

To Vaccinate or Not to Vaccinate—Reasons of Willingness and Reluctance of Students against SARS-CoV-2 Vaccination—An International Experience
 , , , , ,
, , , , ,  , , ,
, , ,  , , , ,
, , , ,  , ,
, ,  , add
Show full author list
, add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Measures
3. Statistical Analysis
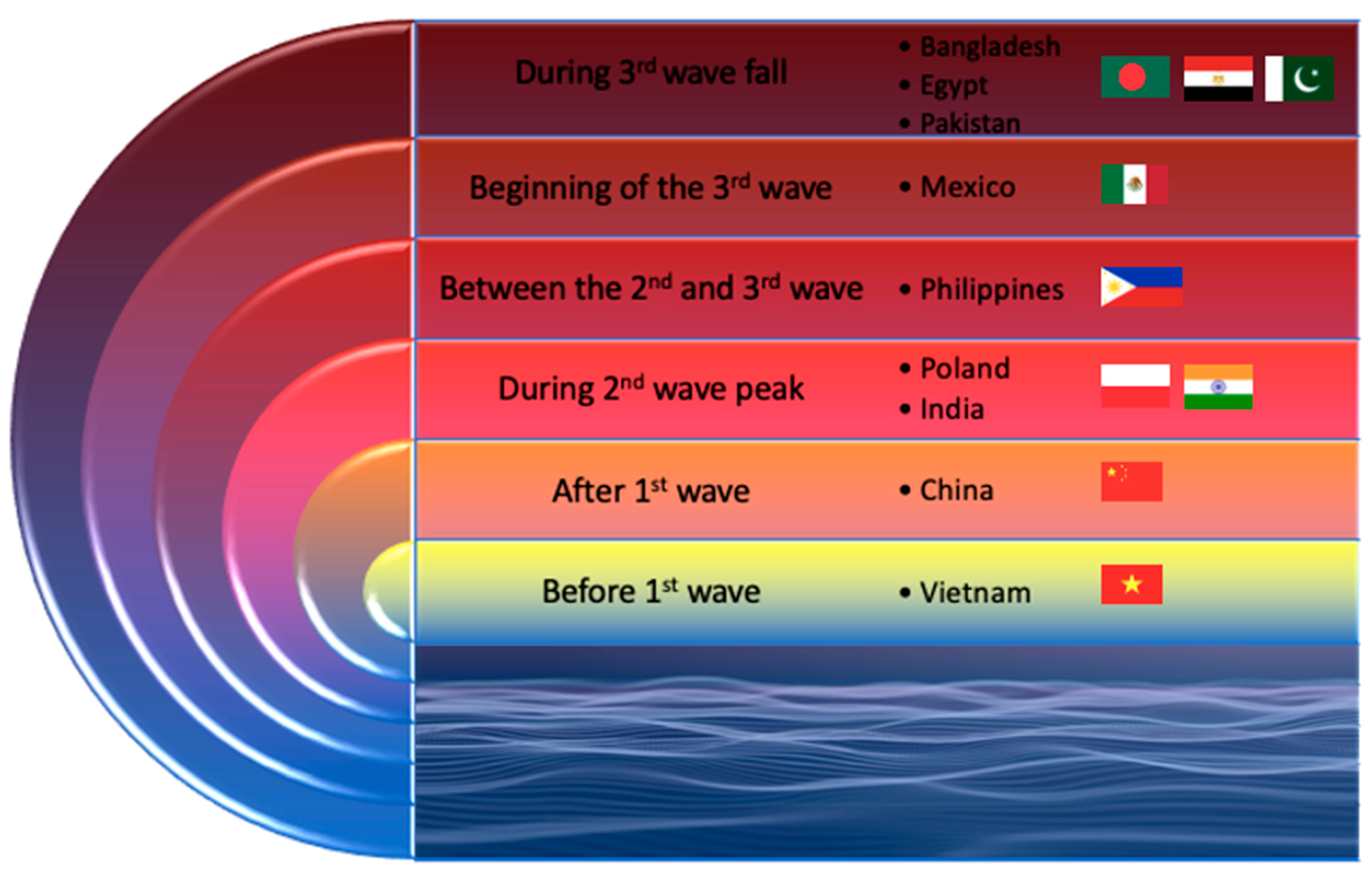
4. The Pandemic Situation during the Questionnaire Distribution
5. Results
5.1. Sociodemographic Characteristics
5.1.1. Gender and Age
5.1.2. Marital Status
5.1.3. Having Children
5.1.4. Place of Residence
5.1.5. Housing Situation
5.1.6. Working Status
5.1.7. Field of Study and Year of Study
5.1.8. Form of Studying
5.1.9. Use of Psychological/Psychiatric Services before the Pandemic
5.1.10. Use of Psychological/Psychiatric Services during the Pandemic
5.1.11. Supplements Intake
5.2. Attitudes toward Vaccinations
5.2.1. Vaccination against Influenza
5.2.2. Vaccinations against COVID-19
5.3. Differences in the Examined Variables between the Vaccinated and Unvaccinated Participants
5.3.1. Gender
5.3.2. Field of Study
5.3.3. Mode of Conducting Classes
5.3.4. Willingness to Vaccinate against COVID-19
5.4. Factors Related to the Willingness to Vaccinate against COVID-19 among Students
5.4.1. Gender
5.4.2. Marital Status
5.4.3. Having Children
5.4.4. Place of Residence
5.4.5. Housing Situation
5.4.6. Working Status
5.4.7. Field of Study
5.4.8. Mode of Conducting Classes
5.4.9. Use of Psychological/Psychiatric Services before the Pandemic
5.4.10. Use of Psychological/Psychiatric Services during the Pandemic
5.4.11. Supplements Intake
5.4.12. Vaccination against Influenza
5.5. The Most Common Reasons against COVID-19 Vaccination
6. Ethical Considerations
7. Strengths and Limitations of the Study
8. Discussion
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus Disease 2019 |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus-2 |
References
- Centers for Disease Control and Prevention (CDC). Ten great public health achievements–United States, 1900–1999. MMWR Morb. Mortal. Wkly. Rep. 1999, 48, 241–243. [Google Scholar]
- Black, S.; Rappuoli, R. A crisis of public confidence in vaccines. Sci. Transl. Med. 2010, 2, 61mr1. [Google Scholar] [CrossRef] [PubMed]
