
A Framework for Interfacing and Partnering with Environmental Justice Communities as a Prelude to Human Health and Hazard Identification in the Vulnerable Census Tracts of Columbus, Ohio
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
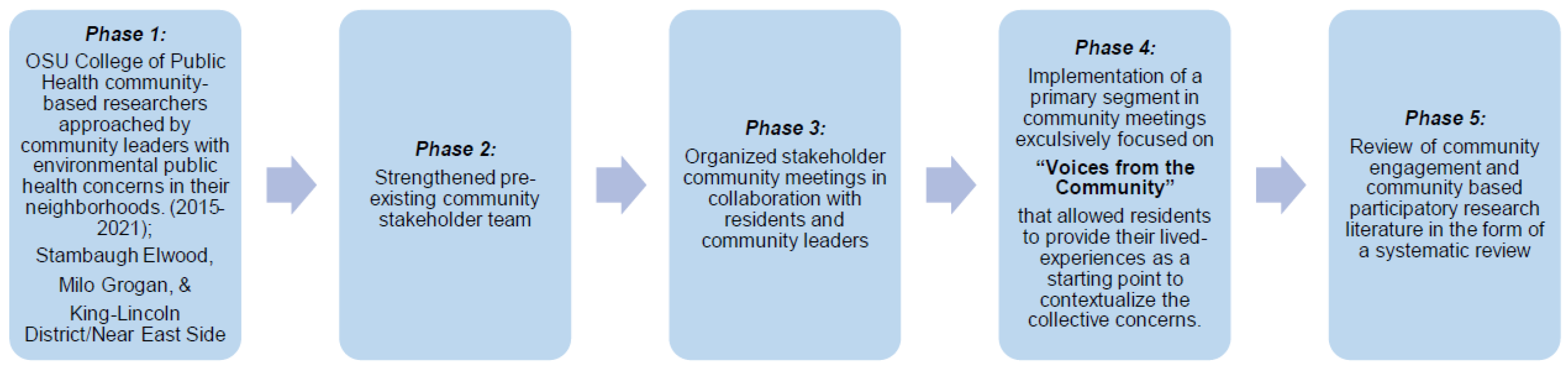
2.1. Phase 1
2.2. Phases 2 and 3
2.3. Phase 4
3. Results and Discussion from Community Meetings
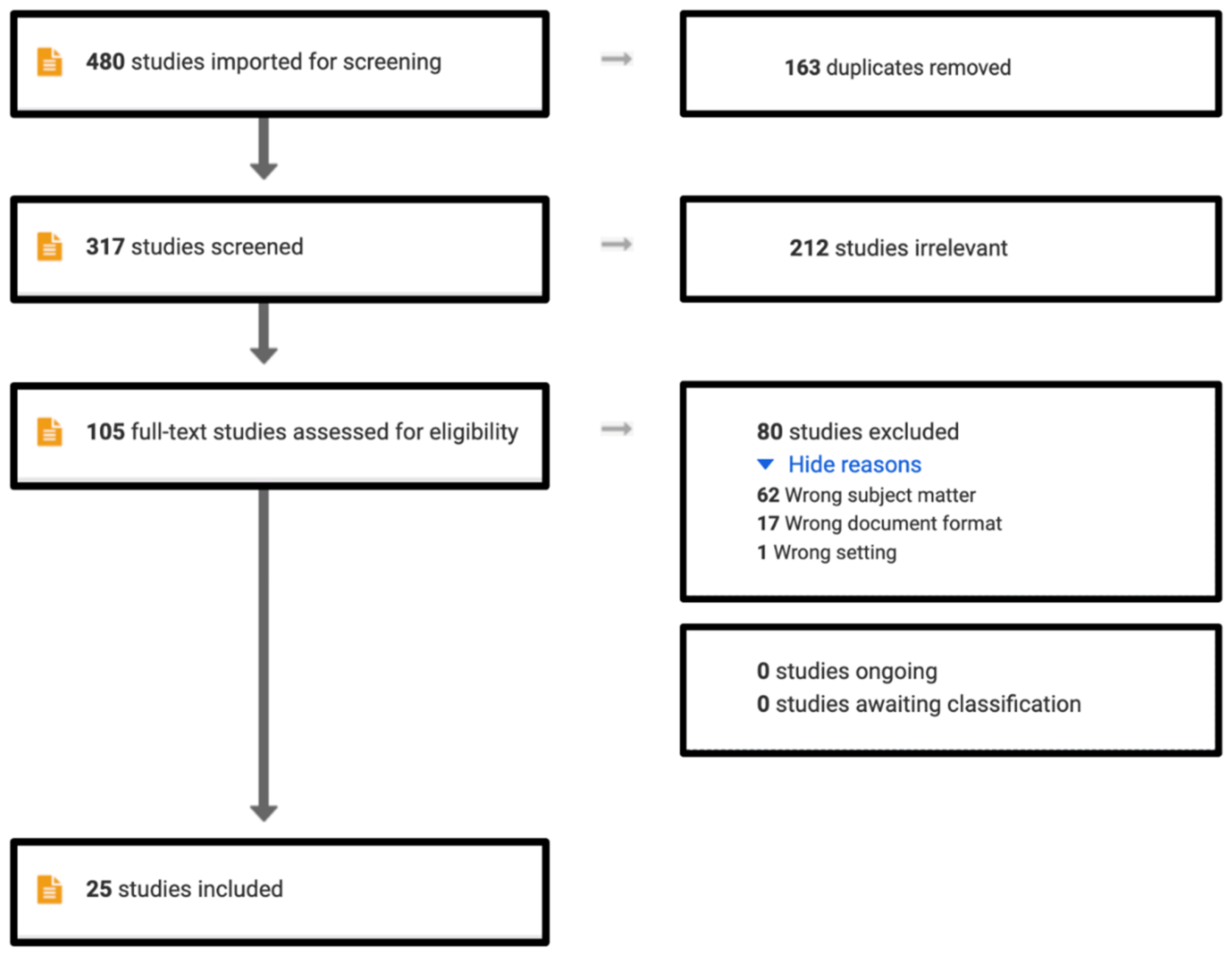
Phase 5
4. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jiao, Y.; Bower, J.K.; Im, W.; Basta, N.; Obrycki, J.; Al-Hamdan, M.Z.; Wilder, A.; Bollinger, C.E.; Zhang, T.; Hatten, L.S.; et al. Application of Citizen Science Risk Communication Tools in a Vulnerable Urban Community. Int. J. Environ. Res. Public Health 2015, 13, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, E.; Gruen, D.; Banerjee, D.; Echeverria, T.; Freelander, L.; Schmeltz, M.; Saganić, E.; Piazza, M.; Galaviz, V.E.; Yost, M.; et al. The Washington State Environmental Health Disparities Map: Development of a Community-Responsive Cumulative Impacts Assessment Tool. Int. J. Environ. Res. Public Health 2019, 16, 4470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jelks, N.O.; Hawthorne, T.L.; Dai, D.; Fuller, C.H.; Stauber, C. Mapping the Hidden Hazards: Community-Led Spatial Data Collection of Street-Level Environmental Stressors in a Degraded, Urban Watershed. Int. J. Environ. Res. Public Health 2018, 15, 825. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, A.; Williams, R.; Barzyk, T.; Greenberg, M.; O’Shea, M.; Sheridan, P.; Hoang, A.; Ash, C.; Teitz, A.; Mustafa, M.; et al. A Citizen Science and Government Collaboration: Developing Tools to Facilitate Community Air Monitoring. Environ. Justice 2017, 10, 51–61. [Google Scholar] [CrossRef] [PubMed]
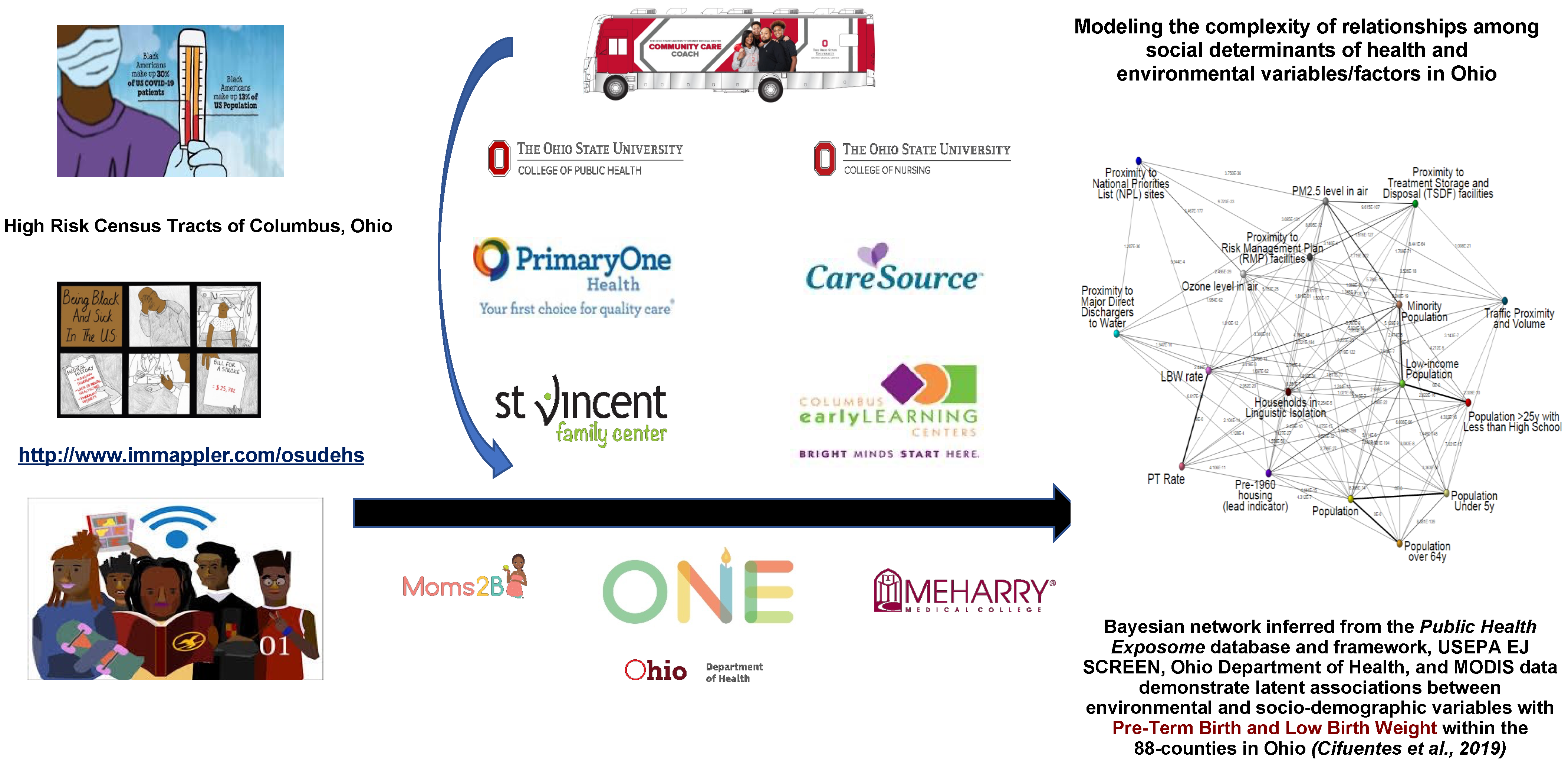
- Cifuentes, P.; Reichard, J.; Im, W.; Smith, S.; Colen, C.; Giurgescu, C.; Williams, K.P.; Gillespie, S.; Juarez, P.D.; Hood, D.B. Application of the Public Health Exposome Framework to Estimate Phenotypes of Resilience in a Model Ohio African-American Women’s Cohort. J. Hered. 2019, 96, 57–71. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine. The Growing Gap in Life Expectancy by Income: Implications for Federal Programs and Policy Responses; The National Academies Press: Washington, DC, USA, 2015. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. COVID-19 and the Present and Future of Black Communities: The Role of Black Physicians, Engineers, and Scientists: Proceedings of a Workshop; The National Academies Press: Washington, DC, USA, 2021. [Google Scholar] [CrossRef]
- Singer, M.; Bulled, N.; Ostrach, B. Whither syndemics?: Trends in syndemics research, a review. 2015–2019. Glob. Public Health 2020, 15, 943–955. [Google Scholar] [CrossRef]
