

Development and Preliminary Evaluation of the Effects of a Preceptor Reflective Practice Program: A Mixed-Method Research


Abstract
:1. Introduction
2. Materials and Methods
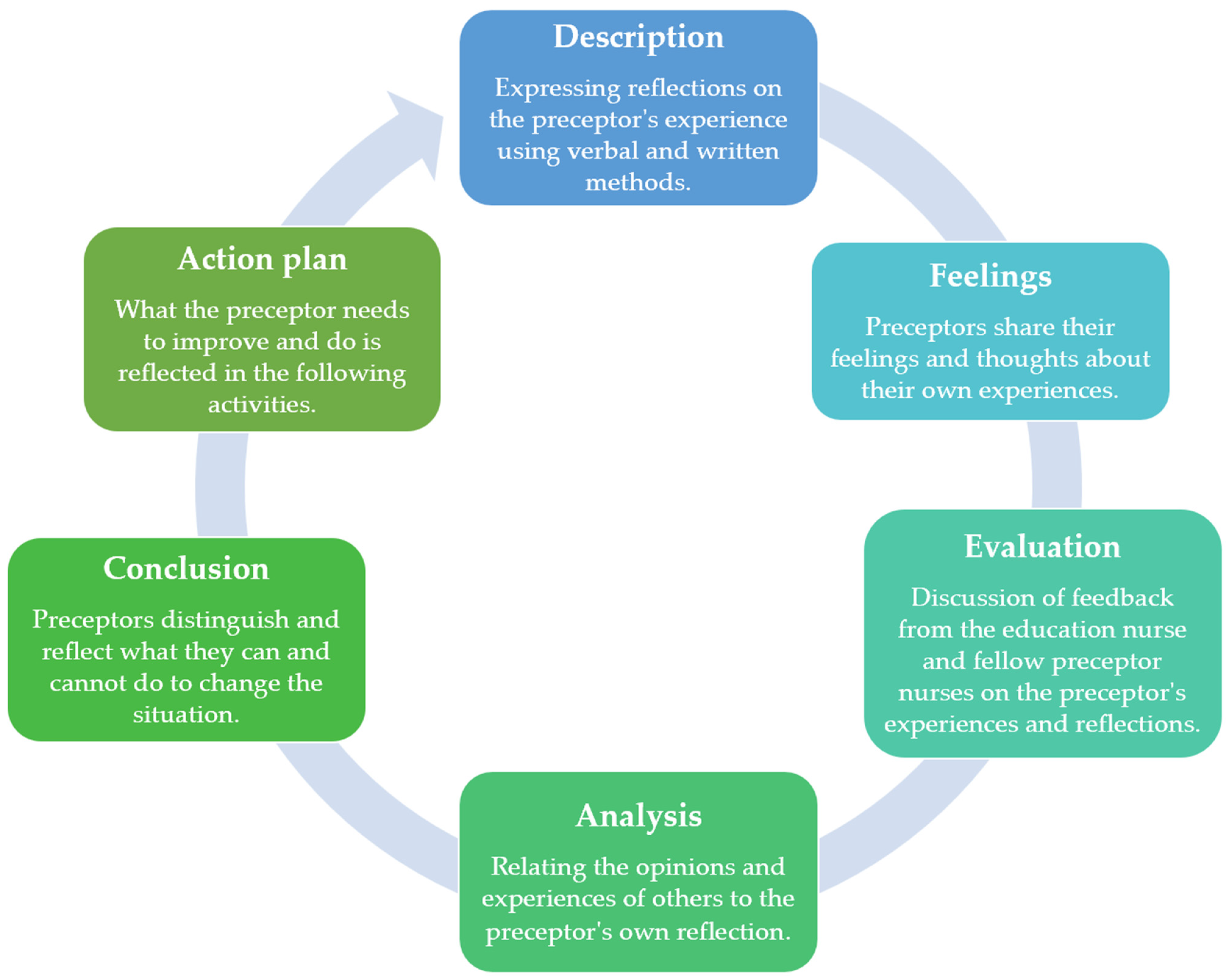
2.1. Theoretical Framework
2.2. Study Design
2.3. Participants
2.4. Research Procedure
2.4.1. Development of the PRPP
2.4.2. Application of the PRPP
2.4.3. Ethical Consideration
2.5. Data Collection and Analysis
2.5.1. Data Collection
2.5.2. Data Analysis
2.6. Rigor
3. Results
3.1. General Characteristics of the Participants
3.2. Preliminary Effects of the Preceptor Reflective Practice Program
3.3. Content Analysis of Self-Reflective Journals
3.3.1. Theme 1. Disappointing Preceptor Education Support System
- (1)
- Insufficient educational support system
“It is very hard for one preceptor to train two new nurses. It was necessary to check whether each individual understood the contents of the training, and it was too difficult to explain several times because each new nurse had a different acquisition rate”.(Participant 3, Participant 12, Participant 14, Participant 19, Participant 32)
“The greatest difficulty in training two new nurses is that one of them follows, but the other one often does not know about it, and it was difficult to train because of the different degrees of activeness. When I saw a new nurse who could not follow, I was very stressed because I was compared to a new nurse who was good at it”.(Participant 20, Participant 37)
“As I teach two new nurses at once, I think that the new nurse’s growth rate seems to be slow as the new nurses have to divide the work they have to do alone”.(Participant 9)
“New nurses need to learn several things, but it feels increasingly burdensome because two people cannot be trained simultaneously”.(Participant 12)
- (2)
- Parallel work and education
“I know that it is inevitable owing to the coronavirus disease 2019 (COVID-19) pandemic, but there are no training days for new nurse training; therefore, I had to train new nurses while caring for patients, and so it was very burdensome and daunting”.(Participant 5, Participant 7, Participant 11, Participant 20, Participant 21, Participant 32, Participant 42, Participant 46)
“There are too many things to teach new nurses, but the situation is not supported. Hence, I feel frustrated, impatient, and anxious”.(Participant 9, Participant 19, Participant 35, Participant 42)
“As I was teaching new nurses while also caring for patients, the flow of education was interrupted, and there were many days when I only gave half of the information and could not tell the whole thing. Thus, I think it was really stressful at work”.(Participant 5, Participant 13, Participant 20)
3.3.2. Theme 2. Complex Emotional Expression of the Preceptor Role
- (1)
- Excitement regarding the first-time preceptor role
“Being a preceptor for the first time, I am nervous and excited, and I want to gather the strengths of good preceptors and teach them as best as I can”.(Participant 19, Participant 40, Participant 46)
“Having been a new nurse at one time in the past, I know that a new nurse really wants to meet a preceptor, so I also want to study and prepare hard to teach”.(Participant 19, Participant 46, Participant 50)
