
Lifestyle Interventions through Participatory Research: A Mixed-Methods Systematic Review of Alcohol and Other Breast Cancer Behavioural Risk Factors


Abstract
:1. Introduction
2. Materials and Methods
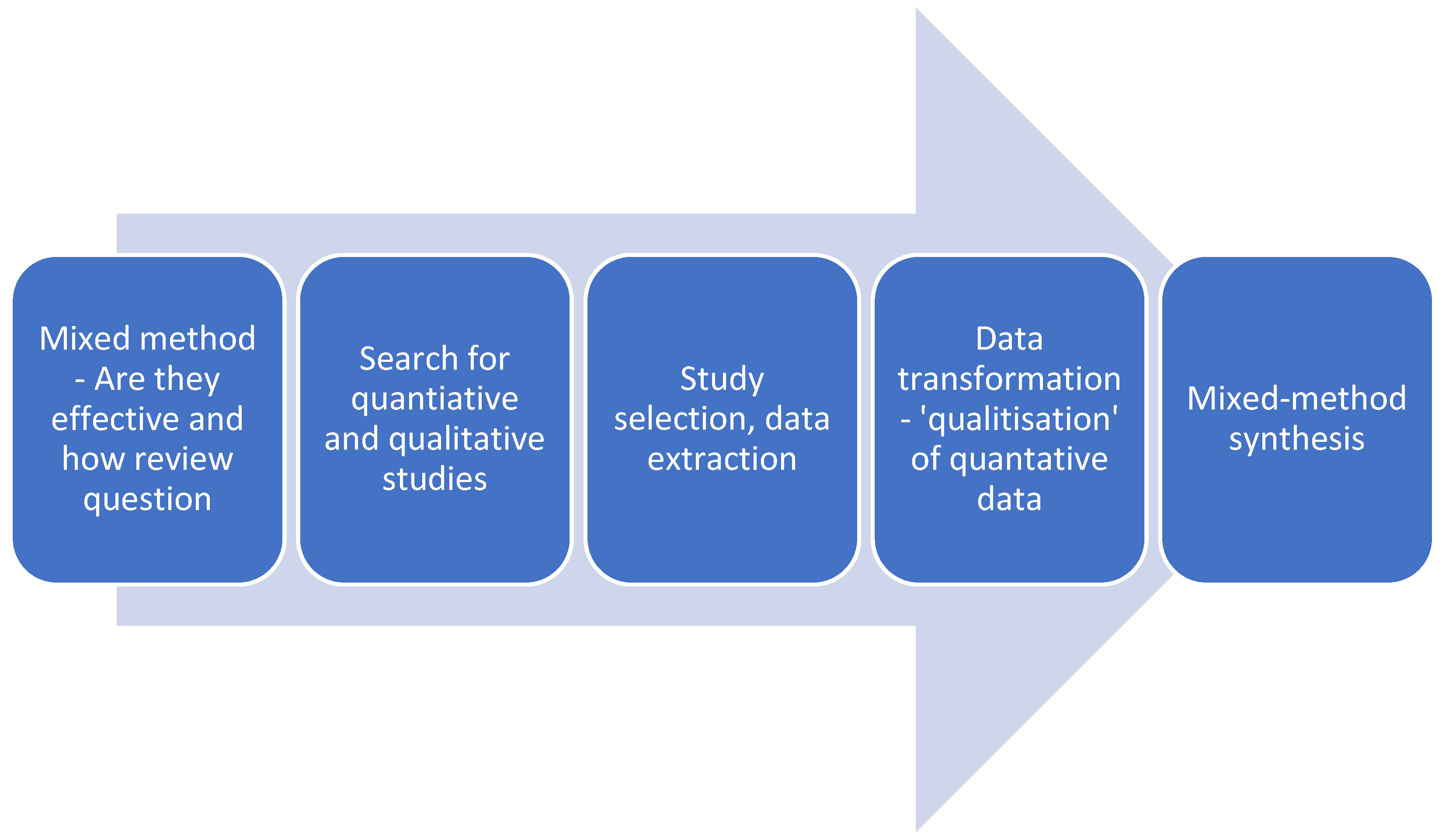
2.1. Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Extraction
2.6. Analysis
3. Results
3.1. Methodological Adequacy
3.2. Intervention Characteristics and Effectiveness
3.3. The Involvement of the Study Population in the Research
3.4. Enablers for Intervention Effectiveness
3.5. Challenges to Interventions
4. Discussion
Review Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Search strategy for Ovid—Medline, PsycInfo, Emcare
- Alcohol
- exp alcohol drinking/ or alcohol$ or
- (alcohol adj2 (problem or pattern or burden or freq* or injury or dependen* or disorder* or drink* or misuse or excess or harm or binge or hazard* or abuse* or consum* or use* or behaviour or behavior or excess* or reduc* or cessation or intoxicat*)).
