
Polydrug Definition and Assessment: The State of the Art

Abstract
:
1. Introduction
2. Materials and Methods
3. Results
3.1. The Beginnings
3.2. Initial Definitions
3.3. Development of the Concept and Its First Forms of Evaluation
3.4. Incorporation of Simultaneity in Polydrug Use Assessment
3.5. Other Developments in Polydrug Use Assessment
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- European Monitoring Centre for Drugs and Drug Abuse. Polydrug Use, 1st ed.; Publications Office of the European Union: Lisbon, Portugal, 2002. [Google Scholar]
- Montanari, L.; Guarita, B. Polydrug Use among Drug Treatment Clients in Europe. What Implications for Treatment? 1st ed.; EMCDDA: Luxembourg, 2015. [Google Scholar]
- European Monitoring Centre for Drugs and Drug Addiction. Polydrug Use: Patterns and Responses, 1st ed.; Publications Office of the European Union: Luxembourg, 2009. [Google Scholar]
- European Monitoring Centre for Drugs and Drug Abuse. Polydrug Use: Health and Social Responses, 1st ed.; Publications Office of the European Union: Lisbon, Portugal, 2021. [Google Scholar]
- Hernández-Serrano, O.; Gras, M.E.; Font-Mayolas, S.; Sullman, M.J.M. Types of polydrug use. In The Neuropathology of Drug Addictions and Substance Misuse, 1st ed.; Preedy, V.R., Ed.; Elsevier Academic Press: London, UK, 2015; pp. 839–849. [Google Scholar]
- World Health Organization. Lexicon of Alcohol and Drug Terms, 1st ed.; WHO: Geneva, Switzerland, 1994. [Google Scholar]
- Kunnes, R. Drugs and public policy. Poly-drug abuse: Drug companyies and doctors. Am. J. Orthopsychiatry 1973, 43, 530–532. [Google Scholar] [CrossRef] [PubMed]
- Wesson, D.R.; Smith, D.E.; Lerner, S.E.; Kettner, V.R. Treatment of polydrug users in San Francisco. Am. J. Drug Alcohol Abuse 1974, 1, 159–179. [Google Scholar] [CrossRef] [PubMed]
- Bourne, P.G. Polydrug abuse: Considerations in a national strategy. Am. J. Drug Alcohol Abuse 1974, 1, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Johnston, L. Defining the term polydrug use. In Research Monograph Series 2. Operational Definitions in Socio-Behavioral Drug Use Research, 1st ed.; Elinson, J., Nurco, D., Eds.; National Institute on Drug Abuse: Gaithersburg, MD, USA, 1975; pp. 36–39. [Google Scholar]
- Kaufman, E. The abuse of multiple drugs. I. Definition, classification, and extent of the problem. Am. J. Drug Alcohol Abuse 1976, 3, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, E. Polydrug abuse or multidrug misuse: It’s here to stay. Br. J. Addict. 1977, 72, 339–347. [Google Scholar] [CrossRef]
- Douglass, F.M.; Khavari, K.A. The Drug Use Index: A measure of the extent of polydrug usage. Int. J. Addict. 1978, 13, 981–993. [Google Scholar] [CrossRef]
