
Demographic and COVID Experience Predictors of COVID-19 Risk Perception among Chinese Residents in Canada

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Survey
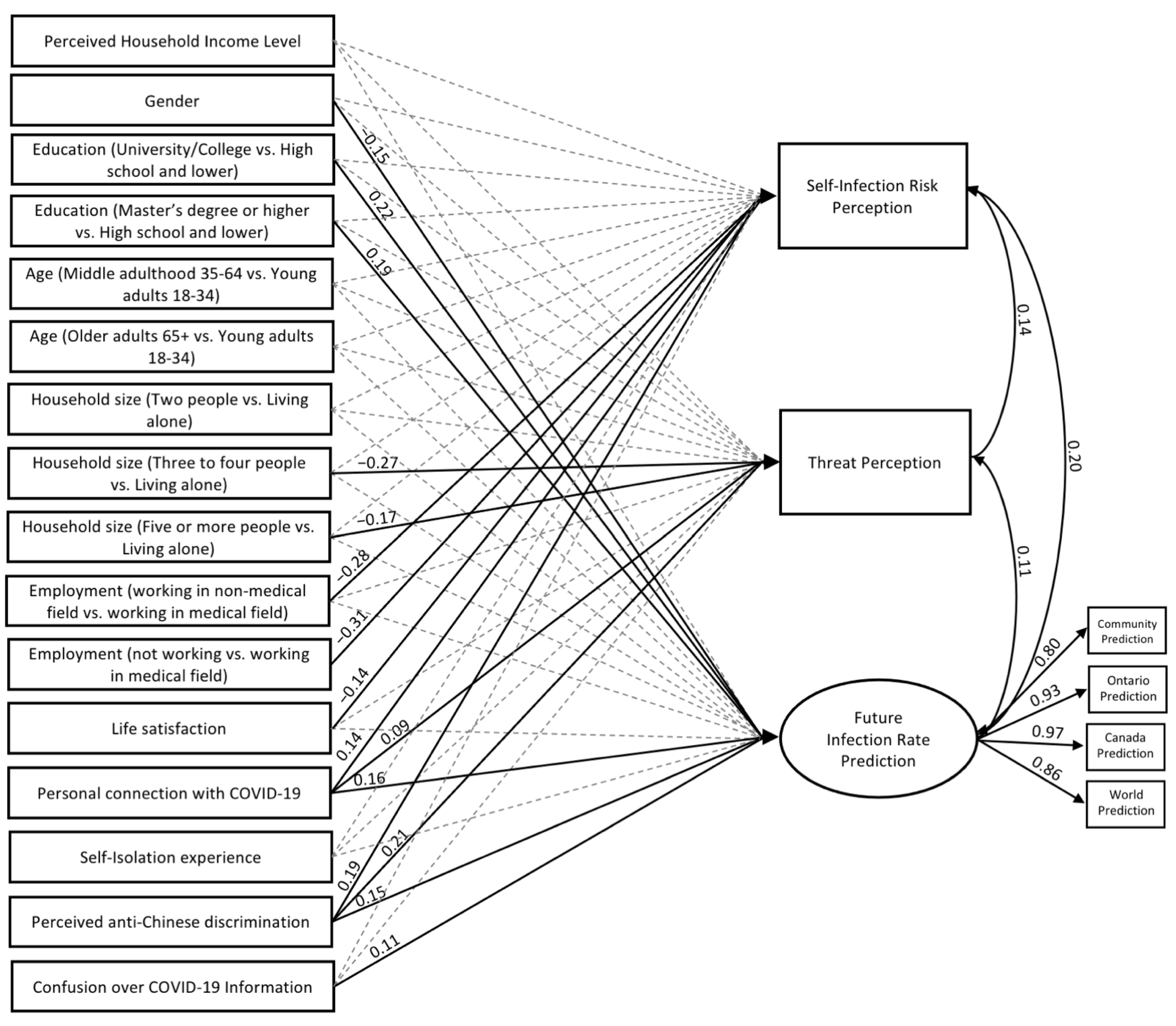
2.3. The Structural Equation Model (SEM)
2.3.1. Demographic Predictors
2.3.2. COVID Experience Predictors
2.3.3. Outcome Variables
3. Results
3.1. Model Fit
3.2. Model Assumptions
3.3. Structural Equation Model (SEM) for COVID-19 Risk Perception

3.3.1. Self-infection Risk Prediction
3.3.2. Threat Prediction
3.3.3. Future Infection Rate Prediction
4. Discussion
4.1. Demographic Predictors
4.2. COVID Experience Predictors
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Archived: WHO Timeline-COVID-19; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Kim, A.W.; Nyengerai, T.; Mendenhall, E. Evaluating the Mental Health Impacts of the COVID-19 Pandemic in Urban South Africa: Perceived Risk of COVID-19 Infection and Childhood Trauma Predict Adult Depressive Symptoms. Psychol. Med. 2020, 52, 1587–1599. [Google Scholar] [CrossRef] [PubMed]
- Hyland, P.; Shevlin, M.; McBride, O.; Murphy, J.; Karatzias, T.; Bentall, R.P.; Martinez, A.; Vallières, F. Anxiety and depression in the Republic of Ireland during the COVID-19 pandemic. Acta Psychiatr. Scand. 2020, 142, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Feng, B.; Liao, W.; Pan, W. Internet Use, Risk Awareness, and Demographic Characteristics Associated With Engagement in Preventive Behaviors and Testing: Cross-Sectional Survey on COVID-19 in the United States. J. Med. Internet Res. 2020, 22, e19782. [Google Scholar] [CrossRef] [PubMed]
- Na LYang, L.; Yu, L.; Bolton, K.; Zhang, W.; Wang, P. The Appraisal and Endorsement of Individual and Public Preventive Measures to Combat COVID-19 and the Associated Psychological predictors among Chinese Living in Canada. Open J. Public Health 2021, 14, 592–599. [Google Scholar] [CrossRef]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.; Recchia, G.; Van Der Bles, A.M.; Spiegelhalter, D.; Van Der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Xin, M.; Luo, S.; She, R.; Yu, Y.; Li, L.; Wang, S.; Ma, L.; Tao, F.; Zhang, J.; Zhao, J.; et al. Negative cognitive and psychological correlates of mandatory quarantine during the initial COVID-19 outbreak in China. Am. Psychol. 2020, 75, 607–617. [Google Scholar] [CrossRef]
- Na, L.; Yang, L.; Mezo, P.G.; Liu, R. Age disparities in mental health during the COVID19 pandemic: The roles of resilience and coping. Soc. Sci. Med. 2022, 305, 115031. [Google Scholar] [CrossRef]
