
The Age of Mobility: Can Equalization of Public Health Services Alleviate the Poverty of Migrant Workers?

Abstract
:1. Introduction
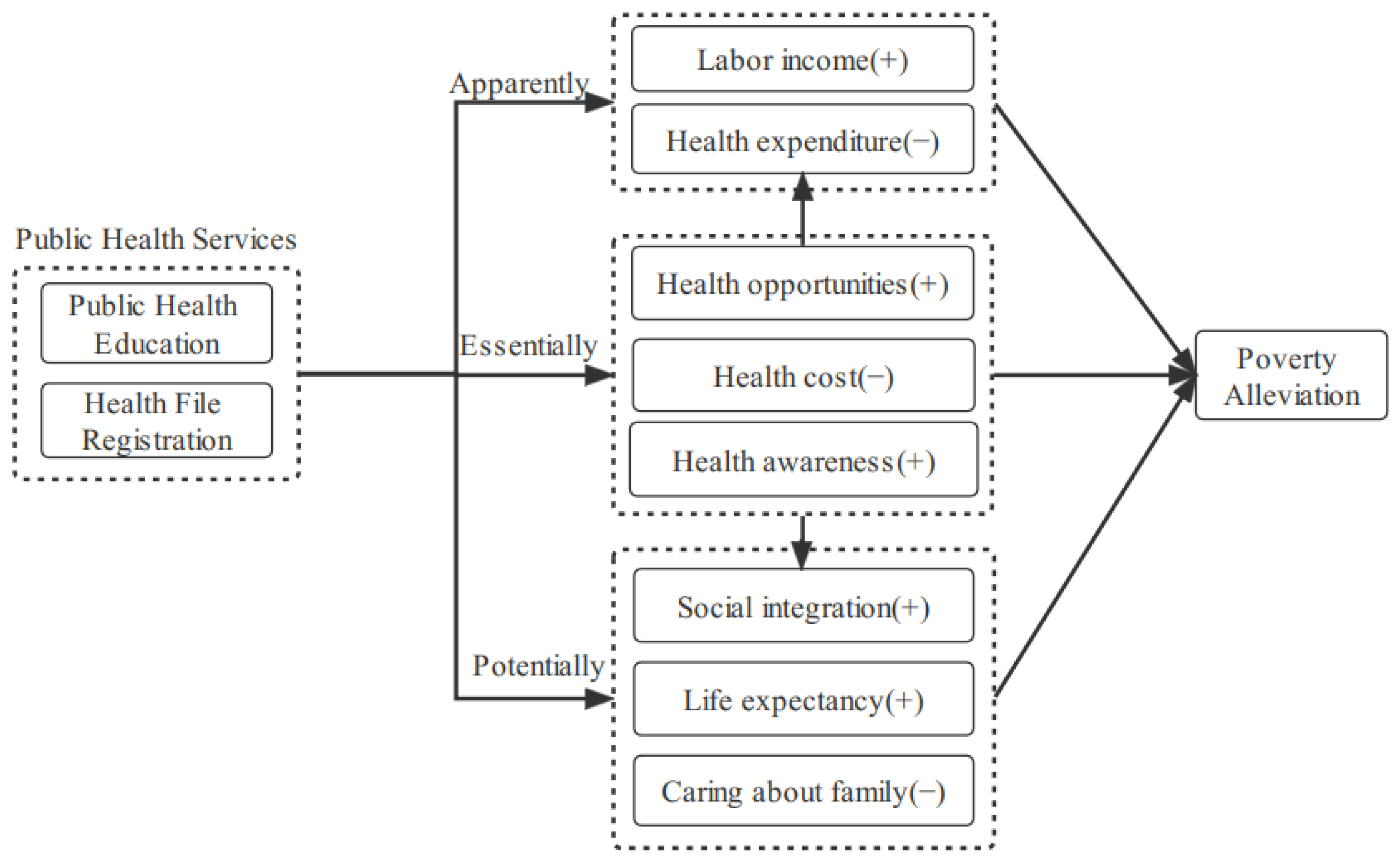
2. Theoretical and Empirical Framework
2.1. The Essential Impact of Public Health Services on Health Poverty
2.2. The Apparent Impact of Public Health Services on Economic Poverty
2.3. The Potential Impact of Public Health Services on Psychological Poverty
3. Materials and Methods
3.1. Research Sample
3.1.1. Data
3.1.2. Variables
3.2. Methods
3.2.1. Benchmark Model
3.2.2. Discussion of Endogenous Problems
4. Estimation Results
4.1. Statistical Analysis
4.2. Benchmark Regression Results
4.3. Endogenous Problems
4.4. Robustness Test
4.4.1. Alleviate the Sample Self-Selection Problem
4.4.2. Use Binary Explanatory Variables
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arouri, M.; Youssef, A.B.; Nguyen, C. Does urbanization reduce rural poverty? Evidence from Vietnam. Econ. Model. 2017, 60, 253–270. [Google Scholar] [CrossRef] [Green Version]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, O.; McKee, M. Public health in the new era: Improving health through collective action. Lancet 2004, 363, 2084–2086. [Google Scholar] [CrossRef]
- Miller, S. Solving the urban dilemma in health care: More poverty, greater demand for public services, reduced financial resources, and fragmentation of services. Bull. N. Y. Acad. Med. 1966, 42, 1150–1156. [Google Scholar]
- Jarrah, S.; Khaldun, J.; Sellers, K.; Rich, N. Bringing the Essential Public Health Services to Life. J. Public Heallth Manag. Pract. 2021, 27, 97–98. [Google Scholar] [CrossRef]
- Tan, X.; Zhang, Y.; Shao, H. Healthy China 2030, a breakthrough for improving health. Glob. Health Promot. 2019, 26, 96–99. [Google Scholar] [CrossRef]
- Chen, S.; Li, J.; Lu, S.; Xiong, B. Escaping from poverty trap: A choice between government transfer payments and public services. Glob. Health Res. Policy 2017, 2, 15. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Mao, Y. Rural resident experience on national basic public health services: A cross-sectional survey in 10 Western provinces of China. Healthcare 2019, 7, 160. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Wu, Q.; Ming, J. The Relationship between Homeownership and the Utilization of Local Public Health Services Among Rural Migrants in China: A Nationwide Cross-Sectional Study. Front. Public Health 2020, 8, 589038. [Google Scholar] [CrossRef]
- Li, Y. Illegal Private Clinics: Ideal Health Services Choices among Rural–Urban Migrants in China? Soc. Work Public Health 2014, 29, 473–480. [Google Scholar] [CrossRef]
- Wang, S. Inching up and socio-economic differentiation: Exploring self-rated health of China’s rural-to-urban migrants from 2005 to 2015. Am. J. Health Behav. 2018, 42, 117–125. [Google Scholar] [CrossRef]
- Wang, S.; Hu, Y. Migration and health in China: Linking sending and host societies. Popul. Space Place. 2019, 25, e2231. [Google Scholar] [CrossRef]