- Khavari, K.A.; Douglass, F.M. The Polydrug Assessment Scale: A psychometric technique for the indirect measurement of drug use. J. Consult. Clin. Psychol. 1978, 46, 1566–1568. [Google Scholar] [CrossRef]
- Morrissey, E.R. The measurement of multiple drug use and its relationship to the patterning of alcohol intake. Am. J. Drug Alcohol Abuse 1981, 8, 311–328. [Google Scholar] [CrossRef]
- Martin, C.S.; Arria, A.M.; Mezzich, Z.C.; Bukstein, O.G. Patterns of polydrug use in adolescent alcohol abusers. Am. J. Drug Alcohol Abuse 1993, 19, 511–521. [Google Scholar] [CrossRef]
- Boys, A.; Lenton, S.; Norcross, K. Polydrug use at raves by a Western Australian sample. Drug Alcohol Rev. 1997, 16, 227–234. [Google Scholar] [CrossRef]
- Schuler, M.S.; Collins, R.L.; Ramchand, R. Disparities in use/misuse of specific illicit and prescription drugs among sexual minority adults in a national sample. Subst. Use Misuse 2022, 57, 461–471. [Google Scholar] [CrossRef]
- Reyes, J.; Perez, C.; Colon, H.; Dowell, M.; Cumsille, F. Prevalence and patterns of polydrug use in Latin America: Analysis of population-based surveys in six countries. Rev. Eur. Stud. 2013, 5, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Kongjareon, Y.; Samoh, N.; Peerawaranun, P.; Guadamuz, T.E. Pride-based violence, intoxicated sex and poly-drug use: A vocational school-based study of heterosexual and LGBT students in Bangkok. BMC Psychiatry 2022, 22, 148. [Google Scholar] [CrossRef]
- Sneed, C.D.; Morisky, D.E.; Rotheram-Borus, M.J.; Lee, S.J.; Ebin, V.J. Indices of lifetime polydrug use among adolescents. J. Adolesc. 2004, 27, 239–249. [Google Scholar] [CrossRef]
- Kandel, D.; Yamaguchi, K. From beer to crack: Developmental patterns of drug use involvement. Am. J. Public Health 1993, 83, 851–855. [Google Scholar] [CrossRef] [Green Version]
- Font-Mayolas, S.; Gras, M.E.; Cebrián, N.; Salamó, A.; Planes, M.; Sullman, M.J.M. Types of polydrug use among Spanish adolescents. Addict. Behav. 2013, 38, 1605–1609. [Google Scholar] [CrossRef]
- Font-Mayolas, S.; Hernández-Serrano, O.; Gras, M.E.; Sullman, M.J.M. Types of polydrug among Spanish students in Health Sciences. J. Addict. Nurs. 2019, 30, 108–113. [Google Scholar] [CrossRef]
- Sañudo, A.; Andreoni, S.; Sanchez, Z.M. Polydrug use among nightclub patrons in a megacity: A latent class analysis. Int. J. Drug Policy 2015, 26, 1207–1214. [Google Scholar] [CrossRef]
- Martínez-Loredo, V.; Fernández-Hermida, J.R.; de La Torre-Luque, A.; Fernández-Artamendi, S. Polydrug use trajectories and differences in impulsivity among adolescents. Int. J. Clin. Health Psychol. 2018, 18, 235–244. [Google Scholar] [CrossRef]
