk in LDCs. Econ. Dev. Cult. Chang. 1982, 31, 191–196. [Google Scholar] [CrossRef]
- Stark, O.; Bloom, D.E. The New Economics of Labor Migration. Am. Econ. Rev. 1985, 75, 173–178. [Google Scholar]
- Wang, Y.; Zhu, Z.; Wang, Z.; Xu, Q.; Zhou, C. Household Registration, Land Property Rights, and Differences in Migrants’ Settlement Intentions—A Regression Analysis in the Pearl River Delta. Land 2022, 11, 31. [Google Scholar] [CrossRef]
- Li, P.; Wu, Y.; Ouyang, H. Effect of hukou Accessibility on Migrants’ Long Term Settlement Intention in Destination. Sustainability 2022, 14, 7209. [Google Scholar] [CrossRef]
- Song, Y.; Zhu, N.; Luo, F. City Size and Permanent Settlement Intention: Evidence from Rural-Urban Migrants in China. Int. J. Environ. Res. Public Health 2022, 19, 676. [Google Scholar] [CrossRef]
- Imbert, C.; Papp, J. Costs and benefits of rural-urban migration: Evidence from India. J. Dev. Econ. 2020, 146, 102473. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Zhu, Y. Types and determinants of migrants’ settlement intention in China’s new phase of urbanization: A multi-dimensional perspective. Cities 2022, 124, 103622. [Google Scholar] [CrossRef]
- Huang, X.; Chen, M. Understanding the role of housing in rural migrants’ intention to settle in cities: Evidence from China. Habitat Int. 2022, 128, 102650. [Google Scholar] [CrossRef]
- Chen, S.; Oliva, P.; Zhang, P. The effect of air pollution on migration: Evidence from China. J. Dev. Econ. 2022, 156, 102833. [Google Scholar] [CrossRef]
- Liu, R.; Greene, R.; Yu, Y.; Lv, H. Are migration and settlement environment-driven? Environment-related residential preferences of migrants in China. J. Clean. Prod. 2022, 377, 134263. [Google Scholar] [CrossRef]
- Wang, C.; Shen, J. Settlement intention of migrants in urban China: The effects of labor-market performance, employment status, and social integration. Appl. Geogr. 2022, 147, 102773. [Google Scholar] [CrossRef]
- Tezcan, T. Return home? Determinants of return migration intention amongst Turkish immigrants in Germany. Geoforum 2019, 98, 189–201. [Google Scholar] [CrossRef]
- Liu, T.; Xiao, W. The ‘intention to stay’ of the floating migrant population: A spatiotemporal meta-analysis in Chinese cities. Popul. Space Place 2022, 28, e2574. [Google Scholar] [CrossRef]
- Wang, C.; Zhang, C.; Ni, J.; Zhang, H.; Zhang, J. Family migration in China: Do migrant children affect parental settlement intention? J. Comp. Econ. 2019, 47, 416–428. [Google Scholar] [CrossRef]
- Zou, J.; Chen, J.; Chen, Y. Hometown landholdings and rural migrants’ integration intention: The case of urban China. Land Use Policy 2022, 121, 106307. [Google Scholar] [CrossRef]
- Zhou, J.; Lin, L.; Tang, S.; Zhang, S. To settle but not convert hukou among rural migrants in urban China: How does family-level eligibility for citizenship benefits matter? Habitat Int. 2022, 120, 102511. [Google Scholar] [CrossRef]
- Liu, T.; Peng, R.; Cao, G. Stay or leave: How migrants respond to dispersal policies in Beijing. Popul. Space Place 2022, e2606. [Google Scholar] [CrossRef]
- Pollakowski, H.O. The Effects of Property Taxes and Local Public Spending on Property Values: A Comment and Further Results. J. Political Econ. 1973, 81, 994–1003. [Google Scholar] [CrossRef]
- Wu, F.; Logan, J. Do rural migrants ‘float’ in urban China? Neighbouring and neighbourhood sentiment in Beijing. Urban Stud. 2016, 53, 2973–2990. [Google Scholar] [CrossRef]
- Liang, J.; Shi, Y.; Osman, M.; Shrestha, B.; Wang, P. The Association between Social Integration and Utilization of Essential Public Health Services among Internal Migrants in China: A Multilevel Logistic Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6524. [Google Scholar] [CrossRef] [PubMed]
- Yang, X. Household Registration, Economic Reform and Migration. Int. Migr. Rev. 1993, 27, 796–818. [Google Scholar] [CrossRef]
- Chan, K.W.; Zhang, L. The Hukou System and Rural-Urban Migration in China: Processes and Changes. China Q. 1999, 160, 818–855. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, A.; Goldstein, S. Migration in China: Methodological and Policy Challenges. Soc. Sci. Hist. 1987, 11, 85–104. [Google Scholar] [CrossRef]