- Zheng, Y.; Ji, Y.; Chang, C.; Liverani, M. The evolution of health policy in China and internal migrants: Continuity, change, and current implementation challenges. Asia Pac. Policy Stud. 2020, 7, 81–94. [Google Scholar] [CrossRef]
- Cioffi, A. Public and private health services: Wait times for health services and the risk of inequality from the Italian perspective. Popul. Health Manag. 2021, 24, 314–315. [Google Scholar] [CrossRef]
- Das Gupta, M.; Dasgupta, R.; Kugananthan, P.; Rao, V.; Somanathan, T.V.; Tewari, K. Flies without borders: Lessons from Chennai on improving India’s municipal public health services. J. Dev. Stud. 2020, 56, 907–928. [Google Scholar] [CrossRef] [Green Version]
- Saksena, P.; Xu, K.; Elovainio, R.; Perrot, J. Health Services Utilization and Out-Of-Pocket Expenditure at Public and Private Facilities in Low-Income Countries. In World Health Report; World Health Organization: Geneva, Switzerland, 2010; Volume 20. [Google Scholar]
- Jiang, Y.; Luo, H.; Yang, F. Influences of migrant construction workers’ environmental risk perception on their physical and mental health: Evidence from china. Int. J. Environ. Res. Public Health 2020, 17, 7424. [Google Scholar] [CrossRef]
- Guo, T.; Tao, C.; Wang, Y. Impacts of Public Medical Services in China on Benefit Incidence and Income Distribution: Micro Evidences Based on the Household Equivalent Scale. J. Coast. Res. 2020, 104, 687–694. [Google Scholar] [CrossRef]
- Benzeval, M.; Judge, K. Income and health: The time dimension. Soc. Sci. Med. 2001, 52, 1371–1390. [Google Scholar] [CrossRef]
- Fogel, R.W. Economic Growth, Population Theory, and Physiology: The Bearing of Long-Term Processes on the Making of Economic Policy; National Bureau of Economic Research: Cambridge, MA, USA, 1994. [Google Scholar] [CrossRef]
- White-Means, S.I. The economic returns from investments in physical and mental health: A case study of migrant farmworkers in rural New York. J. Health Soc. Policy 1991, 2, 39–51. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, Y. The inequality effect of urbanization and social integration. Soc. Sci. China 2016, 37, 117–135. [Google Scholar] [CrossRef]
- Dou, Z.; Cheng, Z.; Huang, D. Research on Migrant Works’ Concern Recognition and Emotion Analysis Based on Web Text Data. Front. Psychol. 2021, 12, 741928. [Google Scholar] [CrossRef]
- Chen, J.; Chen, S.; Landry, P.F.; Davis, D.S. How dynamics of urbanization affect physical and mental health in urban China. China Q. 2014, 220, 988–1011. [Google Scholar] [CrossRef]
- Chen, J.; Wang, W. Economic incentives and settlement intentions of rural migrants: Evidence from China. J. Urban Aff. 2019, 41, 372–389. [Google Scholar] [CrossRef] [Green Version]
- Gebeyaw, G.; Kotecho, M.G.; Adamek, M.E. “Homelessness and Health Problems Are Not Distinct:” The Challenges of Rural-Urban Migrant Homeless Older People in Ethiopia. J. Cross Cult. Gerontol. 2021, 36, 347–368. [Google Scholar] [CrossRef]
