
Empirical Dietary Patterns Associated with Food Insecurity in U.S. Cancer Survivors: NHANES 1999–2018
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Demographic and Physical Health Covariates
2.3. Dietary Assessment Data
2.4. Cancer Status and Food Security Data
2.5. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Discovery Phase: Dietary Patterns Extraction
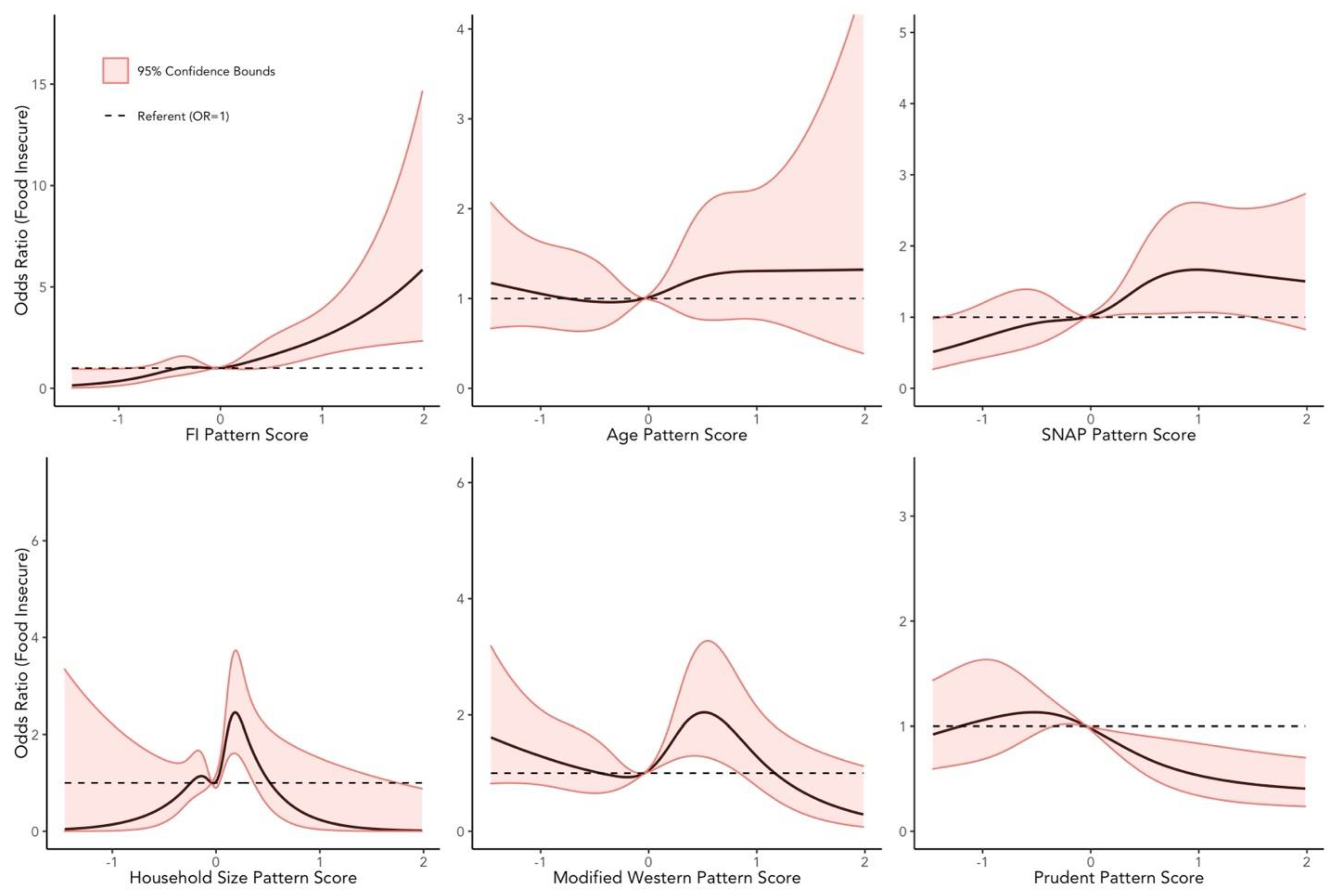
3.3. Validation Phase: Logistic Regression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Dietary Patterns Extraction Procedures: PCA
Appendix A.2. Dietary Patterns Extraction: Penalized Logistic Regression
References
- Coleman-Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2019. Available online: http://www.ers.usda.gov/publications/pub-details/?pubid=99281 (accessed on 12 August 2021).
