

Knee Strength Assessment and Clinical Evaluation Could Predict Return to Running after Anterior Cruciate Ligament Reconstruction Using Patellar Tendon Procedure
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
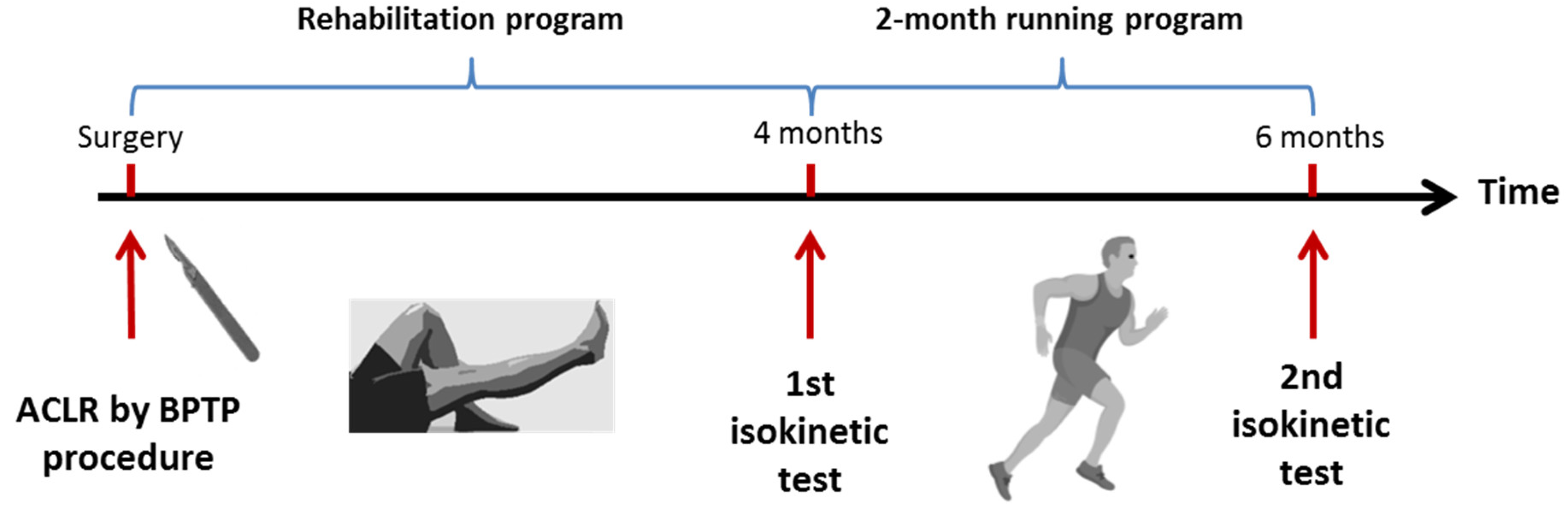
2.2. ACLR Using a BPTB Arthoscopic Procedure
2.3. Rehabilitation Program
2.4. Clinical Evaluation by the Lysholm Knee Scoring Scale
2.5. Isokinetic Procedure
2.6. Statistical Analysis
3. Results
3.1. Comparison between RTR and NRTR Groups
3.2. Predictive Model including LSI for Return to Running
3.3. Predictive Model including Strength to Body Weight for Return to Running
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanders, T.L.; Maradit Kremers, H.; Bryan, A.J.; Larson, D.R.; Dahm, D.L.; Levy, B.A.; Stuart, M.J.; Krych, A.J. Incidence of Anterior Cruciate Ligament Tears and Reconstruction: A 21-Year Population-Based Study. Am. J. Sports Med. 2016, 44, 1502–1507. [Google Scholar] [CrossRef] [PubMed]
- Mouarbes, D.; Menetrey, J.; Marot, V.; Courtot, L.; Berard, E.; Cavaignac, E. Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis of Outcomes for Quadriceps Tendon Autograft Versus Bone-Patellar Tendon-Bone and Hamstring-Tendon Autografts. Am. J. Sports Med. 2019, 47, 3531–3540. [Google Scholar] [CrossRef] [PubMed]
- Gifstad, T.; Foss, O.A.; Engebretsen, L.; Lind, M.; Forssblad, M.; Albrektsen, G.; Drogset, J.O. Lower Risk of Revision with Patellar Tendon Autografts Compared with Hamstring Autografts: A Registry Study Based on 45,998 Primary ACL Reconstructions in Scandinavia. Am. J. Sports Med. 2014, 42, 2319–2328. [Google Scholar] [CrossRef] [PubMed]
- Myer, G.D.; Paterno, M.V.; Ford, K.R.; Quatman, C.E.; Hewett, T.E. Rehabilitation after Anterior Cruciate Ligament Reconstruction: Criteria-Based Progression through the Return-to-Sport Phase. J. Orthop. Sports Phys. Ther. 2006, 36, 385–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A.H.; Capin, J.J.; Zarzycki, R.; Snyder-Mackler, L. Athletes with Bone-Patellar Tendon-Bone Autograft for Anterior Cruciate Ligament Reconstruction Were Slower to Meet Rehabilitation Milestones and Return-to-Sport Criteria Than Athletes With Hamstring Tendon Autograft or Soft Tissue Allograft: Secondary Analysis From the ACL-SPORTS Trial. J. Orthop. Sports Phys. Ther. 2020, 50, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Rice, D.A.; McNair, P.J. Quadriceps Arthrogenic Muscle Inhibition: Neural Mechanisms and Treatment Perspectives. Semin. Arthritis Rheum. 2010, 40, 250–266. [Google Scholar] [CrossRef] [PubMed]
- Pietrosimone, B.G.; Lepley, A.S.; Ericksen, H.M.; Clements, A.; Sohn, D.H.; Gribble, P.A. Neural Excitability Alterations After Anterior Cruciate Ligament Reconstruction. J. Athl. Train. 2015, 50, 665–674. [Google Scholar] [CrossRef] [Green Version]