- Deng, Z.; Law, Y.W. Rural-to-urban migration, discrimination experience, and health in China: Evidence from propensity score analysis. PLoS ONE 2020, 15, e0244441. [Google Scholar] [CrossRef]
- Pfaff, H.; Pförtner, T. Contribution of health care research to establishing social equality in health and health care op-portunities. Gesundheitswesen (Bundesverband der Arzte des Offentlichen Gesundheitsdienstes (Germany)) 2016, 78, 91–96. [Google Scholar] [CrossRef]
- Liang, J.; Shi, Y.; Osman, M.; Shrestha, B.; Wang, P. The association between social integration and utilization of essential public health services among internal migrants in China: A multilevel logistic analysis. Int. J. Environ. Res. Public Health 2020, 17, 6524. [Google Scholar] [CrossRef]
- Alkire, S.; Foster, J. Understandings and misunderstandings of multidimensional poverty measurement. J. Econ. Inequal. 2011, 9, 289–314. [Google Scholar] [CrossRef] [Green Version]
- Caliendo, M.; Kopeinig, S. Some practical guidance for the implementation of propensity score matching. J. Econ. Surv. 2008, 22, 31–72. [Google Scholar] [CrossRef] [Green Version]
- Staiger, D.O.; Stock, J.H. Instrumental Variables Regression with Weak Instruments; National Bureau of Economic Research: Cambridge, MA, USA, 1994. [Google Scholar] [CrossRef]
- Luo, H.; Yang, H.; Xu, X.; Yun, L.; Chen, R.; Chen, Y.; Xu, L.; Liu, J.; Liu, L.; Liang, H.; et al. Relationship between occupational stress and job burnout among rural-to-urban migrant workers in Dongguan, China: A cross-sectional study. BMJ Open 2016, 6, e012597. [Google Scholar] [CrossRef]
- Lee, J.G.; LePrevost, C.E.; Harwell, E.L.; Bloss, J.E.; Cofie, L.E.; Wiggins, M.F.; Firnhaber, G.C. Coronavirus pandemic highlights critical gaps in rural Internet access for migrant and seasonal farmworkers: A call for partnership with medical libraries. J. Med. Libr. Assoc. 2020, 108, 651. [Google Scholar] [CrossRef]
- Tavora, I.; Rubery, J. Female employment, labour market institutions and gender culture in Portugal. Eur. J. Ind. Relat. 2013, 19, 221–237. [Google Scholar] [CrossRef]
- Lattof, S.R.; Coast, E.; Leone, T. Priorities and challenges accessing health care among female migrants. Health Serv. Insights 2018, 11, 1178632918804825. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.B.; Lu, H.Y. Health investment, gender difference and medical subsidy for floating population. Reform 2014, 10, 65–73. [Google Scholar]
- de Souza Vieira, A.C.; Durand, V. Who uses the public health service? An example from North-East Brazil. Cah. D’études Et De Rech. Francoph. St. 2000, 10, 141–144. [Google Scholar]
- He, W.W.; Hu, X.P. Identity, Belonging and Development: A Study on the Influence of New Generation Migrant Workers’ Willingness to Stay in the City: Based on Research Data from Chongqing City. Rural. Econ. 2017, 8, 122–127. [Google Scholar]
- Zhao, L.; Liu, S.; Zhang, W. New trends in internal migration in China: Profiles of the New-generation migrants. China World Econ. 2018, 26, 18–41. [Google Scholar] [CrossRef]
