1. Introduction
During healthy pregnancies, in order to guarantee adequate fetal growth and development, insulin sensitivity is reduced [
1]. As a result, the capacity for glucose uptake is compromised and blood glucose levels increase [
2]. Normally, this reduced insulin sensitivity and hyperglycemia are counteracted by a greater insulin secretion causing a state of hyperinsulinemia. However, if pancreatic beta-cells are incapable of producing sufficient insulin [
1], gestational diabetes mellitus (GDM), one of the most common complications of pregnancy [
3], will develop.
GDM is commonly defined as a carbohydrate intolerance diagnosed for the first time in pregnancy [
1], between the second and third trimester, and which generally resolves after delivery [
4,
5]. The worldwide prevalence of GDM is estimated to be of 14.2% [
6] and a recent meta-analysis estimated that around 12.3% of South European women have GDM [
7].
GDM can lead to serious short- and long-term consequences in the mother, fetus, and newborn. Women who develop GDM are at greater risk of suffering cardiovascular diseases, preeclampsia, preterm birth, and caesarean delivery, in addition to birth canal lacerations [
8]. However, the most important maternal side effect of GDM is the continuation of diabetes after delivery [
9]. The chance of progressing to type 2 diabetes mellitus (T2DM) after GDM increases by 70% within 28 years postpartum [
10]. Similarly, there are increased risks of macrosomia at birth (birth weight ≥ 4 kg) [
4], labor difficulties such as birth trauma, fracture, and shoulder dystocia, and neonatal hypoglycemia [
8] in pregnancies under GDM. Furthermore, research shows that offspring of GDM mothers are at a greater risk of developing T2DM [
11] and obesity [
12] in the future, in addition to insulin resistance [
11] and cardiovascular diseases [
8]. In some cases, where GDM is untreated, perinatal mortality may also occur [
8].
Various risk factors have been associated with the development of GDM. These include being over 35 years old, previous GDM or delivery of macrosomic baby, polycystic ovarian syndrome, use of corticosteroids, or belonging to a high-risk population (Aboriginal, Hispanic, Asian, or African) [
13]. Nevertheless, the major risk factors for developing GDM are being overweight or obese (body mass index (BMI) ≥ 25 kg/m
2) at the beginning of pregnancy [
13,
14], and excessive gestational weight gain [
15].
According to the scientific literature, to reduce the risk of excessive maternal weight gain and thus, the risk of suffering GDM, regular physical activity (PA) is strongly recommended, in the absence of any obstetric contraindications [
16]. In addition, it has been suggested that PA can reduce the risk of GDM by 31% [
17]. However, despite the multiple health benefits demonstrated by the practice of physical activity [
16], it has been observed that pregnant women reduce their activity levels with pregnancy [
18]. International PA guidelines [
19,
20,
21] recommend the equivalent of 150 min/week of moderate-intensity physical activity during pregnancy and, specifically, a recent meta-analysis suggested an accumulation of >90 min/week of moderate-intensity PA to reduce the odds of GDM by 46% [
22].
The COVID-19 global pandemic outbreak and the lockdown measures imposed by governments in March 2020 have contributed to a more sedentary lifestyle and to a significant reduction in physical activity levels among pregnant women [
23], which may lead to numerous chronic pathologies such as cardiovascular diseases, type 2 diabetes [
24], and metabolic syndrome, which includes obesity and dyslipidaemia [
25], and pregnancy disorders including preeclampsia [
26]. Consequently, an increase in the prevalence of GDM was observed among pregnant women in 2020 compared to pregnant women in 2019 when there were no mobility restrictions [
27].
Given these data and the dangerous health consequences associated with GDM for both mother and fetus, an adequate preventive strategy is absolutely necessary.
Although the scientific literature is not entirely conclusive, many pre-pandemic experimental studies show the positive influence of supervised exercise on prevention of GDM in healthy pregnancy [
28,
29].
Therefore, during the ongoing pandemic and with the technological progress of online modalities, the aim of this study was to examine the influence of a supervised online exercise program throughout pregnancy on gestational diabetes. We hypothesized that a supervised, moderate regular exercise program throughout pregnancy using an online model may help prevent the development of gestational diabetes.