- Kuenze, C.M.; Hertel, J.; Weltman, A.; Diduch, D.; Saliba, S.A.; Hart, J.M. Persistent Neuromuscular and Corticomotor Quadriceps Asymmetry after Anterior Cruciate Ligament Reconstruction. J. Athl. Train. 2015, 50, 303–312. [Google Scholar] [CrossRef] [Green Version]
- Perraton, L.; Clark, R.; Crossley, K.; Pua, Y.-H.; Whitehead, T.; Morris, H.; Telianidis, S.; Bryant, A. Impaired Voluntary Quadriceps Force Control Following Anterior Cruciate Ligament Reconstruction: Relationship with Knee Function. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2017, 25, 1424–1431. [Google Scholar] [CrossRef]
- Dauty, M.; Menu, P.; Mesland, O.; Fouasson-Chailloux, A. Arthrogenic Muscle Inhibition and Return to Sport after Arthrofibrosis Complicating Anterior Cruciate Ligament Surgery. Eur. J. Sport Sci. 2021, 22, 627–635. [Google Scholar] [CrossRef]
- Kuenze, C.; Pietrosimone, B.; Lisee, C.; Rutherford, M.; Birchmeier, T.; Lepley, A.; Hart, J. Demographic and Surgical Factors Affect Quadriceps Strength after ACL Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2019, 27, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Maestroni, L.; Read, P.; Turner, A.; Korakakis, V.; Papadopoulos, K. Strength, Rate of Force Development, Power and Reactive Strength in Adult Male Athletic Populations Post Anterior Cruciate Ligament Reconstruction—A Systematic Review and Meta-Analysis. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2021, 47, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Cristiani, R.; Mikkelsen, C.; Wange, P.; Olsson, D.; Stålman, A.; Engström, B. Autograft Type Affects Muscle Strength and Hop Performance after ACL Reconstruction. A Randomised Controlled Trial Comparing Patellar Tendon and Hamstring Tendon Autografts with Standard or Accelerated Rehabilitation. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2021, 29, 3025–3036. [Google Scholar] [CrossRef] [PubMed]
- Tajdini, H.; Letafatkar, A.; Brewer, B.W.; Hosseinzadeh, M. Association between Kinesiophobia and Gait Asymmetry after ACL Reconstruction: Implications for Prevention of Reinjury. Int. J. Environ. Res. Public. Health 2021, 18, 3264. [Google Scholar] [CrossRef] [PubMed]
- Pietrosimone, B.; Davis-Wilson, H.C.; Seeley, M.K.; Johnston, C.; Spang, J.T.; Creighton, R.A.; Kamath, G.M.; Blackburn, J.T. Gait Biomechanics in Individuals Meeting Sufficient Quadriceps Strength Cutoffs Following Anterior Cruciate Ligament Reconstruction. J. Athl. Train. 2021, 56, 960–966. [Google Scholar] [CrossRef] [PubMed]
- Rambaud, A.J.M.; Ardern, C.L.; Thoreux, P.; Regnaux, J.-P.; Edouard, P. Criteria for Return to Running after Anterior Cruciate Ligament Reconstruction: A Scoping Review. Br. J. Sports Med. 2018, 52, 1437–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, E.M.; Greenberg, E.T.; Albaugh, J.; Storey, E.; Ganley, T.J. Anterior Cruciate Ligament Reconstruction Rehabilitation Clinical Practice Patterns: A Survey of the PRiSM Society. Orthop. J. Sports Med. 2019, 7, 2325967119839041. [Google Scholar] [CrossRef] [Green Version]
