
Trends in Prescription Opioid Use in Motor Vehicle Crash Injuries in the United States: 2014–2018

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leading Causes of Death Reports, 1981–2018. Web-Based Injury Statistics Query and Reporting System. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Available online: https://webappa.cdc.gov/sasweb/ncipc/leadcause.html (accessed on 9 February 2021).
- Nonfatal Injury Data. Web-Based Injury Statistics Query and Reporting System. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Available online: https://www.cdc.gov/injury/wisqars/nonfatal.html (accessed on 11 February 2021).
- Cost of Injury Data. Web-Based Injury Statistics Query and Reporting System. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Available online: https://www.cdc.gov/injury/wisqars/cost/ (accessed on 11 February 2021).
- Tabibi, Z.; Schwebel, D.C.; Moghaddam, A.M.; Fadardi, J.S.; Feizabadi, S.M. Differential effects of stimulant versus opiate drugs on driving performance. Accid. Anal. Prev. 2020, 150, 105885. [Google Scholar] [CrossRef] [PubMed]
- Rohrig, T.P.; Nash, E.; Osawa, K.A.; Shan, X.; Scarneo, C.; Youso, K.B.; Tiscione, N.B. Fentanyl and driving impairment. J. Anal. Toxicol. 2021, 45, 389–396. [Google Scholar] [CrossRef] [PubMed]
- NIDA. 27 May 2020. Prescription Opioids DrugFacts. Available online: https://www.drugabuse.gov/publications/drugfacts/prescription-opioids (accessed on 11 February 2021).
- Chihuri, S.; Li, G. Use of prescription opioids and motor vehicle crashes: A meta analysis. Accid. Anal. Prev. 2017, 109, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Chihuri, S.; Li, G. Trends in Prescription Opioids Detected in Fatally Injured Drivers in 6 US States: 1995–2015. Am. J. Public Health 2017, 107, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Rudisill, T.M.; Zhao, S.; Abate, M.A.; Coben, J.H.; Zhu, M. Trends in drug use among drivers killed in US traffic crashes, 1999–2010. Accid. Anal. Prev. 2014, 70, 178–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chihuri, S.; Li, G. Use of Prescription Opioids and Initiation of Fatal 2-Vehicle Crashes. JAMA Netw. Open 2019, 2, e188081. [Google Scholar] [CrossRef] [PubMed]
- Timeline of Selected FDA Activities and Significant Events Addressing Opioid Misuse and Abuse. FDA. Available online: https://wayback.archive-it.org/7993/20180126022507/https:/www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm338566.htm (accessed on 11 February 2021).
- Dowell, D.; Haegerich, T.M.; Chou, R. CDC Guideline for Prescribing Opioids for Chronic Pain—United States, 2016. MMWR. Recomm. Rep. 2016, 65, 1–49. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Transportation, National Highway Traffic Safety Administration. Traffic Safety Facts: Research Notes; NHTSA’s National Center for Statistics and Analysis, 1200 New Jersey Avenue SE: Washington, DC, USA, 2014. [Google Scholar]
- Chang, Z.; Quinn, P.; Hur, K.; Gibbons, R.D.; Sjölander, A.; Larsson, H.; D’Onofrio, B.M. Association Between Medication Use for Attention-Deficit/Hyperactivity Disorder and Risk of Motor Vehicle Crashes. JAMA Psychiatry 2017, 74, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Gomes, T.; Redelmeier, D.A.; Juurlink, D.N.; Dhalla, I.A.; Camacho, X.; Mamdani, M.M. Opioid Dose and Risk of Road Trauma in Canada. JAMA Intern. Med. 2013, 173, 196–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IBM Watson Health. IBM MarketScan Research Databases for Life Sciences Researchers. Available online: https://www.ibm.com/downloads/cas/0NKLE57Y (accessed on 12 April 2021).
- MapIT Automated In-House Stand-Alone Mapping Tool. Agency for Healthcare Research and Quality. Available online: https://qualityindicators.ahrq.gov/resources/toolkits.aspx (accessed on 25 June 2020).