The aim of this study was to examine the effect of an online supervised exercise program during pregnancy on the prevention of GDM, and on maternal and childbirth outcomes.
2. Materials and Methods
2.1. Study Design
The present RCT (Identifier: NCT04563065) was carried out between August 2020 and February 2022 following the ethical guidelines of the Declaration of Helsinki, last modified in 2000.
The protocol for this study was approved by the Ethical Commission of Research of the Universidad Politécnica de Madrid and Ethical Commission of Clinical Research (CEIC) of Hospital Universitario Severo Ochoa in Leganés, Hospital Universitario Puerta de Hierro in Majadahonda, and Clinica Zuatzu in San Sebastián.
2.2. Participants
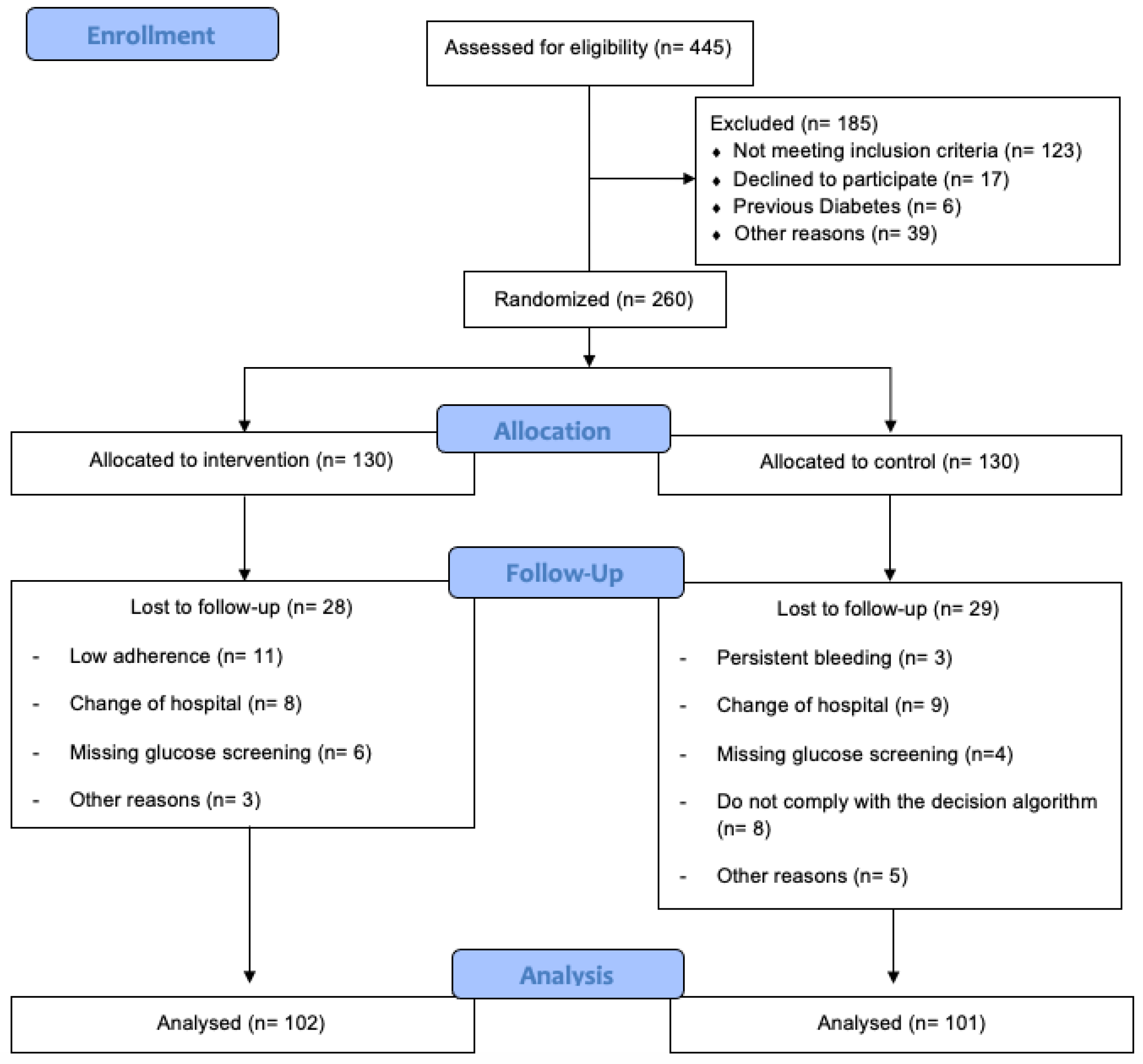
A total of 445 healthy pregnant women from three hospitals were recruited during their first prenatal visit at the hospital (
Figure 1). They were informed about the nature of the study and were assessed for eligibility by their obstetric health providers.