- Lewek, M.; Rudolph, K.; Axe, M.; Snyder-Mackler, L. The Effect of Insufficient Quadriceps Strength on Gait after Anterior Cruciate Ligament Reconstruction. Clin. Biomech. Bristol Avon 2002, 17, 56–63. [Google Scholar] [CrossRef]
- Kline, P.W.; Morgan, K.D.; Johnson, D.L.; Ireland, M.L.; Noehren, B. Impaired Quadriceps Rate of Torque Development and Knee Mechanics After Anterior Cruciate Ligament Reconstruction With Patellar Tendon Autograft. Am. J. Sports Med. 2015, 43, 2553–2558. [Google Scholar] [CrossRef] [Green Version]
- Pamukoff, D.N.; Montgomery, M.M.; Choe, K.H.; Moffit, T.J.; Garcia, S.A.; Vakula, M.N. Bilateral Alterations in Running Mechanics and Quadriceps Function Following Unilateral Anterior Cruciate Ligament Reconstruction. J. Orthop. Sports Phys. Ther. 2018, 48, 960–967. [Google Scholar] [CrossRef]
- Pairot-de-Fontenay, B.; Willy, R.W.; Elias, A.R.C.; Mizner, R.L.; Dubé, M.-O.; Roy, J.-S. Running Biomechanics in Individuals with Anterior Cruciate Ligament Reconstruction: A Systematic Review. Sports Med. Auckl. N. Z. 2019, 49, 1411–1424. [Google Scholar] [CrossRef] [PubMed]
- Knurr, K.A.; Kliethermes, S.A.; Stiffler-Joachim, M.R.; Cobian, D.G.; Baer, G.S.; Heiderscheit, B.C. Running Biomechanics Before Injury and 1 Year After Anterior Cruciate Ligament Reconstruction in Division I Collegiate Athletes. Am. J. Sports Med. 2021, 49, 2607–2614. [Google Scholar] [CrossRef] [PubMed]
- Asaeda, M.; Deie, M.; Kono, Y.; Mikami, Y.; Kimura, H.; Adachi, N. The Relationship between Knee Muscle Strength and Knee Biomechanics during Running at 6 and 12 Months after Anterior Cruciate Ligament Reconstruction. Asia-Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2019, 16, 14–18. [Google Scholar] [CrossRef]
- Dingenen, B.; Gokeler, A. Optimization of the Return-to-Sport Paradigm After Anterior Cruciate Ligament Reconstruction: A Critical Step Back to Move Forward. Sports Med. Auckl. N. Z. 2017, 47, 1487–1500. [Google Scholar] [CrossRef] [PubMed]
- Dauty, M.; Edouard, P.; Menu, P.; Mesland, O.; Fouasson-Chailloux, A. Isokinetic Quadriceps Symmetry Helps in the Decision to Return to Running after Anterior Cruciate Ligament Reconstruction. Ann. Phys. Rehabil. Med. 2021, 65, 101543. [Google Scholar] [CrossRef]
- Iwame, T.; Matsuura, T.; Okahisa, T.; Katsuura-Kamano, S.; Wada, K.; Iwase, J.; Sairyo, K. Quadriceps Strength to Body Weight Ratio Is a Significant Indicator for Initiating Jogging after Anterior Cruciate Ligament Reconstruction. Knee 2021, 28, 240–246. [Google Scholar] [CrossRef]
- Aune, A.K.; Holm, I.; Risberg, M.A.; Jensen, H.K.; Steen, H. Four-Strand Hamstring Tendon Autograft Compared with Patellar Tendon-Bone Autograft for Anterior Cruciate Ligament Reconstruction. A Randomized Study with Two-Year Follow-Up. Am. J. Sports Med. 2001, 29, 722–728. [Google Scholar] [CrossRef]