- Neely, S.R.; Eldredge, C.; Ersing, R.; Remington, C. Vaccine hesitancy and exposure to misinformation: A survey analysis. J. Gen. Intern. Med. 2021, 37, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Toth-Manikowski, S.M.; Swirsky, E.S.; Gandhi, R.; Piscitello, G. COVID-19 vaccination hesitancy among health care workers, communication, and policy-making. Am. J. Infect. Control 2022, 50, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Sekizawa, Y.; Hashimoto, S.; Denda, K.; Ochi, S.; So, M. Association between COVID-19 vaccine hesitancy and Generalized Trust, depression, generalized anxiety, and fear of COVID-19. BMC Public Health 2022, 22, 126. [Google Scholar] [CrossRef] [PubMed]
- Batra, K.; Sharma, M.; Dai, C.-L.; Khubchandani, J. COVID-19 Booster Vaccination Hesitancy in the United States: A Multi-Theory-Model (MTM)-Based National Assessment. Vaccines 2022, 10, 758. [Google Scholar] [CrossRef]
- Fan, J.; Wang, X.; Du, S.; Mao, A.; Du, H.; Qiu, W. Discussion of the Trust in Vaccination against COVID-19. Vaccines 2022, 10, 1214. [Google Scholar] [CrossRef]
- Finsterer, J. Neurological side effects of sars-cov-2 vaccinations. Acta Neurol. Scand. 2021, 145, 5–9. [Google Scholar] [CrossRef]
- Nguyen, T.D.; Mall, G.; Westphal, J.G.; Weingärtner, O.; Möbius-Winkler, S.; Schulze, P.C. Acute myocarditis after COVID-19 vaccination with mRNA-1273 in a patient with former SARS-COV-2 infection. ESC Heart Fail. 2021, 8, 4710–4714. [Google Scholar] [CrossRef]
- Singh, B.; Kaur, P.; Cedeno, L.; Brahimi, T.; Patel, P.; Virk, H.; Shamoon, F.; Bikkina, M. COVID-19 mrna vaccine and myocarditis. Eur. J. Case Rep. Intern. Med. 2021, 8, 002681. [Google Scholar] [CrossRef]
- Williams, C.B.; Choi, J.-I.; Hosseini, F.; Roberts, J.; Ramanathan, K.; Ong, K. Acute myocarditis following mrna-1273 SARS-COV-2 vaccination. CJC Open 2021, 3, 1410–1412. [Google Scholar] [CrossRef] [PubMed]
- Ashaari, S.; Sohaib, H.A.; Bolger, K. A case report: Symptomatic Pericarditis Post-COVID-19 vaccination. Eur. Heart J.-Case Rep. 2021, 5, ytab375. [Google Scholar] [CrossRef] [PubMed]
- Malayala, S.V.; Mohan, G.; Vasireddy, D.; Atluri, P. Purpuric rash and thrombocytopenia after the mRNA-1273 (moderna) COVID-19 vaccine. Cureus 2021, 13, e14099. [Google Scholar] [CrossRef]
- Bhan, C.; Bheesham, N.; Shakuntulla, F.; Sharma, M.; Sun, C.; Weinstein, M. An unusual presentation of acute deep vein thrombosis after the moderna COVID-19 vaccine—A case report. Ann. Transl. Med. 2021, 9, 1605. [Google Scholar] [CrossRef] [PubMed]