- Breast cancer
- breast neoplasms or (breast tumor* or breast tumour* or mammary carcinoma* or human mammary car-cinomas or mammary neoplasms or cancer of the breast or cancer of breast).
- Prevention
- primary prevention/ or secondary prevention/ or (prevent* or control*).
- Intervention
- ((program or randomi* or placebo or random* or trial* or pre or post or before or after or intervention or experiment* or evaluat* or quasi).mp. or (nonequivalent control group or posttesting or pretesting or pretest posttest design or pretest posttest control group design or quasi experimental methods or quasi experimental study or time series or time series analysis).sh. or (((nonequivalent or non equivalent) adj3 control$) or posttest$ or post test$ or pre test$ or pretest$ or quasi experiment$ or quasiexperiment$ or timeseries or time series).mp.) not (observational or case-control or case control or cross-sectional or cross sectional or case report or case series).
- PAR
- Community-Based Participatory Research/ or cooperative inquiry.mp. or appreciative inquiry.mp. or action learning.mp. or Cooperative Behavior/ or cooperative behaviour.mp. or knowledge trans*.mp. or implementation science.mp. or research co-production.mp. or collaborative research.mp. or knowledge mobilization.mp. or knowledge mobilisation.mp. or paradigm science.mp. or citizen science.mp. OR
- (codesign* or co-design* or coproduc* or co-produc* or cocreat* or co-creat* or codevelop* or collaborative design or participatory or e-collaboration or Experience based design or experience-based design or EBCD or ((user* or patient* or consumer* or participant* or client* or stakeholder* or peer* or communit* or decision-maker or female or women or citizen*) adj2 (centre* or center* or centric or involv* or participat* or partner* or activat* or advisor* or engag* or collaborat* or consult* or empower* or input* or led or focus* or develop* or plan* or deliver* or servic* or program or strat*))) OR
- (Social justice or participatory or PAR or action research or Community-driven or community driven or consumer driven or Consumer-driven or Citizen Science or paradigm science or user-led or consumer-panel or advisory board or community health promotion).
- All searches were limited to 2008–2021; no language restriction was applied.
References
- WHO. Breast Cancer [Internet]. Breast Cancer. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 20 November 2021).
- Smith, B.; Smith, G.; Hurria, A.; Hortobagyi, G.N.; Buchholz, T.A. Future of Cancer Incidence in the United States: Burdens Upon an Aging, Changing Nation. J. Clin. Oncol. 2009, 27, 2758–2765. [Google Scholar] [CrossRef] [PubMed]
- Gmeinder, M.; Morgan, D.; Mueller, M. How Much Do OECD Countries Spend on Prevention? OECD Health Working Papers(101):48; OECD Publishing: Paris, France, 2017. [Google Scholar]
- Kruk, J. Lifestyle Components and Primary Breast Cancer Prevention. Asian Pac. J. Cancer Prev. 2015, 15, 10543–10555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.-S.; Zhao, Z.; Yang, Z.-N.; Xu, F.; Lu, H.-J.; Zhu, Z.-Y.; Shi, W.; Jiang, J.; Yao, P.-P.; Zhu, H.-P. Risk Factors and Preventions of Breast Cancer. Int. J. Biol. Sci. 2017, 13, 1387–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund. Changes since the 2007 Second Expert Report [Internet]. World Cancer Research Fund. 2018. Available online: https://www.wcrf.org/dietandcancer/changes-since-2007-second-expert-report (accessed on 5 August 2019).