- Charkhchi, P.; Fazeli Dehkordy, S.; Carlos, R.C. Housing and Food Insecurity, Care Access, and Health Status among the Chronically Ill: An Analysis of the Behavioral Risk Factor Surveillance System. J. Gen. Intern. Med. 2018, 33, 644–650. [Google Scholar] [CrossRef] [Green Version]
- Kudre, D.; Chen, Z.; Richard, A.; Cabaset, S.; Dehler, A.; Schmid, M.; Rohrmann, S. Multidisciplinary Outpatient Cancer Rehabilitation Can Improve Cancer Patients’ Physical and Psychosocial Status—A Systematic Review. Curr. Oncol. Rep. 2020, 22, 122. [Google Scholar] [CrossRef]
- Mariotto, A.B.; Enewold, L.; Zhao, J.; Zeruto, C.A.; Yabroff, K.R. Medical Care Costs Associated with Cancer Survivorship in the United States. Cancer Epidemiol. Biomark. Prev. 2020, 29, 1304–1312. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Zhao, J.; Zheng, Z.; de Moor, J.S.; Virgo, K.S.; Yabroff, K.R. Medical Financial Hardship Intensity and Financial Sacrifice Associated with Cancer in the United States. Cancer Epidemiol. Biomark. Prev. 2020, 29, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Simmons, L.A.; Modesitt, S.C.; Brody, A.C.; Leggin, A.B. Food Insecurity among Cancer Patients in Kentucky: A Pilot Study. J. Oncol. Pract. 2006, 2, 7. [Google Scholar] [CrossRef]
- NCI’s Dictionary of Cancer Terms. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/survivor (accessed on 24 October 2022).
- Gany, F.; Leng, J.; Ramirez, J.; Phillips, S.; Aragones, A.; Roberts, N.; Mujawar, M.I.; Costas-Muñiz, R. Health-Related Quality of Life of Food-Insecure Ethnic Minority Patients With Cancer. J. Oncol. Pract. 2015, 11, 396–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The American Institute for Cancer Research; World Cancer Research Fund. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective, 3rd ed.; The American Institute for Cancer Research: Washington, DC, USA; World Cancer Research Fund: London, UK, 2018. [Google Scholar]
- Thompson, K.L.; Elliott, L.; Fuchs-Tarlovsky, V.; Levin, R.M.; Voss, A.C.; Piemonte, T. Oncology Evidence-Based Nutrition Practice Guideline for Adults. J. Acad. Nutr. Diet. 2017, 117, 297–310.e47. [Google Scholar] [CrossRef]
- Pekmezi, D.W.; Demark-Wahnefried, W. Updated Evidence in Support of Diet and Exercise Interventions in Cancer Survivors. Acta Oncol. 2011, 50, 167–178. [Google Scholar] [CrossRef] [Green Version]
- Balhareth, A.; Aldossary, M.Y.; McNamara, D. Impact of Physical Activity and Diet on Colorectal Cancer Survivors’ Quality of Life: A Systematic Review. World J. Surg. Oncol. 2019, 17, 153. [Google Scholar] [CrossRef] [Green Version]
- Wayne, S.J.; Baumgartner, K.; Baumgartner, R.N.; Bernstein, L.; Bowen, D.J.; Ballard-Barbash, R. Diet Quality Is Directly Associated with Quality of Life in Breast Cancer Survivors. Breast Cancer Res. Treat. 2006, 96, 227–232. [Google Scholar] [CrossRef]
- Zhang, F.; Tapera, T.M.; Gou, J. Application of a New Dietary Pattern Analysis Method in Nutritional Epidemiology. BMC Med. Res. Methodol. 2018, 18, 119. [Google Scholar] [CrossRef] [PubMed]
- McEligot, A.J.; Poynor, V.; Sharma, R.; Panangadan, A. Logistic LASSO Regression for Dietary Intakes and Breast Cancer. Nutrients 2020, 12, 2652. [Google Scholar] [CrossRef] [PubMed]
- Curtin, L.R.; Mohadjer, L.K.; Dohrmann, S.M.; Kruszon-Moran, D.; Mirel, L.B.; Carroll, M.D.; Hirsch, R.; Burt, V.L.; Johnson, C.L. National Health and Nutrition Examination Survey: Sample Design, 2007–2010; Vital and Health Statistics Series, 2; United States Department of Health and Human Services: Washington, DC, USA; Centers for Disease Control and Prevention: Atlanta, GA, USA; National Center for Health Statistics: Hyattsville, MD, USA, 2013; pp. 1–23.
- About the National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 24 October 2022).
- Yaghjyan, L.; Wijayabahu, A.T.; Egan, K.M. RE: The Association between Dietary Quality and Overall and Cancer-Specific Mortality among Cancer Survivors, NHANES III. JNCI Cancer Spectr. 2018, 2, pky044. [Google Scholar] [CrossRef]
- Wolfe, A.M.; Lee, J.A.; Laurson, K.R. Socioeconomic Status and Physical Fitness in Youth: Findings from the NHANES National Youth Fitness Survey. J. Sports Sci. 2020, 38, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S. The Association of Active and Passive Smoking with Peripheral Arterial Disease: Results from NHANES 1999–2004. Angiology 2009, 60, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Dietary Guidelines Advisory Committee; OverDrive, Inc. Dietary Guidelines for Americans 2015–2020; United States Department of Health and Human Services: Washington, DC, USA; United States Department of Agriculture: Washington, DC, USA, 2016; ISBN 978-0-16-093465-0.
