
Prenatal Co-Exposure to Manganese, Mercury, and Lead, and Neurodevelopment in Children during the First Year of Life
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
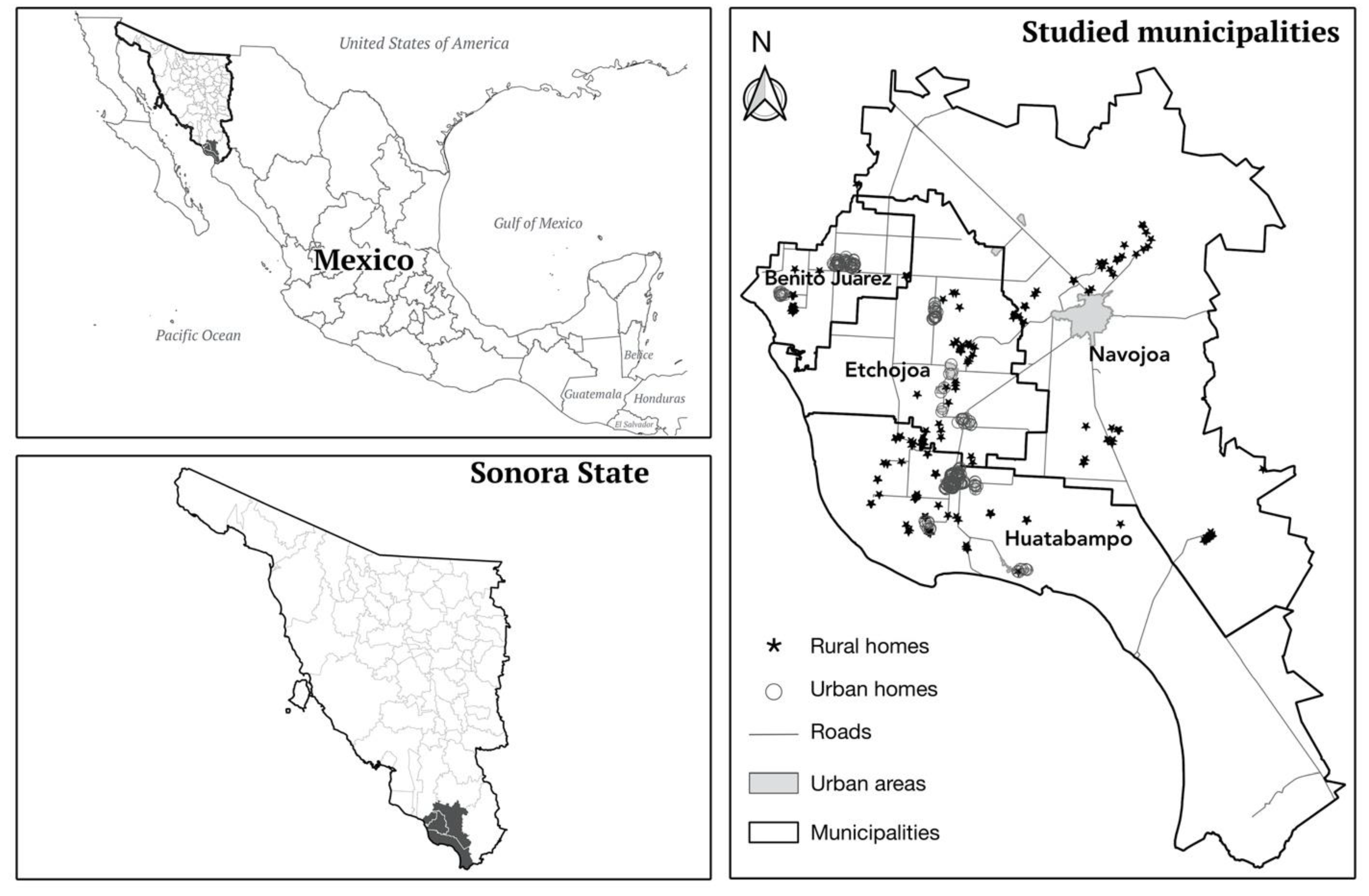
2.1. Study Design and Population
2.2. Sociodemographic and Infant Development Data
2.2.1. Questionnaire and Anthropometrics
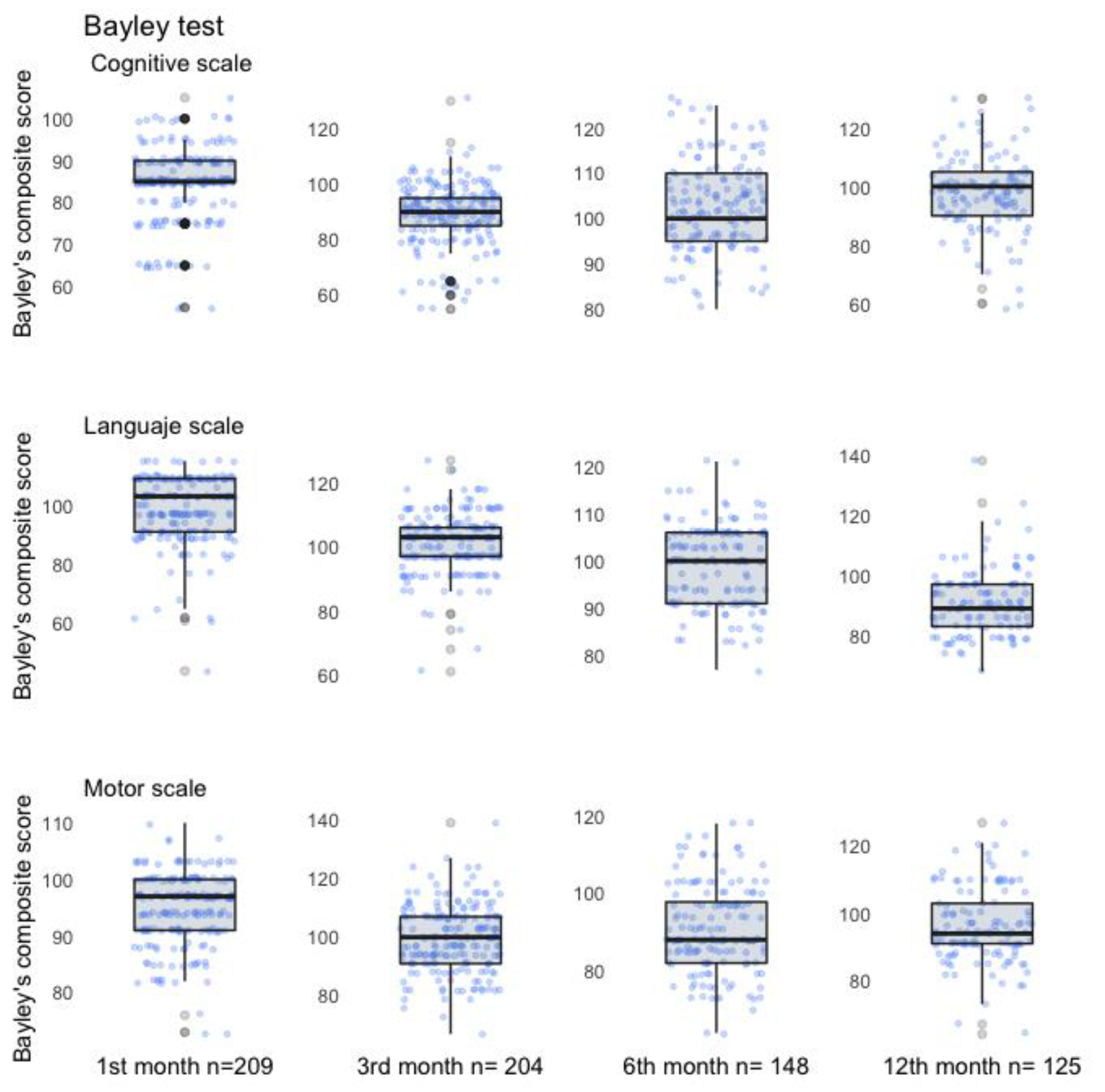
2.2.2. Neurodevelopment Assessment
2.3. Sample Collection
Blood Lead, Manganese, and Mercury Determination
2.4. Statistical Analysis
2.5. Spatial Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tau, G.Z.; Peterson, B.S. Normal Development of Brain Circuits. Neuropsychopharmacology 2010, 35, 147–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Needham, L.L.; Grandjean, P.; Heinzow, B.; Jørgensen, P.J.; Nielsen, F.; Patterson, D.G.; Sjödin, A.; Turner, W.E.; Weihe, P. Partition of Environmental Chemicals between Maternal and Fetal Blood and Tissues. Environ. Sci. Technol. 