- Poteat, T.; Millett, G.A.; Nelson, L.E.; Beyrer, C. Understanding COVID-19 risks and vulnerabilities among black communities in America: The lethal force of syndemics. Ann. Epidemiol. 2020, 47, 1–3. [Google Scholar] [CrossRef]
- U.S. Census Bureau. American Community Survey 5-Year Estimates Detailed Tables. B02001, Race. 2019. Available online: https://data.census.gov/cedsci/table?q=race&g=860XX00US43205,43219,43203&tid=ACSDT5Y2019.B02001 (accessed on 26 September 2022).
- Laurencin, C.T.; McClinton, A. The COVID-19 Pandemic: A Call to Action to Identify and Address Racial and Ethnic Disparities. J. Racial Ethn. Health Disparities 2020, 7, 398–402. [Google Scholar] [CrossRef] [Green Version]
- Laurencin, C.T.; Walker, J.M. Racial Profiling Is a Public Health and Health Disparities Issue. J. Racial Ethn. Health Disparities 2020, 7, 393–397. [Google Scholar] [CrossRef]
- Duru, O.K.; Harawa, N.T.; Kermah, D.; Norris, K.C. Allostatic Load Burden and Racial Disparities in Mortality. J. Natl. Med. Assoc. 2012, 104, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Borno, H.T.; Zhang, S.; Gomez, S. COVID-19 disparities: An urgent call for race reporting and representation in clinical research. Contemp. Clin. Trials Commun. 2020, 19, 100630. [Google Scholar] [CrossRef] [PubMed]
- Bao, X.; Qu, H.; Zhang, R.; Hogan, T.P. Modeling Reading Ability Gain in Kindergarten Children during COVID-19 School Closures. Int. J. Environ. Res. Public Health 2020, 17, 6371. [Google Scholar] [CrossRef]
- Juarez, P.D.; Matthews-Juarez, P.; Hood, D.B.; Im, W.; Levine, R.S.; Kilbourne, B.J.; Langston, M.A.; Al-Hamdan, M.Z.; Crosson, W.L.; Estes, M.G.; et al. The Public Health Exposome: A Population-Based, Exposure Science Approach to Health Disparities Research. Int. J. Environ. Res. Public Health 2014, 11, 12866–12895. [Google Scholar] [CrossRef] [PubMed]
- Castner, J.; Huntington-Moskos, L.; May, A. Generating Data Visualizations of Longitudinal Cohort Ambient Air Pollution Exposure. CIN Comput. Inform. Nurs. 2021, 40, 44–52. [Google Scholar] [CrossRef]
- Baskin-Graves, L.; Mullen, H.; Aber, A.; Sinisterra, J.; Ayub, K.; Amaya-Fuentes, R.; Wilson, S. Rapid Health Impact Assessment of a Proposed Poultry Processing Plant in Millsboro, Delaware. Int. J. Environ. Res. Public Health 2019, 16, 3429. [Google Scholar] [CrossRef] [Green Version]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B.; Community-Campus Partnerships for Health. Community-based participatory research: Policy recommendations for promoting a partnership approach in health research. Educ. Health 2001, 14, 182–197. [Google Scholar] [CrossRef]
