
Re-Starting the Cruise Sector during the COVID-19 Pandemic in Greece: Assessing Effectiveness of Port Contingency Planning

 and
and
Abstract
:1. Introduction
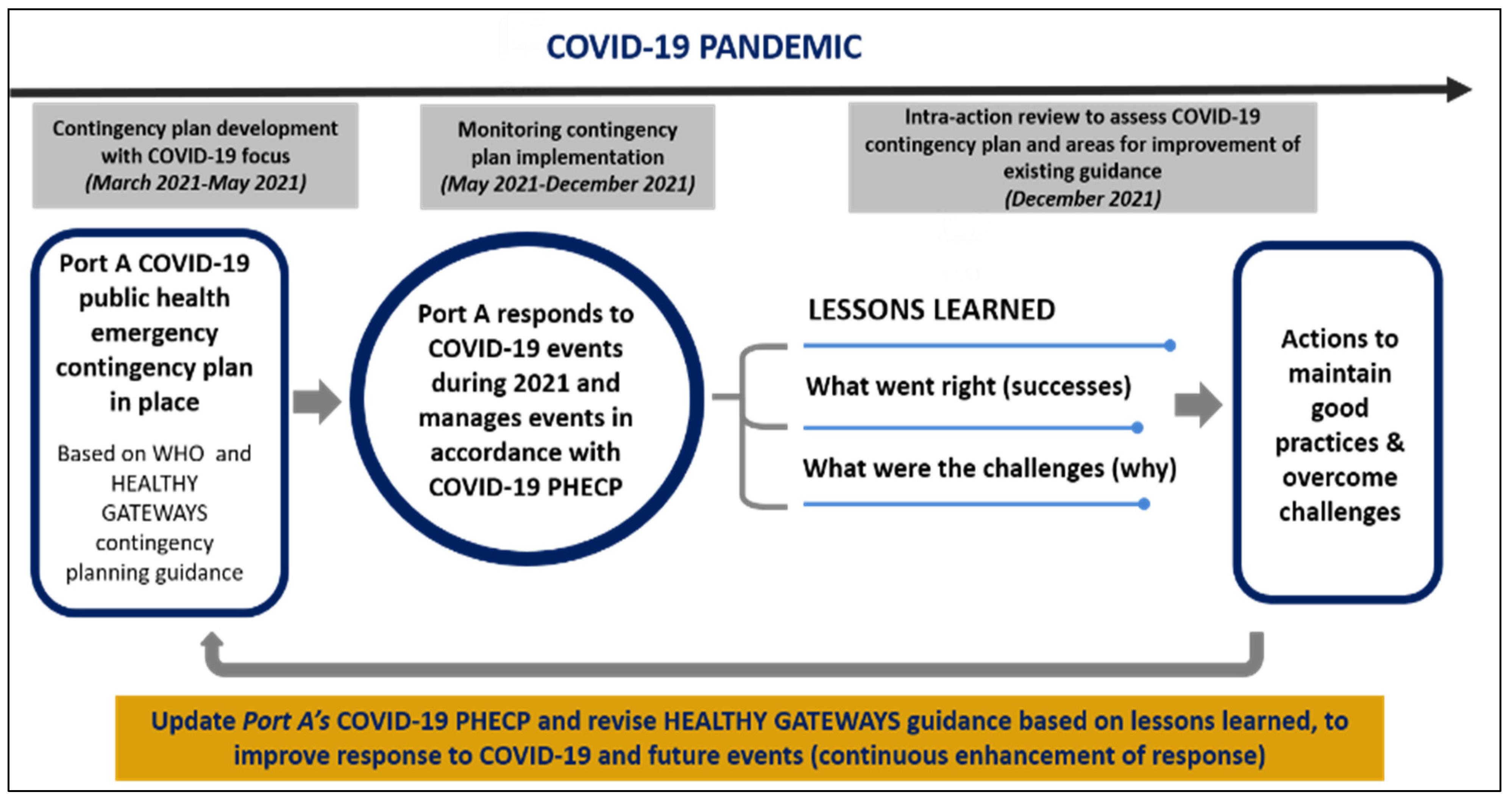
2. Materials and Methods
2.1. Revision of “Initial COVID-19” Port Public Health Emergency Contingency Plan
2.2. Monitoring Implementation of the Revised COVID-19 PHECP during 2021 Cruises
2.3. Conducting a Local Level Intra-Action Review at Port A during the COVID-19 Pandemic
3. Results
3.1. Revision of Port A’s “Initial COVID-19” Plan and Integration of Novel COVID-19 Components

{kind=link}
{kind=link}
| Gaps Identified in “Initial COVID-19” Plan | Elements Included in Port A’s Revised COVID-19 PHECP | Element Description | Added Value for Preparedness Planning | Element Addressed in Existing European HEALTHY GATEWAYS Guidance |
|---|---|---|---|---|
| Phased activation of “pre-pandemic” plan | Formal alert phases for activating PHECP and Task Force | Alert phases color-coded by public health risk level. Each phase associated with specific scenarios and response actions | Defines specific conditions for:
| Addressed in existing guidance |
| Documented procedures for managing COVID-19 events | Standard Operating Procedures (SOPs) | SOPs for COVID-19 management (cases detected on board or at port) from notification, to management of cases, contacts and health measures implementation | Describes for each involved stakeholder step-by-step procedures, promoting coordinated and timely event response | Addressed in existing guidance |
| Documented procedures for internal and external information exchange/communication | Communication plan for: (a) routine operations in COVID-19 context; (b) COVID-19 event management |
| Supports operational communication in both routine circumstances and COVID-19 event management, to promote coordinated responses from internal and external stakeholders | Addressed in existing guidance |
| Interoperability of port’s and cruise ships’ COVID-19 response plans | Monitoring framework for alignment of ships’ COVID-19 PHECP with Port A’s PHECP | Table recording for each ship call:
|
| New method to monitor interoperability—will be incorporated in future version of guidance |
| Identification of responsible authorities for COVID-19 event management | Roles and responsibilities for preparedness and response |
|
| Partially addressed in existing guidance—will be revised in future version to include tasks for monitoring public health capacities |
| Framework to define and monitor local and country level public health response capacities for COVID-19 event management | Templates defining maximum public health capacities | Templates documenting maximum capacities available for:
|
| Capacity templates will be incorporated in future version of guidance |
| Templates monitoring current public health capacities against pre-defined maximum | Monitoring template includes:
|
| Monitoring templates will be incorporated in future version of guidance | |
| Defining local capacities for diagnostic laboratory testing (SARS-CoV-2) | Pre-identification of reliable shore-side laboratories | List of reliable shore-side laboratories performing reverse transcription—polymerase chain reaction (RT-PCR):
|
| Partially addressed in existing guidance—future version of guidance to advise that port PHECP should include written agreements with reliable shore-side laboratories |
| Understanding isolation and quarantine facility requirements for home port calls | Predicted shore-side isolation and quarantine facility requirements during routine and “worst case” scenarios |
|
| Templates will be incorporated in future version of guidance |
| Determining capacities to facilitate repatriations, crew changes etc. | Awareness of local/regional airport/airline operations |
|
| Addressed in existing guidance |
| Documented agreement of all stakeholders regarding their role in PHECP | Memorandum of Understanding (MoU) among stakeholders |
|
| Addressed in existing guidance |
3.2. Implementation of Port A’s Revised COVID-19 Public Health Emergency Contingency Plan
3.3. Results from Port A’s Intra-Action Review to Analyze COVID-19 Event Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mouchtouri, V.A.; Dirksen-Fischer, M.; Hadjichristodoulou, C. Health measures to travellers and cruise ships in response to COVID-19. J. Travel Med. 2020, 27, taaa043. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). International Health Regulations (2005), 3rd ed.; WHO Library Cataloguing-in-Publication Data: Geneva, Switzerland, 2016. [Google Scholar]
- Hatzianastasiou, S.; Mouchtouri, V.A.; Pavli, A.; Tseroni, M.; Sapounas, S.; Vasileiou, C.; Dadouli, K.; Kyritsi, M.; Koureas, M.; Prezerakos, P.; et al. COVID-19 Outbreak on a Passenger Ship and Assessment of Response Measures, Greece, 2020. Emerg. Infect. Dis. 2021, 27, 1927–1930. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, E.; Ino, H.; Akabayashi, A. Chronology of COVID-19 Cases on the Diamond Princess Cruise Ship and Ethical Considerations: A Report From Japan. Disaster Med. Public Health Prep. 2020, 14, 506–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocklöv, J.; Sjödin, H.; Wilder-Smith, A. COVID-19 outbreak on the Diamond Princess cruise ship: Estimating the epidemic potential and effectiveness of public health countermeasures. J. Travel Med. 2020, 27, taaa030. [Google Scholar] [CrossRef] [Green Version]