2011, 45, 1121–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, W.; Aschner, M.; Ghersi-Egea, J.-F. Brain Barrier Systems: A New Frontier in Metal Neurotoxicological Research. Toxicol. Appl. Pharmacol. 2003, 192, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Grandjean, P.; Landrigan, P.J. Neurobehavioural Effects of Developmental Toxicity. Lancet Neurol. 2014, 13, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Goyer, R.A. Transplacental Transport of Lead. Environ. Health Perspect. 1990, 89, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Nandakumaran, M.; Al-Sannan, B.; Al-Sarraf, H.; Al-Shammari, M. Maternal-Fetal Transport Kinetics of Manganese in Perfused Human Placental Lobule in Vitro. J. Matern. Neonatal Med. 2016, 29, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Gundacker, C.; Hengstschläger, M. The Role of the Placenta in Fetal Exposure to Heavy Metals. Wien. Med. Wochenschr. 2012, 162, 201–206. [Google Scholar] [CrossRef]
- WHO. 10 Chemicals of Public Health Concern. Available online: https://www.who.int/news-room/photo-story/photo-story-detail/10-chemicals-of-public-health-concern (accessed on 4 April 2022).
- Liu, X.; Zhang, Y.; Piao, J.; Mao, D.; Li, Y.; Li, W.; Yang, L.; Yang, X. Reference Values of 14 Serum Trace Elements for Pregnant Chinese Women: A Cross-Sectional Study in the China Nutrition and Health Survey 2010–2012. Nutrients 2017, 9, 309. [Google Scholar] [CrossRef] [Green Version]
- Miguel, P.M.; Pereira, L.O.; Silveira, P.P.; Meaney, M.J. Early Environmental Influences on the Development of Children’s Brain Structure and Function. Dev. Med. Child Neurol. 2019, 61, 1127–1133. [Google Scholar] [CrossRef]
- National Toxicology Program Health Effects of Low-Level Lead; NTP Monograph, 1st ed.; NIH Publication: Bethesda, MD, USA, 2012; Volume 5996, ISBN 2330-1279.