- Wallerstein, N.; Duran, B. Community-Based Participatory Research Contributions to Intervention Research: The Intersection of Science and Practice to Improve Health Equity. Am. J. Public Health 2010, 100, S40–S46. [Google Scholar] [CrossRef]
- Chen, C.-K.; Bruce, M.; Tyler, L.; Brown, C.; Garrett, A.; Goggins, S.; Lewis-Polite, B.; Weriwoh, M.L.; Juarez, P.D.; Hood, D.B.; et al. Analysis of an environmental exposure health questionnaire in a metropolitan minority population utilizing logistic regression and Support Vector Machines. J. Health Care Poor Underserved 2013, 24, 153–171. [Google Scholar] [CrossRef]
- Bullard, R.D.; Mohai, P.; Saha, R.; Wright, B. Toxic Wastes and Race at Twenty: Why Race Still Matters after All of These Years. Environ. Law 2008, 38, 371–411. [Google Scholar]
- Sadd, J.; Morello-Frosch, R.; Pastor, M.; Matsuoka, M.; Prichard, M.; Carter, V. The Truth, the Whole Truth, and Nothing but the Ground-Truth: Methods to Advance Environmental Justice and Researcher-Community Partnerships. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 2014, 41, 281–290. [Google Scholar] [CrossRef]
- Freeman, M.A. The distribution of environmental quality. In Environmental Quality Analysis; Kneese, A.V., Bower, B.T., Eds.; Johns Hopkins University Press for Resources for the Future: Baltimore, MD, USA, 1972. [Google Scholar]
- Gianessi, L.; Peskin, H.M.; Wolff, E. The distributional effects of uniform air pollution policy in the U.S. Q. J. Econ. 1979, 93, 281–301. [Google Scholar] [CrossRef]
- Gelobter, M. The distribution of air pollution by income and race. In Proceedings of the Second Symposium on Social Science in Resource Management, Urbana, IL, USA, 11 May 1988. [Google Scholar]
- Wernette, D.R.; Nieves, L.A. Breathing polluted air. EPA J. 1992, 18, 16–17. [Google Scholar]
- Bullard, R.D. Solid Waste Sites and the Black Houston Community. Sociol. Inq. 1983, 53, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Bullard, R.D. Invisible Houston: The Black Experience in Boom and Bust; Texas A&M University Press: College Station, TX, USA, 1987. [Google Scholar]
- Bullard, R.D. Dumping in Dixie: Race, Class, and Environmental Quality; Westview Press: Boulder, CO, USA, 1990. [Google Scholar]
- Bullard, R.D. Environmental racism. Environ. Prot. 1991, 2, 25–26. [Google Scholar]
- Bullard, R.D.; Wright, B.H. Environmental Justice for all: Community Perspectives on Health and Research. Toxicol. Ind. Health 1993, 9, 821–841. [Google Scholar] [CrossRef]
- Lu, T.; Liu, Y.; Garcia, A.; Wang, M.; Li, Y.; Bravo-Villasenor, G.; Campos, K.; Xu, J.; Han, B. Leveraging Citizen Science and Low-Cost Sensors to Characterize Air Pollution Exposure of Disadvantaged Communities in Southern California. Int. J. Environ. Res. Public Health 2022, 19, 8777. [Google Scholar] [CrossRef]