Pregnant women with singleton, uncomplicated pregnancies (no type 1 or 2 diabetes at baseline), with no risk of preterm delivery and with no serious medical contraindications that prevented them from exercising, were invited to participate in the study. Women who were simultaneously participating in another trial or exercise program, planning to give birth in a different hospital, or had no medical surveillance throughout pregnancy were not included in the study. All participants signed an informed consent.
After assessing women according to the aforementioned inclusion and exclusion criteria, they were randomly allocated to either intervention group (IG) or control group (CG) employing REDCap software. A computer-generated list of random numbers was used in order to ensure a blinded randomization sequence, and the access to the REDCap software for randomization was performed by one health professional from each hospital.
2.3. Intervention Group
Women assigned to the intervention group received standard obstetric attention and a structured and supervised online moderate exercise intervention program three days a week (50–60 min/session) from the 8–10th week of pregnancy to the end of the third trimester, at the 38–39th week. Of the three sessions, two were carried out via Zoom 120 and the last session was carried out following YouTube videos, which had been previously 121 filmed by the physical activity professionals in our research group. The content of 122 the videos on YouTube were adapted to the weeks of pregnancy.
The exercise sessions were supervised by a qualified physical activity and sport science professional. The exercise program consisted of complementary and interrelated activities following a methodological model divided into seven components adapted to each trimester of pregnancy, previously established by our research group [
30]:
physical and emotional activation (gradual warm-up);
aerobic exercises;
light muscle strengthening;
coordination and balance;
stretching and relaxation exercises;
pelvic floor muscle strengthening;
final talk.
During the exercise sessions women used a heart rate (HR) monitor. HR was kept under 65–70% of the age-predicted maximum and rate of perceived exertion scale ranged from 12 to 14 (somewhat hard).
2.4. Control Group
Women in the control group attended regular scheduled visits to their obstetricians and midwives, usually every 4–5 weeks until the 36–38th week of gestation and then weekly until delivery. Despite being in the control group, women were not discouraged from exercising during pregnancy, but they were questioned every trimester about their exercise habits using a “Decision Algorithm” (by telephone) [
31] to control their PA levels.
This algorithm contained three questions about the follow-up, frequency, and volume of physical activity pregnant women carried out weekly. If pregnant women exercised excessively, that is, they followed a supervised or autonomous physical activity program three or more days a week, with a duration of over 20 min a day, they were kept out of the study.
Additionally, these women received physical activity and nutritional recommendations throughout pregnancy. They were asked about the amount of exercise they practiced once every trimester.
2.5. Outcomes
Data collected from the pregnant mother before pregnancy, during, and after pregnancy, in addition to data collected from the fetus and newborn, were obtained from the SELENE platform, which is used to manage all hospital obstetric records.
2.6. Primary Outcome
The primary outcome was the diagnosis of GDM. The National Diabetes Data Group criteria were followed and included a 50 g maternal glucose screen (MGS) at 24–28 weeks of gestation, which was used to determine plasma glucose 1 h after a 50 g load of glucose administered orally. The screen test was considered positive when the values were equal or greater than 140 mg/dL. If the screen test was positive, the women were required to have a fasted oral glucose tolerance test (OGTT) before 30 weeks of gestation with data taken from medical records: 100 g of glucose load with blood samples taken fasted and at 1, 2 and 3 h post-glucose ingestion. Positive results were fasting glucose equal to or greater than 95 mg/dL, or values equal to or greater than 180 mg/dL at 1 h, equal to or greater than 155 mg/dL at 2 h, or equal to or greater than 140 mg/dL at 3h. Diagnosis of GDM occurred if there were at least two abnormal results in the OGTT.