- Anan, H.; Kondo, H.; Takeuchi, I.; Nakamori, T.; Ikeda, Y.; Akasaka, O.; Koido, Y. Medical Transport for 769 COVID-19 Patients on a Cruise Ship by Japan Disaster Medical Assistance Team. Disaster Med. Public Health Prep. 2020, 14, e47–e50. [Google Scholar] [CrossRef]
- Kordsmeyer, A.-C.; Mojtahedzadeh, N.; Heidrich, J.; Militzer, K.; von Münster, T.; Belz, L.; Jensen, H.-J.; Bakir, S.; Henning, E.; Heuser, J.; et al. Systematic Review on Outbreaks of SARS-CoV-2 on Cruise, Navy and Cargo Ships. Int. J. Environ. Res. Public Health 2021, 18, 5195. [Google Scholar] [CrossRef]
- Choquet, A.; Sam-Lefebvre, A. Ports closed to cruise ships in the context of COVID-19: What choices are there for coastal states? Ann. Tour. Res. 2021, 86, 103066. [Google Scholar] [CrossRef]
- Cruise Lines International Association (CLIA). Cruise Industry COVID-19 Facts and Resources. Available online: https://cruising.org/en-gb/cruise-industry-covid-19-facts-and-resources (accessed on 8 March 2022).
- World Health Organization (WHO). Operational Considerations for Managing COVID-19 Cases or Outbreaks on Board Ships (Interim Guidance). Available online: https://www.who.int/publications/i/item/operational-considerations-for-managing-covid-19-cases-or-outbreaks-on-board-ships-interim-guidance (accessed on 28 December 2021).
- Eu Healthy Gateways Joint Action. Advice for Cruise Ship Operators for Preparedness and Response to an Outbreak of COVID-19. Version 4. April 2021. Available online: https://www.healthygateways.eu/ (accessed on 28 August 2021).
- Eu Healthy Gateways Joint Action. Advice for Restarting Cruise Ship Operations after Lifting Restrictive Measures in Response to the COVID-19 Pandemic. Version 2. April 2021. Available online: https://www.healthygateways.eu/ (accessed on 28 August 2021).
- Eu Healthy Gateways Joint Action. Tool for Public Health Contingency Plan Development and Assessment for Ports (Milestone 7.9–Deliverable 7.2). Version 1. 19 February 2021. Available online: https://www.healthygateways.eu/Tool-for-contingency-plan-development-and-assessment-for-ports (accessed on 28 December 2021).
- Houser, R.S. Intra Action Reviews as a New Tool in Public Health Emergency Management and Pandemic Response: A Summary of Uses and Applications, 2020–2021. Disaster Med. Public Health Prep. 2022, 1–3. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Emergency Response Reviews. Available online: https://www.who.int/emergencies/operations/emergency-response-reviews (accessed on 20 September 2022).
- World Health Organization (WHO). Guidance for Conducting a Country COVID-19 Intra-Action Review (IAR). Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Country_IAR-2020.1 (accessed on 28 December 2021).