- Williams-Livingston, A.; Akintobi, T.H.; Banerjee, A. Community-Based Participatory Research in Action: The Patient-Centered Medical Home and Neighborhood. J. Prim. Care Community Health 2020, 11, 2150132720968456. [Google Scholar] [CrossRef]
- Mude, W.; Oguoma, V.M.; Nyanhanda, T.; Mwanri, L.; Njue, C. Racial disparities in COVID-19 pandemic cases, hospitalisations, and deaths: A systematic review and meta-analysis. J. Glob. Health 2021, 11, 05015. [Google Scholar] [CrossRef]
- Carrera, J.S.; Key, K.; Bailey, S.; Hamm, J.A.; Cuthbertson, C.A.; Lewis, E.Y.; Woolford, S.J.; DeLoney, E.H.; Greene-Moton, E.; Wallace, K.; et al. Community Science as a Pathway for Resilience in Response to a Public Health Crisis in Flint, Michigan. Soc. Sci. 2019, 8, 94. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, T.B.; Coombe, C.M.; Rowe, Z.E.; Clark, S.J.; Gronlund, C.J.; Lee, M.; Palacios, A.; Larsen, L.S.; Reames, T.G.; Schott, J.; et al. Shifting from “Community-Placed” to “Community-Based” Research to Advance Health Equity: A Case Study of the Heatwaves, Housing, and Health: Increasing Climate Resiliency in Detroit (HHH) Partnership. Int. J. Environ. Res. Public Health 2019, 16, 3310. [Google Scholar] [CrossRef] [Green Version]
- Ziegahn, L.; Joosten, Y.; Nevarez, L.; Hurd, T.; Evans, J.; Dumbauld, J.; Eder, M. Collaboration and Context in the Design of Community-Engaged Research Training. Health Promot. PR 2020, 22, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Shaw-Ridley, M.; Ridley, C.R. The Health Disparities Industry: Is It an Ethical Conundrum? Health Promot. PR 2010, 11, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Boursaw, B.; Oetzel, J.G.; Dickson, E.; Thein, T.S.; Sanchez-Youngman, S.; Peña, J.; Parker, M.; Magarati, M.; Littledeer, L.; Duran, B.; et al. Scales of Practices and Outcomes for Community-Engaged Research. Am. J. Community Psychol. 2021, 67, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.C.; Sorensen, A.E.; Biehler, D.; Wilson, S.; LaDeau, S. Citizen science and civic ecology: Merging paths to stewardship. J. Environ. Stud. Sci. 2018, 9, 133–143. [Google Scholar] [CrossRef]
- Payne-Sturges, D.C.; Schwab, M.; Buckley, T.J. Closing the research loop: A risk-based approach for communicating results of air pollution exposure studies. Environ. Health Perspect. 2004, 112, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Abara, W.; Wilson, S.; Vena, J.; Sanders, L.; Bevington, T.; Culley, J.M.; Annang, L.; Dalemarre, L.; Svendsen, E. Engaging a Chemical Disaster Community: Lessons from Graniteville. Int. J. Environ. Res. Public Health 2014, 11, 5684–5697. [Google Scholar] [CrossRef] [Green Version]