- Zhao, H.; Pan, Y.; Wang, C.; Guo, Y.; Yao, N.; Wang, H.; Li, B. The Effects of Metal Exposures on Charlson Comorbidity Index Using Zero-Inflated Negative Binomial Regression Model: NHANES 2011–2016. Biol. Trace Elem. Res. 2021, 199, 2104–2111. [Google Scholar] [CrossRef] [PubMed]
- Tucker, L.A. Physical Activity and Telomere Length in U.S. Men and Women: An NHANES Investigation. Prev. Med. 2017, 100, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Blanton, C.A.; Moshfegh, A.J.; Baer, D.J.; Kretsch, M.J. The USDA Automated Multiple-Pass Method Accurately Estimates Group Total Energy and Nutrient Intake. J. Nutr. 2006, 136, 2594–2599. [Google Scholar] [CrossRef] [Green Version]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method Reduces Bias in the Collection of Energy Intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [Green Version]
- Jovanovic, C.E.S.; Hoelscher, D.M.; Chen, B.; Ranjit, N.; van den Berg, A.E. The Associations of Plant-Based Food and Metabolic Syndrome Using NHANES 2015–16 Data. J. Public Health 2022, fdab403. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.; Murphy, M.M.; Keast, D.R.; Holick, M.F. Vitamin D Intake in the United States. J. Am. Diet. Assoc. 2004, 104, 980–983. [Google Scholar] [CrossRef] [PubMed]
- Montville, J.B.; Ahuja, J.K.C.; Martin, C.L.; Heendeniya, K.Y.; Omolewa-Tomobi, G.; Steinfeldt, L.C.; Anand, J.; Adler, M.E.; LaComb, R.P.; Moshfegh, A. USDA Food and Nutrient Database for Dietary Studies (FNDDS), 5.0. Procedia Food Sci. 2013, 2, 99–112. [Google Scholar] [CrossRef] [Green Version]
- Bowman, S.A.; Clemens, J.C.; Friday, J.E.; Moshfegh, A.J. Food Patterns Equivalents Database 2017–2018: Methodology and User Guide; Food Surveys Research Group, Beltsville Human Nutrition Research Center, Agricultural Research Service, U.S. Department of Agriculture: Beltsville, MD, USA, 2020. Available online: http://www.Ars.Usda.Gov/Nea/Bhnrc/Fsrg (accessed on 24 October 2022).
- Bowman, S.A.; Friday, J.E.; Moshfegh, A. My Pyramid Equivalents Database, 2.0 for USDA Survey Foods, 2003–2004; Food Surveys Research Group, Beltsville Human Nutrition Research Center, Agricultural Research Service, U.S. Department of Agriculture: Beltsville, MD, USA, 2008. Available online: http://www.Ars.Usda.Gov/Ba/Bhnrc/Fsrg (accessed on 24 October 2022).
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for Total Energy Intake in Epidemiologic Studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrova, D.; Catena, A.; Rodríguez-Barranco, M.; Redondo-Sánchez, D.; Bayo-Lozano, E.; Garcia-Retamero, R.; Jiménez-Moleón, J.-J.; Sánchez, M.-J. Physical Comorbidities and Depression in Recent and Long-Term Adult Cancer Survivors: NHANES 2007–2018. Cancers 2021, 13, 3368. [Google Scholar] [CrossRef]
- Bickel, G.; Nord, M.; Price, C.; Hamilton, W.; Cook, J. Guide to Measuring Household Food Security; U.S. Department of Agriculture: Washington, DC, USA, 2000.
- U.S. Household Food Insecurity Survey Module: Three-Stage Design, with Screeners. Available online: https://www.ers.usda.gov/media/8271/hh2012.pdf (accessed on 24 October 2022).
- Lee, J.S.; Frongillo, E.A. Nutritional and Health Consequences Are Associated with Food Insecurity among U.S. Elderly Persons. J. Nutr. 2001, 131, 1503–1509. [Google Scholar] [CrossRef] [Green Version]
- Kohn, M.J.; Bell, J.F.; Grow, H.M.G.; Chan, G. Food Insecurity, Food Assistance and Weight Status in US Youth: New Evidence from NHANES 2007–08: Food Insecurity, Assistance and Weight. Pediatr. Obes. 2014, 9, 155–166. [Google Scholar] [CrossRef]
- Johnson, C.; Paulose-Ram, R.; Ogden, C.L.; Carroll, M.; Kruszan-Moran, D.; Dohrmann, S.; Curtin, L. National Health and Nutrition Examination Survey. Analytics Guidelines, 1999–2010; Vital and Health Statistics Series 2; United States Department of Health and Human Services: Washington, DC, USA; Centers for Disease Control and Prevention: Atlanta, GA, USA; National Center for Health Statistics: Hyattsville, MD, USA, 2013; pp. 1–16.
- Goldberg, R. PROC FACTOR: How to Interpret the Output of a Realworld Example. Available online: https://support.sas.com/resources/papers/proceedings/proceedings/sugi22/STATS/PAPER268.PDF (accessed on 24 October 2022).