- Takase, B.; Hayashi, K.; Hisada, T.; Tsuchiya, T.; Masaki, N.; Nagata, M. Chest pain with new abnormal electrocardiogram development after injection of COVID-19 vaccine manufactured by Moderna. Intern. Med. 2022, 61, 2089–2090. [Google Scholar] [CrossRef]
- Kaikati, J.; Ghanem, A.; El Bahtimi, R.; Helou, J.; Tomb, R. Eosinophilic panniculitis: A new side effect of Sinopharm COVID-19 vaccine. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e337–e339. [Google Scholar] [CrossRef]
- Ogueji, I.A.; Okoloba, M.M. Underlying factors in the willingness to receive and barriers to receiving the COVID-19 vaccine among residents in the UK and Nigeria: A qualitative study. Curr. Psychol. 2022, 1–12. [Google Scholar] [CrossRef]
- Payberah, E.; Payberah, D.; Sarangi, A.; Gude, J. COVID-19 vaccine hesitancy in patients with mental illness: Strategies to overcome barriers—A review. J. Egypt. Public Health Assoc. 2022, 97, 1–6. [Google Scholar] [CrossRef]
- Wang, Y.; Duan, L.; Li, M.; Wang, J.; Yang, J.; Song, C.; Li, J.; Wang, J.; Jia, J.; Xu, J. COVID-19 vaccine hesitancy and associated factors among diabetes patients: A cross-sectional survey in Changzhi, Shanxi, China. Vaccines 2022, 10, 129. [Google Scholar] [CrossRef]
- Tsai, R.; Hervey, J.; Hoffman, K.; Wood, J.; Johnson, J.; Deighton, D.; Clermont, D.; Loew, B.; Goldberg, S.L. COVID-19 vaccine hesitancy and acceptance among individuals with cancer, autoimmune diseases, or other serious comorbid conditions: Cross-sectional, internet-based survey. JMIR Public Health Surveill. 2022, 8, e29872. [Google Scholar] [CrossRef]
- Ehde, D.M.; Roberts, M.K.; Humbert, A.T.; Herring, T.E.; Alschuler, K.N. COVID-19 vaccine hesitancy in adults with multiple sclerosis in the United States: A follow up survey during the initial vaccine rollout in 2021. Mult. Scler. Relat. Disord. 2021, 54, 103163. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, R.G.; Hagen, L.; Walker, K.; O’Leary, H.; Lengacher, C. The COVID-19 vaccine social media infodemic: Healthcare Providers’ missed dose in addressing misinformation and vaccine hesitancy. Hum. Vaccines Immunother. 2021, 17, 2962–2964. [Google Scholar] [CrossRef] [PubMed]
- Rathore, F.; Farooq, F. Information overload and Infodemic in the COVID-19 pandemic. J. Pak. Med. Assoc. 2020, 70, S162–S165. [Google Scholar] [CrossRef] [PubMed]
- Ghaddar, A.; Khandaqji, S.; Awad, Z.; Kansoun, R. Conspiracy beliefs and vaccination intent for COVID-19 in an infodemic. PLoS ONE 2022, 17, e0261559. [Google Scholar] [CrossRef]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef]