- Shelbourne, K.D.; Nitz, P. Accelerated Rehabilitation after Anterior Cruciate Ligament Reconstruction. J. Orthop. Sports Phys. Ther. 1992, 15, 256–264. [Google Scholar] [CrossRef]
- De Carlo, M.S.; Sell, K.E.; Shelbourne, K.D.; Klootwyk, T.E. Current Concepts on Accelerated ACL Rehabilitation. J. Sport Rehabil. 1994, 3, 304–318. [Google Scholar] [CrossRef]
- Tegner, Y.; Lysholm, J. Rating Systems in the Evaluation of Knee Ligament Injuries. Clin. Orthop. 1985, 198, 43–49. [Google Scholar] [CrossRef]
- Tegner, Y.; Lysholm, J.; Odensten, M.; Gillquist, J. Evaluation of Cruciate Ligament Injuries. A Review. Acta Orthop. Scand. 1988, 59, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Briggs, K.K.; Lysholm, J.; Tegner, Y.; Rodkey, W.G.; Kocher, M.S.; Steadman, J.R. The Reliability, Validity, and Responsiveness of the Lysholm Score and Tegner Activity Scale for Anterior Cruciate Ligament Injuries of the Knee: 25 Years Later. Am. J. Sports Med. 2009, 37, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Shelbourne, K.D.; Patel, D.V.; Martini, D.J. Classification and Management of Arthrofibrosis of the Knee after Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 1996, 24, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Dauty, M.; Tortelier, L.; Huguet, D.; Potiron-Josse, M.; Dubois, C. Consequences of pain on isokinetic performance after anterior cruciate ligament reconstruction using a semitendinosus and gracilis autograft. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2006, 92, 455–463. [Google Scholar] [CrossRef]
- Lepley, A.S.; Pietrosimone, B.; Cormier, M.L. Quadriceps Function, Knee Pain, and Self-Reported Outcomes in Patients With Anterior Cruciate Ligament Reconstruction. J. Athl. Train. 2018, 53, 337–346. [Google Scholar] [CrossRef] [Green Version]
- Impellizzeri, F.M.; Bizzini, M.; Rampinini, E.; Cereda, F.; Maffiuletti, N.A. Reliability of Isokinetic Strength Imbalance Ratios Measured Using the Cybex NORM Dynamometer. Clin. Physiol. Funct. Imaging 2008, 28, 113–119. [Google Scholar] [CrossRef]
- Stoltzfus, J.C. Logistic Regression: A Brief Primer. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2011, 18, 1099–1104. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Diagnostic Tests 3: Receiver Operating Characteristic Plots. BMJ 1994, 309, 188. [Google Scholar] [CrossRef] [Green Version]
- Deeks, J.J.; Altman, D.G. Diagnostic Tests 4: Likelihood Ratios. BMJ 2004, 329, 168–169. [Google Scholar] [CrossRef] [Green Version]
- American Heart Association. Target Heart Rates Chart. Available online: https://www.heart.org/en/healthy-living/fitness/fitness-basics/target-heart-rates (accessed on 1 June 2022).
- Chertoff, J.; Bubnis, D. What’s the Average Running Speed and Can You Improve Your Pace? Available online: https://www.healthline.com/health/fitness-exercise/average-running-speed (accessed on 1 June 2022).