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geidl, W.; Semrau, J.; Pfeifer, K. Health behaviour change theories: Contributions to an ICF-based behavioural exercise therapy for individuals with chronic diseases. Disabil. Rehabil. 2014, 36, 2091–2100. [Google Scholar] [CrossRef] [PubMed]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol consumption and site-specific cancer risk: A comprehensive dose–response meta-analysis. Br. J. Cancer 2014, 112, 580–593. [Google Scholar] [CrossRef]
- Liu, Y.; Nguyen, N.; A Colditz, G. Links between Alcohol Consumption and Breast Cancer: A Look at the Evidence. Women’s Health 2015, 11, 65–77. [Google Scholar] [CrossRef] [Green Version]
- Ba, M.H.W.; Pratt, I.; Chapman, K.; Griffin, H.J.; Croager, E.J.; Olver, I.N.; Sinclair, C.; Slevin, T.J. Alcohol and cancer: A position statement from Cancer Council Australia. Med. J. Aust. 2011, 194, 479–482. [Google Scholar] [CrossRef]
- World Health Organisation. Global Status Report on Alcohol and Health; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Grimshaw, J.M.; Eccles, M.P.; Lavis, J.N.; Hill, S.J.; Squires, J.E. Knowledge translation of research findings. Implement. Sci. 2012, 7, 1–17. [Google Scholar] [CrossRef]
- Wallerstein, N.; Duran, B. Community-Based Participatory Research Contributions to Intervention Research: The Intersection of Science and Practice to Improve Health Equity. Am. J. Public Health 2010, 100, S40–S46. [Google Scholar] [CrossRef]
- Cargo, M.; Mercer, S.L. The Value and Challenges of Participatory Research: Strengthening Its Practice. Annu. Rev. Public Health 2008, 29, 325–350. [Google Scholar] [CrossRef]
- Baum, F.; MacDougall, C.; Smith, D. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, P.A.; Ball, T.J. Balancing empiricism and local cultural knowledge in the design of prevention research. J. Hered. 2005, 82, iii44–iii55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pazoki, R.; Nabipour, I.; Seyednezami, N.; Imami, S.R. Effects of a community-based healthy heart program on increasing healthy women’s physical activity: A randomized controlled trial guided by Community-based Participatory Research (CBPR). BMC Public Health 2007, 7, 216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrison, J.; Akter, K.; Jennings, H.M.; Nahar, T.; Kuddus, A.; Shaha, S.K.; Ahmed, N.; King, C.; Haghparast-Bidgoli, H.; Costello, A.; et al. Participatory learning and action to address type 2 diabetes in rural Bangladesh: A qualitative process evaluation. BMC Endocr. Disord. 2019, 19, 118–210. [Google Scholar] [CrossRef]
- Berger, G.; Peerson, A. Giving young Emirati women a voice: Participatory action research on physical activity. Health Place 2009, 15, 117–124. [Google Scholar] [CrossRef]
- Cardarelli, K.; Jackson, R.; Martin, M.; Linnear, K.; Lopez, R.; Senteio, C.; Weaver, P.; Hill, A.; Banda, J.; Epperson-Brown, M.; et al. Community-based participatory approach to reduce breast cancer disparities in south Dallas. Prog. Community Health Partnersh. Res. Educ. Action 2011, 5, 375–385. [Google Scholar]
- Wong, D.K.P.; Chow, S.F. Beyond clinical trials and narratives: A participatory action research with cancer patient self-help groups. Patient Educ. Couns. 2006, 60, 201–205. [Google Scholar] [CrossRef]
- Morrison, B.; Lilford, R. How can action research apply to health services? Qual. Health Res. 2001, 11, 436–449. [Google Scholar] [CrossRef]
- Anyon, Y.; Bender, K.; Kennedy, H.; DeChants, J. A Systematic Review of Youth Participatory Action Research (YPAR) in the United States: Methodologies, Youth Outcomes, and Future Directions. Health Educ. Behav. 2018, 45, 865–878. [Google Scholar] [CrossRef]
- Jacquez, F.; Vaughn, L.M.; Wagner, E. Youth as partners, participants or passive recipients: A review of children and adolescents in community-based participatory research (CBPR). Am. J. Community Psychol. 2013, 51, 176–189. [Google Scholar] [CrossRef] [PubMed]