- Zang, B.; Lv, P.; Warren, C.M. Housing prices, rural–urban migrants’ settlement decisions and their regional differences in China. Habitat Int. 2015, 50, 149–159. [Google Scholar] [CrossRef]
- Bygren, L.O. Egalitarian aspects of medical and social services. J. Public Health Policy 2001, 22, 175–181. [Google Scholar] [CrossRef]
- Spadaro, A.; Mangiavacchi, L.; Moral-Arce, I.; Adiego-Estella, M.; Blanco-Moreno, A. Evaluating the redistributive impact of public health expenditure using an insurance value approach. Eur. J. Health Econ. 2013, 14, 775–787. [Google Scholar] [CrossRef]
- Arthur, E.; Oaikhenan, H.E. The effects of health expenditure on health outcomes in Sub-Saharan Africa (SSA). Afr. Dev. Rev. 2017, 29, 524–536. [Google Scholar] [CrossRef]
- Wang, Y.; Cheng, C.; Bian, Y. More than double jeopardy: An intersectional analysis of persistent income disadvantages of Chinese female migrant workers. Asian J. Women’s Stud. 2018, 24, 246–269. [Google Scholar] [CrossRef]
- Guan, M. Associations between Geodemographic Factors and Access to Public Health Services Among Chinese Floating Population. Front. Public Health 2020, 8, 847. [Google Scholar] [CrossRef] [PubMed]
- Lasarte Navamuel, E.; Fernández Vázquez, E.; Rubiera Morollón, F. Higher cost of living in urban areas? An AIDS-based analysis of food in Spain. Reg. Stud. 2017, 51, 1665–1677. [Google Scholar] [CrossRef]
- Zheng, L.; Hu, R.; Dong, Z.; Hao, Y. Comparing the needs and utilization of health services between urban residents and rural-to-urban migrants in China from 2012 to 2016. BMC Health Serv. Res. 2018, 18, 717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, W.; Chu, C.; Wang, K.; Meng, Y.; Yang, Y.; Mao, A. Collaboration and Cooperation of Public Health Service Management in China. Disaster Med. Public Health Prep. 2021, 15, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Guo, Q.; Meng, Y. The health service use of aged rural-to-urban migrant workers in different types of cities in China. BMC Health Serv. Res. 2021, 21, 606. [Google Scholar] [CrossRef]
- Aragón, M. City and Welfare: The Tension between Urbanization & Settlement. Revista Costarricense de Psicología 2020, 39, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Aslund, O.; Fredriksson, P. Peer effects in welfare dependence quasi-experimental evidence. J. Hum. Resour. 2009, 44, 798–825. [Google Scholar] [CrossRef]


{kind=link}
| Dimension | Indicator | Explanation | Weight |
|---|---|---|---|
| Economy | Eco1: Difficulties with low income in current residence | Yes = 1; No = 0; | 1/15 |
| Eco2: Difficulties in finding a stable job in the current residence | Yes = 1; No = 0; | 1/15 | |
| Eco3: Difficulties in doing business in the current residence | Yes = 1; No = 0; | 1/15 | |
| Healthy | Hel: Your self-assessment of your physical health in the current residence | Healthy =0; Others =1; | 1/5 |
| Social Integration | Int1: Do you have any difficulties in your current residence that you are not used to? | Yes = 1; No = 0; | 1/10 |
| Int2: Do you think the locals are unwilling to accept you? | Yes = 1; No = 0; | 1/10 | |