- Higgins, K.; O’Neill, N.; O’Hara, L.; Jordan, J.A.; McCann, M.; O’Neill, T.; Clarke, M.; O’Neill, T.; Kelly, G.; Campbell, A. New psychoactives within polydrug use trajectòries—Evidence from a mixed-method longitudinal study. Addiction 2021, 116, 2454–2462. [Google Scholar] [CrossRef]
- Guerras, J.M.; Hoyos, J.; García, P.; de la Fuente, L.; Herrero, L.; Palma, D.; del Romero, J.; García-Pérez, J.N.; Belza, M.J.; The Methysos Project Group. Comparison of polydrug use prevalences ans typologies between men who have sex with men and general population men, in Madrid and Barcelona. Int. J. Environ. Res. Public Health 2021, 18, 11609. [Google Scholar] [CrossRef]
- Schepis, T.S.; McCabe, S.E. The latent class structure of substance use in US adults 50 years and older. Int. J. Geriatr. Psychiatry 2021, 36, 1867–1877. [Google Scholar] [CrossRef]
- De Jonge, M.C.; Bukman, A.J.; van Leeuwen, L.; Onrust, S.A.; Kleinjan, M. Latent classes of substance use in young adults—A systematic review. Subst. Use Misuse 2022, 57, 769–785. [Google Scholar] [CrossRef]
- Grant, B.F.; Harford, T.C. Concurrent and simultaneous use of alcohol with sedatives and with tranquilizers: Results of a national survey. J. Subst. Abuse 1990, 2, 1–14. [Google Scholar] [CrossRef]
- Grant, B.F.; Harford, T.C. Concurrent and simultaneous use of alcohol with cocaine: Results of national survey. Drug Alcohol Depend. 1990, 25, 97–104. [Google Scholar] [CrossRef]
- Martin, C.S.; Clifford, P.R.; Clapper, R.L. Patterns and predictors of simultaneous and concurrent use of alcohol, tobacco, marijuana, and hallucinogens in first-year college students. J. Subst. Abuse 1992, 4, 319–326. [Google Scholar] [CrossRef]
- Earleywine, M.; Newcomb, M.D. Concurrent versus simultaneous polydrug use: Prevalence, correlates, discriminant validity, and prospective effects on health outcomes. Exp. Clin. Psychopharmacol. 1997, 5, 353–364. [Google Scholar] [CrossRef]
- Collins, R.L.; Ellickson, P.L.; Bell, R.M. Simultaneous polydrug use among teens: Prevalence and predictors. J. Subst. Abuse 1998, 10, 233–253. [Google Scholar] [CrossRef]
- McCabe, S.E.; Cranford, J.A.; Morales, M.; Young, A. Simultaneous and concurrent polydrug use of alcohol and prescription drugs: Prevalence, correlates, and consequences. J. Stud. Alcohol 2006, 67, 529–537. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.S. Timing of alcohol and other drug use. Alcohol Res. Health 2008, 31, 96–99. [Google Scholar]
- Boileau-Falardeau, M.; Contreras, G.; Gariépy, G.; Laprise, C. Patterns and motivations of polysubstance use: A rapid review of the qualitative evidence. Health Promot. Chronic Dis. Prev. Can. 2022, 42, 47–59. [Google Scholar] [CrossRef]
- King, C.P.; Meyer, P.J. The incentive ampliflying effects of nicotine: Roles in alcohol seeking and consumption. Adv. Pharmacol. 2022, 93, 171–218. [Google Scholar] [CrossRef]