“I want to be a preceptor who can kindly and generously answer and educate new nurses when they ask a question and approach them like a friend”.(Participant 46, Participant 49, Participant 50)
- (2)
- The burden of the preceptor role
“As my career progressed, the burden of becoming a preceptor increased, and I received a notice from the team leader to become a preceptor. I am scared and worried about whether I will do well”.(Participant 17, Participant 18, Participant 20, Participant 22, Participant 24, Participant 32, Participant 41, Participant 42)
“When new nurses do not work well in the department, I think that new nurses do not adapt well because I teach incorrectly, and it is difficult and burdensome to train new nurses”.(Participant 4, Participant 14, Participant 28)
“There are many things I do not know yet, but the burden and pressure to train new nurses was too great”.(Participant 8, Participant 29, Participant 32, Participant 46)
- (3)
- Pressure because of the limited time
“I have not much to tell new nurses, but time flies so fast that I still have a lot to tell them, but I am worried whether I can tell them all before they become independent”.(Participant 2, Participant 3, Participant 10, Participant 13, Participant 28, Participant 33)
“There are many things I want to tell new nurses, but as independence approached, I felt impatient as if I were about to become independent, so I scolded and rushed the new nurses”.(Participant 13, Participant 14, Participant 18, Participant 28, Participant 29)
“When new nurses become independent, they will have to deal with the work alone and should be of some help to the ward, but they are still clumsy in their work, so I feel heavy and worried ahead”.(Participant 7, Participant 14, Participant 18, Participant 19, Participant 20, Participant 24)
“I feel bittersweet because I have become attached to new nurses”.(Participant 10, Participant 19, Participant 20, Participant 32, Participant 33, Participant 42)
3.3.3. Theme 3. Self-Growth through the Preceptor Role
- (1)
- Feeling a lack of competence as a preceptor
“There were many days when I felt that I needed to study more because I was afraid that I would give wrong information while training new nurses, and I felt a lot of things and reflected on myself watching new nurses learning while following me”.(Participant 7, Participant 10, Participant 13, Participant 40)
“Even though I made a plan to teach new nurses, I was upset because it did not go as expected owing to the nature of the ward”.(Participant 3, Participant 29, Participant 43)
“I am so sorry and reflect on myself because I am not good enough to wait for new nurses, and I am just scolding them and not giving them a good education”.(Participant 14, Participant 24, Participant 40, Participant 43)
- (2)
- Commitment as a preceptor
“Although the new nurses are still clumsy and slow, I should support and encourage them so that they may adapt well to the ward and grow well after becoming independent”.(Participant 8, Participant 9, Participant 16, Participant 17, Participant 18, Participant 19)