- Zarzycki, R.; Morton, S.M.; Charalambous, C.C.; Pietrosimone, B.; Williams, G.N.; Snyder-Mackler, L. Examination of Corticospinal and Spinal Reflexive Excitability During the Course of Postoperative Rehabilitation After Anterior Cruciate Ligament Reconstruction. J. Orthop. Sports Phys. Ther. 2020, 50, 516–522. [Google Scholar] [CrossRef]
- Dauty, M.; Tortellier, L.; Rochcongar, P. Isokinetic and Anterior Cruciate Ligament Reconstruction with Hamstrings or Patella Tendon Graft: Analysis of Literature. Int. J. Sports Med. 2005, 26, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Wellsandt, E.; Failla, M.J.; Snyder-Mackler, L. Limb Symmetry Indexes Can Overestimate Knee Function After Anterior Cruciate Ligament Injury. J. Orthop. Sports Phys. Ther. 2017, 47, 334–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, K.S.; Ha, J.K.; Yeom, C.H.; Ra, H.J.; Lim, J.W.; Kwon, M.S.; Kim, J.G. Are Muscle Strength and Function of the Uninjured Lower Limb Weakened After Anterior Cruciate Ligament Injury? Two-Year Follow-up After Reconstruction. Am. J. Sports Med. 2015, 43, 3013–3021. [Google Scholar] [CrossRef] [PubMed]
- Lepley, A.S.; Gribble, P.A.; Thomas, A.C.; Tevald, M.A.; Sohn, D.H.; Pietrosimone, B.G. Quadriceps Neural Alterations in Anterior Cruciate Ligament Reconstructed Patients: A 6-Month Longitudinal Investigation. Scand. J. Med. Sci. Sports 2015, 25, 828–839. [Google Scholar] [CrossRef]
- Zult, T.; Gokeler, A.; van Raay, J.J.A.M.; Brouwer, R.W.; Zijdewind, I.; Hortobágyi, T. An Anterior Cruciate Ligament Injury Does Not Affect the Neuromuscular Function of the Non-Injured Leg except for Dynamic Balance and Voluntary Quadriceps Activation. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2017, 25, 172–183. [Google Scholar] [CrossRef] [Green Version]
- Harbo, T.; Brincks, J.; Andersen, H. Maximal Isokinetic and Isometric Muscle Strength of Major Muscle Groups Related to Age, Body Mass, Height, and Sex in 178 Healthy Subjects. Eur. J. Appl. Physiol. 2012, 112, 267–275. [Google Scholar] [CrossRef]
- Risberg, M.A.; Steffen, K.; Nilstad, A.; Myklebust, G.; Kristianslund, E.; Moltubakk, M.M.; Krosshaug, T. Normative Quadriceps and Hamstring Muscle Strength Values for Female, Healthy, Elite Handball and Football Players. J. Strength Cond. Res. 2018, 32, 2314–2323. [Google Scholar] [CrossRef] [Green Version]
- Logerstedt, D.; Lynch, A.; Axe, M.J.; Snyder-Mackler, L. Symmetry Restoration and Functional Recovery before and after Anterior Cruciate Ligament Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2013, 21, 859–868. [Google Scholar] [CrossRef] [Green Version]
- Abrams, G.D.; Harris, J.D.; Gupta, A.K.; McCormick, F.M.; Bush-Joseph, C.A.; Verma, N.N.; Cole, B.J.; Bach, B.R. Functional Performance Testing After Anterior Cruciate Ligament Reconstruction: A Systematic Review. Orthop. J. Sports Med. 2014, 2, 2325967113518305. [Google Scholar] [CrossRef]