- Tsuruga, K.; Sugawara, N.; Sato, Y.; Saito, M.; Furukori, H.; Nakagami, T.; Nakamura, K.; Takahashi, I.; Nakaji, S.; Yasui-Furukori, N. Dietary Patterns and Schizophrenia: A Comparison with Healthy Controls. Neuropsychiatr. Dis. Treat. 2015, 11, 1115–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp, W. How Western Diet And Lifestyle Drive The Pandemic Of Obesity And Civilization Diseases. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzam, A. Is the World Converging to a ‘Western Diet’? Public Health Nutr. 2021, 24, 309–317. [Google Scholar] [CrossRef]
- Arthur, A.E.; Peterson, K.E.; Rozek, L.S.; Taylor, J.M.G.; Light, E.; Chepeha, D.B.; Hébert, J.R.; Terrell, J.E.; Wolf, G.T.; Duffy, S.A.; et al. Pretreatment Dietary Patterns, Weight Status, and Head and Neck Squamous Cell Carcinoma Prognosis. Am. J. Clin. Nutr. 2013, 97, 360–368. [Google Scholar] [CrossRef] [PubMed]
- El Zein, A.; Colby, S.E.; Zhou, W.; Shelnutt, K.P.; Greene, G.W.; Horacek, T.M.; Olfert, M.D.; Mathews, A.E. Food Insecurity Is Associated with Increased Risk of Obesity in US College Students. Curr. Dev. Nutr. 2020, 4, nzaa120. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.; Laska, M.N.; Neumark-Sztainer, D. Food Insecurity, Diet Quality, Home Food Availability, and Health Risk Behaviors Among Emerging Adults: Findings From the EAT 2010–2018 Study. Am. J. Public Health 2020, 110, 1422–1428. [Google Scholar] [CrossRef]
- Eicher-Miller, H.A.; Zhao, Y. Evidence for the Age-Specific Relationship of Food Insecurity and Key Dietary Outcomes among US Children and Adolescents. Nutr. Res. Rev. 2018, 31, 98–113. [Google Scholar] [CrossRef]
- Shi, Y.; Davies, A.; Allman-Farinelli, M. The Association between Food Insecurity and Dietary Outcomes in University Students: A Systematic Review. J. Acad. Nutr. Diet. 2021, 121, 2475–2500.e1. [Google Scholar] [CrossRef] [PubMed]
- Faught, E.L.; Williams, P.L.; Willows, N.D.; Asbridge, M.; Veugelers, P.J. The Association between Food Insecurity and Academic Achievement in Canadian School-Aged Children. Public Health Nutr. 2017, 20, 2778–2785. [Google Scholar] [CrossRef] [Green Version]
- Mello, J.A.; Gans, K.M.; Risica, P.M.; Kirtania, U.; Strolla, L.O.; Fournier, L. How Is Food Insecurity Associated with Dietary Behaviors? An Analysis with Low-Income, Ethnically Diverse Participants in a Nutrition Intervention Study. J. Am. Diet. Assoc. 2010, 110, 1906–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Li, Z.; Gao, Q.; Zhao, H.; Chen, S.; Huang, L.; Wang, W.; Wang, T. A Review of Statistical Methods for Dietary Pattern Analysis. Nutr. J. 2021, 20, 37. [Google Scholar] [CrossRef]
- Jung, N.M.; de Bairros, F.S.; Pattussi, M.P.; Pauli, S.; Neutzling, M.B. Gender Differences in the Prevalence of Household Food Insecurity: A Systematic Review and Meta-Analysis. Public Health Nutr. 2017, 20, 902–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, M.A.; Lippert, A.M. Feeding Her Children, but Risking Her Health: The Intersection of Gender, Household Food Insecurity and Obesity. Soc. Sci. Med. 2012, 74, 1754–1764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, B.; Jones, A.; Love, D.; Puckett, S.; Macklin, J.; White-Means, S. Exploring Mediators of Food Insecurity and Obesity: A Review of Recent Literature. J. Community Health 2012, 37, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Lohman, B.J.; Neppl, T.K.; Lee, Y.; Diggs, O.N.; Russell, D. The Association between Household Food Insecurity and Body Mass Index: A Prospective Growth Curve Analysis. J. Pediatr. 2018, 202, 115–120.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nettle, D.; Andrews, C.; Bateson, M. Food Insecurity as a Driver of Obesity in Humans: The Insurance Hypothesis. Behav. Brain Sci. 2017, 40, e105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmusson, G.; Lydecker, J.A.; Coffino, J.A.; White, M.A.; Grilo, C.M. Household Food Insecurity Is Associated with Binge-Eating Disorder and Obesity. Int. J. Eat. Disord. 2019, 52, 28–35. [Google Scholar] [CrossRef] [Green Version]
- Trego, M.L.; Baba, Z.M.; DiSantis, K.I.; Longacre, M.L. Food Insecurity among Adult Cancer Survivors in the United States. J. Cancer Surviv. 2019, 13, 641–652. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.G.; Borno, H.T.; Seligman, H.K. Food Insecurity Screening: A Missing Piece in Cancer Management. Cancer 2019, 125, 3494–3501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gany, F.; Lee, T.; Ramirez, J.; Massie, D.; Moran, A.; Crist, M.; McNish, T.; Winkel, G.; Leng, J.C.F. Do Our Patients Have Enough to Eat?: Food Insecurity among Urban Low-Income Cancer Patients. J. Health Care Poor Underserved 2014, 25, 1153–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gany, F.; Bari, S.; Crist, M.; Moran, A.; Rastogi, N.; Leng, J. Food Insecurity: Limitations of Emergency Food Resources for Our Patients. J. Urban Health N. Y. Acad. Med. 2013, 90, 552–558. [Google Scholar] [CrossRef] [Green Version]
- McConville, K. Improved Estimation for Complex Surveys Using Modern Regression Techniques; Colorado State University: Fort Collins, CO, USA, 2011. [Google Scholar]
- McConville, K.S.; Breidt, F.J.; Lee, T.C.M.; Moisen, G.G. Model-Assisted Survey Regression Estimation with the Lasso. J. Surv. Stat. Methodol. 2017, 5, 131–158. [Google Scholar] [CrossRef] [Green Version]
- Fransen, H.P.; May, A.M.; Stricker, M.D.; Boer, J.M.A.; Hennig, C.; Rosseel, Y.; Ocké, M.C.; Peeters, P.H.M.; Beulens, J.W.J. A Posteriori Dietary Patterns: How Many Patterns to Retain? J. Nutr. 2014, 144, 1274–1282. [Google Scholar] [CrossRef] [Green Version]
- Kant, A.K. Dietary Patterns and Health Outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef]
- Abdi, H.; Williams, L.J. Principal Component Analysis: Principal Component Analysis. Wiley Interdiscip. Rev. Comput. Stat. 2010, 2, 433–459. [Google Scholar] [CrossRef]
- Lumley, T. Analysis of Complex Survey Samples. J. Stat. Softw. 2004, 9, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Soc. Ser. B Methodol. 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Hastie, T.; Qian, J.; Tay, K. An Introduction to ‘Glmnet’. 2021. Available online: https://glmnet.stanford.edu/articles/glmnet.html (accessed on 24 October 2022).