- Quek, R.H.; Chan, G.C.K.; White, A.; Connor, J.P.; Baker, P.J.; Saunders, J.B.; Kelly, A.B. Concurrent and simultaneous polydrug use: Latent class analysis of an Australian nationally representatives sample of young adults. Front. Public Health 2013, 1, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baggio, S.; Studer, J.; Mohler-Kuo, M.; Daeppen, J.B.; Gmel, G. Concurrent and simultaneous polydrug use among Young Swiss males: Use patterns and associations of number of substances used with health issues. Int. J. Adolesc. Med. Health 2014, 26, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Baggio, S.; Deline, S.; Studer, J.; N’Goran, A.; Mohler-Kuo, M.; Daeppen, J.B.; Gmel, G. Concurrent versus simultaneous use of alcohol and non-medical use of prescription drugs: Is simultaneous use worse for mental, social, and health issues? J. Psychoact. Drugs 2014, 46, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, K.; Kuussaari, K.; Kataja, K.; Tigerstedt, C.; Hakkarainen, P. Measuring concurrent polydrug use in general populations: A critical assessment. Eur. Addict. Res. 2017, 23, 163–169. [Google Scholar] [CrossRef]
- Garrido-González, I.; Bugarín-González, R.; Machín-Fernández, A.J. Consumo de drogas en estudiantes de enfermería. Enferm. Clin. 2016, 26, 174–180. [Google Scholar] [CrossRef]
- Hernández-Serrano, O.; Gras, M.E.; Font-Mayolas, S. Concurrent and simultaneous use of cannabis and tobacco and its relationship with acadèmic achievement amongst university students. Behav. Sci. 2018, 8, 31. [Google Scholar] [CrossRef] [Green Version]
- Bombard, J.M.; Pederson, L.L.; Nelson, D.E.; Marlarcher, A.M. Are smokers only using cigarettes? Exploring current polytobacco use among an adult population. Addict. Behav. 2007, 32, 2411–2419. [Google Scholar] [CrossRef] [Green Version]
- Pebley, K.; Krukowski, R.A.; Mallawaarachchi, I.; Talcott, G.W.; Klesger, R.C.; Little, M.A. Dual and polytobacco use after a period of enforced tobacco cessation. Addict. Behav. 2021, 123, 107077. [Google Scholar] [CrossRef]
- Font-Mayolas, S.; Sullman, M.J.M.; Gras, M.E. Sex and polytobacco use among Spanish and Turkish university students. Int J Environ Res Public Health 2019, 16, 5038. [Google Scholar] [CrossRef] [PubMed]
- Haardörfer, R.; Berg, C.J.; Lewis, M.; Payne, J.; Pillai, D.; McDonald, B.; Windle, M. Polytobacco, marihuana, and alcohol use paterns in college students: A latent class analysis. Addict. Behav. 2016, 59, 58–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arango, E.; Toriello, A.; Rosario, Z.; Cooper, G. Increasing prevalence of ketamine in drivers in New York city including the identification of 2-Fluoro-Deschloroketamine. J. Anal. Toxicol. 2021, 45, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.H.; Liu, Y.H.; Huang, Y.J.; Tang, W.K.; Wang, Y.; Hu, S.; Lin, C.P.; Li, C.S.R.; Hung, C.C. Clinical and behavior characteristics of individuals who used ketamine. Sci. Rep. 2022, 12, 801. [Google Scholar] [CrossRef] [PubMed]