- Sun, S.; Lin, D.; Operario, D. Interest in COVID-19 vaccine trials participation among young adults in China: Willingness, reasons for hesitancy, and demographic and psychosocial determinants. medRxiv. 2020. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Guidry, J.P.D.; Laestadius, L.I.; Vraga, E.K.; Miller, C.A.; Perrin, P.B.; Burton, C.W.; Ryan, M.; Fuemmeler, B.F.; Carlyle, K.E. Willingness to get the COVID-19 vaccine with and without emergency use authorization. Am. J. Infect. Control 2021, 49, 137–142. [Google Scholar] [CrossRef]
- Gan, L.; Chen, Y.; Hu, P.; Wu, D.; Zhu, Y.; Tan, J.; Li, Y.; Zhang, D. Willingness to Receive SARS-CoV-2 Vaccination and Associated Factors among Chinese Adults: A Cross Sectional Survey. Int J Env. Res. Public Health 2021, 18, 1993. [Google Scholar] [CrossRef]
- Szmyd, B.; Bartoszek, A.; Karuga, F.F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical Students and SARS-CoV-2 Vaccination: Attitude and Behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef]
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.; Sanchis, J.; Bertomeu-González, V.; Fácila, L.; Ariza, A.; Núñez, J.; Cordero, A. The effect of age on mortality in patients with COVID-19: A meta-analysis with 611, 583 subjects. J. Am. Med. Dir. Assoc. 2020, 21, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.T.; Hanage, W.P.; Owusu-Boaitey, N.; Cochran, K.B.; Walsh, S.P.; Meyerowitz-Katz, G. Assessing the age specificity of infection fatality rates for COVID-19: Systematic review, meta-analysis, and public policy implications. Eur. J. Epidemiol. 2020, 35, 1123–1138. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, F.; Bor, A.; Petersen, M.B. Compliance without fear: Individual-level protective behaviour during the first wave of the COVID-19 pandemic. Br. J. Health Psychol. 2021, 26, 679–696. [Google Scholar] [CrossRef] [PubMed]
- van der Made, C.I.; Simons, A.; Schuurs-Hoeijmakers, J.; van den Heuvel, G.; Mantere, T.; Kersten, S.; van Deuren, R.C.; Steehouwer, M.; van Reijmersdal, S.V.; Jaeger, M.; et al. Presence of genetic variants among young men with severe COVID-19. JAMA 2020, 324, 663. [Google Scholar] [CrossRef]
- Nivette, A.; Ribeaud, D.; Murray, A.; Steinhoff, A.; Bechtiger, L.; Hepp, U.; Shanahan, L.; Eisner, M. Non-compliance with COVID-19-related public health measures among young adults in Switzerland: Insights from a longitudinal cohort study. Soc. Sci. Med. 2021, 268, 113370. [Google Scholar] [CrossRef]