- Bose-O’Reilly, S.; McCarty, K.M.; Steckling, N.; Lettmeier, B. Mercury Exposure and Children’s Health. Curr. Probl. Pediatr. Adolesc. Health Care 2010, 40, 186–215. [Google Scholar] [CrossRef]
- Balachandran, R.C.; Mukhopadhyay, S.; McBride, D.; Veevers, J.; Harrison, F.E.; Aschner, M.; Haynes, E.N.; Bowman, A.B. Brain Manganese and the Balance between Essential Roles and Neurotoxicity. J. Biol. Chem. 2020, 295, 6312–6329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guilarte, T.R. Manganese Neurotoxicity: New Perspectives from Behavioral, Neuroimaging, and Neuropathological Studies in Humans and Non-Human Primates. Front. Aging Neurosci. 2013, 5, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.; Bornhorst, J.; Aschner, M. Manganese Metabolism in Humans. Front. Biosci. 2018, 23, 1655–1679. [Google Scholar] [CrossRef] [Green Version]
- Laborde, A.; Tomasina, F.; Bianchi, F.; Bruné, M.-N.; Buka, I.; Comba, P.; Corra, L.; Cori, L.; Duffert, C.M.; Harari, R.; et al. Children’s Health in Latin America: The Influence of Environmental Exposures. Environ. Health Perspect. 2015, 123, 201–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claus Henn, B.; Coull, B.A.; Wright, R.O. Chemical Mixtures and Children’s Health. Curr. Opin. Pediatr. 2014, 26, 223–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dufault, R.J.; Wolle, M.M.; Kingston, H.M.S.; Gilbert, S.G.; Murray, J.A. Connecting Inorganic Mercury and Lead Measurements in Blood to Dietary Sources of Exposure That May Impact Child Development. World J. Methodol. 2021, 11, 144–159. [Google Scholar] [CrossRef] [PubMed]
- Carmona, A.; Roudeau, S.; Ortega, R. Molecular Mechanisms of Environmental Metal Neurotoxicity: A Focus on the Interactions of Metals with Synapse Structure and Function. Toxics 2021, 9, 198. [Google Scholar] [CrossRef]
- Sanders, A.P.; Claus Henn, B.; Wright, R.O. Perinatal and Childhood Exposure to Cadmium, Manganese, and Metal Mixtures and Effects on Cognition and Behavior: A Review of Recent Literature. Curr. Environ. Health Rep. 2015, 2, 284–294. [Google Scholar] [CrossRef] [Green Version]
- Stanwood, G.D.; Leitch, D.B.; Savchenko, V.; Wu, J.; Fitsanakis, V.A.; Anderson, D.J.; Stankowski, J.N.; Aschner, M.; McLaughlin, B. Manganese Exposure Is Cytotoxic and Alters Dopaminergic and GABAergic Neurons within the Basal Ganglia. J. Neurochem. 2009, 110, 378–389. [Google Scholar] [CrossRef] [Green Version]
- Loreto-Gómez, C.; Farías, P.; Moreno-Macías, H.; Romano-Riquer, S.P.; Riojas-Rodríguez, H. Anogenital Distance: A Longitudinal Evaluation of Its Variants and Indices in Boys and Girls of Sonora, Mexico. Reprod. Toxicol. 2017, 73, 167–174. [Google Scholar] [CrossRef]
- Wechsler Abbreviated Scale of Intelligence--Second Edition–PsycNET. Available online: https://psycnet.apa.org/doiLanding?doi=10.1037%2Ft15171-000 (accessed on 4 April 2022).
- Bayley, N. Bayley Scales of Infant and Toddler Development|Third Edition. Available online: https://www.pearsonassessments.com/store/usassessments/en/Store/Professional-Assessments/Behavior/Adaptive/Bayley-Scales-of-Infant-and-Toddler-Development-%7C-Third-Edition/p/100000123.html (accessed on 5 April 2022).
- Weiss, L.G.; Oakland, T.; Aylward, G.P. Bayley-III Clinical Use and Interpretation; Academic Press: Cambridge, MA, USA, 2010; ISBN 978-0-08-092107-5. [Google Scholar]
- Sergio Montes Biomarkers of Manganese Exposure in a Population Living Close to a Mine and Mineral Processing Plant in Mexico. Environ. Res. 2008, 106, 89–95. [CrossRef] [PubMed]
- Ilmiawati, C.; Yoshida, T.; Itoh, T.; Nakagi, Y.; Saijo, Y.; Sugioka, Y.; Sakamoto, M.; Ikegami, A.; Ogawa, M.; Kayama, F. Biomonitoring of Mercury, Cadmium, and Lead Exposure in Japanese Children: A Cross-Sectional Study. Environ. Health Prev. Med. 2015, 20, 18–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- StataCorp. Stata Statistical Software: Release 13, StataCorp LP: College Station, TX, USA, 2013.