- Brunt, T.M.; Lefrançois, E.; Gunnar, T.; Arponen, A.; Seyler, T.; Goudriaan, A.E.; McAuley, A.; McKeown, D.A.; Detrez, V.; Csorba, J.; et al. Substances detected in used syringes of injecting drug users across 7 cities in Europe in 2017 and 2018: The European Syringe Collection and Analysis Project Enterprise (ESCAPE). Int. J. Drug Policy 2021, 95, 103130. [Google Scholar] [CrossRef]
- Stevens, C.; Li, T.; Ton, E.; Zou, J.; Douglas, E.; Jones, P. Longitudinal Opioid Surveillance Project Involving Toxicologic Analysis of Postmortem Specimens from 9 Counties in Michigan Suggests the Discovery of New High-Intensity Drug Trafficking Areas. Am. J. Forensic Med. Pathol. 2021, 42, 216–224. [Google Scholar] [CrossRef]
- Gili, A.; Lania, M.; Mercurio, I.; Bacci, M.; Nicoletti, A.; Pelliccia, C.; Gambelunghe, C. Patterns of prescription medicine, illicit drugs, and alcohol misuse among high-risk population: A factor analysis to delineate profil·les of polydrug users. Healthcare 2022, 10, 710. [Google Scholar] [CrossRef]
- Pollard, C.; Sievers, C.; Royall, P.G.; Wolf, K. Evaluation of latent fingerprints for drug screening in a social care setting. J. Anal. Toxicol. 2022, 46, 47–54. [Google Scholar] [CrossRef]
- Bergström, M.A.; Lövgrren, H.; Abrahamsson, A.; Eriksson, E.K.; Andersson, M.L.; Komorowska, M.; Axelsson, M.A.B. Rethinking drug analysis in Health care: High-throghput analysis of 71 drugs of abuse in oral fluid using ion mobility- high resolution mass spectometry. J. Anal. Toxicol. 2022, 46, 765–775. [Google Scholar] [CrossRef]
- Smith, K.E.; Rogers, J.M.; Schriefer, D.; Grundman, O. Therapeutic benefit with caveats?: Analyzing social media data to understand the complexities of kratom use. Drug Alcohol Depend. 2021, 226, 188879. [Google Scholar] [CrossRef]
- Shiue, K.Y.; Austin, A.E.; Proescholdbell, S.; Cox, M.E.; Aurelius, M.; Naumann, R.B. Literal text analysis of poly-class overdose deaths in North Carolina, 2015–2019. Drug Alcohol Depend. 2021, 228, 109048. [Google Scholar] [CrossRef] [PubMed]
- West, H.; Fitzgerald, J.; Hopkins, K.; Li, E.; Clark, N.; Tzanetis, S.; Greene, S.L.; Reid, G.E. Early warning system for illicit drug use at large public events: Trace residue analysis of discarded drug packaging samples. J. Am. Soc. Mass Spectrom. 2021, 32, 2604–2614. [Google Scholar] [CrossRef]