- Haque, A.; Mumtaz, S.; Khattak, O.; Mumtaz, R.; Ahmed, A. Comparing the preventive behavior of medical students and physicians in the era of COVID-19: Novel Medical Problems Demand novel curricular interventions. Biochem. Mol. Biol. Educ. 2020, 48, 473–481. [Google Scholar] [CrossRef]
- Bhattacharyya, R.; Chatterjee, S.S.; Bhattacharyya, S.; Gupta, S.; Das, S.; Banerjee, B.B. Attitude, practice, behavior, and mental health impact of COVID-19 on doctors. Indian J. Psychiatry 2020, 62, 257. [Google Scholar] [CrossRef]
- Khubchandani, J.; Biswas, N.; Mustapha, T.; Talbert, S.; Dharamsi, S. COVID-19 vaccination refusal among college students: Global trends and action priorities. Brain Behav. Immun. 2022, 99, 218–222. [Google Scholar] [CrossRef]
- Baj, J.; Karakuła-Juchnowicz, H.; Teresiński, G.; Buszewicz, G.; Ciesielka, M.; Sitarz, R.; Forma, A.; Karakuła, K.; Flieger, W.; Portincasa, P.; et al. COVID-19: Specific and non-specific clinical manifestations and symptoms: The current state of knowledge. J. Clin. Med. 2020, 9, 1753. [Google Scholar] [CrossRef]
- Juchnowicz, D.; Baj, J.; Forma, A.; Karakuła, K.; Sitarz, R.; Bogucki, J.; Karakula-Juchnowicz, H. The outbreak of SARS-COV-2 pandemic and the well-being of Polish students: The risk factors of the emotional distress during COVID-19 lockdown. J. Clin. Med. 2021, 10, 944. [Google Scholar] [CrossRef]
- Sitarz, R.; Forma, A.; Karakuła, K.; Juchnowicz, D.; Baj, J.; Bogucki, J.; Karakuła-Juchnowicz, H. How do Polish students manage emotional distress during the COVID-19 lockdown? A web-based cross-sectional study. J. Clin. Med. 2021, 10, 4964. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.E.; Islam, M.S.; Ghose, T.K.; Jahan, H.; Chakrobortty, S.; Hossen, M.S.; Ema, N.S. COVID-19 vaccine acceptability among public university students in Bangladesh: Highlighting knowledge, perceptions, and attitude. Hum. Vaccines Immunother. 2021, 17, 5089–5098. [Google Scholar] [CrossRef] [PubMed]
- Pierwsze Szczepienia Przeciwko COVID-19 W Polsce Już Pod Koniec Grudnia-Szczepienie Przeciwko COVID-19-Portal Gov.Pl. Szczepienie Przeciwko COVID-19. 22 December 2020. Available online: https://www.gov.pl/web/szczepimysie/pierwsze-szczepienia-przeciwko-COVID-19-w-polsce-juz-pod-koniec-grudnia (accessed on 16 May 2022).