“When I was a new nurse, I was full of things I did not know, but I should remember that time and teach new nurses”.(Participant 2, Participant 7, Participant 12, Participant 20, Participant 24, Participant 26, Participant 39)
- (3)
- Personal growth as a preceptor
“It is meaningful that I am having a new experience as a preceptor, and I hope that new nurses will grow well”.(Participant 3)
“In order to teach new nurses, it was an opportunity to redefine the knowledge I had learnt and known, and it was an opportunity for growth”.(Participant 5, Participant 8, Participant 13, Participant 18, Participant 39)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kang, Y.A.; Seol, M.; Yi, M. Focus group study on hospital nurses’ lived experience of being a Preceptor. Perspect. Nurs. Sci. 2013, 10, 77–86. [Google Scholar]
- Hong, K.J.; Yoon, H.-J. Effect of nurses’ preceptorship experience in educating new graduate nurses and preceptor training courses on clinical teaching behavior. Int. J. Environ. Res. Public Health 2021, 18, 975. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.M.; Eun, Y. The effects of self-efficacy, critical thinking disposition, self-leadership, and communication competency on the core competencies of the preceptor in advanced general hospitals. J. Korean Acad. Soc. Nurs. Educ. 2018, 24, 279–289. [Google Scholar] [CrossRef] [Green Version]
- Jung, M.S.; Kim, E.K.; Kim, S.Y.; Kim, J.K.; You, S.J. Validity and reliability of the clinical teaching behavior inventory (CTBI) for nurse preceptors in Korea. J. Korean Acad. Nurs. 2019, 49, 526–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.; Choi, E. Effect of preceptors’ teaching behavior on new graduate nurses’ intention to stay: The mediating effect of resilience and organizational socialization. J. Korean Acad. Nurs. Adm. 2022, 28, 57–66. [Google Scholar] [CrossRef]
- Shin, S.; Park, Y.W.; Kim, M.; Kim, J.; Lee, I. Survey on the education system for new graduate nurses in hospitals: Focusing on the preceptorship. Korean Med. Educ. Rev. 2019, 21, 112–122. [Google Scholar] [CrossRef]
- McKinney, S.; Aguilar, M. Implementing a comprehensive preceptor development program through professional governance. J. Nurses Prof. Dev. 2020, 36, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, B. Types of role perception of preceptors for new nurses: A Q methodology approach. J. Korean Acad. Nurs. Adm. 2021, 27, 204–214. [Google Scholar] [CrossRef]
- Jeong, H.W.; Ju, D.; Choi, M.L.; Kim, S. Development and evaluation of a preceptor education program based on the one-minute preceptor model: Participatory action research. Int. J. Environ. Res. Public Health 2021, 18, 11376. [Google Scholar] [CrossRef]
- Jeoung, Y.O.; Park, S.C.; Jin, J.K.; Kim, J.Y.; Lee, J.U.; Park, S.Y.; Sok, S. Content analysis of communication between nurses during preceptorship. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2014, 23, 82–92. [Google Scholar] [CrossRef] [Green Version]
- Han, J.; Yoo, E.K. The study of preceptor nurses’ occupational stress and burden. STRESS 2018, 26, 38–45. [Google Scholar] [CrossRef]