- Kataja, K.; Tigerstedt, C.; Hakkarainen, P. More social research into polydrug use. Nordisk Alkohol Nark. 2018, 35, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.J.; Johnson, M.W. Verbal behaviour related to drug reinforcement in polysubstance cannabis users: Comparison across drugs. Exp. Clin. Psychopharmacol. 2022, 30, 172–179. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Polydrug Use | Key Information |
|---|---|
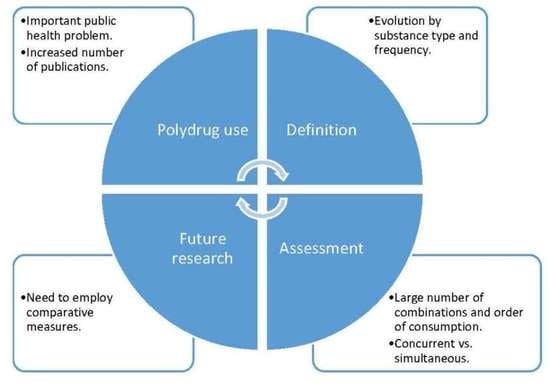
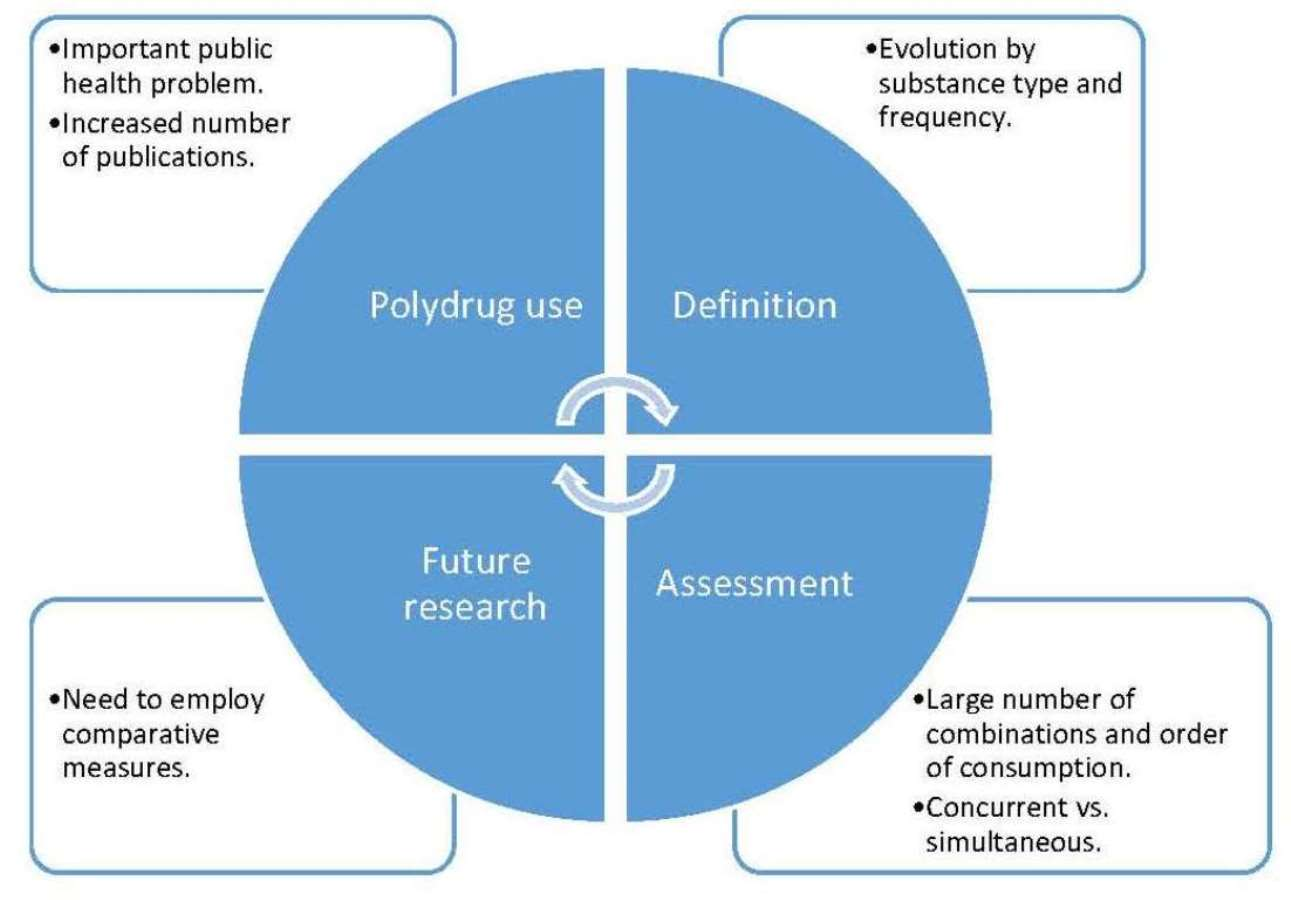
| Definition | The term “polydrug” (or polysubstance use) has imposed itself over the term “multidrug”, which was situated mainly in the medical field of resistance in bacteria. |
| Currently, polydrug use is defined as the use of more than one kind of substance (whether illicit or legal) by an individual, either at the same time or sequentially. | |
| The EMCDDA [4] proposes a classification of polydrug use types according to substance combination: Type A (alcohol and tobacco); Type B (cannabis together with alcohol and/or tobacco); and Type C (cannabis together with alcohol and/or tobacco and at least one of the following substances: ecstasy, cocaine, amphetamines, LSD or heroin). | |
| Assessment | The assessment of polydrug use began with the incorporation of measures aimed at defining severity of consumption by awarding weights according to type of substance or combinations thereof, and the frequency and duration of consumption of each substance or combination. |
| Analysing simultaneity of use allows for a distinction to be made between concurrent and simultaneous polydrug use, these being two constructs that correlate but are distinguished at the level of discriminant validity (different intentionality of consumption, for example). | |
| Combinations of substances, the period of consumption being referred to and the types of scales used to evaluate frequency of consumption all vary in concurrent and simultaneous polydrug use assessment. The main difficulties arise from delimiting the large number of combinations of psychoactive substances and, in the case of simultaneous consumption, the time intervals recorded. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Font-Mayolas, S.; Calvo, F. Polydrug Definition and Assessment: The State of the Art. Int. J. Environ. Res. Public Health 2022, 19, 13542. https://doi.org/10.3390/ijerph192013542
Font-Mayolas S, Calvo F. Polydrug Definition and Assessment: The State of the Art. International Journal of Environmental Research and Public Health. 2022; 19(20):13542. https://doi.org/10.3390/ijerph192013542
Chicago/Turabian StyleFont-Mayolas, Sílvia, and Fran Calvo. 2022. "Polydrug Definition and Assessment: The State of the Art" International Journal of Environmental Research and Public Health 19, no. 20: 13542. https://doi.org/10.3390/ijerph192013542