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Survivors (n = 3317) | Food Insecure (n = 433) | Food Secure (n = 2884) | p |
|---|---|---|---|---|
| Age | <0.01 | |||
| Mean (SD) | 62.6 (14.8) | 50.8 (15.7) | 64.1 (14) | |
| Sex | <0.01 | |||
| Male | 1527 (40.9) | 143 (24.5) | 1384 (42.9) | |
| Female | 1790 (59.1) | 290 (75.5) | 1500 (57.1) | |
| Race/Ethnicity | <0.01 | |||
| Mexican American | 235 (2.7) | 67 (9.2) | 168 (1.9) | |
| Other Hispanic | 183 (2.6) | 48 (5.8) | 135 (2.2) | |
| Non-Hispanic White | 2219 (84.3) | 208 (68.3) | 2011 (86.3) | |
| Non-Hispanic Black | 534 (6.9) | 88 (11.2) | 446 (6.4) | |
| Other/Multiracial | 146 (3.5) | 22 (5.5) | 124 (3.2) | |
| Education Attained | <0.01 | |||
| ≤High School | 1577 (36.8) | 279 (59.3) | 1298 (34.1) | |
| ≥Some College | 1737 (63.2) | 152 (40.7) | 1585 (65.9) | |
| FIPR | <0.01 | |||
| ≥1.3 | 2279 (82.2) | 128 (39.1) | 2151 (87.6) | |
| <1.3 | 800 (17.8) | 288 (60.9) | 512 (12.4) | |
| Household Size | <0.01 | |||
| <5 Persons | 3027 (92.3) | 345 (79.3) | 2682 (93.9) | |
| ≥5 Persons | 290 (7.7) | 88 (20.7) | 202 (6.1) | |
| BMI (kg/m2) | 0.23 | |||
| Mean (SD) | 29.2 (6.6) | 29.7 (7.2) | 29.1 (6.5) | |
| Weekly MET Minutes | <0.01 | |||
| Mean (SD) | 2314.2 (4475.2) | 4641.1 (7771) | 2034.9 (3804.1) | |
| Daily Caloric Intake (kcal) | <0.01 | |||
| Mean (SD) | 1894.6 (687) | 1711.1 (740.2) | 1917 (677.0) | |
| Charlson Comorbidity Score | <0.01 | |||
| Mean (SD) | 3.0 (1.4) | 3.3 (1.8) | 3.0 (1.4) | |
| SNAP Assistance | <0.01 | |||
| No | 2839 (88.6) | 220 (49.9) | 2619 (93.3) | |
| Yes | 478 (11.4) | 213 (50.1) | 265 (6.7) | |
| Cancer Site | <0.01 | |||
| Breast | 563 (17.2) | 58 (10.2) | 505 (18.0) | |
| Gastrointestinal | 321 (7.7) | 45 (11.3) | 276 (7.3) | |
| Genitourinary | 145 (3.7) | 15 (3.7) | 130 (3.7) | |
| Gynecological | 522 (17.8) | 132 (38.1) | 390 (15.3) | |
| Male Reproductive | 620 (13.8) | 50 (6.0) | 570 (14.7) | |
| Melanoma | 240 (9.3) | 15 (2.0) | 225 (10.2) | |
| Other | 592 (19.1) | 99 (23.1) | 493 (18.6) | |
| Years Since Diagnosis | 0.53 | |||
| <2 years | 817 (22.0) | 113 (21.4) | 704 (22) | |
| ≥2 and <6 years | 1991 (64.4) | 257 (67.4) | 1734 (64.1) | |
| ≥6 years | 497 (13.6) | 60 (11.2) | 437 (13.9) | |
| Smoking Status | <0.01 | |||
| Current | 517 (16.4) | 142 (37.8) | 375 (13.8) | |
| Former | 1347 (38.9) | 120 (26.8) | 1227 (40.4) | |
| Never | 1451 (44.7) | 170 (35.4) | 1281 (45.8) | |
| Alcohol Use | 0.13 | |||
| Heavy | 323 (12.8) | 29 (6.6) | 294 (13.6) | |
| Moderate | 498 (16.1) | 48 (15.0) | 450 (16.2) | |
| None-drinking | 2496 (71.1) | 356 (78.5) | 2140 (70.2) | |
| Pattern | Food Insecurity (FI) † | Age † | Food Assistance (SNAP) † | Household Size † | Modified Western ‡ | Prudent ‡ |
|---|---|---|---|---|---|---|
| Food Groups | ||||||
| Processed Meats | −0.05 | −0.01 | 0.04 | 0.03 | 0.12 | −0.22 |
| Meats | 0.22 | −0.03 | 0.08 | 0.00 | 0.07 | −0.17 |
| Poultry | 0.00 | −0.26 | −0.08 | 0.20 | −0.03 | 0.35 |