- European Centre for Disease Prevention and Control (ECDC). Conducting in-Action and After-Action Reviews of the Public Health Response to COVID-19. Available online: https://www.ecdc.europa.eu/en/publications-data/conducting-action-and-after-action-reviews-public-health-response-covid-19 (accessed on 28 December 2021).
- Bank of Greece. Developments in the Balance of Travel Services: 2020 (27 April 2021—Press Releases). Available online: https://www.bankofgreece.gr/en/news-and-media/press-office/news-list/news?announcement=670af725-5fcf-4805-8947-583c99fb161e (accessed on 28 December 2021).
- European Maritime Safety Agency (EMSA) and European Centre for Disease Prevention and Control (ECDC). COVID-19: EU Guidance for Cruise Ship Operations—Revision 1. Available online: https://www.ecdc.europa.eu/en/publications-data/COVID-19-cruise-ship-guidance (accessed on 8 January 2022).
- Papadakis, A.; (University of Crete, Rethymnon, Greece). Personal communication, 2021.
- Port, A. Emergency response plan/contingency plan for management of single or multiple possible or confirmed SARS-CoV-2 cases on passengers ships (cruise ships) at Port A, Protocol number 200118. Hellenic Republic, Region of Crete. 2020; (unpublished work, confidential). [Google Scholar]
- Hellenic Republic—Ministry of Health. General Directorate of Public Health & Quality of Life, Directorate of Public Health & Environmental Hygiene. Circular: Basic Health Requirements of the Country’s Ports of Entry for Preparedness and Response against SARS-CoV-2. 05 May 2021-Δ1α/Γ.Π.οικ.28690. Available online: https://www.ynanp.gr/media/documents/2021/05/13/%CE%A9%CE%9D%CE%A1%CE%94465%CE%A6%CE%A5%CE%9F-%CE%9F5%CE%A7_1.pdf (accessed on 30 May 2021).
- World Health Organization (WHO). International Health Regulations (2005): A Guide For Public Health Emergency Contingency Planning at Designated Points of Entry; WHO Library Cataloguing in Publication Data: Geneva, Switzerland, 2012. [Google Scholar]
- Eu Healthy Gateways Joint Action. EU Common Ship Sanitation Database. Available online: https://sis.shipsan.eu/ (accessed on 25 August 2022).
- European Centre for Disease Prevention and Control (ECDC). Case Definition for Coronavirus Disease 2019 (COVID-19), as of 29 May 2020. Available online: https://www.ecdc.europa.eu/en/covid-19/surveillance/case-definition (accessed on 3 June 2020).
- Eu Healthy Gateways Joint Action; Laboratory of Hygiene and Epidemiology, Medical Faculty: Larisa, Greece, 2022; manuscript in preparation.
- Alene, M.; Yismaw, L.; Assemie, M.A.; Ketema, D.B.; Gietaneh, W.; Birhan, T.Y. Serial interval and incubation period of COVID-19: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 257. [Google Scholar] [CrossRef]
- Rai, B.; Shukla, A.; Dwivedi, L.K. Estimates of serial interval for COVID-19: A systematic review and meta-analysis. Clin. Epidemiol. Glob. Health 2021, 9, 157–161. [Google Scholar] [CrossRef]
- McAloon, C.G.; Wall, P.; Griffin, J.; Casey, M.; Barber, A.; Codd, M.; Gormley, E.; Butler, F.; McV Messam, L.L.; Walsh, C.; et al. Estimation of the serial interval and proportion of pre-symptomatic transmission events of COVID− 19 in Ireland using contact tracing data. BMC Public Health 2021, 21, 805. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.-J.; Wang, Z.-X.; Xu, Y.; Hu, M.-X.; Chen, K.; Qin, G. Assessment of basic reproductive number for COVID-19 at global level: A meta-analysis. Medicine 2021, 100, e25837. [Google Scholar] [CrossRef] [PubMed]
- Ke, R.; Romero-Severson, E.; Sanche, S.; Hengartner, N. Estimating the reproductive number R(0) of SARS-CoV-2 in the United States and eight European countries and implications for vaccination. J. Theor. Biol. 2021, 517, 110621. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Xiao, J.; Deng, A.; Zhang, Y.; Zhuang, Y.; Hu, T.; Li, J.; Tu, H.; Li, B.; Zhou, Y.; et al. Notes from the Field: Transmission Dynamics of an Outbreak of the COVID-19 Delta Variant B.1.617.2—Guangdong Province, China, May–June 2021. China CDC Weekly 2021, 3, 584–586. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). One-Day in-Action Review (IAR) Protocol in the Context of COVID-19. Available online: https://www.ecdc.europa.eu/en/publications-data/one-day-action-review-iar-protocol-context-covid-19] (accessed on 28 December 2021).