- McElroy, E.; Patalay, P.; Moltrecht, B.; Shevlin, M.; Shum, A.; Creswell, C.; Waite, P. Demographic and health factors associated with pandemic anxiety in the context of COVID-19. Br. J. Health Psychol. 2020, 25, 934–944. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Ustun, G. Determining depression and related factors in a society affected by COVID-19 pandemic. Int. J. Soc. Psychiatry 2021, 67, 54. [Google Scholar] [CrossRef]
- Han, X.; Chen, S.; Bi, K.; Yang, Z.; Sun, P. Depression Following COVID-19 Lockdown in Severely, Moderately, and Mildly Impacted Areas in China. Front. Psychiatry 2021, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- Yeung, L. Early Efforts By B.c.’s Chinese Community to CURB COVID-19 Should Be ‘Applauded,’ Doctor Says|CBC News. CBCnews. (8 June 2020). Available online: https://www.cbc.ca/news/canada/british-columbia/early-efforts-by-chinese-community-to-curb-covid-19-should-be-applauded-says-b-c-doctor-1.5600943. (accessed on 20 August 2021).
- Diener, E.D.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Shrikanth, S.; Szpunar, P.M.; Szpunar, K.K. Staying positive in a dystopian future: A novel dissociation between personal and collective cognition. J. Exp. Psychol. Gen. 2018, 147, 1200. [Google Scholar] [CrossRef] [PubMed]
- Deng, W.; Rosenblatt, A.K.; Talhelm, T.; Putnam, A.L. People from the US and China think about their personal and collective future differently. Mem. Cogn. 2022, 1–14. [Google Scholar] [CrossRef]
- Howard, M.C. A review of exploratory factor analysis decisions and overview of current practices: What we are doing and how can we improve? Int. J. Hum.-Comput. Interact. 2016, 32, 51–62. [Google Scholar] [CrossRef]
- Kaiser, H.F. The application of electronic computers to factor analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Cattell, R.B. The scree test for the number of factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Xia, Y.; Yang, Y. RMSEA, CFI, and TLI in structural equation modeling with ordered categorical data: The story they tell depends on the estimation methods. Behav. Res. Methods 2019, 51, 409–428. [Google Scholar] [CrossRef] [Green Version]
- Beaujean, A.A. Latent Variable Modeling Using r: A Step-by-Step Guide, 1st ed.; Routledge: London, UK; Taylor & Francis Group: Abingdon, UK, 2014; Available online: https://www.taylorfrancis.com/books/mono/10.4324/9781315869780/latent-variable-modeling-using-alexander-beaujean (accessed on 14 June 2021).