- Han, J.W.; Lee, B. The relationship of post-traumatic stress, job stress and turnover intention in emergency department nurses. J. Korean Acad. Nurs. Adm. 2013, 19, 340–350. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.H. A study on job stress, stress coping and self-efficacy according to DISC behavior types of nurses. J. Korean Assn. Learner Cent. Curric. Instr. 2022, 22, 427–442. [Google Scholar] [CrossRef]
- Park, M.S.; An, H.K. Resilience as a mediator in the relationship between stress coping style and burnout in long-term care hospital nurses. JKDAS 2019, 21, 513–529. [Google Scholar] [CrossRef]
- Salovey, P.; Mayer, J.D. Emotional intelligence. Imagin. Cogn. Pers. 1990, 9, 185–211. [Google Scholar] [CrossRef]
- Tak, J.K. Differences in both emotional intelligence and the relations of emotional intelligence to job stress and stress coping based on sex and job position. Korean J. Health Psychol. 2007, 12, 307–324. [Google Scholar] [CrossRef]
- Wong, C.S.; Law, K.S. The effects of leader and follower emotional intelligence on performance and attitude: An exploratory study. In Leadership Perspectives; Routledge: London, UK, 2017; pp. 97–128. [Google Scholar]
- Schon, D.A. Educating the reflective practitioner: Toward a new design for teaching and learning in the professions. Aust. J. Adult Learn. 2010, 50, 448–451. [Google Scholar]
- Choperena, A.; Oroviogoicoechea, C.; Zaragoza Salcedo, A.; Olza Moreno, I.; Jones, D. Nursing narratives and reflective practice: A theoretical review. J. Adv. Nurs. 2019, 75, 1637–1647. [Google Scholar] [CrossRef]
- Lee, M.; Jang, K.S. Reflection-related research in Korean nursing: A literature review. J. Korean Acad. Nurs. Adm. 2019, 25, 83–96. [Google Scholar] [CrossRef] [Green Version]
- Dubé, V.; Ducharme, F. Nursing reflective practice: An empirical literature. J. Nurs. Educ. Pract. 2015, 5, 91–99. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, L.; Johnson, J.; Mandela, R. Reflective practice groups: Are they useful for liaison psychiatry nurses working within the Emergency Department? Arch. Psychiatr. Nurs. 2019, 33, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.M.; Chiu, H.T.; Lin, Y.K.; Chang, W.Y. Development of a situational initiation training program for preceptors to retain new graduate nurses: Process and initial outcomes. Nurse Educ. Today 2016, 37, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kim, J.K.; Park, K.-O. The role experience of preceptor nurses in hospitals. J. Korean Acad. Nurs. Adm. 2012, 18, 33–45. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.S.; Yang, N.Y. Nursing performance and organizational socialization of new nurses according to teaching style of preceptors and personality of new nurses. J. Korean Acad. Nurs. Adm. 2012, 18, 281–289. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.C.; Park, H.S. Clinical competence and organizational socialization according to communication style of preceptors as perceived by new nurses. J. Korean Fund. Nurs. 2016, 23, 42–50. [Google Scholar] [CrossRef]
- Lee, J.; Kim, H.; Lim, S. An integrative review of job stress and mental health intervention programs for experienced nurses. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2019, 28, 190–204. [Google Scholar] [CrossRef]
- Gibbs, G. Learning by Doing: A Guide to Teaching and Learning Methods; Further Education Unit: Oxford, UK, 1988.