| Seafood—High n-3 | −0.16 | 0.05 | −0.11 | −0.06 | −0.04 | 0.30 |
| Seafood—Low n-3 | −0.17 | 0.08 | −0.06 | −0.16 | −0.04 | 0.07 |
| Eggs | 0.07 | 0.11 | 0.00 | 0.15 | 0.24 | 0.07 |
| Solid Fats | 0.12 | 0.04 | 0.22 | −0.12 | 0.21 | −0.46 |
| Oils | −0.26 | 0.04 | −0.24 | 0.09 | 0.34 | 0.12 |
| Milk | −0.10 | 0.37 | 0.00 | −0.19 | −0.06 | 0.12 |
| Yogurt | −0.09 | 0.05 | −0.10 | −0.32 | 0.07 | 0.35 |
| Cheese | −0.06 | −0.39 | 0.05 | −0.19 | 0.34 | −0.28 |
| Alcohol | −0.19 | −0.27 | −0.34 | −0.09 | −0.36 | −0.16 |
| Fruit—Other | −0.23 | 0.41 | −0.24 | −0.33 | 0.03 | 0.49 |
| Fruit—Citrus, melons, and berries | −0.20 | 0.18 | −0.19 | −0.36 | 0.04 | 0.50 |
| Tomatoes | −0.21 | 0.04 | −0.17 | −0.36 | 0.48 | 0.14 |
| Dark-Green Vegetables | −0.21 | −0.19 | −0.26 | −0.22 | 0.26 | 0.53 |
| Dark-Yellow Vegetables | −0.16 | 0.10 | −0.34 | −0.06 | 0.14 | 0.45 |
| Other Vegetables | −0.50 | 0.17 | −0.65 | −0.48 | 0.46 | 0.45 |
| Potatoes | 0.41 | 0.25 | 0.06 | 0.05 | 0.16 | −0.04 |
| Other Starchy Vegetables | −0.03 | 0.16 | −0.11 | −0.15 | −0.12 | 0.17 |
| Legumes | 0.01 | −0.24 | 0.21 | 0.23 | 0.04 | −0.08 |
| Soy | −0.08 | −0.11 | −0.20 | 0.22 | 0.08 | 0.21 |
| Refined Grains | −0.13 | −0.12 | 0.17 | 0.13 | 0.11 | −0.34 |
| Whole Grains | −0.20 | 0.47 | −0.25 | −0.27 | −0.05 | 0.38 |
| Nuts | −0.28 | 0.10 | −0.31 | −0.02 | 0.18 | 0.19 |
| Added Sugars | 0.76 | −0.28 | 0.64 | 0.48 | −0.32 | −0.27 |
| FI | -- | |||||
| Age | −0.28 | -- | ||||
| SNAP | 0.80 | −0.37 | -- | |||
| Household Size | 0.63 | −0.50 | 0.62 | -- | ||
| Modified Western | −0.26 | 0.09 | −0.29 | −0.31 | -- | |
| Prudent | −0.40 | 0.35 | −0.56 | −0.41 | 0.16 | -- |
| Food Insecurity (FI) Pattern † | Age Pattern † | Food Assistance (SNAP) Pattern † | Household Size Pattern † | Modified Western ‡ | Prudent ‡ | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M1 (n = 1658) | M2 (n = 1659) | M1 (n = 1658) | M2 (n = 1659) | M1 (n = 1658) | M2 (n = 1659) | M1 (n = 1658) | M2 (n = 1659) | M1 (n = 1658) | M2 (n = 1659) | M1 (n = 1658) | M2 (n = 1659) | |
| Age | ** | ** | ** | ** | ** | |||||||
| Mean (SD) | 64.1 (13.5) | 61.1 (15.9) | 58.6 (14.9) | 67.4 (13.1) | 64.5 (13.3) | 60.5 (16.0) | 65.2 (13.3) | 59.8 (15.8) | 63 (15.1) | 62.3 (14.5) | 60.3 (15.4) | 65.1 (13.6) |
| Sex | * | ** | ||||||||||
| Male | 752 (41.0) | 775 (40.8) | 741 (41.1) | 786 (40.6) | 762 (41.1) | 765 (40.6) | 741 (38.9) | 786 (43.0) | 821 (44.1) | 706 (38.2) | 836 (46.9) | 691 (34.4) |
| Female | 906 (59.0) | 884 (59.2) | 917 (58.9) | 873 (59.4) | 896 (58.9) | 894 (59.4) | 917 (61.1) | 873 (57.0) | 837 (55.9) | 953 (61.8) | 822 (53.1) | 968 (65.6) |
| Race/Ethnicity | * | ** | ** | ** | ** | * | ||||||
| Minority | 513 (14.2) | 585 (17.2) | 663 (18.2) | 435 (12.6) | 474 (12.8) | 624 (18.8) | 428 (11.8) | 670 (19.8) | 639 (19.3) | 459 (12.6) | 528 (14.2) | 570 (17.3) |
| White | 1145 (85.8) | 1074 (82.8) | 995 (81.8) | 1224 (87.4) | 1184 (87.2) | 1035 (81.2) | 1230 (88.2) | 989 (80.2) | 1019 (80.7) | 1200 (87.4) | 1130 (85.8) | 1089 (82.7) |