- Bari, M.S.; Hossain, M.J.; Ahmmed, F.; Sarker, M.M.; Khandokar, L.; Chaithy, A.P.; Aziz, F.; Mitra, S.; Emran, T.B.; Islam, M.S.; et al. Knowledge, perception, and willingness towards immunization among Bangladeshi population during COVID-19 vaccine rolling period. Vaccines 2021, 9, 1449. [Google Scholar] [CrossRef] [PubMed]
- Jain, L.; Vij, J.; Satapathy, P.; Chakrapani, V.; Patro, B.; Kar, S.S.; Singh, R.; Pala, S.; Sankhe, L.; Modi, B.; et al. Factors influencing COVID-19 vaccination intentions among college students: A cross-sectional study in India. Front. Public Health 2021, 9, 735902. [Google Scholar] [CrossRef]
- Jain, J.; Saurabh, S.; Kumar, P.; Verma, M.K.; Goel, A.D.; Gupta, M.K.; Bhardwaj, P.; Raghav, P.R. COVID-19 vaccine hesitancy among medical students in India. Epidemiol. Infect. 2021, 149, 1–28. [Google Scholar] [CrossRef]
- Capeding, M.R.; Tran, N.H.; Hadinegoro, S.R.; Ismail, H.I.; Chotpitayasunondh, T.; Chua, M.N.; Luong, C.Q.; Rusmil, K.; Wirawan, D.N.; Nallusamy, R.; et al. Clinical efficacy and safety of a novel tetravalent dengue vaccine in healthy children in Asia: A phase 3, randomised, observer-masked, placebo-controlled trial. Lancet 2014, 384, 1358–1365. [Google Scholar] [CrossRef]
- Villar, L.; Dayan, G.H.; Arredondo-García, J.L.; Rivera, D.M.; Cunha, R.; Deseda, C.; Reynales, H.; Costa, M.S.; Morales-Ramírez, J.O.; Carrasquilla, G.; et al. Efficacy of a tetravalent dengue vaccine in children in Latin America. N. Engl. J. Med. 2015, 372, 113–123. [Google Scholar] [CrossRef]
- Flasche, S.; Wilder-Smith, A.; Hombach, J.; Smith, P.G. Estimating the proportion of vaccine-induced hospitalized dengue cases among dengvaxia vaccinees in the Philippines. Wellcome Open Res. 2019, 4, 165. [Google Scholar] [CrossRef] [Green Version]
- Mendoza, R.U.; Dayrit, M.M.; Alfonso, C.R.; Ong, M.M. Public trust and the COVID-19 Vaccination Campaign: Lessons from the Philippines as it emerges from the Dengvaxia controversy. Int. J. Health Plan. Manag. 2021, 36, 2048–2055. [Google Scholar] [CrossRef]
- CHED. 💉COVID-19 Vaccination Update💉As of Feb 17, 89.34% of HEI Teaching and Non-Teaching Personnel and 69.32% of Tertiary Students are Now Vaccinated Against COVID-19. this Data was Based on Heis’ Reports Received by Chedros. Help Ph Reach Herd Immunity and Get Vaccinated Now. 24 February 2022. Available online: https://twitter.com/PhCHED/status/1496752726809608194 (accessed on 16 May 2022).
- Tee, M.L.; Tee, C.A.; Anlacan, J.P.; Aligam, K.J.G.; Reyes, P.W.C.; Kuruchittham, V.; Ho, R.C. Psychological impact of COVID-19 pandemic in the Philippines. J Affect Disord. 2020, 277, 379–391. [Google Scholar] [CrossRef]
- El-Monshed, A.H.; Loutfy, A.; Saad, M.T.; Ali, A.S.; El-Gilany, A.-H.; Soliman Mohamed, A.; Salah, M.; Zoromba, M. Satisfaction with life and psychological distress during the COVID-19 pandemic: An Egyptian online cross-sectional study. Afr. J. Prim. Health Care Fam. Med. 2022, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Bukhsh, A.; Rehman, H.; Mallhi, T.H.; Ata, H.; Rehman, I.U.; Lee, L.-H.; Goh, B.-H.; Khan, T.M. Parents’ attitude, awareness and behaviour towards influenza vaccination in Pakistan. Hum. Vaccines Immunother. 2018, 14, 952–957. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.M.; Mohammad, D.; Qureshi, M.F.; Abbas, M.Z.; Aleem, S. Prevalence, psychological responses and associated correlates of depression, anxiety and stress in a global population, during the coronavirus disease (COVID-19) pandemic. Community Ment. Health J. 2020, 57, 101–110. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Population | Total Cases | Daily New Cases | Active Cases | Total Deaths | Daily New Deaths | New Recoveries | |