- National Center for Injury Prevention and Control. CDC Compilation of Benzodiazepines, Muscle Relaxants, Stimulants, Zolpidem, and Opioid Analgesics with Oral Morphine Milligram Equivalent Conversion Factors, 2017 Version. Centers for Disease Control and Prevention: Atlanta, GA, USA, 2017. Available online: https://www.cdc.gov/drugoverdose/resources/data.html (accessed on 4 February 2021).
- Schieber, L.Z.; Guy, G.P.; Seth, P.; Young, R.; Mattson, C.L.; Mikosz, C.A.; Schieber, R.A. Trends and Patterns of Geographic Variation in Opioid Prescribing Practices by State, United States, 2006–2017. JAMA Netw. Open 2019, 2, e190665. [Google Scholar] [CrossRef] [PubMed]
- Keller, T.; Keller, A.; Tutsch-Bauer, E.; Monticelli, F. Driving under the influence of drugs and alcohol in Salzburg and Upper Austria during the years 2003–2007. Leg. Med. 2009, 11, S98–S99. [Google Scholar] [CrossRef] [PubMed]
- Papadodima, S.A.; Athanaselis, S.A.; Stefanidou, M.E.; Dona, A.A.; Papoutsis, I.; Maravelias, C.P.; Spiliopoulou, C.A. Driving under the influence in Greece: A 7-year survey (1998–2004). Forensic Sci. Int. 2008, 174, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Senna, M.-C.; Augsburger, M.; Aebi, B.; Briellmann, T.A.; Donzé, N.; Dubugnon, J.-L.; Iten, P.X.; Staub, C.; Sturm, W.; Sutter, K. First nationwide study on driving under the influence of drugs in Switzerland. Forensic Sci. Int. 2010, 198, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Favretto, D.; Visentin, S.; Stocchero, G.; Vogliardi, S.; Snenghi, R.; Montisci, M. Driving under the influence of drugs: Prevalence in road traffic accidents in Italy and considerations on per se limits legislation. Traffic Inj. Prev. 2018, 19, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Thomas, F.D.; Berning, A.; Darrah, J.; Graham, L.A.; Blomberg, R.D.; Griggs, C.; Rayner, M. Drug and Alcohol Prevalence in Seriously and Fatally Injured Road Users before and during the COVID-19 Public Health Emergency; National Highway Traffic Safety Administration. Office of Behavioral Safety Research: Washington, DC, USA, 2020.
- Kelley-Baker, T.; Berning, A.; Ramirez, A.; Lacey, J.; Carr, K.; Waehrer, G.; Moore, C.; Pell, K.; Yao, J.; Compton, R. 2013–2014 National Roadside Study of Alcohol and Drug Use by Drivers: Drug Results (Report No. DOT HS 812 411). National Highway Traffic Safety Administration: Washington, DC, USA. Available online: https://www.nhtsa.gov/behavioral-research/2013-14-national-roadside-study-alcohol-and-drug-use-drivers (accessed on 24 March 2021).
- Lund, B.C.; E Ohl, M.; Hadlandsmyth, K.; Mosher, H.J. Regional and Rural–Urban Variation in Opioid Prescribing in the Veterans Health Administration. Mil. Med. 2019, 184, 894–900. [Google Scholar] [CrossRef] [PubMed]
- CDC; U.S. Opioid Prescribing Rate Maps. Available online: https://www.cdc.gov/drugoverdose/maps/rxrate-maps.html (accessed on 27 March 2019).