- Grossoehme, D.H. Overview of qualitative research. J. Health Care Chaplain. 2014, 20, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Kahlke, R.M. Generic qualitative approaches: Pitfalls and benefits of methodological mixology. Int. J. Qual. Methods 2014, 13, 37–52. [Google Scholar] [CrossRef]
- Lee, J.; Shin, J.; Kim, M.; Jo, M.; Lee, I. Development and evaluation pf cognitive behavior group treatment to reduce psychological stress of emotion labor workers: A preliminary study. STRESS 2016, 24, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Pennebaker, J.W. Writing to Heal: A Guided Journal for Recovering from Trauma and Emotional Upheaval; Center for Journal Therapy Company: Wheat Ridge, CO, USA, 2004. [Google Scholar]
- Forneris, S.G.; Peden-McAlpine, C.J. Contextual learning: A reflective learning intervention for nursing education. IJNES 2006, 3. [Google Scholar] [CrossRef]
- Jeong, S.H.; Shin, J.H. A comparative study of the availability and effectiveness of cinema and role-playing in nursing ethics education. Korean J. Med. Ethics 2015, 18, 276–295. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: Danvers, MA, USA, 1984; pp. 22–223. [Google Scholar]
- Kim, J.; Lee, J. The relationship between factor of stress coping mechanism and depression. Korean J. Behav. Sci. 1985, 7, 127–138. [Google Scholar]
- Park, J. A study on the relationship among character type A & B ego-identity and stress coping. Master’s Thesis, Sookmyung Women’s University, Seoul, South Korea, 1995. [Google Scholar]
- Park, S.Y.; Kim, J.S.; Kim, M.H. A study of the burden of preceptors. J. Korean Fund. Nurs. 2003, 10, 37–46. [Google Scholar]
- Park, J.W. A study to development a scale of social support. Ph.D. Dissertation, Yonsei University, Seoul, South Korea, 1985. [Google Scholar]
- Choi, E.; Yoo, K.H. The influence of social support and health promotion behaviors on nursing work performance among nurses. J. Korean Acad. Soc. Nurs. Educ. 2021, 27, 333–341. [Google Scholar] [CrossRef]
- Yang, C.H.; Kang, Y.S. The impact of a supervisor’s conflict resolution style on a nurse’s organizational citizenship behavior and turnover intention in hospital: The moderating role of emotional intelligence. Korean Assoc. Hum. Resour. Dev. 2017, 20, 137–157. [Google Scholar] [CrossRef]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Guba, E.G.; Lincoln, Y.S. Effective Evaluation: Improving the Usefulness of Evaluation Results through Responsive and Naturalistic Approaches; Jossey-Bass: San Francisco, CA, USA, 1981; pp. 53–225. [Google Scholar]
- Chew, N.W.; Lee, G.K.; Tan, B.Y.; Jing, M.; Goh, Y.; Ngiam, N.J.; Yeo, L.L.; Ahmad, A.; Khan, F.A.; Shanmugam, G.N. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J. Psychological resilience, coping behaviours and social support among health care workers during the COVID-19 pandemic: A systematic review of quantitative studies. J. Nurs. Manag. 2021, 29, 1893–1905. [Google Scholar] [CrossRef] [PubMed]
- Alnazly, E.; Khraisat, O.M.; Al-Bashaireh, A.M.; Bryant, C.L. Anxiety, depression, stress, fear and social support during COVID-19 pandemic among Jordanian healthcare workers. PLoS ONE 2021, 16, e0247679. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A. Nurse preceptors and preceptor education: Implications for preceptor programs, retention strategies, and managerial support. Medsurg. Nurs. 2019, 28, 107–113. [Google Scholar]
- Wu, X.V.; Enskär, K.; Heng, D.; Pua, L.; Wang, W. The perspectives of preceptors regarding clinical assessment for undergraduate nursing students. Int. Nurs. Rev. 2016, 63, 473–481. [Google Scholar] [CrossRef]
- Liu, Y.; Aungsuroch, Y. Work stress, perceived social support, self-efficacy and burnout among Chinese registered nurses. J. Nurs. Manag. 2019, 27, 1445–1453. [Google Scholar] [CrossRef] [PubMed]
- Ebben, V.Z.; Motselisi, M.; Petrus, N. The effect of work stress and emotional intelligence on self-leadership among nurses in leadership positions in the Lesotho Ministry of Health and Social Welfare. Afr. J. Nurs. Midwifery 2017, 19, 88–104. [Google Scholar] [CrossRef]