| Life Expectancy | Exp1: Difficulties in not being able to buy a house in the current residence | Yes = 1; No = 0; | 1/10 |
| Exp 2: Difficulties with children enrolling in the current residence | Yes = 1; No = 0; | 1/10 | |
| Caring about Family | Care1: Difficulties in supporting the elderly in the hometown | Yes = 1; No = 0; | 1/15 |
| Care2: Difficulties in caring for children in the hometown | Yes = 1; No = 0; | 1/15 | |
| Care3: Difficulties in spouse loneliness in the hometown | Yes = 1; No = 0; | 1/15 |
| Variable Name | Definition | Mean | SE | Min | Max |
|---|---|---|---|---|---|
| Explained variable (dimension) | |||||
| PDL | Poverty deprivation levels of migrant workers | 0.1806 | 0.1833 | 0 | 0.9333 |
| Economy | Poverty level of migrant workers’ economic dimension | 0.2685 | 0.3430 | 0 | 1 |
| Healthy | Poverty level of migrant workers’ health dimension | 0.1564 | 0.3632 | 0 | 1 |
| Social integration | Poverty level of migrant workers’ social integration dimension | 0.0687 | 0.1832 | 0 | 1 |
| Life expectancy | Poverty level of migrant workers’ future development dimension | 0.2711 | 0.3501 | 0 | 1 |
| Family concern | Poverty level of migrant workers’ family concern dimension | 0.1381 | 0.2196 | 0 | 1 |
| Core explanatory variables | |||||
| Public health education | Number who received public health education | 3.5358 | 3.3707 | 0 | 9 |
| Health file registration | Not established = 0, established = 1 | 0.2578 | 0.4375 | 0 | 1 |
| Human capital characteristics | |||||
| Gender | Female = 0, male = 1 | 0.5940 | 0.4911 | 0 | 1 |
| Age | Age of respondent in 2017 | 35.7808 | 9.8497 | 15 | 79 |
| Age2 | Age × Age/100 | 13.7728 | 7.6126 | 2.25 | 62.41 |
| Marriage | Unmarried = 0; married = 1 | 0.7964 | 0.4027 | 0 | 1 |
| Education | Have not attended school = 0; elementary or junior high school = 1; high school = 2; university and above = 3 | 1.4800 | 0.7598 | 0 | 3 |
| Party | CCP member = 1; others = 0 | 0.0384 | 0.1921 | 0 | 1 |
| Ethnicity | Han nationality = 1; others = 0 | 0.9188 | 0.2731 | 0 | 1 |
| Stability | Stable = 1; unstable = 0; | 0.1727 | 0.3780 | 0 | 1 |
| Family characteristics | |||||
| Family size | Family population | 3.0326 | 1.2166 | 1 | 10 |
| Social capital | Participation in activities such as trade unions, associations, classmate get-togethers, and fellow villagers’ associations | 0.7469 | 1.0196 | 0 | 6 |
| Regional characteristics | |||||
| lnGDP | Logarithmic value of provincial GDP in 2017 | 10.3574 | 0.8058 | 7.3450 | 11.5124 |
| Capital city | Provincial capital city = 1; nonprovincial capital city = 0 | 0.4725 | 0.4992 | 0 | 1 |
| Urban | Town = 1; countryside = 2 | 1.3409 | 0.4740 | 1 | 2 |
| Variables | Explained Variable: PDL | |||
|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |
| Public health education | −0.0013 *** | −0.0014 *** | ||
| (0.0002) | (0.0002) | |||
| Health file registration | −0.0150 *** | −0.0162 *** | ||
| (0.0017) | (0.0017) | |||