| Education | ** | * | ** | ** | ** | |||||||
| ≤HS | 691 (31.5) | 886 (42.6) | 752 (34.4) | 825 (39.6) | 700 (30.3) | 877 (43.9) | 722 (33.3) | 855 (40.6) | 800 (37.6) | 777 (36.2) | 867 (40.2) | 710 (33.2) |
| ≥Some College | 966 (68.5) | 771 (57.4) | 905 (65.6) | 832 (60.4) | 957 (69.7) | 780 (56.1) | 934 (66.7) | 803 (59.4) | 856 (62.4) | 881 (63.8) | 791 (59.8) | 946 (66.8) |
| FIPR | ** | ** | ** | ** | * | |||||||
| ≥1.3 | 1214 (86.9) | 1065 (77.2) | 1104 (81.4) | 1175 (83.2) | 1232 (87.5) | 1047 (76.4) | 1189 (84.9) | 1090 (79.4) | 1100 (79.2) | 1179 (84.8) | 1089 (80.2) | 1190 (84.5) |
| <1.3 | 327 (13.1) | 473 (22.8) | 443 (18.6) | 357 (16.8) | 307 (12.5) | 493 (23.6) | 342 (15.1) | 458 (20.6) | 437 (20.8) | 363 (15.2) | 462 (19.8) | 338 (15.5) |
| Household size | ||||||||||||
| <5 Persons | 1547 (94.5) | 1480 (90.0) | 1460 (90.0) | 1567 (95.1) | 1563 (95.4) | 1464 (89.0) | 1557 (96.6) | 1470 (87.7) | 1495 (91.8) | 1532 (92.8) | 1482 (90.4) | 1545 (94.4) |
| ≥5 Persons | 111 (5.5) | 179 (10.0) | 198 (10.0) | 92 (4.9) | 95 (4.6) | 195 (11.0) | 101 (3.4) | 189 (12.3) | 163 (8.2) | 127 (7.2) | 176 (9.6) | 114 (5.6) |
| BMI | ||||||||||||
| Mean (SD) | 29.3 (6.6) | 29 (6.6) | 29.3 (6.8) | 29 (6.4) | 29 (6.3) | 29.4 (6.9) | 29.2 (6.3) | 29.1 (6.9) | 28.6 (6.2) | 29.7 (6.9) | 29.7 (6.9) | 28.6 (6.2) |
| Weekly MET Minutes | * | |||||||||||
| Mean (SD) | 2185.6 (3865.4) | 2454.4 (5054.7) | 2611.5 (4911.5) | 1959 (3862.2) | 2117.8 (3584.0) | 2529.2 (5274.0) | 2056.1 (3644.8) | 2593.5 (5214.2) | 2313.3 (4364.1) | 2314.9 (4567.9) | 2504.3 (5077.2) | 2108.2 (3705.2) |
| Daily Caloric Intake | ||||||||||||
| Mean (SD) | 1836.2 (660.8) | 1958.3 (709.2) | 1938.4 (696.4) | 1842.8 (672.3) | 1842.1 (655.0) | 1952.2 (716.2) | 1848 (655.0) | 1945.1 (716.8) | 1898.6 (705.1) | 1891.3 (671.6) | 2041.2 (746.9) | 1736.6 (575.7) |
| CCI | ||||||||||||
| Mean (SD) | 3.1 (1.4) | 3.0 (1.4) | 2.9 (1.3) | 3.1 (1.5) | 3.0 (1.4) | 3.0 (1.4) | 3.0 (1.4) | 3.0 (1.4) | 3.0 (1.4) | 3.0 (1.4) | 3.0 (1.4) | 3.0 (1.4) |
| Food Security | ||||||||||||
| Food Secure | 1482 (93.7) | 1357 (83.1) | 1351 (85.4) | 1488 (92.5) | 1512 (95.0) | 1327 (81.7) | 1476 (92.9) | 1363 (84.0) | 1379 (86.5) | 1460 (90.5) | 1352 (84.7) | 1487 (92.9) |
| Food Insecure | 176 (6.3) | 302 (16.9) | 307 (14.6) | 171 (7.5) | 146 (5.0) | 332 (18.3) | 182 (7.1) | 296 (16.0) | 279 (13.5) | 199 (9.5) | 306 (15.3) | 172 (7.1) |
| SNAP Assistance | * | |||||||||||
| No | 1482 (93.7) | 1357 (83.1) | 1351 (85.4) | 1488 (92.5) | 1512 (95.0) | 1327 (81.7) | 1476 (92.9) | 1363 (84.0) | 1379 (86.5) | 1460 (90.5) | 1352 (84.7) | 1487 (92.9) |
| Yes | 176 (6.3) | 302 (16.9) | 307 (14.6) | 171 (7.5) | 146 (5.0) | 332 (18.3) | 182 (7.1) | 296 (16.0) | 279 (13.5) | 199 (9.5) | 306 (15.3) | 172 (7.1) |
| Smoking Status | * | ** | ||||||||||