- Wilson, S.M.; Murray, R.T.; Jiang, C.; Dalemarre, L.; Burwell-Naney, K.; Fraser-Rahim, H. Environmental Justice Radar: A Tool for Community-Based Mapping to Increase Environmental Awareness and Participatory Decision Making. Prog. Community Health Partnersh. Res. Educ. Action 2015, 9, 439–446. [Google Scholar] [CrossRef]
- Sangaramoorthy, T.; Jamison, A.M.; Boyle, M.D.; Payne-Sturges, D.C.; Sapkota, A.; Milton, D.K.; Wilson, S.M. Place-based perceptions of the impacts of fracking along the Marcellus Shale. Soc. Sci. Med. 2016, 151, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Heaney, C.D.; Wing, S.; Wilson, S.M.; Campbell, R.L.; Caldwell, D.; Hopkins, B.; O’Shea, S.; Yeatts, K. Public infrastructure disparities and the microbiological and chemical safety of drinking and surface water supplies in a community bordering a landfill. J. Environ. Health 2013, 75, 24–36. [Google Scholar]
- Patra, D.; Chanse, V.; Rockler, A.; Wilson, S.; Montas, H.; Shirmohammadi, A.; Leisnham, P.T. Towards attaining green sustainability goals of cities through social transitions: Comparing stakeholders’ knowledge and perceptions between two Chesapeake Bay watersheds, USA. Sustain. Cities Soc. 2021, 75, 103318. [Google Scholar] [CrossRef]
- Ilie, A.M.C.; McCarthy, N.; Velasquez, L.; Moitra, M.; Eisl, H.M. Air pollution exposure assessment at schools and playgrounds in Williamsburg Brooklyn NYC, with a view to developing a set of policy solutions. J. Environ. Stud. Sci. 2022, 12, 838–852. [Google Scholar] [CrossRef] [PubMed]
- Environmental Defense. Scorecard. 2001. Available online: http://www.scorecard.org (accessed on 30 November 2020).
- Mayer, A.L.; Shuster, W.D.; Beaulieu, J.J.; Hopton, M.E.; Rhea, L.K.; Roy, A.H.; Thurston, H.W. Environmental Reviews and Case Studies: Building Green Infrastructure via Citizen Participation: A Six-Year Study in the Shepherd Creek (Ohio). Environ. PR 2012, 14, 57–67. [Google Scholar] [CrossRef]
- Dernoga, M.A.; Wilson, S.; Jiang, C.; Tutman, F. Environmental justice disparities in Maryland’s watershed restoration programs. Environ. Sci. Policy 2015, 45, 67–78. [Google Scholar] [CrossRef]
- Reckhow, K.H.; Norris, P.E.; Budell, R.J.; DI Toro, D.M.; Galloway, J.N.; Greening, H.; Sharply, A.N.; Shirmohammadi, A.; Stacey, P.E.; Johnson, S.E.; et al. Achieving Nutrient and Sediment Reduction Goals in the Chesapeake Bay: An Evaluation of Program Strategies and Implementation; National Research Council (NRC) of National Academies, The National Academies Press: Washington, DC, USA, 2011; p. 246. [Google Scholar]
- Chesapeake EcoCheck. 2013. Available online: http://ian.umces.edu/ecocheck/reportcards/chesapeakebay/2013/ (accessed on 5 January 2020).