2.7. Secondary Outcomes
Maternal characteristics collected were maternal age, weight, height, pre-pregnancy BMI, parity, smoking during pregnancy, occupation, and previous miscarriage. BMI was calculated as weight (kg) divided by height (m
2), and individuals were classified as underweight (BMI < 18.5 kg/m
2), normal weight (BMI < 18.5 to 24.9 kg/m
2), overweight (BMI ≥ 25 to 29.9 kg/m
2), and obese (BMI ≥ 30 kg/m
2) [
32].
Gestational weight gain was calculated based on pre-pregnancy weight and weight on the last medical visit before delivery. Childbirth data included maternal gestational age, mode of delivery (non-instrumental, instrumental, or c-section), birth weight, birth length, head circumference, and Apgar Scores 1 and 5 min. Excessive maternal weight gain was defined according to pre-pregnancy BMI [
33]. If pre-pregnancy BMI was below 18.5 kg/m
2, the healthy weight gain range was between 12.5 and 18 kg; if BMI was between 18.5 and 24.9 kg/m
2, the recommendation was between 11.5 and 16 kg; if BMI was between 25 and 29.9 kg/m
2, the healthy weight gain recommendation was between 7 and 11.5 kg; and if BMI was greater than 30 kg/m
2, the weight gain should be between 5 and 9 kg [
33]. All data were collected at the first prenatal visit by reviewing the medical records.
2.8. Power Sample Calculation
For the primary outcome (gestational diabetes mellitus) [
34], power calculations were based on earlier studies, and a prevalence of 8% and 25% was used in the intervention and usual care group, respectively. Following a two-sample comparison (χ
2) with a 5% level of significance and a statistical power of 0.90, the study population was set to 98 participants in each group. Assuming 25% lost to follow-up, we recruited 130 participants for each study group.
2.9. Statistical Analysis
Version 25.0 of IBM SPSS for Windows (IBM Corporation, Armonk, NY, USA) was utilized for the statistical analysis. Screening for the hypothesis of normality was performed using the Kolmogorov–Smirnov test.
Pearson’s chi-square test was used to compare maternal characteristics at baseline (number of participants by BMI subcategory, parity, maternal smoking during pregnancy, occupation, and previous miscarriages), cases of diagnosed gestational diabetes mellitus, number of abnormal glucose screenings, number of excessive maternal weight gains according to pre-pregnancy BMI, and mode of delivery between groups. Standardized adjusted residuals were used to complete and interpret with precision the observed association. Binary logistic regressions were used to assess risk estimation (odds ratio (OR)) of GDM in relation to IG and CG.
Independent t-tests were conducted to assess differences in maternal age, weight, height, maternal weight and gestational weight gain at glucose screening, final maternal weight, final gestational weight gain, gestational age at the beginning of the program, at glucose screening, and at delivery, basal glucose at 50 g OGTT, O’Sullivan values, basal glucose at 75 g OGTT, 60 min OGTT, 120 in OGTT, 180 min OGTT, birth weight, birth length, head circumference, Apgar Scores 1 and 5 min, between the IG and CG. This same test was used within GDM diagnosis or not for maternal weight at glucose screening, final maternal weight birth weight, birth length, head circumference, and Apgar Scores 1 and 5 min between IG and CG. The effect size was obtained using Cohen’s d index.
Data for continuous variables are shown as means and standard deviations, and categorical variables are shown as frequencies and percentages. Analyses were performed under intention-to-treat principles. The risk level was set at 0.05.
4. Discussion
The purpose of the present study was to investigate the effect of an online structured exercise program throughout pregnancy on the prevention of GDM. This innovative method consisted of online group exercise sessions which combined different forms of physical exercise (aerobic, strength conditioning, coordination, or flexibility). Our findings suggest that the pregnant population can significantly benefit from joining an online group training session throughout pregnancy during the COVID-19 pandemic.