- Shamrova, D.P.; Cummings, C.E. Participatory action research (PAR) with children and youth: An integrative review of methodology and PAR outcomes for participants, organizations, and communities. Child. Youth Serv. Rev. 2017, 81, 400–412. [Google Scholar] [CrossRef]
- Roberts, L.; Leonard, K. An Empirical Typology of Drinking Partnerships and Their Relationship to Marital Functioning and Drinking Consequences on JSTOR. J. Marriage Fam. 1998, 60, 515–526. Available online: https://www-jstor-org.ezproxy.flinders.edu.au/stable/353866?seq=1#metadata_info_tab_contents (accessed on 7 January 2022). [CrossRef]
- Aromataris, M. JBI Manual for Evidence Synthesis [Internet]. Adelaide: JBI. 2020. Available online: https://jbi-global-wiki.refined.site/space/MANUAL/3318284344/8.3+The+JBI+approach+to+mixed+method+systematic+reviews (accessed on 18 November 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Pearson, A.; White, H.; Bath-Hextall, F.; Salmond, S.; Apostolo, J.L.A.; Kirkpatrick, P. A mixed-methods approach to systematic reviews. Int. J. Evid. -Based Healhc. 2015, 13, 121–131. [Google Scholar] [CrossRef]
- de Paula Gebara, C.F.; de Castro Bhona, F.M.; Ronzani, T.M.; Lourenço, L.M.; Noto, A.R. Brief intervention and decrease of alcohol consumption among women: A systematic review. Subst. Abus. Treat. Prev. Policy 2013, 8, 1–8. [Google Scholar]
- Kaner, E.F.; Beyer, F.R.; Muirhead, C.; Campbell, F.; Pienaar, E.D.; Bertholet, N.; Daeppen, J.B.; Saunders, J.B.; Burnand, B. Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [Green Version]
- Scott, S.; Parkinson, K.; Kaner, E.; Robalino, S.; Stead, M.; Power, C.; Fitzgerald, N.; Wrieden, W.; Adamson, A. Non-pharmacological interventions designed to reduce health risks due to unhealthy eating behaviour and linked risky or excessive drinking in adults aged 18–25 years: A systematic review protocol. Syst. Rev. 2017, 6, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, R.; Waters, E.; Jackson, N. Systematic Reviews of Health Promotion and Public Health Interventions. 2007. Available online: https://ph.cochrane.org/sites/ph.cochrane.org/files/public/uploads/Guidelines%20HP_PH%20reviews.pdf (accessed on 8 May 2018).
- Aromataris, E. Furthering the science of evidence synthesis with a mix of methods. JBI Evid. Synth. 2020, 18, 2106–2107. [Google Scholar] [CrossRef]
- Gough, D. Qualitative and mixed methods in systematic reviews. Syst. Rev. 2015, 4, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Sandelowski, M.; Leeman, J.; Knafl, K.; Crandell, J.L. Text-in-context: A method for extracting findings in mixed-methods mixed research synthesis studies. J. Adv. Nurs. 2012, 69, 1428–1437. [Google Scholar] [CrossRef] [Green Version]
- Guénel, P.; Cyr, D.; Sabroe, S.; Lynge, E.; Merletti, F.; Ahrens, W.; Baumgardt-Elms, C.; Ménégoz, F.; Olsson, H.; Paulsen, S.; et al. Alcohol Drinking May Increase Risk of Breast Cancer in Men: A European Population-Based Case–Control Study. Cancer Causes Control. 2004, 15, 571–580. [Google Scholar] [CrossRef] [PubMed]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans; World Health Organization; International Agency for Research on Cancer (Eds.) Alcohol Consumption and Ethyl Carbamate; IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; International Agency for Research on Cancer: Lyon, France; Distributed by WHO Press: Geneva, Switzerland, 2010; 1424p. [Google Scholar]
- Calabria, B.; Shakeshaft, A.P.; Havard, A. A systematic and methodological review of interventions for young people experiencing alcohol-related harm. Addiction 2011, 106, 1406–1418. [Google Scholar] [CrossRef]
- World Cancer Research Fund AI for CR. Food, Nutrition, Physical Activity and the Prevention of Cancer: A Global Perspective [Internet]. Washington, DC. 2007. Available online: https://www.wcrf.org/sites/default/files/english.pdf (accessed on 25 February 2019).