- ArcGis ArcGIS Resource Center. Available online: https://resources.arcgis.com/es/help/getting-started/articles/026n00000012000000.htm (accessed on 12 July 2022).
- INEGI Marco Geoestadístico. Available online: https://www.inegi.org.mx/temas/mg/ (accessed on 12 July 2022).
- Budtz-Jørgensen, E.; Bellinger, D.; Lanphear, B.; Grandjean, P. An International Pooled Analysis for Obtaining a Benchmark Dose for Environmental Lead Exposure in Children. Risk Anal. 2013, 33, 450–461. [Google Scholar] [CrossRef]
- DOF-Diario Oficial de La Federación. Available online: https://www.dof.gob.mx/nota_detalle.php?codigo=5495551&fecha=30/08/2017 (accessed on 4 April 2022).
- Tellez-Rojo, M.M.; Bautista-Arredondo, L.F.; Trejo-Valdivia, B.; Tamayo-Ortiz, M.; Sánchez, D.E.; Kraiem, R.; Pantic, I.; Mercado-García, A.; Romero-Martínez, M.; Shamah-Levy, T.; et al. Análisis de la distribución nacional de intoxicación por plomo en niños de 1 a 4 años. Implicaciones para la política pública en México. Salud Pública De México 2020, 62, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Henn, B.C.; Austin, C.; Coull, B.A.; Schnaas, L.; Gennings, C.; Horton, M.K.; Hernández-Ávila, M.; Hu, H.; Tellez-Rojo, M.M.; Wright, R.O.; et al. Uncovering Neurodevelopmental Windows of Susceptibility to Manganese Exposure Using Dentine Microspatial Analyses. Environ. Res. 2018, 161, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Guan, H.; Wang, M.; Li, X.; Piao, F.; Li, Q.; Xu, L.; Kitamura, F.; Yokoyama, K. Manganese Concentrations in Maternal and Umbilical Cord Blood: Related to Birth Size and Environmental Factors. Eur. J. Public Health 2014, 24, 150–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.; Chakraborty, S.; Mukhopadhyay, S.; Lee, E.; Paoliello, M.M.B.; Bowman, A.B.; Aschner, M. Manganese Homeostasis in the Nervous System. J. Neurochem. 2015, 134, 601–610. [Google Scholar] [CrossRef] [Green Version]
- DOF Diario Oficial de La Federación. Available online: https://www.dof.gob.mx/nota_detalle.php?codigo=2063863&fecha=22/11/2000 (accessed on 4 April 2022).
- Chung, S.E.; Cheong, H.-K.; Ha, E.-H.; Kim, B.-N.; Ha, M.; Kim, Y.; Hong, Y.-C.; Park, H.; Oh, S.-Y. Maternal Blood Manganese and Early Neurodevelopment: The Mothers and Children’s Environmental Health (MOCEH) Study. Environ. Health Perspect. 2015, 123, 717–722. [Google Scholar] [CrossRef] [Green Version]
- Henn, B.C.; Schnaas, L.; Ettinger, A.S.; Schwartz, J.; Lamadrid-Figueroa, H.; Hernández-Avila, M.; Amarasiriwardena, C.; Hu, H.; Bellinger David, C.; Wright Robert, O.; et al. Associations of Early Childhood Manganese and Lead Coexposure with Neurodevelopment. Environ. Health Perspect. 2012, 120, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.-C.; Chen, Y.-C.; Su, F.-C.; Lin, C.-M.; Liao, H.-F.; Hwang, Y.-H.; Hsieh, W.-S.; Jeng, S.-F.; Su, Y.-N.; Chen, P.-C. In Utero Exposure to Environmental Lead and Manganese and Neurodevelopment at 2 Years of Age. Environ. Res. 2013, 123, 52–57. [Google Scholar] [CrossRef]