- Fisher, S.L.; Smith, B.E. Transforming Places: Lessons from Appalachia; University of Illinois Press: Urbana, IL, USA, 2012. [Google Scholar]
- Taylor, B. “Place” as Prepolitical Grounds of Democracy. Am. Behav. Sci. 2009, 52, 826–845. [Google Scholar] [CrossRef]
- Collier-Oxandale, A.; Papapostolou, V.; Feenstra, B.; Der Boghossian, B.; Polidori, A. Towards the Development of a Sensor Educational Toolkit to Support Community and Citizen Science. Sensors 2022, 22, 2543. [Google Scholar] [CrossRef]
- Pace, C.; Fencl, A.; Baehner, L.; Lukacs, H.; Cushing, L.J.; Morello-Frosch, R. The Drinking Water Tool: A Community-Driven Data Visualization Tool for Policy Implementation. Int. J. Environ. Res. Public Health 2022, 19, 1419. [Google Scholar] [CrossRef]
- Fawkes, L.S.; McDonald, T.J.; Roh, T.; Chiu, W.A.; Taylor, R.J.; Sansom, G.T. A Participatory-Based Research Approach for Assessing Exposure to Lead-Contaminated Drinking Water in the Houston Neighborhood of the Greater Fifth Ward. Int. J. Environ. Res. Public Health 2022, 19, 8135. [Google Scholar] [CrossRef]
- De Marco, M.; Kearney, W.; Smith, T.; Jones, C.; Kearney-Powell, A.; Ammerman, A. Growing Partners: Building a Community–Academic Partnership to Address Health Disparities in Rural North Carolina. Prog. Community Health Partnersh. Res. Educ. Action 2014, 8, 181–186. [Google Scholar] [CrossRef]
- Moore, T.; Payne-Foster, P.; Oliver, J.S.; Spears, E.G.; Spencer, C.H.; Maye, J.; Allen, R.S. Community Perspectives and Environmental Justice Issues in an Unincorporated Black Township. Int. J. Environ. Res. Public Health 2022, 19, 7490. [Google Scholar] [CrossRef]
- Jelks, N.O.; Smith-Perry, D.J.; Fuller, C.H.; Stauber, C. Participatory research in Northwest Atlanta’s Proctor Creek Watershed: Using photovoice to explore environmental health risks at the water’s edge. Health Place 2020, 66, 102444. [Google Scholar] [CrossRef]
- Ou, J.Y.; Peters, J.L.; Levy, J.I.; Bongiovanni, R.; Rossini, A.; Scammell, M.K. Self-rated health and its association with perceived environmental hazards, the social environment, and cultural stressors in an environmental justice population. BMC Public Health 2018, 18, 970. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Lopez, A.; Malloy, N.; Morello-Frosch, R. Our Environment, Our Health. Health Educ. Behav. 2011, 39, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Cantu, A.G.; Graham, M.A.; Millard, A.V.; Flores, I.; Mugleston, M.K.; Reyes, I.Y.; Carbajal, E.S. Environmental Justice and Community-Based Research in Texas Borderland Colonias. Public Health Nurs. 2015, 33, 65–72. [Google Scholar] [CrossRef] [Green Version]
- King, A.; Odunitan-Wayas, F.; Chaudhury, M.; Rubio, M.; Baiocchi, M.; Kolbe-Alexander, T.; Montes, F.; Banchoff, A.; Sarmiento, O.; Bälter, K.; et al. Community-Based Approaches to Reducing Health Inequities and Fostering Environmental Justice through Global Youth-Engaged Citizen Science. Int. J. Environ. Res. Public Health 2021, 18, 892. [Google Scholar] [CrossRef] [PubMed]
- Spencer-Hwang, R.; Soret, S.; Valladares, J.; Torres, X.; Pasco-Rubio, M.; Dougherty, M.; Kim, W.; Montgomery, S. Strategic Partnerships for Change in an Environmental Justice Community: The ENRRICH Study. Prog. Community Health Partnersh. Res. Educ. Action 2016, 10, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Mansyur, C.L.; Jeng, H.A.; Holloman, E.; DeBrew, L. Using Community-Based Participatory Research to Identify Environmental Justice Issues in an Inner-City Community and Inform Urban Planning. Fam. Community Health 2016, 39, 169–177. [Google Scholar] [CrossRef]
- Symanski, E.; Han, H.A.; Hopkins, L.; Smith, M.A.; McCurdy, S.; Han, I.; Jimenez, M.; Markham, C.; Richner, D.; James, D.; et al. Metal air pollution partnership solutions: Building an academic-government-community-industry collaboration to improve air quality and health in environmental justice communities in Houston. Environ. Health 2020, 19, 39. [Google Scholar] [CrossRef] [Green Version]