| Gender | −0.0078 *** | −0.0079 *** | ||
| (0.0016) | (0.0016) | |||
| Age | 0.0076 *** | 0.0076 *** | ||
| (0.0006) | (0.0006) | |||
| Age2 | −0.0071 *** | −0.0070 *** | ||
| (0.0007) | (0.0007) | |||
| Marriage | 0.0095 *** | 0.0100 *** | ||
| (0.0025) | (0.0025) | |||
| Education | −0.0136 *** | −0.0136 *** | ||
| (0.0011) | (0.0011) | |||
| Party | −0.0016 | −0.0014 | ||
| (0.0039) | (0.0039) | |||
| Ethnicity | −0.0329 *** | −0.0318 *** | ||
| (0.0029) | (0.0029) | |||
| Family size | 0.0190 *** | 0.0189 *** | ||
| (0.0008) | (0.0008) | |||
| Social capital | 0.0008 | 0.0007 | ||
| (0.0008) | (0.0008) | |||
| Stability | −0.0035 * | −0.0037 * | ||
| (0.0021) | (0.0021) | |||
| LnGDP | −0.0056 *** | −0.0053 *** | ||
| (0.0010) | (0.0010) | |||
| Capital city | 0.0053 *** | 0.0049 *** | ||
| (0.0016) | (0.0016) | |||
| Urban | −0.0173 *** | −0.0172 *** | ||
| (0.0017) | (0.0017) | |||
| Cons | 0.2333 *** | 0.2328 *** | 0.1106 *** | 0.1072 *** |
| (0.0036) | (0.0036) | (0.0153) | (0.0153) | |
| Industry FE | YES | YES | YES | YES |
| Outflow areas FE | YES | YES | YES | YES |
| N | 53,857 | 53,857 | 53,857 | 53,857 |
| R2 | 0.0303 | 0.0310 | 0.0906 | 0.0914 |
| Variables | First Stage | Second Stage | First Stage | Second Stage |
|---|---|---|---|---|
| (1) Public Health Education | (2) PDL | (3) Health File Registration | (4) PDL | |
| IV1: Community public health attention | 0.0734 *** | —— | 0.0082 *** | —— |
| IV2: Policy cognition of migrant workers | 2.3217 *** | —— | 0.3457 *** | —— |
| Public health education | —— | −0.0084 *** (0.0007) | —— | —— |
| Health file registration | —— | —— | —— | −0.0566 *** (0.0046) |
| Human capital characteristics | YES | YES | YES | YES |
| Family characteristics | YES | YES | YES | YES |
| Regional characteristics | YES | YES | YES | YES |
| Industry FE | YES | YES | YES | YES |
| Outflow areas FE | YES | YES | YES | YES |
| First stage F value | 722.31 *** | —— | 601.84 *** | —— |
| Over-identification test p-value | —— | 0.5901 | —— | 0.7667 |
| N | 53,153 | 53,153 | 53,153 | 53,153 |
| R2 | 0.2136 | 0.0760 | 0.1874 | 0.0829 |
| Variable Name | ATT | Standard Error | t Test Value | |
|---|---|---|---|---|
| Public health education | At least 1 public health education | −0.0042 * | 0.0025 | −1.6900 |
| At least 5 public health education | −0.0190 *** | 0.0022 | −8.7400 | |
| Occupational disease prevention education | −0.0321 *** | 0.0021 | −15.0400 | |
| Emergency public service education | −0.0149 *** | 0.0021 | −6.9800 | |
| Health file registration | −0.0212 *** | 0.0022 | −9.4600 | |
| Explained Variable | Poverty Status | Difficult Status | ||
|---|---|---|---|---|
| Public health education | −0.0482 *** | −0.0474 *** | ||
| (0.0060) | (0.0049) | |||
| Health file registration | −0.3230 *** (0.0405) | −0.3195 *** (0.0333) | ||
| Human capital characteristics | YES | YES | YES | YES |
| Family characteristics | YES | YES | YES | YES |
| Regional characteristics | YES | YES | YES | YES |
| Industry FE | YES | YES | YES | YES |