{kind=link}
{kind=link}
| Number of MVC Injuries (N = 142,204) | Percentage of MVC Injuries Involving Opioids | Prevalence Ratio (95% CI) a | |
|---|---|---|---|
| Year of MVC injuries | |||
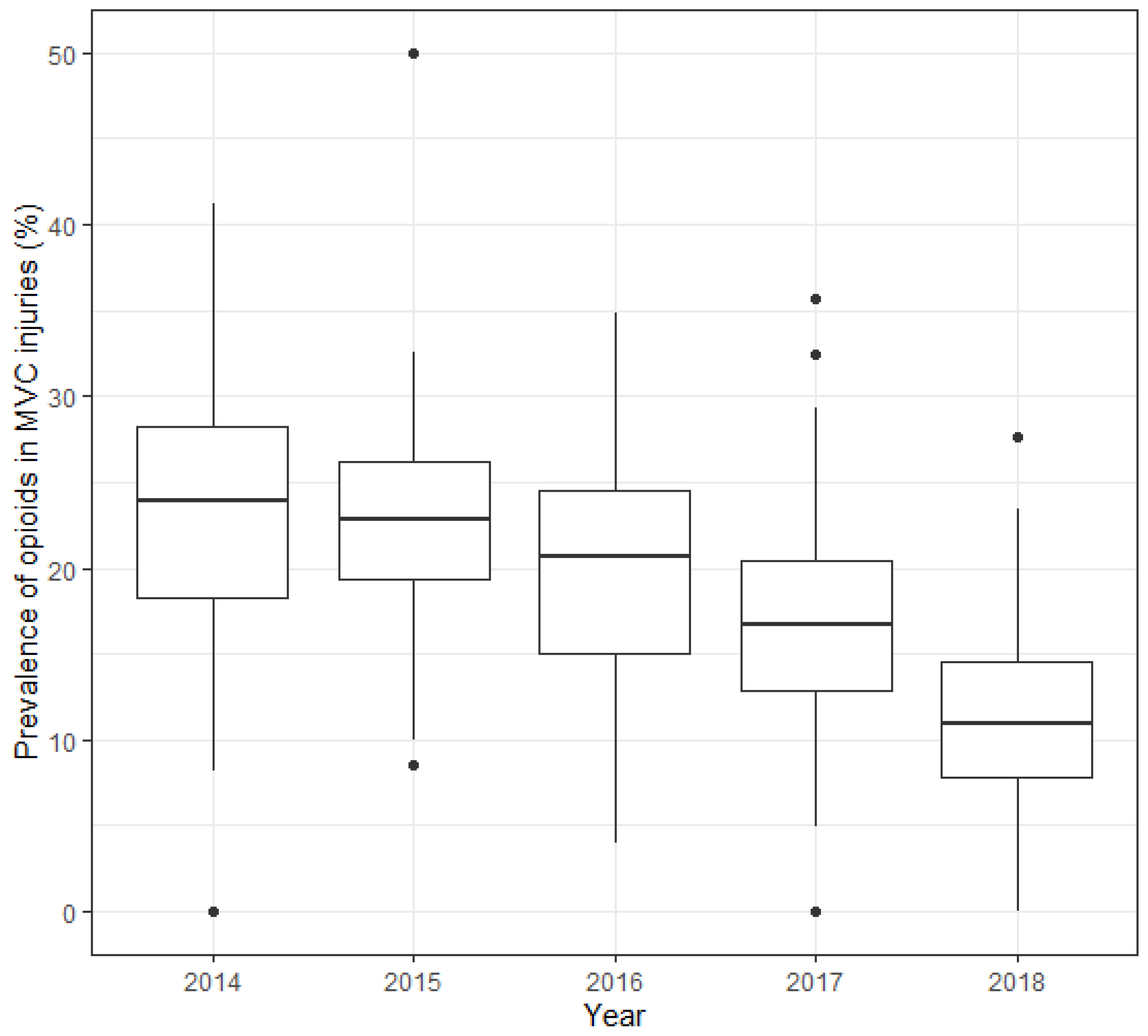
| 2014 | 20,818 | 24% | 1 (Reference) |
| 2015 | 33,452 | 23% | 0.93 (0.90, 0.95) |
| 2016 | 36,350 | 20% | 0.80 (0.78, 0.83) |
| 2017 | 27,673 | 16% | 0.67 (0.65, 0.70) |
| 2018 | 23,911 | 12% | 0.50 (0.48, 0.52) |
| MVC injuries occurred before or after the CDC guidelines | |||
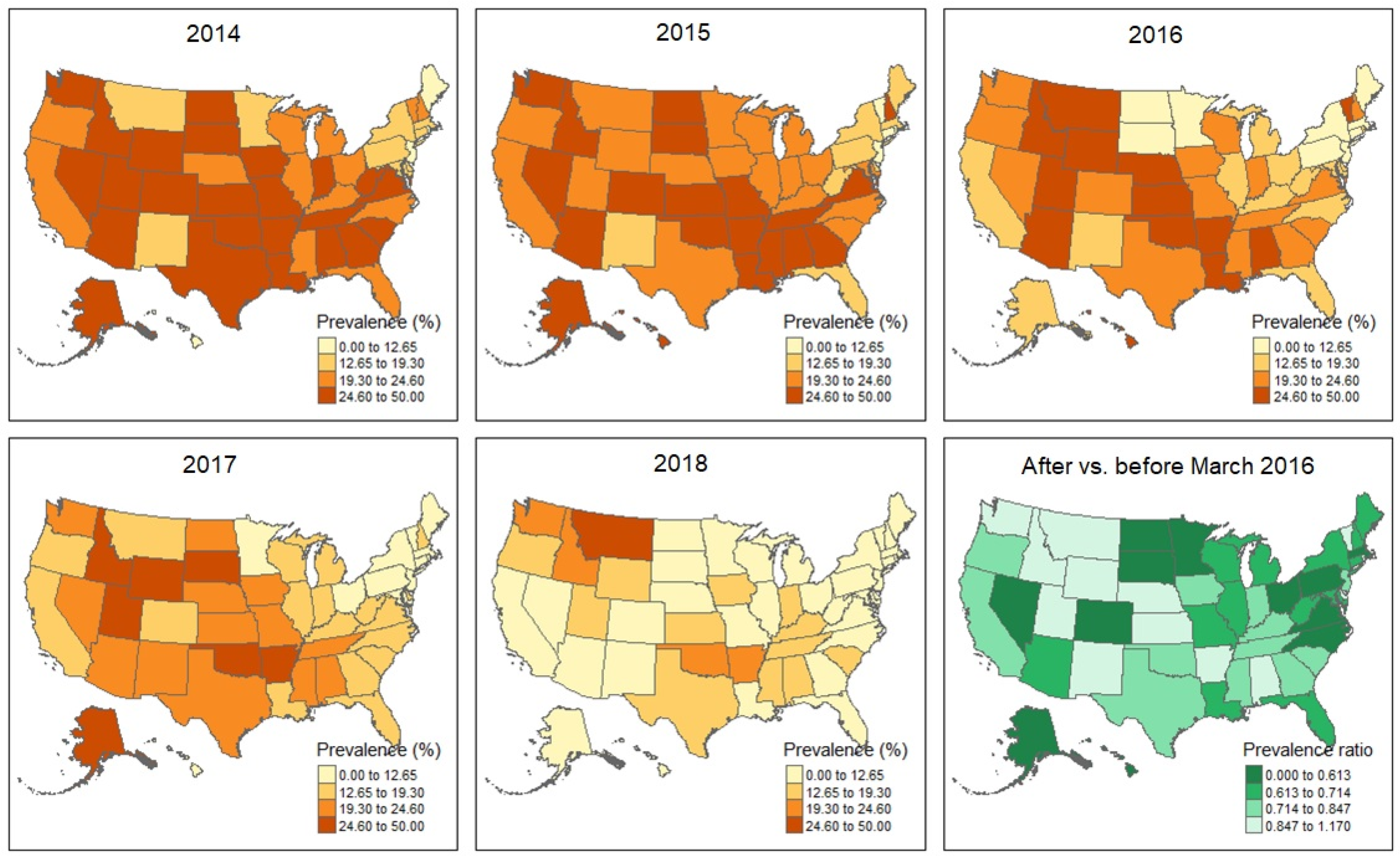
| Before (<March 2016) | 59,678 | 23% | 1 (Reference) |
| After (≥March 2016) | 82,526 | 16% | 0.71 (0.70, 0.73) |
| Region | |||
| Northeast | 14,041 | 11% | 1 (Reference) |
| North-Central | 33,837 | 18% | 1.70 (1.43, 2.02) |
| South | 67,480 | 21% | 1.83 (1.56, 2.14) |
| West | 26,846 | 20% | 2.01 (1.69, 2.39) |
| Metropolitan statistical area | |||
| Yes | 125,199 | 19% | 1 (Reference) |
| No | 17,005 | 21% | 1.04 (1.01, 1.08) |
| Number of Prescriptions Involved in MVC Injuries, 2014–2018 | Prevalence Ratio (after vs. before the CDC Guidelines in March 2016) | |
|---|---|---|
| All opioids | 31,584 | 0.71 (0.70, 0.73) |