- World Health Organization (WHO). AAR Toolkits. Available online: https://www.who.int/publications/m/item/aar-toolkits (accessed on 28 December 2021).
- European Centre for Disease Prevention and Control (ECDC). Case Definition for Coronavirus Disease 2019 (COVID-19), as of 3 December 2020. Available online: https://www.ecdc.europa.eu/en/covid-19/surveillance/case-definition (accessed on 25 August 2022).
- World Health Organization (WHO). Intra-Action Review (IAR). Available online: https://extranet.who.int/sph/intra-action-review (accessed on 20 August 2022).
- The First Intra-Action Review of Indonesia’s Response to the COVID-19 Pandemic, August 2020. Health Security 2021, 19, 521–531. [CrossRef]
- Talisuna, A.; Iwu, C.; Okeibunor, J.; Stephen, M.; Musa, E.O.; Herring, B.L.; Ramadan, O.P.C.; Yota, D.; Nanyunja, M.; Mpairwe, A.; et al. Assessment of COVID-19 pandemic responses in African countries: Thematic synthesis of WHO intra-action review reports. BMJ Open 2022, 12, e056896. [Google Scholar] [CrossRef]
- Schöll, M.; Seidel, J.; Boldt, M.; Czerwonka, H.; Ehlkes, L.; Frühsammer, L.; Ippisch, S.; Rexroth, U.; an der Heiden, M. In(tra)-Action Review (IAR): COVID-19-Management an IGV-benannten Flughäfen in Deutschland, September 2020 bis Mai 2021. Epidemiol. Bull. 2022, 23, 3–11. [Google Scholar] [CrossRef]
- Hoang, N.V.; Hoang, N.-A.; Pham Quang, T.; Quach, H.-L.; Nguyen, K.C.; Vu, L.N.; Hoang, D.M.; Field, E.; Vogt, F. Evaluating Epidemic Preparedness and Response to COVID-19: A Nation-Wide Multisectorial Intra-Action Review of the Points of Entry Surveillance System in Vietnam, January to September 2020. Asia Pac. J. Public Health 2022, 34, 10105395221112863. [Google Scholar] [CrossRef]
- Eu Healthy Gateways Joint Action: Preparedness and Action at Points of Entry (Ports, Airports, Ground Crossings). (Grant Agreement Nr. 801493). Available online: https://www.healthygateways.eu/ (accessed on 20 August 2022).
- de Rooij, D.; van de Watering, M.; van Dijk, R.; Appels, R.; Veenstra, T.; Swaan, C.; Timen, A. Experience with in-action reviewing at points of entry. Eur. J. Public Health 2021, 31, 658. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Organisation mondiale de la, S. Operationalizing COVID-19 intra-action reviews—preliminary findings—Mise en œuvre opérationnelle des examens de l’action en cours pour la COVID-19—résultats préliminaire. Wkly. Epidemiol. Rec. Relev. Épidémiologique Hebd. 2021, 96, xliii–xlvi. [Google Scholar]
- Klein, A.; Heuser, J.; Henning, E.; Sprössel, N.; Kordsmeyer, A.-C.; Oldenburg, M.; Mojtahedzadeh, N.; Heidrich, J.; Militzer, K.C.; Belz, L.; et al. A mass casualty incident of infectious diseases at the port of Hamburg: An analysis of organizational structures and emergency concepts. J. Occup. Med. Toxicol. 2021, 16, 36. [Google Scholar] [CrossRef] [PubMed]
- Martin, G.; Boland, M. Planning and preparing for public health threats at airports. Glob. Health 2018, 14, 28. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Joint External Evaluation Tool: International Health Regulations (2005), 3rd ed.; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- The International Academic Forum. Toward Safe and Healthy Trans-border Cruises: International Challenges for Building Resilient and Trusted Ships and Ports Report (Concise Version). Available online: https://www.mofa.go.jp/files/100184031.pdf (accessed on 4 April 2022).