| Outflow areas FE | YES | YES | YES | YES |
| N | 53,153 | 53,153 | 53,153 | 53,153 |
| Explained Variable PDL | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| Male Sample | Female Sample | |||
| Public health education | −0.0079 *** (0.0009) | —— | −0.0090 *** (0.0011) | —— |
| Health file registration | —— | −0.0526 *** (0.0060) | —— | −0.0607 *** (0.0072) |
| Human capital characteristics | Yes | Yes | Yes | Yes |
| Family characteristics | Yes | Yes | Yes | Yes |
| Regional characteristics | Yes | Yes | Yes | Yes |
| Industry FE | Yes | Yes | Yes | Yes |
| Outflow areas FE | Yes | Yes | Yes | Yes |
| N | 31,573 | 31,573 | 21,580 | 21,580 |
| R2 | 0.0719 | 0.0795 | 0.0845 | 0.0904 |
| Explained Variable PDL | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| New Generation Samples | Old Generation Sample | |||
| Public health education | −0.0084 *** (0.0009) | —— | −0.0082 *** (0.0011) | —— |
| Health file registration | —— | −0.0571 *** (0.0058) | —— | −0.0543 *** (0.0074) |
| Human capital characteristics | Yes | Yes | Yes | Yes |
| Family characteristics | Yes | Yes | Yes | Yes |
| Regional characteristics | Yes | Yes | Yes | Yes |
| Industry FE | Yes | Yes | Yes | Yes |
| Outflow areas FE | Yes | Yes | Yes | Yes |
| N | 31,954 | 31,954 | 21,199 | 21,199 |
| R2 | 0.0655 | 0.0723 | 0.0314 | 0.0389 |
| Explained Variable: PDL | (1) | (2) | (3) | (4) | (5) | (6) |
|---|---|---|---|---|---|---|
| Eastern Sample | Central Sample | Western Sample | ||||
| Public health education | −0.0086 *** (0.0010) | —— | −0.0047 *** (0.0014) | —— | −0.0140 *** (0.0015) | —— |
| Health file registration | —— | −0.0595 *** (0.0067) | —— | −0.0291 *** (0.0086) | —— | −0.0927 *** (0.0096) |
| Human capital characteristics | Yes | Yes | Yes | Yes | Yes | Yes |
| Family characteristics | Yes | Yes | Yes | Yes | Yes | Yes |
| Regional characteristics | Yes | Yes | Yes | Yes | Yes | Yes |
| Industry FE | Yes | Yes | Yes | Yes | Yes | Yes |
| Outflow areas FE | Yes | Yes | Yes | Yes | Yes | Yes |
| N | 26,596 | 26,596 | 12,214 | 12,214 | 14,343 | 14,343 |
| R2 | 0.0672 | 0.0736 | 0.0848 | 0.0880 | 0.0919 | 0.0975 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Z.; Jiang, Y.; Wu, H.; Jiang, F.; Yu, Z. The Age of Mobility: Can Equalization of Public Health Services Alleviate the Poverty of Migrant Workers? Int. J. Environ. Res. Public Health 2022, 19, 13342. https://doi.org/10.3390/ijerph192013342
Zhou Z, Jiang Y, Wu H, Jiang F, Yu Z. The Age of Mobility: Can Equalization of Public Health Services Alleviate the Poverty of Migrant Workers? International Journal of Environmental Research and Public Health. 2022; 19(20):13342. https://doi.org/10.3390/ijerph192013342
Chicago/Turabian StyleZhou, Ziming, Yumeng Jiang, Haitao Wu, Fan Jiang, and Zhiming Yu. 2022. "The Age of Mobility: Can Equalization of Public Health Services Alleviate the Poverty of Migrant Workers?" International Journal of Environmental Research and Public Health 19, no. 20: 13342. https://doi.org/10.3390/ijerph192013342