- Song, Y.; Zhu, N. Does Natural Amenity Matter on the Permanent Settlement Intention? Evidence from Elderly Migrants in Urban China. Int. J. Environ. Res. Public Health 2022, 19, 1022. [Google Scholar] [CrossRef]
- Oster, E. Unobservable Selection and Coefficient Stability: Theory and Evidence. J. Bus. Econ. Stat. 2019, 37, 187–204. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Karlson, K.B.; Holm, A.; Breen, R. Comparing Regression Coefficients Between Same-sample Nested Models Using Logit and Probit: A New Method. Sociol. Methodol. 2012, 42, 286–313. [Google Scholar] [CrossRef]
- Chen, F.; Zheng, M.; Xu, J.; Hall, B.J.; Pan, Y.; Ling, L.; Chen, W. Impact of migration status on incidence of depression in the middle-aged and elderly population in China: Exploring healthy migrant and salmon bias hypotheses from a mental health perspective. J. Affect. Disord. 2022, 315, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Boas, I.; de Pater, N.; Furlong, B.T. Moving beyond stereotypes: The role of gender in the environmental change and human mobility nexus. Clim. Dev. 2022, 1–9. [Google Scholar] [CrossRef]
- Liu, Y.; Deng, W.; Song, X. Influence factor analysis of migrants’ settlement intention: Considering the characteristic of city. Appl. Geogr. 2018, 96, 130–140. [Google Scholar] [CrossRef]
- de Haas, H. A theory of migration: The aspirations-capabilities framework. Comp. Migr. Stud. 2021, 9, 8. [Google Scholar] [CrossRef]
- Qin, L.; Chen, C.-P.; Wang, W.; Chen, H. How migrants get integrated in urban China—The impact of health insurance. Soc. Sci. Med. 2021, 272, 113700. [Google Scholar] [CrossRef]
- Chen, J.; Wang, W. Economic incentives and settlement intentions of rural migrants: Evidence from China. J. Urban Aff. 2019, 41, 372–389. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Wang, J. Bringing city size in understanding the permanent settlement intention of rural–urban migrants in China. Popul. Space Place 2020, 26, e2295. [Google Scholar] [CrossRef]
- Xie, S.; Wang, J.; Chen, J.; Ritakallio, V.-M. The effect of health on urban-settlement intention of rural-urban migrants in China. Health Place 2017, 47, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Jiang, C. Impact of social capital, sex and education on the utilization of public health services: A cross sectional study based on the China migrant dynamic survey. BMC Public Health 2021, 21, 751. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.; Liu, C.; Ma, Y.; Wang, L. Does City Public Service Distance Increase Sense of Gain to Public Health Service? Evidence from 1394 Migrant Workers in Six Provinces. Int. J. Environ. Res. Public Health 2022, 19, 6131. [Google Scholar] [CrossRef]
- Lu, H.; Li, Z.; Wu, J. Generational differences in urban settlement intentions of rural-to-urban migrants in China: Exploring the role of farmland holding. Soc. Sci. J. 2021, 1–14. [Google Scholar] [CrossRef]
- Cheng, Z.; Wang, H.; Smyth, R. Happiness and job satisfaction in urban China: A comparative study of two generations of migrants and urban locals. Urban Stud. 2014, 51, 2160–2184. [Google Scholar] [CrossRef]


| Variables | (1) | (2) | (3) | (4) | (5) |
|---|---|---|---|---|---|
| PHSA | 0.029 *** | 0.030 *** | 0.078 *** | 0.064 *** | 0.023 *** |
| (0.009) | (0.010) | (0.010) | (0.010) | (0.003) | |
| Gender | −0.033 *** | −0.018 ** | −0.006 ** | ||
| (0.009) | (0.009) | (0.003) | |||
| Age | −0.001 | −0.001 | −0.000 | ||
| (0.001) | (0.001) | (0.000) | |||
| Marriage | 0.054 *** | 0.017 | 0.006 | ||
| (0.015) | (0.015) | (0.005) | |||
| Education | 0.183 *** | 0.160 *** | 0.057 *** | ||
| (0.010) | (0.010) | (0.004) | |||
| Migration range | −0.139 *** | −0.029 *** | −0.010 *** | ||
| (0.006) | (0.006) | (0.002) | |||
| Residence time | 0.015 *** | 0.014 *** | 0.005 *** | ||
| (0.001) | (0.001) | (0.000) | |||
| Income | 0.073 *** | 0.020 *** | 0.007 *** | ||
| (0.008) | (0.007) | (0.003) | |||
| Medicare | 0.248 *** | 0.165 *** | 0.059 *** | ||
| (0.011) | (0.011) | (0.004) | |||