| Common opioids | ||
| hydrocodone | 15,655 | 0.63 (0.61, 0.65) |
| oxycodone | 6407 | 0.73 (0.69, 0.76) |
| tramadol | 5635 | 0.79 (0.75, 0.83) |
| codeine | 2445 | 0.98 (0.91, 1.07) |
| buprenorphine | 438 | 1.15 (0.94, 1.42) |
| morphine | 326 | 1.01 (0.79, 1.29) |
| fentanyl | 217 | 0.61 (0.45, 0.82) |
| methadone | 82 | 0.50 (0.31, 0.80) |
| Year | Number of Prescriptions | Number of Prescriptions per 100 Injuries | MME | Daily MME | Duration (Days) | % High-Dosage a Prescription b | % Long-Acting Prescription b |
|---|---|---|---|---|---|---|---|
| All states | |||||||
| 2014 | 5811 | 28 | 828 | 73 | 9.2 | 6.2% | 4.3% |
| 2015 | 8389 | 25 | 638 | 83 | 8.9 | 5.9% | 3.9% |
| 2016 | 7903 | 22 | 857 | 107 | 9.4 | 5.4% | 4.7% |
| 2017 | 5812 | 21 | 499 | 57 | 9.4 | 5.3% | 4.7% |
| 2018 | 3669 | 15 | 893 | 66 | 9.6 | 5.1% | 5.7% |
| States with larger decrease (PR ≤ 0.71 c after versus before the CDC guidelines) | |||||||
| 2014 | 2675 | 26 | 1273 | 108 | 9.3 | 7.2% | 4.4% |
| 2015 | 3977 | 24 | 728 | 116 | 8.8 | 5.1% | 3.7% |
| 2016 | 3438 | 20 | 1318 | 186 | 10.2 | 5.7% | 5.4% |
| 2017 | 2043 | 16 | 547 | 66 | 9.6 | 4.9% | 5.4% |
| 2018 | 1285 | 10 | 1730 | 105 | 10.8 | 3.7% | 8.2% |