- Haynes, E.N.; Sucharew, H.; Hilbert, T.J.; Kuhnell, P.; Spencer, A.; Newman, N.C.; Burns, R.; Wright, R.; Parsons, P.J.; Dietrich, K.N. Impact of air manganese on child neurodevelopment in East Liverpool, Ohio. NeuroToxicology 2017, 64, 94–102. [Google Scholar] [CrossRef]
- Clark, R.S.; Pellom, S.T.; Booker, B.; Ramesh, A.; Zhang, T.; Shanker, A.; Maguire, M.; Juarez, P.D.; Patricia, M.-J.; Langston, M.A.; et al. Validation of research trajectory 1 of an Exposome framework: Exposure to benzo(a)pyrene confers enhanced susceptibility to bacterial infection. Environ. Res. 2016, 146, 173–184. [Google Scholar] [CrossRef] [Green Version]
- Fox, E.R.; Samdarshi, T.E.; Musani, S.K.; Pencina, M.J.; Sung, J.H.; Bertoni, A.; Xanthakis, V.; Balfour, P.C.; Shreenivas, S.S.; Covington, C.; et al. Development and Validation of Risk Prediction Models for Cardiovascular Events in Black Adults. JAMA Cardiol. 2016, 1, 15–25. [Google Scholar] [CrossRef] [Green Version]
- Bethea, T.N.; Palmer, J.R.; Rosenberg, L.; Cozier, Y.C. Neighborhood Socioeconomic Status in Relation to All-cause, Cancer, and Cardiovascular Mortality in the Black Women’s Health Study. Ethn. Dis. 2016, 26, 157–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knapp, R.G.; Sutherland, S.E.; Keil, J.E.; Rust, P.F.; Lackland, D.T. A comparison of the effects of cholesterol on CHD mortality in black and white women: Twenty-eight years of follow-up in the Charleston heart study. J. Clin. Epidemiol. 1992, 45, 1119–1129. [Google Scholar] [CrossRef]
- Peters, A.; McEwen, B.S. Stress habituation, body shape and cardiovascular mortality. Neurosci. Biobehav. Rev. 2015, 56, 139–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogojiaku, C.N.; Allen, J.C.; Anson-Dwamena, R.; Barnett, K.S.; Adetona, O.; Im, W.; Hood, D.B. The Health Opportunity Index: Understanding the Input to Disparate Health Outcomes in Vulnerable and High-Risk Census Tracts. Int. J. Environ. Res. Public Health 2020, 17, 5767. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, R.B.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General Cardiovascular Risk Profile for Use in Primary Care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacco, R.L.; Khatri, M.; Rundek, T.; Xu, Q.; Gardener, H.; Boden-Albala, B.; Di Tullio, M.R.; Homma, S.; Elkind, M.S.; Paik, M.C. Improving Global Vascular Risk Prediction with Behavioral and Anthropometric Factors: The Multiethnic NOMAS (Northern Manhattan Cohort Study). J. Am. Coll. Cardiol. 2009, 54, 2303–2311. [Google Scholar] [CrossRef] [Green Version]
- Vos, T.A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Criqui, M.H. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef] [Green Version]
- Sexton, K.; Linder, S.H. The Role of Cumulative Risk Assessment in Decisions about Environmental Justice. Int. J. Environ. Res. Public Health 2010, 7, 4037–4049. [Google Scholar] [CrossRef]
- Horowitz, C.R.; Shameer, K.; Gabrilove, J.; Atreja, A.; Shepard, P.; Goytia, C.N.; Smith, G.W.; Dudley, J.; Manning, R.; Bickell, N.A.; et al. Accelerators: Sparking Innovation and Transdisciplinary Team Science in Disparities Research. Int. J. Environ. Res. Public Health 2017, 14, 225. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measure | 43203 | 43205 | Franklin County | Columbus | Ohio |
|---|---|---|---|---|---|
| Population | 8108 1 | 12,272 1 | 1,163,481 1 | 787,324 1 | 11,536,503 1 |
| 8415 ± 1006 3 | 12,590 ± 1054 3 | 1,323,807 2 | 905,748 2 | 11,799,448 2 | |
| Percent African American | 62 ± 10 3 | 49.5 ± 7 3 | 21.2 1 | 27.9 1 | 12.2 1 |
| 22.5 2 | 28.6 2 | 12.5 2 | |||
| Percent White | 29.9 ± 7 3 | 41.1 ± 6 3 | 69.2 1 | 61.5 1 | 82.7 1 |
| 60.6 2 | 53.2 2 | 77 2 | |||
| Educational Attainment for Population 25+ (Percent) | |||||
| Less than high school | 11.5 ± 3.1 3 | 12.5 ± 2.8 3 | 8.2 ± 0.7 3 | 9.2 ± 0.9 3 | 8.3 ± 0.2 3 |
| High school + | 88.5 ± 3.1 3 | 87.5 ± 2.8 3 | 91.8 ± 0.7 3 | 90.8 ± 0.9 3 | 91.7 ± 0.2 3 |
| Bachelor’s degree + | 23 ± 4.9 3 | 32.3 ± 4.7 3 | 41.8 ± 1.2 3 | 38.4 ± 1.6 3 | 30.7 ± 0.3 3 |