- Peraza, M.A.; Ayala-Fierro, F.; Barber, D.S.; Casarez, E.; Rael, L.T. Effects of Micronutrients on Metal Toxicity. Environ. Health Perspect. 1998, 106, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Stern, A.H.; Smith, A.E. An Assessment of the Cord Blood:Maternal Blood Methylmercury Ratio: Implications for Risk Assessment. Environ. Health Perspect. 2003, 111, 1465–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Research Council (US) Committee on the Toxicological Effects of Methylmercury. Toxicological Effects of Methylmercury. National Academies Press: Washington, DC, USA, 2000; ISBN 978-0-309-07140-6. [Google Scholar]
- Starling, P.; Charlton, K.; McMahon, A.T.; Lucas, C. Fish Intake during Pregnancy and Foetal Neurodevelopment—A Systematic Review of the Evidence. Nutrients 2015, 7, 2001–2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Khoury, J.C.; Sucharew, H.; Dietrich, K.; Yolton, K. Low-Level Gestational Exposure to Mercury and Maternal Fish Consumption: Associations with Neurobehavior in Early Infancy. Neurotoxicol. Teratol. 2016, 54, 61–67. [Google Scholar] [CrossRef]
- Shah-Kulkarni, S.; Lee, S.; Jeong, K.S.; Hong, Y.-C.; Park, H.; Ha, M.; Kim, Y.; Ha, E.-H. Prenatal Exposure to Mixtures of Heavy Metals and Neurodevelopment in Infants at 6 Months. Environ. Res. 2020, 182, 109122. [Google Scholar] [CrossRef]
- Bauer, J.A.; Fruh, V.; Howe, C.G.; White, R.F.; Henn, B.C. Associations of Metals and Neurodevelopment: A Review of Recent Evidence on Susceptibility Factors. Curr. Epidemiol. Rep. 2020, 7, 237–262. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | All a | Complete Information b | Incomplete Information c | p-Value |
|---|---|---|---|---|
| Q50 (Q25–Q75) | Q50 (Q25–Q75) | Q50 (Q25–Q75) | ||
| Mother | ||||
| Blood Pb (µg/L) | 7.60 (5.00–14.30) | 7.80 (5.65–14.70) | 7.55 (4.60–14.25) | 0.83 |
| Blood Hg (µg/L) | 1.93 (1.34–2.77) | 1.79 (1.25–2.35) | 2.01 (13.40–2.80) | 0.49 |
| Blood Mn (µg/L) | 9.92 (7.65–12.45) | 9.07 (7.51–11.80) | 10.15 (7.56–12.95) | 0.22 |
| Age (years) | 23 (20–27) | 21 (19–26) | 23 (20–27) | 0.09 |
| IQ score (points) | 73 (64- 84) | 78 (68–93) | 72 (64–83) | 0.05 |
| Pre-pregnancy BMI | 26.34 (23.12–29.07) | 28.24 (24.34–31.25) | 26.10 (23.05–28.46) | 0.05 |
| Offspring | ||||
| Birth weight (kg) | 3.40 (3.15–3.70) | 3.40 (3.20–3.75) | 3.40 (3.10–3.67) | 0.77 |
| Birth length (cm) | 53.00 (51.00–55.00) | 54.00 (52.00–55.00) | 53.00 (51.00–55.00) | 0.30 |
| Head circumference (cm) | 36 (35.00–36.70) | 35.50 (34.20–36.50) | 36.00 (35.00–36.70) | 0.25 |