- Mouchtouri, V.A.; Westacott, S.; Nichols, G.; Riemer, T.; Skipp, M.; Bartlett, C.L.R.; Kremastinou, J.; Hadjichristodoulou, C.; SHIPSAN partnership. Hygiene inspections on passenger ships in Europe—An overview. BMC Public Health 2010, 10, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mouchtouri, V.A.; Van Reusel, D.; Bitsolas, N.; Katsioulis, A.; Van den Bogaert, R.; Helewaut, B.; Steenhout, I.; Damman, D.; Dávila Cornejo, M.; Hadjichristodoulou, C.; et al. European Web-Based Platform for Recording International Health Regulations Ship Sanitation Certificates: Results and Perspectives. Int. J. Environ. Res. Public Health 2018, 15, 1833. [Google Scholar] [CrossRef] [Green Version]
- Moriarty, L.F.; Plucinski, M.M.; Marston, B.J.; Kurbatova, E.V.; Knust, B.; Murray, E.L.; Pesik, N.; Rose, D.; Fitter, D.; Kobayashi, M.; et al. Public Health Responses to COVID-19 Outbreaks on Cruise Ships—Worldwide, February-March 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 347–352. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Emergency Situational Updates. Weekly Operational Update on COVID-19. 31 May 2021. Available online: https://www.who.int/publications/m/item/weekly-operational-update-on-covid-19-31-may-2021 (accessed on 20 August 2022).
- Anagnostopoulos, L.; Kourentis, L.; Dávila-Cornejo, M.; Moreno-Lorente, I.; Dionisio, M.; Marotta, C.; Hadjichristodoulou, C.; Mouchtouri, V.A. Using the intra-action review methodology at European level to assess effectiveness of measures for cruise ship operations in the COVID-19 context. Medical Sciences Forum. In Proceedings of the Public Health Congress on Maritime Transport and Ports 2022: Sailing to the Post-COVID-19 Era, Athens, Greece, 21–22 October 2022. [Google Scholar]
- Yamahata, Y.; Shibata, A. Preparation for Quarantine on the Cruise Ship Diamond Princess in Japan due to COVID-19. JMIR Public Health Surveill. 2020, 6, e18821. [Google Scholar] [CrossRef]
- Jimi, H.; Hashimoto, G. Challenges of COVID-19 outbreak on the cruise ship Diamond Princess docked at Yokohama, Japan: A real-world story. Glob. Health Med. 2020, 2, 63–65. [Google Scholar] [CrossRef] [PubMed]


| Date of Call (Month/Year) | Cruise Ship | Total Number of Passengers | Passengers at Arrival | Number of COVID-19 Cases 2 | Number of Close Contacts 3 | Port A’s Designated Role in Itinerary |
|---|---|---|---|---|---|---|
| 05/2021 | Cruise ship A | 1971 | 949 | 1 | 5 | Home port |
| 05/2021 | Cruise ship A | 2313 | 1316 | 2 | 2 | Home port |
| 08/2021 | Cruise ship B | 155 | 88 | 1 | 1 | Transit port |
| 09/2021 | Cruise ship C | 408 | 403 | 1 | 1 | Transit port |
| 09/2021 | Cruise ship D | 1335 | 1335 | 1 | 0 | Transit port |
| 10/2021 | Cruise ship E | 457 | 455 | 2 | 2 | Transit port |
| 10/2021 | Cruise ship A | 2284 | 1258 | 3 | 0 | Home port |
| 10/2021 | Cruise ship D | 1278 | 1278 | 1 | 1 | Transit port |
| 11/2021 | Cruise ship F | 1135 | 1134 | 1 | 1 | Transit port |
| 11/2021 | Cruise ship G | 117 | 115 | 1 | 0 | Transit port |
| Event Number | Cruise Ship Name | Illness | Number of Cases | Passenger or Crew | Symptom Status | Disembarkation Location | Number of Close Contacts 2 | Number of Crew | Number of Passengers |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Cruise ship A | COVID-19 | 1 | Passenger | Symptomatic | Port A | 5 | 745 | 958 |
| 2 | Cruise ship A | COVID-19 | 1 | Passenger | Symptomatic | Port A | 1 | 750 | 1316 |
| Cruise ship A | COVID-19 | 1 | Passenger | Symptomatic | Port A | 1 | 750 | 1316 | |
| 3 | Cruise ship B | COVID-19 | 1 | Passenger | Symptomatic | Port A | 1 | Not known | Not known |
| 4 | Cruise ship D | COVID-19 | 1 | Crew member | Symptomatic | No disembarkation | Not known | Not known | Not known |