| Graduate/professional degree + | 8.9 ± 4.2 3 | 11.5 ± 2.9 3 | 16.1 ± 0.8 3 | 13.4 ± 0.9 3 | 11.8 ± 0.2 3 |
| Employment, Income, Poverty, Healthcare Coverage | |||||
| Percent of unemployed among individuals > 16 years in civilian labor force | 13.8 ± 5.6 3 | 8.6 ± 2.3 3 | 4.8 ± 0.2 3 | 5.4 ± 0.3 3 | 5.3 ± 0.1 3 |
| Median Household income (in 2020 U.S. dollars) | 36,418 ± 5440 3 | 40,559 ± 3617 3 | 62,352 ± 706 3 | 54,902 ± 835 3 | 58,116 ± 228 3 |
| Percent of families below the poverty level (for which poverty is determined) | 35.9 ± 6.9 3 | 31.2 ± 5.4 3 | 15.1 ± 0.4 3 | 19.1 ± 0.6 3 | 13.6 ± 0.2 3 |
| Percent of insured to health care (civilian non-institutionalized population) | 91.8 ± 2.4 3 | 91 ± 2.3 3 | 92.3 ± 0.3 3 | 90.8 ± 0.4 3 | 93.8 ± 0.1 3 |
| Chronic Health Outcomes (crude prevalence) | |||||
| Prevalence of diabetes | 20% (19.4,20.5) 4 | 17% (16.5, 17.5) 4 | 10.7 (10.1, 11.4) 4 | 12.4 (8.0–16.9) 4 | 11.8 (11.0, 12.7) 4 |
| Prevalence of obesity | 48.5% (47.9, 49.2) 4 | 45.9% (45.3, 46.5) 4 | 35.6 (34.4, 36.7) 4 | 37.6 (36.5, 36.8) 4 | 37.6 (36.0, 39.1) 4 |
| Prevalence of current asthma (adults) | 13.4% (12.9, 13.8) 4 | 12.2% (11.9, 12.5) 4 | 10 (9.5–10.5) 4 | 10.8 (10.7, 10.8) 4 | 10.3 (9.7, 11.0) 4 |
| Prevalence of Smoking | 28.8% (27.1, 30.6) 4 | 26.7% (25.2, 28.3) 4 | 20.5 (17.5, 23.5) 4 | 22.8 (22.6, 23.0) 4 | 23.3 (20.0, 26.4) 4 |
| Prevalence of Depression | 19.9% (19.3, 20.4) 4 | 19.7% (19.4, 20.2) 4 | 20.7 (19.6, 21.7) 4 | 21.9 (21.8, 22.0) 4 | 22.5 (21.2, 23.8) 4 |
| Adverse Pregnancy Outcomes | |||||
| Total Number of Births | 824 5 | 902 5 | 38,053 6 | 48,086 5 | 674,202 7 |
| Percent Low Birth Weight | 15.7 5 | 14.5 5 | 9.0 6 | 10.5 5 | 8.6 7 |
| Percent of Preterm Births | 14.8 5 | 15.0 5 | 10.5 6 | 11.6 5 | 10.4 7 |
| Percent of Teenage Mothers | 9.6 5 | 7.9 5 | 1.5 6 | 6.2 5 | 5.4 7 |
| Infant Mortality Rate (2010–2014) | 13.3 5 | 10.0 5 | 8.4 5 | 9.3 5 | 7.5 7 |
| Leading Causes of Death (cases; ADR (95% CI)) | |||||
| Heart Disease | 61; 270.9 8 | 95; 325.0 8 | 176; 205.28 8 | 2060; 165.6 9 | 29,159; 188.8 9 |
| Cancer | 47; 195.8 8 | 67; 226.8 8 | 172; 205.6 8 | 1934; 149.7 9 | 25,166; 163.0 9 |
| Stroke | 18; 79.2 8 | 17; 69.8 8 | 51; 56.9 8 | 515; 43.1 9 | 6504; 42.1 9 |
| Chronic Lower Respiratory Disease | ** | 15; 48.3 8 | 41; 48.7 8 | 559; 44.8 9 | 7168; 45.9 9 |
| Diabetes | 13; 96.5 8 | 18; 58.9 8 | 32; 38.0 8 | 305; 23.8 9 | 3876; 25.4 9 |
| Accident/Unintentional Injury | 18; 81.5 8 | 35; 92.3 8 | 54; 61.7 8 | 918; 70.1 9 | 8.291; 67.7 9 |
| Homicide | ** | 12; 27.3 8 | 19; 21.3 8 | 115; 8.5 9 | 726; 6.6 9 |
| Suicide | ** | ** | 14; 16.1 8 | 153; 11.4 9 | 1809; 15.2 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lochotzki, H.; Williams, K.P.; Colen, C.G.; Adetona, O.; Tavares, C.B.; Ginn, G.M.; Haynes, R.; Im, W.; Bils, T.; Hood, D.B. A Framework for Interfacing and Partnering with Environmental Justice Communities as a Prelude to Human Health and Hazard Identification in the Vulnerable Census Tracts of Columbus, Ohio. Int. J. Environ. Res. Public Health 2022, 19, 13846. https://doi.org/10.3390/ijerph192113846
Lochotzki H, Williams KP, Colen CG, Adetona O, Tavares CB, Ginn GM, Haynes R, Im W, Bils T, Hood DB. A Framework for Interfacing and Partnering with Environmental Justice Communities as a Prelude to Human Health and Hazard Identification in the Vulnerable Census Tracts of Columbus, Ohio. International Journal of Environmental Research and Public Health. 2022; 19(21):13846. https://doi.org/10.3390/ijerph192113846
Chicago/Turabian StyleLochotzki, Heather, Karen Patricia Williams, Cynthia G. Colen, Olorunfemi Adetona, Charleta B. Tavares, Georgina M. Ginn, Rejeana Haynes, Wansoo Im, Tanya Bils, and Darryl B. Hood. 2022. "A Framework for Interfacing and Partnering with Environmental Justice Communities as a Prelude to Human Health and Hazard Identification in the Vulnerable Census Tracts of Columbus, Ohio" International Journal of Environmental Research and Public Health 19, no. 21: 13846. https://doi.org/10.3390/ijerph192113846