- World Health Organization. Global Strategy to Reduce the Harmful Use of Alcohol; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Lash, S. Critique of Information; Sage: Newcastle upon Tyne, UK, 2002; 248p. [Google Scholar]
- Carter, B.; Rees, P.; Hale, L.; Bhattacharjee, D.; Paradkar, M.S. Association between portable screen-based media device access or use and sleep outcomes: A systematic review and meta-analysis. JAMA Pediatrics 2016, 170, 1202–1208. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Stern, C.; Lizarondo, L.; Carrier, J.; Godfrey, C.; Rieger, K.; Salmond, S.; Apóstolo, J.; Kirkpatrick, P.; Loveday, H. Methodological guidance for the conduct of mixed methods systematic reviews. JBI Evid. Synth. 2020, 18, 2108–2118. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Castañeda, S.F.; Giacinto, R.E.; Medeiros, E.A.; Brongiel, I.; Cardona, O.; Perez, P.; Talavera, G.A. Academic-community partnership to develop a patient-centered breast cancer risk reduction program for Latina primary care patients. J. Racial Ethn. Health Disparities 2016, 3, 189–199. [Google Scholar] [CrossRef] [Green Version]
- Cordova, D.; Munoz-Velazquez, J.; Lua, F.M.; Fessler, K.; Warner, S.; Delva, J.; Adelman, N.; Council, Y.L.; Fernandez, A.; Bauermeister, J. Pilot study of a multilevel mobile health app for substance use, sexual risk behaviors, and testing for sexually transmitted infections and HIV among youth: Randomized controlled trial. JMIR mHealth uHealth 2020, 8, e16251. [Google Scholar] [CrossRef]
- Galai, N.; Sirirojn, B.; Aramrattana, A.; Srichan, K.; Thomson, N.; Golozar, A.; Flores, J.M.; Willard, N.; Ellen, J.M.; Sherman, S.G.; et al. A cluster randomized trial of community mobilization to reduce methamphetamine use and HIV risk among youth in Thailand: Design, implementation and results. Soc. Sci. Med. 2018, 211, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Gray, N.; Mays, M.Z.; Wolf, D.; Jirsak, J. A culturally focused wellness intervention for American Indian women of a small southwest community: Associations with alcohol use, abstinence self-efficacy, symptoms of depression, and self-esteem. Am. J. Health Promot. 2010, 25, e1–e10. [Google Scholar] [CrossRef] [PubMed]
- Hanks, R.A.; Rapport, L.J.; Wertheimer, J.; Koviak, C. Randomized controlled trial of peer mentoring for individuals with traumatic brain injury and their significant others. Arch. Phys. Med. Rehabil. 2012, 93, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Tollison, S.J.; Lee, C.M.; Neighbors, C.; Neil, T.A.; Olson, N.D.; Larimer, M.E. Questions and reflections: The use of motivational interviewing microskills in a peer-led brief alcohol intervention for college students. Behav. Ther. 2008, 39, 183–194. [Google Scholar] [CrossRef] [Green Version]
- Jongudomkarn, D. A volunteer alcohol consumption reduction campaign: Participatory action research among Thai women in the Isaan region. Asian Pac. J. Cancer Prev. 2014, 15, 7343–7350. [Google Scholar] [CrossRef] [PubMed]
- Jongudomkarn, D.; Singhawara, P.; Macduff, C. Village voices: Lessons about processes for disease prevention from a qualitative study of family health leaders in a community in northeastern Thailand. Asian Pac. J. Cancer Prev. 2015, 16, 4401–4408. [Google Scholar] [CrossRef] [Green Version]
- Day, S.J.; Altman, D.G. Blinding in clinical trials and other studies. BMJ 2000, 321, 504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sciacca, J.P. Student peer health education: A powerful yet inexpensive helping strategy. Peer Facil. Q. 1987, 5, 4–6. [Google Scholar]
- Skizim, M.; Harris, N.; Leonardi, C.; Scribner, R. Academic-community partnership development to enhance program outcomes in underserved communities: A case study. Ethn. Dis. 2017, 27 (Suppl. 1), 321. [Google Scholar] [CrossRef] [Green Version]
- Harden, A.; Thomas, J. Mixed methods and systematic reviews: Examples and emerging issues. Sage Handb. Mix. Methods Soc. Behav. Res. 2010, 2, 749–774. [Google Scholar]



{kind=link}
{kind=link}
| Criterion | Inclusion | Exclusion |
|---|---|---|
| Time period | 2008 to May 2021 | Studies prior to 2008 |
| Study design | Qualitative, mixed-method, and quantitative empirical studies published in peer-reviewed scientific journals. | Literature not published in peer-reviewed scientific journals. |
| Intervention focus | Intervention with participatory action research principles where the study population participated in at least one stage of agenda setting, research planning, data collection, analysis, or data interpretation. | Observational studies or studies with no evidence of participatory action research principles, for example, where the study population are passive participants. |