- Werner, J.L.; Burland, J.P.; Mattacola, C.G.; Toonstra, J.; English, R.A.; Howard, J.S. Decision to Return to Sport Participation After Anterior Cruciate Ligament Reconstruction, Part II: Self-Reported and Functional Performance Outcomes. J. Athl. Train. 2018, 53, 464–474. [Google Scholar] [CrossRef]
- Rambaud, A.J.M.; Semay, B.; Samozino, P.; Morin, J.-B.; Testa, R.; Philippot, R.; Rossi, J.; Edouard, P. Criteria for Return to Sport after Anterior Cruciate Ligament Reconstruction with Lower Reinjury Risk (CR’STAL Study): Protocol for a Prospective Observational Study in France. BMJ Open 2017, 7, e015087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welling, W.; Benjaminse, A.; Seil, R.; Lemmink, K.; Zaffagnini, S.; Gokeler, A. Low Rates of Patients Meeting Return to Sport Criteria 9 Months after Anterior Cruciate Ligament Reconstruction: A Prospective Longitudinal Study. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2018, 26, 3636–3644. [Google Scholar] [CrossRef] [Green Version]
- Curran, M.T.; Lepley, L.K.; Palmieri-Smith, R.M. Continued Improvements in Quadriceps Strength and Biomechanical Symmetry of the Knee After Postoperative Anterior Cruciate Ligament Reconstruction Rehabilitation: Is It Time to Reconsider the 6-Month Return-to-Activity Criteria? J. Athl. Train. 2018, 53, 535–544. [Google Scholar] [CrossRef]
- Meyer, C.A.G.; Gette, P.; Mouton, C.; Seil, R.; Theisen, D. Side-to-Side Asymmetries in Landing Mechanics from a Drop Vertical Jump Test Are Not Related to Asymmetries in Knee Joint Laxity Following Anterior Cruciate Ligament Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2018, 26, 381–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitt, L.C.; Paterno, M.V.; Ford, K.R.; Myer, G.D.; Hewett, T.E. Strength Asymmetry and Landing Mechanics at Return to Sport after Anterior Cruciate Ligament Reconstruction. Med. Sci. Sports Exerc. 2015, 47, 1426–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gokeler, A.; Schmalz, T.; Knopf, E.; Freiwald, J.; Blumentritt, S. The Relationship between Isokinetic Quadriceps Strength and Laxity on Gait Analysis Parameters in Anterior Cruciate Ligament Reconstructed Knees. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2003, 11, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Luc-Harkey, B.A.; Franz, J.R.; Losina, E.; Pietrosimone, B. Association between Kinesiophobia and Walking Gait Characteristics in Physically Active Individuals with Anterior Cruciate Ligament Reconstruction. Gait Posture 2018, 64, 220–225. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| RTR Group (n = 103) | NRTR Group (n = 113) | p | |
|---|---|---|---|
| Age (year) | 24.0 ± 6.0 | 24.9 ± 5.6 | 0.22 |
| Sex (Male/Female) | 74/29 | 82/31 | 0.90 a |
| Body weight (Kg) | 72.8 ± 9.3 | 75.2 ± 9.3 | 0.13 |
| Body Height (cm) | 175.0 ± 8.0 | 176.0 ± 9.0 | 0.31 |
| Sport practice before ACL tear: | 0.25 a | ||
| Soccer | 58 (56.3%) | 58 (51.4%) | |
| Basket | 14 (13.7%) | 18 (15.9%) | |
| Handball | 9 (8.7%) | 8 (7.1%) | |
| Rugby | 11 (10.7%) | 5 (4.4%) | |
| Fighting sport | 2 (1.9%) | 7 (6.2%) | |
| Skiing | 1 (0.9%) | 3 (2.6%) | |