A major finding of this study is the significantly lower diagnosis of GDM in the IG compared to CG (4.9% vs. 16.8%, respectively) and the reduction in its overall risk by 74.5%. These results are in accordance with previous studies conducted by Koivusalo et al., where the prevalence of GDM in the IG was significantly lower compared to the CG (13.9% vs. 21.6%, respectively,
p = 0.044) [
35]. Similarly, Barakat et al. in 2018 showed that the prevalence of GDM was significantly higher in the CG compared to the IG (6.8% vs. 2.6%, respectively,
p = 0.033) [
28]. Possible mechanisms by which physical exercise reduces the risk of GDM include the increased energy expenditure and glucose consumption during exercise. During exercise, due to muscle contraction, a greater translocation of glucose transporter-4 (GLUT-4) to the muscle cell’s surface occurs. As a result, glucose uptake from the bloodstream increases, thereby reducing blood glucose levels and insulin resistance by not requiring as much insulin [
36]. Similarly, exercise increases adiponectin concentration, which improves cellular sensitivity to insulin, and reduces inflammatory markers associated with insulin resistance [
37]. Additionally, it has been demonstrated that physical exercise during pregnancy is effective in reducing maternal weight gain, which is one of the main risk factors in GDM [
28].
This study also found significant differences in the mode of delivery between groups (
p = 0.046), wherein instrumental and caesarean deliveries were more common among women in the CG than in IG (13.1% vs. 11.3%; 23.3% vs. 9.9%, respectively). These results are similar to previous literature where the percentage of caesarean and instrumental delivery was lower in the exercise group compared to control [
38]. In addition, Sanda et al. found that the odds of caesarean delivery were significantly lower in the high active group compared to the low active group, and that being in the high active group was associated with higher odds of vaginal delivery [
39]. The results obtained in our study could be explained by the COVID-19 [
23] pandemic, which may have further increased the sedentary behavior among pregnant women in the CG.
Further, final maternal weight and excessive maternal weight gain were higher in the CG. Previous interventions, and a recent systematic review and meta-analysis, also conclude that exercise interventions are effective in preventing excessive maternal weight gain [
28,
40,
41]. Reduced leptin concentrations in active women may be the mechanism behind reduced weight gain. Nevertheless, these results should be interpreted with caution because there is a limited number of RCTs which have studied the effect of physical exercise on maternal weight gain.
Moreover, our results showed higher values in the 50 g MGS in the CG, which called for the need to carry out the OGTT, with the associated higher health costs and the greater discomfort of women exposed to this 3 h test.
Furthermore, overall glucose levels were higher in the CG and more specifically, these were significantly higher in the 75 g OGTT measurements (basal, 60, 120, and 180 min). Our intervention has shown that exercise can be effective for maintaining lower glucose levels, which has also been demonstrated in previous literature
In addition, of the women diagnosed with GDM, pregnant women in the CG had higher weight at the time of measurement of diabetes and at the end of pregnancy, and their newborn had a larger birth length and head circumference. Thus, these data suggest that exercise during pregnancy may serve as a tool for controlling final weight and excessive weight gain in gestational diabetic mothers and their offspring.
Our findings indicate further benefits of exercise for the healthy pregnant population, which may be essential to reduce the prevalence of GDM and to prevent future comorbidities such as type 2 diabetes, cardiovascular diseases, or preeclampsia in the mother, in addition to birth trauma, hypoglycemia, or macrosomia in the newborn, and type 2 diabetes, obesity, or cardiovascular diseases in the offspring [
4,
7,
8,
9,
11,
12].
Overall, our findings confirm the results of a previous systematic review and meta-analysis, which concluded that exercise during pregnancy has a significant protective effect against GDM [
16]. However, further data on the relationship between maternal exercise, GDM, and the COVID-19 situation are needed.
We believe that this is the first study to connect an online structured and supervised exercise program with high adherence to the reduction in the prevalence and diagnosis of GDM, and the control and management of GDM limiting future comorbidities and ensuring an optimal quality of life throughout pregnancy, postpartum, and even the lifetime. Moreover, this RCT, which was intended as an intervention focused on lifestyle, confirms the benefit of physical exercise as a determinant element for the prevention and management of gestational diabetes mellitus. In summary, performing a physical exercise intervention with comprehensive lifestyle patterns may be necessary for the health of the pregnant population during a pandemic.
In conclusion, an online supervised exercise program throughout pregnancy, aiming to address the COVID-19 limitation, reduced rates and prevalence of GDM in healthy pregnant women. These results should be used with caution to recommend supervised exercise during healthy pregnancy as a preventive tool for GDM.



 ,
, 


{kind=link}