- Korkmaz, S.; Goksuluk, D.; Zararsiz, G. MVN: An R Package for Assessing Multivariate Normality. R J. 2014, 6, 151–162. Available online: https://journal.r-project.org/archive/2014-2/korkmaz-goksuluk-zararsiz.pdf. (accessed on 26 August 2022). [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Suhr, D. The Basics of Structural Equation Modeling; SAS User Group of the Western Region of the United States (WUSS): Irvine, CA, USA, 2006. [Google Scholar]
- Pek, J.; Flora, D.B. Reporting effect sizes in original psychological research: A discussion and tutorial. Psychol. Methods 2018, 23, 208–225. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Ringle, C.M.; Sarstedt, M. PLS-SEM: Indeed a silver bullet. J. Mark. Theory Pract. 2011, 19, 139–152. [Google Scholar] [CrossRef]
- Neumer, A.; Schweizer, T.; Bogdanić, V.; Boecker, L.; Loschelder, D.D. How health message framing and targets affect distancing during the COVID-19 pandemic. Health Psychol. 2022, 41, 630. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Scott, J. Family and gender values in China: Generational, geographic, and gender differences. J. Fam. Issues 2016, 37, 1267–1293. [Google Scholar] [CrossRef] [Green Version]
- Lai, D.W.; Luk, P.K.; Andruske, C.L. Gender differences in caregiving: A case in Chinese Canadian caregivers. J. Women Aging 2007, 19, 161–178. [Google Scholar] [CrossRef]
- Best, L.A.; Law, M.A.; Roach, S.; Wilbiks, J.M. The psychological impact of COVID-19 in Canada: Effects of social isolation during the initial response. Can. Psychol. Psychol. Can. 2021, 62, 143. [Google Scholar] [CrossRef]
- Su, C.; Yang, L.; Dong, L.; Zhang, W. The Psychological Well-Being of Older Chinese Immigrants in Canada amidst COVID-19: The Role of Loneliness, Social Support, and Acculturation. Int. J. Environ. Res. Public Health 2022, 19, 8612. [Google Scholar] [CrossRef]
- Lee, A.D.Y.; Wang, P.P.; Zhang, W.; Yang, L. COVID-19 Peritraumatic Distress and Loneliness in Chinese Residents in North America: The Role of Contraction Worry. Int. J. Environ. Res. Public Health 2022, 19, 7639. [Google Scholar] [CrossRef]
- Yu, L.; Lecompte, M.; Zhang, W.; Wang, P.; Yang, L. Sociodemographic and COVID-Related Predictors for Mental Health Condition of Mainland Chinese in Canada Amidst the Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 171. [Google Scholar] [CrossRef]
- Yang, L.; Kandasamy, K.; Na, L.; Zhang, W.; Wang, P.P. Perceived and Experienced Discrimination and Its Associated Psychological Impacts among Chinese Canadians during the Wave 2 of the COVID-19 Pandemic. Psychol Health Med. 2022; in press. [Google Scholar] [CrossRef]

{kind=link}
| Predictor Category | Predictors | Response Rate: n (%) | Code | |
|---|---|---|---|---|
| Demographic | Perceived Household Income Level | Low | 55 (8.42%) | 1 |
| Lower than average | 67 (10.26%) | 2 | ||
| Average | 202 (30.93%) | 3 | ||
| Higher than average | 118 (18.07%) | 4 | ||
| High | 17 (2.60%) | 5 | ||
| Gender | Women | 334 (51.15%) | 1 | |
| Men | 124 (18.99%) | 2 | ||
| Education | High school/secondary school or less | 38 (5.82%) | 0 | |
| University/College | 256 (39.20%) | 1 | ||
| Master’s degree or higher | 167 (25.57%) | 2 | ||
| Age | Young adults (18–34) | 44 (6.74%) | 0 | |
| Middle adulthood (35–64) | 364 (55.74%) | 1 | ||
| Older adults (65+) | 54 (8.27%) | 2 | ||
| Household Size | Alone (1 person) | 22 (3.37%) | 0 | |
| 2 people | 98 (15.01%) | 1 | ||
| 3–4 people | 249 (38.13%) | 2 | ||
| 5 or more | 85 (13.02%) | 3 | ||
| Employment Status | Working in a medical field | 18 (2.76%) | 0 | |
| Working (non-medical field) | 284 (43.49%) | 1 | ||
| Not currently employed | 158 (24.20%) | 2 | ||