| 5 | Cruise ship D | COVID-19 | 1 | Crew member | Asymptomatic | No disembarkation | 1 | Not known | Not known |
| 6 | Cruise ship A | COVID-19 | 1 | Passenger | Symptomatic | No disembarkation | 0 | 789 | 1258 |
| Cruise ship A | COVID-19 | 1 | Passenger | Symptomatic | No disembarkation | 0 | 789 | 1258 | |
| Cruise ship A | COVID-19 | 1 | Passenger | Symptomatic | No disembarkation | 0 | 789 | 1258 | |
| 7 | Cruise ship F | COVID-19 | 1 | Passenger | Symptomatic | Port A | 1 | Not known | Not known |
| 8 | Cruise ship G | COVID-19 | 1 | Passenger | Asymptomatic | No disembarkation | Not known | 444 | 115 |
| 9 | Cruise ship C | COVID-19 | 1 | Not known | Not known | Not known | 1 | Not known | Not known |
| 10 | Cruise ship E | COVID-19 | 2 | Not known | Not known | Not known | 2 | Not known | Not known |
| Challenges, Successes, and Recommendations to Improve COVID-19 Response | Description of Findings |
|---|---|
| Challenges: | Port A designated as transit port but functioned as home port for public health event management, due to inability of other contingency ports to deal with events 1,2,3 |
| Other ports of call in cruise itinerary within the country lacked preparedness plans and capacities for COVID-19 event management 3 | |
| Considered less feasible for cruise ship with event on board to return to home port for event management 1,2 | |
| Limited/no communication with next port of call in non-European country 1 | |
| Lack of formal communication channels between cruise ports of European and non-European countries 1 | |
| Cruise operator possibly unfamiliar with response plans in non-European country, or anticipated non-European port may implement different/more rigid COVID-19 response measures 1 | |
| Lack of coordinated and common standards for COVID-19 event management between cruise ports of European and non-European countries 1 | |
| Health measures (disembarkation, shore-side isolation/quarantine) at Port A implemented before verification of diagnostic test results 2 | |
| Limited alternatives and time to verify diagnostic test results in shore-side laboratory before cruise ship arrival at Port A and implementation of health measures 2 | |
| Verification of diagnostic test results revealed all COVID-19 cases false positive, but travelers characterized as COVID-19 cases in national case registry database 2 | |
| Difficulties in declassifying false positive cases in the national case registry database, in order for travelers to continue their voyage 2 | |
| Diagnostic testing conducted on board cruise ship cannot be recorded in national case registry, thus false positives cannot be declassified using test results conducted on board 2 | |
| Health measures recommended by Port A authorities were not implemented by the cruise ship after leaving European waters for next port of call in non-European country 2 | |
| On the tourist-based island, designated “COVID-19” hotels for isolation/quarantine facilities do not operate in winter season, meanwhile Port A continues to receive cruise calls during winter 4 | |
| Good practices: | Port A communicated directly with cruise ship and requested verification of event before decision-making 1 |
| Port A conducted risk assessment before managing COVID-19 event as a transit port, considering: current port and local public health capacity levels; risk that event presents to port; feasibility of ship returning to home port 1,2,3 | |
| Port A’s PHECP included list of reliable shore-side laboratories with capacity for RT-PCR, to verify unexpected diagnostic test results 2 | |
| Joint Ministerial Decision passed at national level, defining process to declassify COVID-19 cases in the national case registry database, defining situations where declassification is permitted 2 | |