| Occupation | −0.066 *** | −0.015 | −0.005 | ||
| (0.009) | (0.010) | (0.003) | |||
| Family size | −0.002 | −0.000 | −0.000 | ||
| (0.005) | (0.005) | (0.002) | |||
| GDP | 0.193 *** | 0.152 *** | 0.054 *** | ||
| (0.011) | (0.011) | (0.004) | |||
| City size | 0.242 *** | 0.221 *** | 0.078 *** | ||
| (0.006) | (0.006) | (0.002) | |||
| Constant | −0.377 *** | −0.879 *** | −3.048 *** | −2.782 *** | |
| (0.005) | (0.071) | (0.114) | (0.133) | ||
| Pseudo R2 | 0.0001 | 0.0226 | 0.0380 | 0.0463 | |
| Observations | 92,002 | 92,002 | 92,002 | 92,002 | 92,002 |
| Variables | IVprobit | Eprobit | ||
|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |
| PHSA | 1.351 *** | 1.772 *** | ||
| (0.468) | (0.295) | |||
| Instrumental variable | 0.022 *** | 0.010 *** | ||
| (0.003) | (0.003) | |||
| Wald test of exogeneity | 9.000 *** | |||
| AR weak Instrumental variable test | 9.960 *** | |||
| Corr (e. PHSA, e. PMI) | −0.774 *** | |||
| (0.137) | ||||
| Constant | 0.308 *** | −3.160 *** | 0.272 *** | −2.222 *** |
| (0.048) | (0.170) | (0.002) | (0.409) | |
| Control variables | YES | YES | YES | YES |
| Observations | 92,002 | 92,002 | 92,002 | 92,002 |
| Variables | Standard of Judgment | Pass The Test | ||||
|---|---|---|---|---|---|---|
| PHSA | [0.0183, 0.0323] | 0.0243 | 0.0240 | 0.0236 | 0.0233 | YES |
| > 1 | 21.6355 | 16.3251 | 13.1079 | 10.9499 | YES | |
| Variables | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| Health education | 0.030 *** | |||
| (0.010) | ||||
| Health checkup | 0.087 ** | |||
| (0.035) | ||||
| PHSA | 0.064 *** | 0.086 *** | ||
| (0.010) | (0.010) | |||
| Constant | −2.913 *** | −2.887 *** | −2.782 *** | −2.876 *** |
| (0.132) | (0.131) | (0.133) | (0.149) | |
| Control variables | YES | YES | YES | YES |
| Pseudo R2 | 0.0486 | 0.0486 | 0.0463 | 0.0730 |
| Observations | 92,002 | 92,002 | 92,002 | 92,002 |
| Variables | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) |
|---|---|---|---|---|---|---|---|---|
| PHSA | 0.119 *** | 0.064 *** | 0.101 *** | 0.066 *** | 0.213 *** | 0.040 *** | 0.128 *** | 0.055 *** |
| (0.011) | (0.010) | (0.011) | (0.010) | (0.011) | (0.010) | (0.015) | (0.010) | |
| Healthy habits | 0.123 *** | |||||||
| (0.011) | ||||||||
| Health level | 0.029 *** | |||||||
| (0.010) | ||||||||
| Identity | 0.459 *** | |||||||
| (0.010) | ||||||||
| Social Integration | 1.085 *** | |||||||
| (0.021) | ||||||||
| Constant | −0.349 ** | −2.963 *** | −3.009 *** | 3.167 *** | −3.641 *** | 0.807 *** | −3.917 *** | |
| (0.143) | (0.131) | (0.137) | (0.143) | (0.133) | (0.187) | (0.135) | ||
| Control variables | YES | YES | YES | YES | YES | YES | YES | YES |
| Pseudo R2 | 0.028 | 0.050 | 0.065 | 0.049 | 0.058 | 0.065 | 0.028 | 0.075 |
| Total effect | 0.067 *** | 0.067 *** | 0.069 *** | 0.073 *** | ||||
| (0.010) | (0.010) | (0.010) | (0.010) | |||||
| Direct effect | 0.064 *** | 0.066 *** | 0.040 *** | 0.055 *** | ||||
| (0.010) | (0.010) | (0.010) | (0.010) | |||||
| Indirect effect | 0.004 *** | 0.001 *** | 0.029 *** | 0.018 *** | ||||
| (0.000) | (0.000) | (0.002) | (0.002) | |||||
| Observations | 92,002 | 92,002 | 92,002 | 92,002 | 92,002 | 92,002 | 92,002 | 92,002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Q.; Song, M.; Wang, H. Voting with Your Feet: The Impact of Urban Public Health Service Accessibility on the Permanent Migration Intentions of Rural Migrants in China. Int. J. Environ. Res. Public Health 2022, 19, 14624. https://doi.org/10.3390/ijerph192214624
Zhao Q, Song M, Wang H. Voting with Your Feet: The Impact of Urban Public Health Service Accessibility on the Permanent Migration Intentions of Rural Migrants in China. International Journal of Environmental Research and Public Health. 2022; 19(22):14624. https://doi.org/10.3390/ijerph192214624
Chicago/Turabian StyleZhao, Qingjun, Meijing Song, and Hanrui Wang. 2022. "Voting with Your Feet: The Impact of Urban Public Health Service Accessibility on the Permanent Migration Intentions of Rural Migrants in China" International Journal of Environmental Research and Public Health 19, no. 22: 14624. https://doi.org/10.3390/ijerph192214624