| COVID Experience | Personal Connection with COVID-19 | No | 466 (71.36%) | 1 |
| Yes (Confirmed/Suspected/Unsure) | 147 (22.51%) | 2 | ||
| Self-isolation experience | No/Not selected Yes | 285 (43.64%) | 1 | |
| 324 (49.62%) | 2 | |||
| Perceived Discrimination | Completely disagree | 10 (1.53%) | 1 | |
| Somewhat disagree | 62 (9.49%) | 2 | ||
| Neutral | 172 (26.34%) | 3 | ||
| Somewhat agree | 198 (30.32%) | 4 | ||
| Completely agree | 85 (13.02%) | 5 | ||
| Confusion over COVID-19 Information | Never | 43 (6.58%) | 1 | |
| Seldom | 98 (15.01%) | 2 | ||
| Sometimes | 255 (39.05%) | 3 | ||
| Often | 114 (17.46%) | 4 | ||
| Always | 21 (3.22%) | 5 | ||
| Outcome Variables | Survey Question | Likert Scale | Response Rate n (%) |
|---|---|---|---|
| Self-infection Risk Perception | How likely do you think it is that you will be infected with the COVID-19? | 1 = Very unlikely | 28 (4.28%) |
| 2 = Unlikely | 124 (18.99%) | ||
| 3 = Neutral | 290 (44.41%) | ||
| 4 = Likely | 132 (20.21%) | ||
| 5 = Very likely | 30 (4.59%) | ||
| Threat Perception | Do you believe that COVID-19 pandemic is a real threat? | 1 = Completely disagree | 3 (0.46%) |
| 2 = Somewhat disagree | 17 (2.60%) | ||
| 3 = Neutral | 69 (10.57%) | ||
| 4 = Somewhat agree | 229 (35.07%) | ||
| 5 = Completely agree | 212 (32.47%) | ||
| Future Infection Rate Prediction | Please estimate the percentage of your community population will be infected? | Percentage (%) input | 419 (64.17%) |
| Please estimate the percentage of Ontario population will be infected? | Percentage (%) input | 412 (63.09%) | |
| Please estimate the percentage of Canadian population will be infected? | Percentage (%) input | 398 (60.95%) | |
| Please estimate the percentage of World population will be infected? | Percentage (%) input | 401 (61.41%) |
| Self-Infection Risk Perception | Threat Perception | Community | Ontario | Canada | World | |
|---|---|---|---|---|---|---|
| Percieved household income | 0.016 | −0.087 | −0.110 * | −0.061 | −0.115 * | −0.024 |
| Gender | −0.053 | 0.018 | −0.115 * | −0.184 ** | −0.196 ** | −0.249 ** |
| Education | −0.041 | −0.152 * | −0.015 | −0.049 | −0.064 | −0.033 |
| Age | −0.083 | 0.029 | −0.027 | −0.058 | −0.005 | −0.010 |
| Household size | −0.024 | −0.133 ** | 0.115 * | −0.052 | −0.063 | 0.000 |
| Employmnet Status | −0.145 ** | −0.004 | −0.075 | −0.022 | −0.006 | 0.005 |
| Life Satisfaction | −0.194 ** | −0.148 ** | −0.161 ** | −0.126 * | −0.101 | −0.082 |
| Personal connection with COVID | 0.229 ** | 0.111 * | 0.199 ** | 0.198 ** | 0.233 ** | 0.206 ** |
| Self-isolation expereince | −0.031 | 0.110 * | 0.024 | 0.032 | 0.015 | −0.013 |
| Percieved anti-Chinese discrimination | 0.235 ** | 0.239 ** | 0.182 ** | 0.193 ** | 0.179 ** | 0.162 ** |
| Confusion over COVID-19 information | 0.086 * | 0.089 * | 0.101 * | 0.105 * | 0.088 | 0.073 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lecompte, M.; Counsell, A.; Yang, L. Demographic and COVID Experience Predictors of COVID-19 Risk Perception among Chinese Residents in Canada. Int. J. Environ. Res. Public Health 2022, 19, 14448. https://doi.org/10.3390/ijerph192114448
Lecompte M, Counsell A, Yang L. Demographic and COVID Experience Predictors of COVID-19 Risk Perception among Chinese Residents in Canada. International Journal of Environmental Research and Public Health. 2022; 19(21):14448. https://doi.org/10.3390/ijerph192114448
Chicago/Turabian StyleLecompte, Mariah, Alyssa Counsell, and Lixia Yang. 2022. "Demographic and COVID Experience Predictors of COVID-19 Risk Perception among Chinese Residents in Canada" International Journal of Environmental Research and Public Health 19, no. 21: 14448. https://doi.org/10.3390/ijerph192114448