| States with smaller decrease (PR > 0.71 after versus before the CDC guidelines) | |||||||
| 2014 | 2906 | 28 | 455 | 44 | 9.2 | 5.5% | 4.1% |
| 2015 | 4372 | 26 | 557 | 53 | 8.9 | 6.8% | 4.1% |
| 2016 | 4446 | 23 | 504 | 46 | 8.8 | 5.2% | 4.2% |
| 2017 | 2872 | 20 | 396 | 48 | 8.7 | 3.9% | 3.9% |
| 2018 | 1778 | 16 | 395 | 37 | 8.8 | 3.1% | 4.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, L.; Vermund, S.H.; Zhang, Y. Trends in Prescription Opioid Use in Motor Vehicle Crash Injuries in the United States: 2014–2018. Int. J. Environ. Res. Public Health 2022, 19, 14445. https://doi.org/10.3390/ijerph192114445
Jin L, Vermund SH, Zhang Y. Trends in Prescription Opioid Use in Motor Vehicle Crash Injuries in the United States: 2014–2018. International Journal of Environmental Research and Public Health. 2022; 19(21):14445. https://doi.org/10.3390/ijerph192114445
Chicago/Turabian StyleJin, Lan, Sten H. Vermund, and Yawei Zhang. 2022. "Trends in Prescription Opioid Use in Motor Vehicle Crash Injuries in the United States: 2014–2018" International Journal of Environmental Research and Public Health 19, no. 21: 14445. https://doi.org/10.3390/ijerph192114445