| Others | 8 (7.8%) | 14 (12.4%) | |
| Level of sport practice: | 0.71 a | ||
| Tegner score 5 | 8 (7.8%) | 15 (13.3%) | |
| Tegner score 6 | 15 (14.6%) | 17 (15.1%) | |
| Tegner score 7 | 43 (41.7%) | 46 (40.7%) | |
| Tegner score 8 | 29 (28.1%) | 24 (21.2%) | |
| Tegner score 9 | 6 (5.9%) | 8 (7.1%) | |
| Tegner score 10 | 2 (1.9%) | 3 (2.6%) | |
| Associated Surgery: - | 0.65 a | ||
| -None | 79 (76.6%) | 87 (77.0%) | |
| -Medial meniscus | 14 (13.7%) | 10 (8.9%) | |
| -Lateral meniscus | 7 (6.9%) | 9 (8.0%) | |
| -Both menici | 1 (0.9%) | 2 (1.7%) | |
| Anterolateral tenodesis | 2 (1.9%) | 5 (4.4%) | |
| ACL tear-ACLR delay (months) | 250 ± 391 | 223 ± 344 | 0.58 |
| ACLR-Isokinetic testing delay (days) | 122 ± 16 | 122 ± 17 | 0.68 |
| Lysholm score | 95 ± 8 | 88 ± 9 | <0.001 |
| RTR Group | NRTR Group | p | |
|---|---|---|---|
| (n = 103) | (n = 113) | ||
| Isokinetic LSI | |||
| -Q-LSI at 60°/s | 68.5 ± 10.3 | 50 ± 15.5 | <0.001 |
| -Q-LSI at 180°/s | 76.2 ± 8.5 | 60.7 ± 19.7 | <0.001 |
| -H-LSI at 60°/s | 96.5 ± 12.5 | 85.3 ± 15.8 | <0.001 |
| -H-LSI at 180°/s | 100 ± 13.1 | 91.6 ± 18.0 | <0.001 |
| Isokinetic strength to Body weight | |||
| QS/BW at 60°/s: | |||
| -Surgical limb | 1.90 ± 0.38 | 1.31 ± 0.42 | <0.001 |
| -Uninvolved limb | 2.78 ± 0.39 | 2.64 ± 0.39 | 0.008 |
| QS/BW at 180°/s: | |||
| -Surgical limb | 1.33 ± 0.21 | 1.03 ± 0.29 | <0.001 |
| -Uninvolved limb | 1.50 ± 0.23 | 1.44 ± 0.25 | 0.04 |
| HS/BW at 60°/s: | |||
| -Surgical limb | 1.44 ± 0.24 | 1.22 ± 0.29 | <0.001 |
| -Uninvolved limb | 1.33 ± 0.21 | 1.03 ± 0.29 | <0.001 |
| HS/BW at 180°/s: | |||
| -Surgical limb | 1.10 ± 0.19 | 0.95 ± 0.23 | <0.001 |
| -Uninvolved limb | 1.10 ± 0.20 | 1.05 ± 0.22 | 0.05 |
| Isokinetic strength ratio (%) | |||
| H/Q at 60°/s: | |||
| -Surgical limb | 77.4 ± 14.2 | 101 ± 39.4 | <0.001 |
| -Uninvolved limb | 54.4 ± 5.8 | 54.9 ± 8.5 | 0.58 |
| H/Q at 180°/s: | |||
| -Surgical limb | 83.1 ± 13.2 | 97.6 ± 32.5 | <0.001 |
| -Uninvolved limb | 63.1 ± 9.3 | 60.9 ± 9.6 | 0.1 |
| Knee complications | |||
| -None | 85 (82.5%) * | 51 (45.1) * | <0.001 a |
| -Arthrofibrosis | 3 (2.9%) * | 20 (17.7%) * | |
| -Anterior knee pain | 12 (11.7%) * | 37 (32.7%) * | |
| -Knee effusion | 3 (2.9%) | 5 (4.4%) |
| B | Wald | OR | 95% CIs | p | |
|---|---|---|---|---|---|
| Lysholm | 0.06 | 25 | 1.06 | [1.03–1.08] | <0.001 |
| Knee complications: | |||||
| -Arthrofibrosis | 1.02 | 1.84 | 2.77 | [0.63–12] | 0.17 |
| -Anterior knee pain | −1.38 | 2.09 | 0.25 | [0.03–1.63] | 0.14 |
| -Knee joint swelling | −0.61 | 0.58 | 0.54 | [0.11–2.6] | 0.44 |
| QS/BW at 60°/s: | |||||
| -Surgical limb | 3.6 | 51.9 | 36 | [13.7–97] | <0.001 |
| -Uninvolved limb | 0.93 | 6.8 | 2.5 | [1.2–5.1] | 0.009 |
| QS/BW at 180°/s: | |||||
| -Surgical limb | 4.46 | 41.1 | 87 | [22–340] | <0.001 |
| -Uninvolved limb | 1.13 | 3.99 | 3.09 | [1.02–9.3] | 0.046 |
| HS/BW at 60°/s: | |||||
| -Surgical limb | 3 | 26.5 | 20 | [6.4–62] | <0.001 |
| -Uninvolved limb | 4.46 | 41.1 | 87 | [22–340] | <0.001 |
| HS/BW at 180°/s: | |||||