| Outcomes | Study reports on the outcomes or impact of the program on the study population related to the behaviour, perception, knowledge, risk, or attitudes of drinking alcohol or breast cancer prevention risk factors (smoking, physical activity, diet). | Exclude studies reporting outcomes solely on screening rates, surgical, genetic, pharmacological, or alcohol dependence/disorder. |
| Population | Human participants with a mean age greater than 18 years. | Animal studies or studies with male-only participants or participants diagnosed with breast cancer or where the majority are veterans (armed forces current or have previously served) or prisoners or homeless people or preconception-focused or pregnant women or sex workers or emergency/trauma acute care setting interventions. |
| Project Name | Risk Factor | Population and Setting | Paradigm | Study Design | Intervention and Select Results |
|---|---|---|---|---|---|
| Nuestra Cocina: Cancer Risk Reduction Intervention [49] | Nutrition | Women at community health centres | Quantitative | Quasi-experimental | The academic-community partnership intervention found improvements in breast cancer prevention knowledge and dietary improvements. |
| Storytelling 4 Empowerment Group [52] | Alcohol | Young people at community health centres | Quantitative | Randomized control trial (RCT) | The mHealth tablet-based application intervention found reductions in alcohol use compared to the control group. |
| Preventing Rural Thai Methamphetamine Abuse and HIV by Community Mobilization [53] | Alcohol | Young people in multiple settings; rural primary schools, community health/hospital and community settings | Quantitative | RCT | The community coalition intervention found that alcohol use remained high in control and intervention communities. Only minor changes were present from baseline, and the overall study reported a null effect. |
| Community-developed health promotion intervention [51] | Alcohol | Women at a house in their local neighbourhood | Quantitative | Quasi-experimental | The culturally-focused wellness intervention found reductions in alcohol consumption with women consuming moderate to high levels of alcohol prior to the intervention achieving greater substantial absolute decrease than lighter drinkers. |
| Peer Mentoring for Individuals With Traumatic Brain Injury and Their Significant Others [48] | Alcohol | Women and men at a rehabilitation hospital | Quantitative | RCT | Significant reductions in alcohol use were found in the intervention group compared to the control. |
| Brief Alcohol Screening and Intervention for College Students [50] | Alcohol | Young people at a college campus | Quantitative | RCT | Significant reductions in alcohol use were found in the experimental group from baseline to 3-month follow-up. |
| Family Health Leader project in north eastern Iaan region of Thailand [55] | Alcohol | Women in community forums and home visits | Qualitative | Quasi-experimental | Peer modelling was effective in reducing alcohol consumption through empowering participants to share knowledge regarding alcohol use and providing family support for members with problematic alcohol consumption. |
| Family Health Leader project north eastern Loie region of Thailand [54] | Alcohol | Women and men in community forums and home visits | Qualitative | Quasi-experimental | Peer-led interventions led to significant decrease in AUDIT (Alcohol use Disorder Identification Test) scores compared to pre-intervention levels. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomas, J.A.; Miller, E.R.; Ward, P.R. Lifestyle Interventions through Participatory Research: A Mixed-Methods Systematic Review of Alcohol and Other Breast Cancer Behavioural Risk Factors. Int. J. Environ. Res. Public Health 2022, 19, 980. https://doi.org/10.3390/ijerph19020980
Thomas JA, Miller ER, Ward PR. Lifestyle Interventions through Participatory Research: A Mixed-Methods Systematic Review of Alcohol and Other Breast Cancer Behavioural Risk Factors. International Journal of Environmental Research and Public Health. 2022; 19(2):980. https://doi.org/10.3390/ijerph19020980
Chicago/Turabian StyleThomas, Jessica A., Emma R. Miller, and Paul R. Ward. 2022. "Lifestyle Interventions through Participatory Research: A Mixed-Methods Systematic Review of Alcohol and Other Breast Cancer Behavioural Risk Factors" International Journal of Environmental Research and Public Health 19, no. 2: 980. https://doi.org/10.3390/ijerph19020980