| Vaginal Birth (%) | 71.3 | 65.9 | 72.5 | 0.38 |
| Female sex (%) | 47.9 | 47.3 | 48.1 | 0.91 |
| Metals (µg/L) | Bayley Scales | ||
|---|---|---|---|
| Language | Motor | Cognitive | |
| ß (CI 95%) | ß (CI 95%) | ß (CI 95%) | |
| n = 522 | |||
| Hg b | −0.51 (−1.43–0.41) | 0.04 (−0.89–0.97) | −0.25 (−1.16–0.67) |
| Pb c | −0.15 (−0.24–−0.56) ** | −0.08 (−0.17–0.01) | −0.01 (−0.10–0.08) |
| n = 252 | |||
| Pb only in women with Hg >1.9 b | −0.16 (−0.29–−0.34) ** | −0.08 (−0.20–0.04) | −0.03 (−0.15–0.09) |
| n = 247 | |||
| Pb only in women with Mn <9.6 b | −0.19 (−0.31–−0.06) ** | −0.01 (−0.02–0.02) | −0.08 (−0.02–0.04) |
| Mn b | n = 364 | ||
| 1st tertile (2.40–6.86) | −1.21 (−3.71–1.30) | −1.02 (−3.55–1.52) | 0.21 (−2.16–2.58) |
| 2nd tertile (6.87–12.80) | Ref. | Ref. | Ref. |
| 3rd tertile (12.9–21.30) | −1.95 (−4.30–0.40) | −1.20 (−3.58–1.17) | −1.25 (−3.48–0.97) |
| Metals (µg/L) | Bayley Scales | ||
|---|---|---|---|
| Language | Motor | Cognitive | |
| ß (CI 95%) | ß (CI 95%) | ß (CI 95%) | |
| Pb | −0.35 (−0.12–0.52) | −1.06 (−1.95–−0.17) ** | −0.13 (−0.97–0.70) |
| Hg | 0.07 (−4.73–4.86) | −2.79 (−7.70–2.11) | 0.68 (−3.98–5.34) |
| Mn | −0.30 (−1.32–0.73) | −0.82 (−1.87–0.22) | 0.09 (−0.90–1.08) |
| Pb # Hg | 0.04 (−0.32–0.39) | 0.38 (0.02–0.75) * | 0.03 (−0.32–0.37) |
| Pb # Mn | 0.03 (−0.05–0.11) | 0.09 (0.01–0.18) * | 0.004 (−0.74–0.83) |
| Hg # Mn | 0.006 (−0.44–0.45) | 0.29 (−0.17–0.75) | −0.11 (−0.31–0.33) |
| Pb # Hg # Mn | 0.007 (−0.04–0.03) | −0.04 (−0.07–−0.003) * | 0.0008 (−0.03–0.03) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farías, P.; Hernández-Bonilla, D.; Moreno-Macías, H.; Montes-López, S.; Schnaas, L.; Texcalac-Sangrador, J.L.; Ríos, C.; Riojas-Rodríguez, H. Prenatal Co-Exposure to Manganese, Mercury, and Lead, and Neurodevelopment in Children during the First Year of Life. Int. J. Environ. Res. Public Health 2022, 19, 13020. https://doi.org/10.3390/ijerph192013020
Farías P, Hernández-Bonilla D, Moreno-Macías H, Montes-López S, Schnaas L, Texcalac-Sangrador JL, Ríos C, Riojas-Rodríguez H. Prenatal Co-Exposure to Manganese, Mercury, and Lead, and Neurodevelopment in Children during the First Year of Life. International Journal of Environmental Research and Public Health. 2022; 19(20):13020. https://doi.org/10.3390/ijerph192013020
Chicago/Turabian StyleFarías, Paulina, David Hernández-Bonilla, Hortensia Moreno-Macías, Sergio Montes-López, Lourdes Schnaas, José Luis Texcalac-Sangrador, Camilo Ríos, and Horacio Riojas-Rodríguez. 2022. "Prenatal Co-Exposure to Manganese, Mercury, and Lead, and Neurodevelopment in Children during the First Year of Life" International Journal of Environmental Research and Public Health 19, no. 20: 13020. https://doi.org/10.3390/ijerph192013020