| Current | 188 (11.4) | 329 (21.9) | 344 (20.6) | 173 (11.4) | 191 (11.4) | 326 (21.9) | 179 (11.3) | 338 (21.9) | 284 (18.3) | 233 (14.8) | 393 (24.5) | 124 (7.6) |
| Former | 724 (42.3) | 623 (35.2) | 628 (36.3) | 719 (42.0) | 712 (42.6) | 635 (34.8) | 727 (43.0) | 620 (34.4) | 664 (38.6) | 683 (39.2) | 670 (37.8) | 677 (40.1) |
| Never | 745 (46.3) | 706 (43.0) | 685 (43.1) | 766 (46.6) | 754 (46.0) | 697 (43.3) | 750 (45.7) | 701 (43.6) | 709 (43.2) | 742 (46.0) | 594 (37.7) | 857 (52.2) |
| Alcohol Use | * | |||||||||||
| Heavy | 214 (16.3) | 109 (9.1) | 242 (18.9) | 81 (5.6) | 265 (20.7) | 58 (4.2) | 206 (16.1) | 117 (9.3) | 227 (19.9) | 96 (6.9) | 207 (15.2) | 116 (10.2) |
| Moderate | 272 (16.3) | 226 (15.9) | 264 (17.2) | 234 (14.8) | 294 (17.3) | 204 (14.8) | 266 (15.0) | 232 (17.3) | 276 (17.4) | 222 (15.0) | 250 (16.9) | 248 (15.3) |
| Non-drinking | 1172 (67.5) | 1324 (75.0) | 1152 (63.9) | 1344 (79.6) | 1099 (62.0) | 1397 (81.0) | 1186 (68.9) | 1310 (73.5) | 1155 (62.7) | 1341 (78.1) | 1201 (67.9) | 1295 (74.5) |
| Dietary Pattern a | Q1 | Q2 | Q3 | Q4 | Q5 | pQ5–Q1 | ptrend | HR bcontinuous | pcquadratic |
|---|---|---|---|---|---|---|---|---|---|
| Food Insecurity † | 1.00 | 1.09 (0.58–2.02) | 1.18 (0.57–2.45) | 1.91 (1.04–3.53) * | 2.42 (1.21–4.82) * | 0.01 * | <0.01 ** | 1.50 (1.19–1.90) ** | 0.11 |
| Age † | 1.00 | 1.91 (1.12–3.27) * | 1.41 (0.67–2.93) | 1.14 (0.49–2.69) | 1.82 (0.93–3.56) | 0.08 | 0.28 | 1.05 (0.87–1.27) | 0.57 |
| Food Assistance (SNAP) † | 1.00 | 1.38 (0.65–2.93) | 1.44 (0.77–2.71) | 2.54 (1.22–5.30) * | 2.23 (1.26–3.94) ** | <0.01 ** | <0.01 ** | 1.37 (1.12–1.68) ** | 0.46 |
| Household Size † | 1.00 | 1.63 (0.78–3.43) | 1.00 (0.52–1.92) | 2.77 (1.46–5.25) ** | 2.02 (0.98–4.18) | 0.06 | 0.01 * | 1.27 (1.04–1.54) * | 0.36 |
| Modified Western ‡ | 1.00 | 0.86 (0.48–1.51) | 0.69 (0.33–1.45) | 1.46 (0.81–2.64) | 1.33 (0.66–2.67) | 0.42 | 0.16 | 1.05 (0.88–1.25) | 0.70 |
| Prudent ‡ | 1.00 | 0.81 (0.37–1.78) | 1.09 (0.53–2.26) | 0.54 (0.26–1.10) | 0.40 (0.20–0.80) ** | <0.01 ** | <0.01 ** | 0.76 (0.63–0.92) ** | 0.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maino Vieytes, C.A.; Zhu, R.; Gany, F.; Burton-Obanla, A.; Arthur, A.E. Empirical Dietary Patterns Associated with Food Insecurity in U.S. Cancer Survivors: NHANES 1999–2018. Int. J. Environ. Res. Public Health 2022, 19, 14062. https://doi.org/10.3390/ijerph192114062
Maino Vieytes CA, Zhu R, Gany F, Burton-Obanla A, Arthur AE. Empirical Dietary Patterns Associated with Food Insecurity in U.S. Cancer Survivors: NHANES 1999–2018. International Journal of Environmental Research and Public Health. 2022; 19(21):14062. https://doi.org/10.3390/ijerph192114062
Chicago/Turabian StyleMaino Vieytes, Christian A., Ruoqing Zhu, Francesca Gany, Amirah Burton-Obanla, and Anna E. Arthur. 2022. "Empirical Dietary Patterns Associated with Food Insecurity in U.S. Cancer Survivors: NHANES 1999–2018" International Journal of Environmental Research and Public Health 19, no. 21: 14062. https://doi.org/10.3390/ijerph192114062