| -Surgical limb | 3.21 | 20.4 | 25 | [6.1–100] | <0.001 |
| -Uninvolved limb | 1.25 | 3.61 | 3.5 | [0.96–12] | 0.056 |
| Q-LSI at 60°/s | 10.07 | 50.78 | 46390 | [2415–890,872] | <0.001 |
| Q-LSI at 180°/s | 8.75 | 37.38 | 6351 | [383–105,163] | <0.001 |
| H-LSI at 60°/s | 5.69 | 24.66 | 296 | [31–2809] | <0.001 |
| H-LSI at 180°/s | 3.61 | 14.8 | 37 | [5.9–232] | <0.001 |
| H/Q at 60°/s: | |||||
| -Surgical limb | −4.91 | 31.5 | 0.007 | [0.001–0.04] | <0.001 |
| -Uninvolved limb | −0.97 | 0.3 | 0.37 | [0.01–11.9] | 0.58 |
| H/Q at 180°/s: | |||||
| -Surgical limb | −3.46 | 16.3 | 0.031 | [0.006–0.16] | <0.001 |
| -Uninvolved limb | 2.46 | 3.13 | 11.4 | [0.67–204] | 0.1 |
| B | Wald | p | Exp(B) | 95%CIs | |
|---|---|---|---|---|---|
| Lysholm score | 0.074 | 12.6 | 0.001 | 1.07 | 1.03–1.12 |
| Q-LSI at 60°/s | 10.13 | 36.4 | 0.001 | 25,098 | 936–672,590 |
| H-LSI at 60°/s | 3.50 | 5.6 | 0.018 | 33.3 | 1.83–606 |
| Constant | −16.3 | 36.2 |
| ROC Curve Area [95%CI] | Cut-Off [95%CI] | Se | Sp | LR+ | LR− | |
|---|---|---|---|---|---|---|
| Lysholm Score | 0.691 [0.621–0.762] | 97 points [95–98] | 65% | 66% | 1.91 | 0.53 |
| Q-LSI at 60°/s | 0.847 [0.795–0.899] | 0.60 [0.58–0.62] | 77.5% | 77% | 3.39 | 0.29 |
| H-LSI at 60°/s | 0.830 [0.774–0.886] | 0.90 [0.87–0.93] | 65.7% | 61.9% | 1.72 | 0.55 |
| QS/BW at 60°/s | B | Wald | p | Exp(B) | 95%CIs |
|---|---|---|---|---|---|
| Surgical limb | 4.33 | 50.6 | 0.001 | 75.3 | 22–247 |
| Uninvolved limb | −1.33 | 6.9 | 0.008 | 0.25 | 0.09–0.70 |
| Constant | −3.38 | 7.7 |
| QS/BW at 60°/s | ROC Curve Area [95%CI] | Cut-Off (Nm/kg) [95%CI] | Se | Sp | LR+ | LR− |
|---|---|---|---|---|---|---|
| Surgical limb | 0.851 [0.802–0.900] | 1.60 [1.55–1.61] | 74.5% | 73.5% | 2.81 | 0.34 |
| Uninvolved limb | 0.600 [0.525–0.676] | 2.70 [1.65–1.75] | 56.3% | 54.9% | 1.24 | 0.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dauty, M.; Menu, P.; Daley, P.; Grondin, J.; Quinette, Y.; Crenn, V.; Fouasson-Chailloux, A. Knee Strength Assessment and Clinical Evaluation Could Predict Return to Running after Anterior Cruciate Ligament Reconstruction Using Patellar Tendon Procedure. Int. J. Environ. Res. Public Health 2022, 19, 13396. https://doi.org/10.3390/ijerph192013396
Dauty M, Menu P, Daley P, Grondin J, Quinette Y, Crenn V, Fouasson-Chailloux A. Knee Strength Assessment and Clinical Evaluation Could Predict Return to Running after Anterior Cruciate Ligament Reconstruction Using Patellar Tendon Procedure. International Journal of Environmental Research and Public Health. 2022; 19(20):13396. https://doi.org/10.3390/ijerph192013396
Chicago/Turabian StyleDauty, Marc, Pierre Menu, Pauline Daley, Jérôme Grondin, Yonis Quinette, Vincent Crenn, and Alban Fouasson-Chailloux. 2022. "Knee Strength Assessment and Clinical Evaluation Could Predict Return to Running after Anterior Cruciate Ligament Reconstruction Using Patellar Tendon Procedure" International Journal of Environmental Research and Public Health 19, no. 20: 13396. https://doi.org/10.3390/ijerph192013396