| In situations where state designated COVID-19 hotels are available for ashore isolation/quarantine, local public health authority insists cases/close contacts are accommodated there, rather than other options (e.g., AirBnB), since designated facilities have capacity to monitor health measures implementation 4 | |
| Additional revisions proposed for Port A’s COVID-19 PHECP: | Port A will conduct risk assessment in situations when designated as transit port and requested to respond as home/contingency port for non-emergency situations. If results of risk assessment determine that required capacities exist for the duration needed and it is feasible, Port A can activate their PHECP for event management, while informing national authorities and the home port 1,3 |
| Port A communication plan to consider that competent port authority will communicate directly with next port of call in non-European country, informing about COVID-19 event and health measures recommended (via email or telephone) until formal communication channels for information exchange established 1 | |
| Describe process for risk assessment prior to health measures implementation when number of COVID-19 cases exceeds expected/probable. Requires verification of diagnostic test results, either retesting via RT-PCR on board or at reliable shore-side laboratory 2 Define situations where reclassification of COVID-19 cases may be required, and procedures for Port A to initiate reclassification 2 | |
| Proposed revisions to EU HEALTHY GATEWAYS guidance: | Describe specific considerations for managing non-emergency COVID-19 events as a transit port and define risk assessment procedures considering: current port capacities; current public health capacities; risk COVID-19 event presents to travelers on board, at port facility and to local port community; other relevant factors 1,3 |
| Contingency planning guidance to include considerations for verification of diagnostic test results (defining risk assessment process) 2 | |
| Contingency planning guidance to include cooperation/written agreements with “reliable” shore-side laboratories (if possible accredited and/or certified) 2 | |
| Contingency planning guidance to describe scenarios for re-classification of incorrect diagnostic test results in national case registries 2 | |
| In certain situations if it is confirmed that no state-designated shore-side isolation/quarantine facilities are available and cruise operators have not arranged other facilities, consider that COVID-19 case may have to remain on board until next port of call, emphasizing preference to disembark case for public health reasons 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anagnostopoulos, L.; Kourentis, L.; Papadakis, A.; Mouchtouri, V.A. Re-Starting the Cruise Sector during the COVID-19 Pandemic in Greece: Assessing Effectiveness of Port Contingency Planning. Int. J. Environ. Res. Public Health 2022, 19, 13262. https://doi.org/10.3390/ijerph192013262
Anagnostopoulos L, Kourentis L, Papadakis A, Mouchtouri VA. Re-Starting the Cruise Sector during the COVID-19 Pandemic in Greece: Assessing Effectiveness of Port Contingency Planning. International Journal of Environmental Research and Public Health. 2022; 19(20):13262. https://doi.org/10.3390/ijerph192013262
Chicago/Turabian StyleAnagnostopoulos, Lemonia, Leonidas Kourentis, Antonios Papadakis, and Varvara A. Mouchtouri. 2022. "Re-Starting the Cruise Sector during the COVID-19 Pandemic in Greece: Assessing Effectiveness of Port Contingency Planning" International Journal of Environmental Research and Public Health 19, no. 20: 13262. https://doi.org/10.3390/ijerph192013262