|---|---|---|---|---|---|---|---|
Poland | 38,265,000 | 2,586,623 | 22,966 | 405,187 | 54,941 | 204 | 32,439 |
Bangladesh | 163,187,000 | 754,614 | 2955 | 73,504 | 11,305 | 77 | N/A |
India | 1,339,330,514 | 17,625,735 | 319,435 | 2,879,642 | 200,751 | 2845 | 248,702 |
Mexico | 128,600,000 | 2,519,269 | 6105 | 285,692 | 227,807 | 61 | 3149 |
Egypt | 100,000,408 | 261,666 | 1007 | 55,144 | 15,047 | 46 | N/A |
Philippines | 106,651,394 | 1,165,145 | 6090 | 52,000 | 19,622 | 116 | N/A |
Pakistan | 238,181,034 | 922,824 | 1771 | 57,336 | 20,850 | 71 | 3397 |
Vietnam | 102,789,598 | 2905 | 0 | 361 | 35 | 0 | N/A |
China | 1,411,778,724 | 90,468 | 11 | 299 | 4636 | 0 | N/A |
| COVID-19 Vaccine Policy during Conducting the Study | |||
|---|---|---|---|
| Were vaccinations for students compulsory at the time of the study? | Fields of study where it was mandatory to vaccinate | Vaccine company by which students were vaccinated at the time of conducting the study most often | |
| Poland | yes | medical students | Pfizer, Moderna |
| Bangladesh | no | not applicable | Sinopharm, AstraZeneca, Pfizer, and Moderna were distributed in the different regions. |
| India | no | not applicable | not applicable |
| Mexico | no | not applicable | Pfizer for the pediatric population. Pfizer-BioNTech, Cansino, COVAX, AstraZeneca, Sputnik V, Sinovac, Janssen y Moderna The most used one has been AstraZeneca for adults |
| Egypt | no | not applicable | Sinopharm was the most commonly used vaccine. |
| Philippines | no | not applicable | Pfizer, moderna, astra zeneca and coronavac in almost equal distribution |
| Pakistan | yes | medical and all other students whose institutions were open in lockdown | Sinopharm and PakVac |
| Vietnam | yes | all students | Astra, Pfizer, Moderna |
| China | no | not applicable | Sinovac |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sitarz, R.; Forma, A.; Karakuła, K.; Juchnowicz, D.; Baj, J.; Bogucki, J.; Rog, J.; Tee, M.L.; Tee, C.A.; Ly-Uson, J.T.; et al. To Vaccinate or Not to Vaccinate—Reasons of Willingness and Reluctance of Students against SARS-CoV-2 Vaccination—An International Experience. Int. J. Environ. Res. Public Health 2022, 19, 14012. https://doi.org/10.3390/ijerph192114012
Sitarz R, Forma A, Karakuła K, Juchnowicz D, Baj J, Bogucki J, Rog J, Tee ML, Tee CA, Ly-Uson JT, et al. To Vaccinate or Not to Vaccinate—Reasons of Willingness and Reluctance of Students against SARS-CoV-2 Vaccination—An International Experience. International Journal of Environmental Research and Public Health. 2022; 19(21):14012. https://doi.org/10.3390/ijerph192114012
Chicago/Turabian StyleSitarz, Ryszard, Alicja Forma, Kaja Karakuła, Dariusz Juchnowicz, Jacek Baj, Jacek Bogucki, Joanna Rog, Michael L. Tee, Cherica A. Tee, Josefina T. Ly-Uson, and et al. 2022. "To Vaccinate or Not to Vaccinate—Reasons of Willingness and Reluctance of Students against SARS-CoV-2 Vaccination—An International Experience" International Journal of Environmental Research and Public Health 19, no. 21: 14012. https://doi.org/10.3390/ijerph192114012