- Foster, K.; McCloughen, A.; Delgado, C.; Kefalas, C.; Harkness, E. Emotional intelligence education in pre-registration nursing programmes: An integrative review. Nurse Educ. Today 2015, 35, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Kozlowski, D.; Hutchinson, M.; Hurley, J.; Browne, G. Increasing nurses’ emotional intelligence with a brief intervention. Appl. Nurs. Res. 2018, 41, 59–61. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| The Components of the Written Reflective Practice | |
 | |
| The Components of the Verbal Reflective Practice | |
| First workshop |  |
| Second workshop |  |
| Characteristics | Categories | (N = 47) | |
|---|---|---|---|
| n (%) | Mean (SD) | ||
| Age (years) | ≤26 | 15 (31.9) | 27.81 (2.52) |
| 27–29 | 25 (53.2) | ||
| ≥30 | 7 (14.9) | ||
| Sex | Men | 3 (6.4) | |
| Women | 44 (93.6) | ||
| Marital status | Single | 44 (93.6) | |
| Married | 3 (6.4) | ||
| Total working career (years) | <4 | 20 (42.6) | 4.85 (2.80) |
| 4–6 | 20 (42.6) | ||
| >6 | 7 (14.9) | ||
| Work unit | Medical ward | 8 (17.0) | |
| Surgical ward | 10 (21.3) | ||
| Medical ICU | 6 (12.8) | ||
| Surgical ICU | 6 (12.8) | ||
| Other ICU | 8 (17.0) | ||
| Others (OR, ER, Delivery room, Pediatric ward, Emergency ward) | 9 (19.1) | ||
| Voluntarily applied for the preceptor’s role | Yes | 9 (19.1) | |
| No | 38 (80.9) | ||
| Number of preceptor experiences (times) | 1 | 25 (53.2) | |
| 2–5 | 22 (46.8) | ||
| Whether to continue In the role of the preceptor | Yes | 24 (51.1) | |
| No | 23 (48.9) | ||
| Variables | (N = 47) | |||
|---|---|---|---|---|
| Pre-Test | Post-Test | t/z | p | |
| Mean (SD) | Mean (SD) | |||
| Stress coping | 2.80 (0.25) | 2.89 (0.30) | −2.15 | 0.037 |
| Active coping | 3.01 (0.37) | 3.06 (0.39) | −1.08 | 0.285 |
| Problem-focused coping | 2.88 (0.39) | 2.97 (0.43) | −1.52 | 0.135 |
| Seeking social support | 3.14 (0.45) | 3.16 (0.48) | −0.32 | 0.754 |
| Passive coping | 2.59 (0.29) | 2.71 (0.34) | −2.52 | 0.015 |
| Emotional focusing stress coping | 2.32 (0.40) | 2.49 (0.47) | −2.75 | 0.009 |
| Desire thought | 2.85 (0.40) | 2.92 (0.34) | −1.14 | 0.258 |
| Burden of preceptor | 1.61 (0.57) | 1.64 (0.73) | −0.35 | 0.725 |
| Preceptor’s burden related to new nurses | 1.52 (0.66) | 1.54 (0.78) | −0.29 | 0.769 * |
| Preceptor’s burden related to oneself | 1.63 (0.70) | 1.63 (0.81) | −0.40 | 0.968 |
| Preceptor’s burden related to colleagues or others | 1.71 (0.70) | 1.87 (0.83) | −1.30 | 0.201 |
| Social support | 3.23 (0.42) | 3.36 (0.46) | −2.03 | 0.043 * |
| Emotional intelligence | 3.52 (0.63) | 3.82 (0.58) | −3.97 | <0.001 |
| Self-emotions appraisal | 3.97 (0.73) | 4.08 (0.60) | −1.17 | 0.242 * |
| Others-emotions appraisal | 3.79 (0.73) | 4.04 (0.65) | −2.84 | 0.007 |
| Regulation of emotion | 3.34 (0.84) | 3.69 (0.71) | −2.92 | 0.005 |
| Use of emotion | 2.97 (0.77) | 3.45 (0.89) | −3.59 | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-S.; Jeong, H.-W.; Ju, D.; Lee, J.-A.; Ahn, S.-H. Development and Preliminary Evaluation of the Effects of a Preceptor Reflective Practice Program: A Mixed-Method Research. Int. J. Environ. Res. Public Health 2022, 19, 13755. https://doi.org/10.3390/ijerph192113755
Kim H-S, Jeong H-W, Ju D, Lee J-A, Ahn S-H. Development and Preliminary Evaluation of the Effects of a Preceptor Reflective Practice Program: A Mixed-Method Research. International Journal of Environmental Research and Public Health. 2022; 19(21):13755. https://doi.org/10.3390/ijerph192113755
Chicago/Turabian StyleKim, Heui-Seon, Hye-Won Jeong, Deok Ju, Jung-A Lee, and Shin-Hye Ahn. 2022. "Development and Preliminary Evaluation of the Effects of a Preceptor Reflective Practice Program: A Mixed-Method Research" International Journal of Environmental Research and Public Health 19, no. 21: 13755. https://doi.org/10.3390/ijerph192113755